
Diagnostic Accuracy of HPV Detection in Patients with Oropharyngeal Squamous Cell Carcinomas: A Systematic Review and Meta-Analysis

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
3. Results
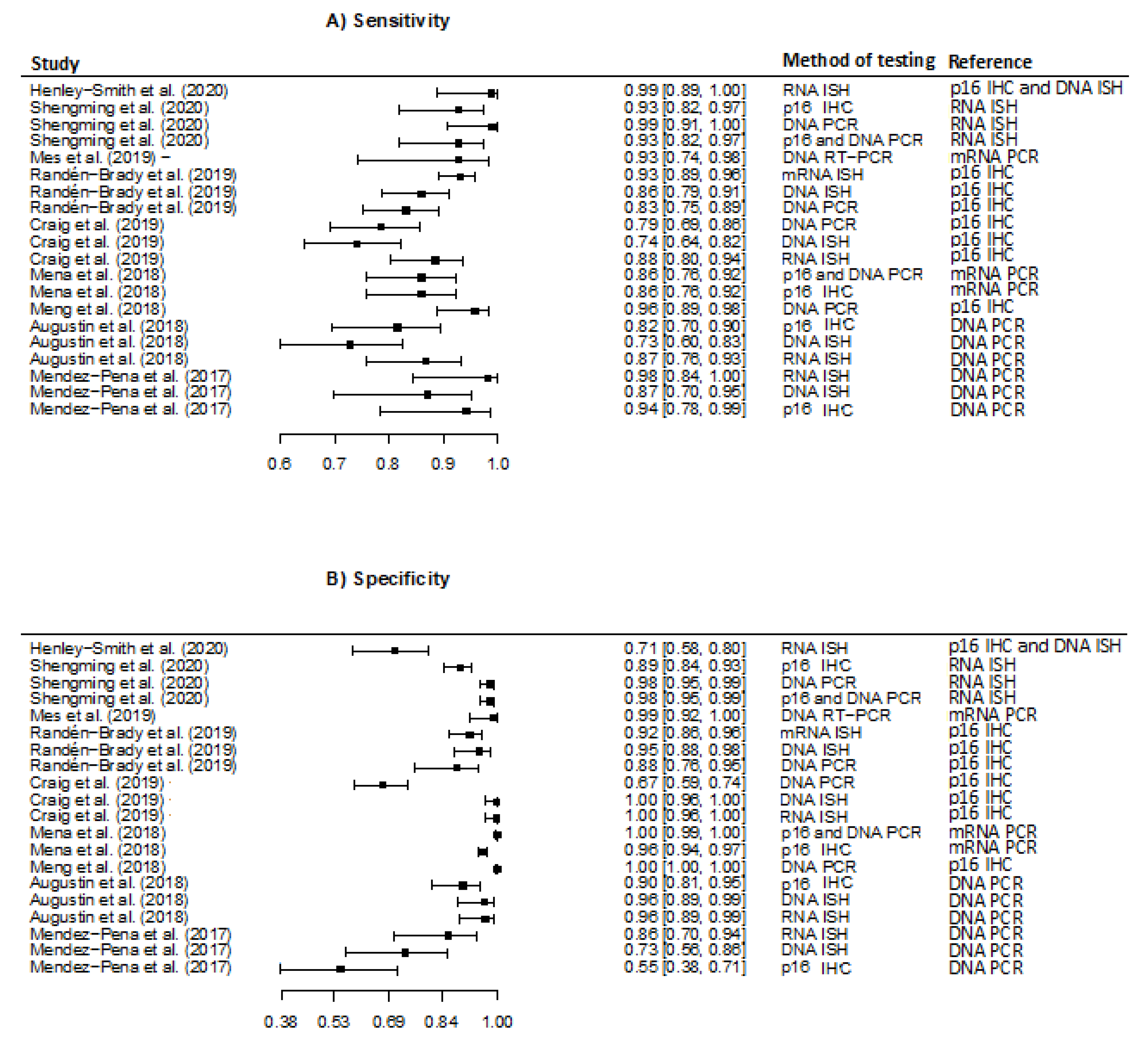
3.1. Diagnostic Accuracy of HPV in Tissue Samples
3.2. Diagnostic Accuracy of Detecting HPV in Blood Samples
3.3. Diagnostic Accuracy of Detecting HPV in Oral Samples
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Garnaes, E.; Kiss, K.; Andersen, L.; Therkildsen, M.H.; Franzmann, M.B.; Filtenborg-Barnkob, B.; Hoegdall, E.; Krenk, L.; Josiassen, M.; Lajer, C.B.; et al. A high and increasing HPV prevalence in tonsillar cancers in Eastern Denmark, 2000–2010: The largest registry-based study to date. Int. J. Cancer 2015, 136, 2196–2203. [Google Scholar] [CrossRef]
- Carlander, A.-L.F.; Grønhøj Larsen, C.; Jensen, D.H.; Garnæs, E.; Kiss, K.; Andersen, L.; Olsen, C.H.; Franzmann, M.; Høgdall, E.; Kjær, S.K.; et al. Continuing rise in oropharyngeal cancer in a high HPV prevalence area: A Danish population-based study from 2011 to 2014. Eur. J. Cancer 2017, 70, 75–82. [Google Scholar] [CrossRef]
- Ang, K.K.; Harris, J.; Wheeler, R.; Weber, R.; Rosenthal, D.I.; Nguyen-Tan, P.F.; Westra, W.H.; Chung, C.H.; Jordan, R.C.; Lu, C.; et al. Human papillomavirus and survival of patients with oropharyngeal cancer. N. Engl. J. Med. 2010, 363, 24–35. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chaturvedi, A.K.; Engels, E.A.; Pfeiffer, R.M.; Hernandez, B.Y.; Xiao, W.; Kim, E.; Jiang, B.; Goodman, M.T.; Sibug-Saber, M.; Cozen, W.; et al. Human papillomavirus and rising oropharyngeal cancer incidence in the United States. J. Clin. Oncol. 2011, 29, 4294–4301. [Google Scholar] [CrossRef] [PubMed]
- Lai, S.; Wenaas, A.E.; Sandulache, V.C.; Hartman, C.; Chiao, E.; Kramer, J.; Zevallos, J.P. Prognostic significance of p16 cellular localization in oropharyngeal squamous cell carcinoma. Ann. Clin. Lab. Sci. 2016, 46, 132–139. [Google Scholar]
- Tomaic, V. Functional roles of E6 and E7 oncoproteins in HPV-induced malignancies at diverse anatomical sites. Cancers 2016, 8, 95. [Google Scholar] [CrossRef] [Green Version]
- Zamani, M.; Grønhøj, C.; Jensen, D.H.; Carlander, A.F.; Agander, T.; Kiss, K.; Olsen, C.; Baandrup, L.; Nielsen, F.C.; Andersen, E.; et al. The current epidemic of HPV-associated oropharyngeal cancer: An 18-year Danish population-based study with 2,169 patients. Eur. J. Cancer 2020, 134, 52–59. [Google Scholar] [CrossRef]
- Gillison, M.L.; Zhang, Q.; Jordan, R.; Xiao, W.; Westra, W.H.; Trotti, A.; Spencer, S.; Harris, J.; Chung, C.H.; Ang, K.K. Tobacco smoking and increased risk of death and progression for patients with p16-positive and p16-negative oropharyngeal cancer. J. Clin. Oncol. 2012, 30, 2102–2111. [Google Scholar] [CrossRef] [PubMed]
- Gillison, M.L.; Koch, W.M.; Capone, R.B.; Spafford, M.; Westra, W.H.; Wu, L.; Zahurak, M.L.; Daniel, R.W.; Viglione, M.; Symer, D.E.; et al. Evidence for a causal association between human papillomavirus and a subset of head and neck cancers. J. Natl. Cancer Inst. 2000, 92, 709–720. [Google Scholar] [CrossRef] [PubMed]
- Ragin, C.C.R.; Taioli, E. Survival of squamous cell carcinoma of the head and neck in relation to human papillomavirus infection: Review and meta-analysis. Int. J. Cancer 2007, 121, 1813–1820. [Google Scholar] [CrossRef] [PubMed]
- Grønhøj Larsen, C.; Jensen, D.H.; Fenger Carlander, A.-L.; Kiss, K.; Andersen, L.; Holkmann Olsen, C.; Andersen, E.; Garnæs, E.; Cilius, F.; Specht, L.; et al. Novel nomograms for survival and progression in HPV+ and HPV- oropharyngeal cancer: A population-based study of 1,542 consecutive patients. Oncotarget 2016, 7, 71761. [Google Scholar] [CrossRef] [PubMed]
- Fakhry, C.; Zhang, Q.; Nguyen-Tan, P.F.; Rosenthal, D.; El-Naggar, A.; Garden, A.S.; Soulieres, D.; Trotti, A.; Avizonis, V.; Ridge, J.A.; et al. Human papillomavirus and overall survival after progression of oropharyngeal squamous cell carcinoma. J. Clin. Oncol. 2014, 32, 3365. [Google Scholar] [CrossRef] [PubMed]
- Argiris, A.; Li, S.; Ghebremichael, M.; Egloff, A.M.; Wang, L.; Forastiere, A.A.; Burtness, B.; Mehra, R. Prognostic significance of human papillomavirus in recurrent or metastatic head and neck cancer: An analysis of Eastern Cooperative Oncology Group trials. Ann. Oncol. 2014, 25, 1410–1416. [Google Scholar] [CrossRef] [PubMed]
- Garnaes, E.; Frederiksen, K.; Kiss, K.; Andersen, L.; Therkildsen, M.H.; Franzmann, M.B.; Specht, L.; Andersen, E.; Norrild, B.; Kjaer, S.K.; et al. Double positivity for HPV DNA/p16 in tonsillar and base of tongue cancer improves prognostication: Insights from a large population-based study. Int. J. Cancer 2016, 139, 2598–2605. [Google Scholar] [CrossRef]
- Lewis, J.S.; Beadle, B.; Bishop, J.A.; Chernock, R.D.; Colasacco, C.; Lacchetti, C.; Moncur, J.T.; Rocco, J.W.; Schwartz, M.R.; Seethala, R.R.; et al. Human papillomavirus testing in head and neck carcinomas guideline from the college of American pathologists. Arch. Pathol. Lab. Med. 2018, 142, 559–597. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lewis, J.S. p16 Immunohistochemistry As a Standalone Test for Risk Stratification in Oropharyngeal Squamous Cell Carcinoma. Head Neck Pathol. 2012, 6, 75–82. [Google Scholar] [CrossRef]
- Emergence of a Novel Staging System for Oropharyngeal Squamous Cell Carcinoma Based on HPV Status. Available online: https://www.cancernetwork.com/view/emergence-novel-staging-system-oropharyngeal-squamous-cell-carcinoma-based-hpv-status (accessed on 7 May 2021).
- Schache, A.; Liloglou, T.; Risk, J.M.; Filia, A.; Jones, T.M.; Sheard, J.; Woolgar, J.A.; Helliwell, T.R.; Triantafyllou, A.; Robinson, M.; et al. Evaluation of human papilloma virus diagnostic testing in oropharyngeal squamous cell carcinoma: Sensitivity, specificity and prognostic discrimination Conclusions—Caution must be exercised in applying HPV16 diagnostic tests due to significant disparities. Clin. Cancer Res. 2011, 17, 6262–6271. [Google Scholar] [CrossRef] [Green Version]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.J. PRISMA 2009 Flow Diagram. Prism. Statement 2009, 6, e1000097. [Google Scholar]
- Reitsma, J.B.; Glas, A.S.; Rutjes, A.W.S.; Scholten, R.J.; Bossuyt, P.M.; Zwinderman, A.H. Bivariate analysis of sensitivity and specificity produces informative summary measures in diagnostic reviews. J. Clin. Epidemiol. 2005, 58, 982–990. [Google Scholar] [CrossRef]
- Henley-Smith, R.; Santambrogio, A.; Andoniadou, C.L.; Odell, E.; Thavaraj, S. RNA in situ hybridization for human papillomavirus testing in oropharyngeal squamous cell carcinoma on a routine clinical diagnostic platform. J. Oral Pathol. Med. 2021, 50, 68–75. [Google Scholar] [CrossRef]
- Xu, S.; Sun, B.; Zhou, R.; Shi, C.; Han, Y.; Li, J.; Sun, J.; Tian, Z.; Zhang, Z.; Li, J. Evaluation of p16 as a surrogate marker for transcriptionally active human papillomavirus status of oropharyngeal squamous cell carcinoma in an eastern Chinese population. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2020, 129, 236–245.e2. [Google Scholar] [CrossRef] [PubMed]
- Mes, S.W.; Heideman, D.A.M.; Bloemena, E.; Brink, A.; Bogaarts, M.; Leemans, C.R.; Brakenhoff, R.H. Development and Validation of a Novel and Rapid Molecular Detection Method for High-Risk Human Papillomavirus in Formalin-Fixed, Paraffin-Embedded Tumor Tissue. J. Mol. Diagn. 2020, 22, 262–271. [Google Scholar] [CrossRef]
- Randén-Brady, R.; Carpén, T.; Jouhi, L.; Syrjänen, S.; Haglund, C.; Tarkkanen, J.; Remes, S.; Mäkitie, A.; Mattila, P.S.; Silén, S.; et al. In situ hybridization for high-risk HPV E6/E7 mRNA is a superior method for detecting transcriptionally active HPV in oropharyngeal cancer. Hum. Pathol. 2019, 90, 97–105. [Google Scholar] [CrossRef] [PubMed]
- Craig, S.G.; Anderson, L.A.; Moran, M.; Graham, L.; Currie, K.; Rooney, K.; Robinson, M.; Bingham, V.; Cuschieri, K.S.; McQuaid, S.; et al. Comparison of molecular assays for HPV testing in oropharyngeal squamous cell carcinomas: A population-based study in Northern Ireland. Cancer Epidemiol. Biomark. Prev. 2020, 29, 31–38. [Google Scholar] [CrossRef] [PubMed]
- Mena, M.; Taberna, M.; Tous, S.; Marquez, S.; Clavero, O.; Quiros, B.; Lloveras, B.; Alejo, M.; Leon, X.; Quer, M.; et al. Double positivity for HPV-DNA/p16ink4a is the biomarker with strongest diagnostic accuracy and prognostic value for human papillomavirus related oropharyngeal cancer patients. Oral Oncol. 2018, 78, 137–144. [Google Scholar] [CrossRef] [Green Version]
- Meng, H.X.; Miao, S.S.; Chen, K.; Li, H.N.; Yao, G.; Geng, J.; Wang, H.; Shi, Q.T.; He, J.; Mao, X.; et al. Association of p16 as prognostic factors for oropharyngeal cancer: Evaluation of p16 in 1470 patients for a 16 year study in Northeast China. Biomed Res. Int. 2018, 2018, 9594568. [Google Scholar] [CrossRef] [Green Version]
- Augustin, J.; Outh-Gauer, S.; Mandavit, M.; Gasne, C.; Grard, O.; Denize, T.; Nervo, M.; Mirghani, H.; Laccourreye, O.; Bonfils, P.; et al. Evaluation of the efficacy of the 4 tests (p16 immunochemistry, polymerase chain reaction, DNA, and RNA in situ hybridization) to evaluate a human papillomavirus infection in head and neck cancers: A cohort of 348 French squamous cell carcinomas. Hum. Pathol. 2018, 78, 63–71. [Google Scholar] [CrossRef] [PubMed]
- Mendez-Pena, J.E.; Sadow, P.M.; Nose, V.; Hoang, M.P. RNA chromogenic in situ hybridization assay with clinical automated platform is a sensitive method in detecting high-risk human papillomavirus in squamous cell carcinoma. Hum. Pathol. 2017, 63, 184–189. [Google Scholar] [CrossRef]
- Wright, M.F.; Weiss, V.L.; Lewis, J.S.; Schmitz, J.E.; Ely, K.A. Determination of high-risk HPV status of head and neck squamous cell carcinoma using the Roche cobas HPV test on cytologic specimens and acellular supernatant fluid. Cancer Cytopathol. 2020, 128, 482–490. [Google Scholar] [CrossRef]
- Menegaldo, A.; Schroeder, L.; Holzinger, D.; Tirelli, G.; Dal Cin, E.; Tofanelli, M.; Rigo, S.; Mantovani, M.; Stellin, M.; Del Mistro, A.; et al. Detection of HPV16/18 E6 Oncoproteins in Head and Neck Squamous Cell Carcinoma Using a Protein Immunochromatographic Assay. Laryngoscope 2021, 131, 1042–1048. [Google Scholar] [CrossRef]
- Channir, H.I.; Grønhøj Larsen, C.; Ahlborn, L.B.; van Overeem Hansen, T.; Gerds, T.A.; Charabi, B.W.; Vainer, B.; von Buchwald, C.; Lajer, C.B.; Kiss, K. Validation study of HPV DNA detection from stained FNA smears by polymerase chain reaction: Improving the diagnostic workup of patients with a tumor on the neck. Cancer Cytopathol. 2016, 124, 820–827. [Google Scholar] [CrossRef]
- Sivars, L.; Landin, D.; Haeggblom, L.; Tertipis, N.; Grün, N.; Bersani, C.; Marklund, L.; Ghaderi, M.; Näsman, A.; Ramqvist, T.; et al. Human papillomavirus DNA detection in fine-needle aspirates as indicator of human papillomavirus–positive oropharyngeal squamous cell carcinoma: A prospective study. Head Neck 2017, 39, 419–426. [Google Scholar] [CrossRef] [Green Version]
- Chernesky, M.; Jang, D.; Schweizer, J.; Arias, M.; Doerwald-Munoz, L.; Gupta, M.; Jackson, B.; Archibald, S.; Young, J.; Lytwyn, A.; et al. HPV E6 oncoproteins and nucleic acids in neck lymph node fine needle aspirates and oral samples from patients with oropharyngeal squamous cell carcinoma. Papillomavirus Res. 2018, 6, 1–5. [Google Scholar] [CrossRef] [PubMed]
- Hanna, G.J.; Supplee, J.G.; Kuang, Y.; Mahmood, U.; Lau, C.J.; Haddad, R.I.; Jänne, P.A.; Paweletz, C.P. Plasma HPV cell-free DNA monitoring in advanced HPV-associated oropharyngeal cancer. Ann. Oncol. 2018, 29, 1980–1986. [Google Scholar] [CrossRef] [PubMed]
- Reder, H.; Taferner, V.F.; Wittekindt, C.; Bräuninger, A.; Speel, E.J.M.; Gattenlöhner, S.; Wolf, G.; Klussmann, J.P.; Wuerdemann, N.; Wagner, S. Plasma Cell-Free Human Papillomavirus Oncogene E6 and E7 DNA Predicts Outcome in Oropharyngeal Squamous Cell Carcinoma. J. Mol. Diagn. 2020, 22, 1333–1343. [Google Scholar] [CrossRef]
- Chera, B.S.; Kumar, S.; Beaty, B.T.; Marron, D.; Jefferys, S.; Green, R.; Goldman, E.C.; Amdur, R.; Sheets, N.; Dagan, R.; et al. Rapid clearance profile of plasma circulating tumor HPV type 16 DNA during chemoradiotherapy correlates with disease control in HPV-associated oropharyngeal cancer. Clin. Cancer Res. 2019, 25, 4682–4690. [Google Scholar] [CrossRef]
- Ren, J.; Xu, W.; Su, J.; Ren, X.; Cheng, D.; Chen, Z.; Bender, N.; Mirshams, M.; Habbous, S.; de Almeida, J.R.; et al. Multiple imputation and clinico-serological models to predict human papillomavirus status in oropharyngeal carcinoma: An alternative when tissue is unavailable. Int. J. Cancer 2020, 146, 2166–2174. [Google Scholar] [CrossRef] [PubMed]
- Damerla, R.R.; Lee, N.Y.; You, D.; Soni, R.; Shah, R.; Reyngold, M. Detection of Early Human Papillomavirus—Associated Cancers by Liquid Biopsy. JCO Precis. Oncol. 2019, 3, 1–17. [Google Scholar] [CrossRef]
- Mazurek, A.M.; Rutkowski, T.; Śnietura, M.; Pigłowski, W.; Suwiński, R.; Składowski, K. Detection of circulating HPV16 DNA as a biomarker in the blood of patients with human papillomavirus-positive oropharyngeal squamous cell carcinoma. Head Neck 2019, 41, 632–641. [Google Scholar] [CrossRef]
- Economopoulou, P.; Koutsodontis, G.; Avgeris, M.; Strati, A.; Kroupis, C.; Pateras, I.; Kirodimos, E.; Giotakis, E.; Kotsantis, I.; Maragoudakis, P.; et al. HPV16 E6/E7 expression in circulating tumor cells in oropharyngeal squamous cell cancers: A pilot study. PLoS ONE 2019, 14, e0215984. [Google Scholar] [CrossRef]
- Lang Kuhs, K.A.; Kreimer, A.R.; Trivedi, S.; Holzinger, D.; Pawlita, M.; Pfeiffer, R.M.; Gibson, S.P.; Schmitt, N.C.; Hildesheim, A.; Waterboer, T.; et al. Human papillomavirus 16 E6 antibodies are sensitive for human papillomavirus–driven oropharyngeal cancer and are associated with recurrence. Cancer 2017, 123, 4382–4390. [Google Scholar] [CrossRef] [Green Version]
- Holzinger, D.; Wichmann, G.; Baboci, L.; Michel, A.; Höfler, D.; Wiesenfarth, M.; Schroeder, L.; Boscolo-Rizzo, P.; Herold-Mende, C.; Dyckhoff, G.; et al. Sensitivity and specificity of antibodies against HPV16 E6 and other early proteins for the detection of HPV16-driven oropharyngeal squamous cell carcinoma. Int. J. Cancer 2017, 140, 2748–2757. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Qureishi, A.; Ali, M.; Fraser, L.; Shah, K.A.; Møller, H.; Winter, S. Saliva testing for human papilloma virus in oropharyngeal squamous cell carcinoma: A diagnostic accuracy study. Clin. Otolaryngol. 2018, 43, 151–157. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fakhry, C.; Blackford, A.L.; Neuner, G.; Xiao, W.; Jiang, B.; Agrawal, A.; Gillison, M.L. Association of Oral Human Papillomavirus DNA Persistence with Cancer Progression after Primary Treatment for Oral Cavity and Oropharyngeal Squamous Cell Carcinoma. JAMA Oncol. 2019, 5, 985–992. [Google Scholar] [CrossRef] [PubMed]
- Martin-Gomez, L.; Fulp, J.; Schell, M.J.; Sirak, B.; Abrahamsen, M.; Isaacs-Soriano, K.A.; Lorincz, A.; Wenig, B.; Chung, C.H.; Caudell, J.; et al. Oral Gargle-Tumor Biopsy Human Papillomavirus (HPV) Agreement and Associated Factors Among Oropharyngeal Squamous Cell Carcinoma (OPSCC) Cases. Oral Oncol. 2019, 92, 85–91. [Google Scholar] [CrossRef] [PubMed]
- Borena, W.; Schartinger, V.H.; Dudas, J.; Ingruber, J.; Greier, M.C.; Steinbichler, T.B.; Laimer, J.; Stoiber, H.; Riechelmann, H.; Kofler, B. HPV-induced oropharyngeal cancer and the role of the E7 oncoprotein detection via brush test. Cancers 2020, 12, 2388. [Google Scholar] [CrossRef] [PubMed]
- Prigge, E.S.; Arbyn, M.; von Knebel Doeberitz, M.; Reuschenbach, M. Diagnostic accuracy of p16INK4a immunohistochemistry in oropharyngeal squamous cell carcinomas: A systematic review and meta-analysis. Int. J. Cancer 2017, 140, 1186–1198. [Google Scholar] [CrossRef] [Green Version]
- Larsen, C.G.; Gyldenløve, M.; Jensen, D.H.; Therkildsen, M.H.; Kiss, K.; Norrild, B.; Konge, L.; Von Buchwald, C. Correlation between human papillomavirus and p16 overexpression in oropharyngeal tumours: A systematic review. Br. J. Cancer 2014, 110, 1587–1594. [Google Scholar] [CrossRef]
- Christensen, E.; Birkenkamp-Demtröder, K.; Sethi, H.; Shchegrova, S.; Salari, R.; Nordentoft, I.; Wu, H.T.; Knudsen, M.; Lamy, P.; Lindskrog, S.V.; et al. Early detection of metastatic relapse and monitoring of therapeutic efficacy by ultra-deep sequencing of plasma cell-free DNA in patients with urothelial bladder carcinoma. J. Clin. Oncol. 2019, 37, 1547–1557. [Google Scholar] [CrossRef]
- Reinert, T.; Henriksen, T.V.; Christensen, E.; Sharma, S.; Salari, R.; Sethi, H.; Knudsen, M.; Nordentoft, I.; Wu, H.T.; Tin, A.S.; et al. Analysis of Plasma Cell-Free DNA by Ultradeep Sequencing in Patients with Stages i to III Colorectal Cancer. JAMA Oncol. 2019, 5, 1124–1131. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schøler, L.V.; Reinert, T.; Ørntoft, M.B.W.; Kassentoft, C.G.; Arnadøttir, S.S.; Vang, S.; Nordentoft, I.; Knudsen, M.; Lamy, P.; Andreasen, D.; et al. Clinical implications of monitoring circulating Tumor DNA in patients with colorectal cancer. Clin. Cancer Res. 2017, 23, 5437–5445. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wuerdemann, N.; Jain, R.; Adams, A.; Speel, E.J.M.; Wagner, S.; Joosse, S.A.; Klussmann, J.P. Cell-free hpv-dna as a biomarker for oropharyngeal squamous cell carcinoma—A step towards personalized medicine? Cancers 2020, 12, 2997. [Google Scholar] [CrossRef] [PubMed]
- Kreimer, A.R.; Chaturvedi, A.K.; Alemany, L.; Anantharaman, D.; Bray, F.; Carrington, M.; Doorbar, J.; D’Souza, G.; Fakhry, C.; Ferris, R.L.; et al. Summary from an international cancer seminar focused on human papillomavirus (HPV)-positive oropharynx cancer, convened by scientists at IARC and NCI. Oral Oncol. 2020, 108, 104736. [Google Scholar] [CrossRef] [PubMed]
- Gipson, B.J.; Robbins, H.A.; Fakhry, C.; D’Souza, G. Sensitivity and specificity of oral HPV detection for HPV-positive head and neck cancer. Oral Oncol. 2018, 77, 52–56. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Author (Year of Publication) Country [Study] | Study Period | OPSCC Patients. Total/HPV+ | Sample | Method of Testing | Reference | True Positive | False Positive | False Negative | True Negative | Results |
|---|---|---|---|---|---|---|---|---|---|---|
| Henley-Smith et al. (2020) London [21] | 2005–2016 | 100/38 | FFPE | RNA ISH | p16 IHC, staining >70% and DNA ISH | 38 | 18 | 0 | 44 | NR. The 18 false positive cases were p16+/HPV- |
| Shengming et al. (2020) China [22] | 2014–2019 | 257/47 | FFPE | p16 IHC staining >70% DNA PCR | RNA ISH | p16: 44 DNA PCR: 47 p16/DNA PCR: 44 | p16: 22 DNA PCR: 4 p16/DNA PCR: 4 | p16: 3 DNA PCR: 0 p16/DNA PCR: 3 | p16: 188 DNA PCR: 206 p16/DNA PCR: 206 | p16 ISH: Sen: 93.6%; Spe: 89.10% DNA PCR: Sen: 97.9%; Spe: 97.6% p16 and DNA PCR: Sen: 91.7%; Spe: 98.1% |
| Mes et al. (2019) Netherlands [23] | 2008–2011 | 80/20 | FFPE | DNA RT-PCR | HPV16 E6 mRNA RT-PCR | 19 | 0 | 1 | 55 | NR |
| Randén-Brady et al. (2019) Finland [24] | Study I: 2000–2009 Study 2: 2012–2016 | Study 1: 202/NR Study 2: 155/NR Study 1 + 2: HPV positive: 226 | FFPE | Study 1: DNA ISH Study 2: DNA PCR Study 1 + 2: results combined: E6/E7 mRNA ISH | p16 IHC, staining >70% | mRNA: 211 DNA ISH: 101 DNA PCR: 91 | mRNA: 10 DNA ISH: 4 HPV PCR: 5 | mRNA: 15 DNA ISH: 16 HPV PCR: 18 | mRNA: 121 DNA ISH: 81 HPV PCR: 41 | mRNA ISH: Sen: 93.4%; Spe: 92.4% DNA ISH: Sen: 86.3%; Spe: 95.3% DNA PCR: Sen: 83.5%; Spe: 89.1% |
| Craig et al. (2019) Ireland [25] | 2000–2011 | 221/90 | FFPE | RNA-ISH DNA-ISH DNA-PCR | p16 IHC, staining >70% | DNA PCR: 71 DNA ISH: 67 RNA ISH:80 | DNA PCR: 43 DNA ISH: 0 RNA ISH: 0 | DNA PCR: 19 DNA ISH: 23 RNA ISH:10 | DNA PCR: 88 DNA ISH: 131 RNA ISH: 131 | DNA PCR: Sen: 79% (95% CI: 69–87); Spe: 67% (95% CI: 58–75) DNA ISH: Sen: 74% (95% CI: 64–83); Spe: 100% (95% CI: 87–100) RNA ISH: Sen: 88% (95% CI: 80–94); Spe: 100% (95% CI: 96–100) |
| Mena et al. (2018) Spain [26] | 1990–2013 | 788/80 | FFPE | DNA PCR p16 IHC, staining >70% | E6 mRNA RT-PCR | DNA PCR/p16: 58 p16: 58 | DNA PCR/p16: 0 p16: 28 | DNA PCR/p16: 9 p16: 9 | DNA PCR/p16: 721 p16: 691 | DNA PCR/p16: Sen: 86.6% (95% CI 76.0–93.7); Spe: 100.0% (95% CI 99.5–100.0). p16: Sen: 86.6% (95% CI 76.0–93.7); Spe: 96.1% (95% CI 94.4–97.4) |
| Meng et al. (2018) China [27] | 2000–2016 | 1470/81 | FFPE | DNA PCR | p16 IHC, staining >80% | 78 | 0 | 3 | 1389 | Sen: 100% Spe: 96% |
| Augustin et al. (2018) France [28] | 2011–2013 | 126/56 | FFPE | p16 IHC, staining >70% DNA-ISH RNA-ISH | DNA PCR | p16: 46 DNA ISH: 41 RNA ISH:49 | p16: 7 DNA ISH: 2 RNA ISH: 2 | p16: 10 DNA ISH: 15 RNA ISH: 7 | p16: 68 DNA ISH: 63 RNA ISH: 68 | p16: Sen: 82% (95% CI 70–91); Spe: 90% (95% CI 80–96) DNA ISH: Sen: 73% (95% CI 60–84); Spe: 97% (95% CI 90–100) RNA ISH: Sen: 88% (95% CI 76–95); Spe: 97% (95% CI 90–100) p16 and DNA ISH: Sen: 88% (95% CI 76–95); Spe: 97% (95% CI 90–100) p16 and RNA ISH: Sen: 95% (95% CI 85–99); Spe: 100% (95% CI 92–100) |
| Mendez-Pena et al. (2017) Boston, USA [29] | 2015–2016 | 57/26 | FFPE | RNA ISH DNA ISH p16 IHC, staining >50% | DNA PCR | RNA ISH: 26 DNA ISH: 23 p16: 24 | RNA ISH: 4 DNA ISH: 8 p16: 13 | RNA ISH: 0 DNA ISH: 3 p16: 1 | RNA ISH: 27 DNA ISH: 23 p16: 16 | RNA ISH: Sen: 100%; Spe: 87% DNA ISH: Sen: 88%; Spe: 74% p16: Sen: 96%; Spe: 55% |
| Wright et al. (2020) Tennessee, USA [30] | NR | 20/19 | FNA | DNA RT-PCR | p16 IHC, staining >70% | 19 | 0 | 0 | 1 | Sen: 100%; Spe: 100% |
| Menegaldo et al. (2020) Italy [31] | 2016–2019 | 29/16 | FNA | HPV16 and HPV18 E6 oncoproteins, lateral flow immunochromatographic strip test | p16 IHC, staining >70% combined with DNA PCR and/or E6 seropositivity | 15 | 0 | 1 | 11 | Sen: 94% (95% CI: 70–100); Spe: 100% (95% CI: 72–100) |
| Channir (2016) Denmark [32] | 2002–2016 | 71/71 (HPV- group: 47/7 with OSCC, 20 Warthin’s tumour, 20 branchial cleft cyst) | FNA | DNA PCR p16 IHC, staining <75% | DNA PCR | 68 | 0 | 3 | 47 | Sen: NR. Spe: 100% (95% CI 92.5–100.0) |
| Sivars et al. (2016) Sweden [33] | 2013–2016 | 16/13 | FNA | DNA multiplex assay | p16 IHC, staining >70% | 13 | 0 | 0 | 3 | Sen: 100%; Spe: 100% |
| Chernesky et al. (2018) Canada [34] | NR | 59/48 | Saliva and oral swabs (BOT and tonsillar area) pooled and FNA | (1) OncoE6 proteins–lateral flow strip (2) HPV E6/E7 mRNA assay (3) DNA PCR | p16 IHC, staining >70% | Oral sample: (1) 3 (2) 22 (3) 35 FNA: (1) 38 (2) 46 (3) 42 | Oral sample: (1) 0 (2) 0 (3) 1 FNA: (1) 1 (2) 1 (3) 2 | Oral sample: (1) 45 (2) 26 (3) 11 FNA: (1) 10 (2) 2 (3) 2 | Oral sample: (1) 11 (2) 11 (3) 10 FNA: (1) 10 (2) 10 (3) 9 | NR |
| Borena et al. (2020) Austria [35] | 2018–2020 | 50/23 | Cytology brush tests of tumour surface | E7 antigen test, ELISA | p16 IHC, staining >66% and DNA PCR | 14 | 9 | 9 | 18 | Sen: 60.9% (95% CI 38.5–80.3); Spe: 66.7% (95% CI 46–83.5) |
| Martin-Gomez et al. (2019) Florida, USA [36] | 2014–2017 | 171/157 | Oral rinse | DNA PCR | p16 IHC, staining >70% and DNA PCR | 119 | 7 | 38 | 7 | Sen: 75.8%; Spe: 50.0% |
| Fakhry et al. (2019) Ohio and Baltimore USA [37] | 2011–2016 | 217/187 | Oral rinse | DNA PCR | mRNA E6 or E7 or p16 IHC/combined with DNA ISH | 161 | 5 | 26 | 25 | NR |
| Qureishi et al. (2018) United Kingdom [38] | 2015–2016 | 46/36 | Oral rinse | DNA PCR | p16 IHC, staining >70% and DNA ISH. Positive if: p16+/no HPV DNA test, p16+/HPV DNA+ or p16- and HPV DNA+. | p16/HPV: 26 | p16/HPV: 1 | p16/HPV: 10 | p16/HPV: 9 | Oral rinse vs. p16: Sen: 73.5% (95% CI 55.6–87.1); Spe: 83.3% (95% CI 51.6–97.9). Oral rinse vs. DNA ISH: Sen: 66.7% (95% CI 43–85.4); Spe: 87.5% (95% CI 47.4–99.7). Oral rinse vs. p16/HPV: Sen: 72.2 (95% CI 54.8–85.8); Spe: 90 (95% CI 55.5–99.8) |
| Reder et al. (2020) Germany [39] | 2014–2017 | 48/28 | Plasma | E6 and E7 oncogenes RT-PCR | HPV16-DNA RT-PCR | 23 | 0 | 7 | 20 | Sen: 77%; Spe: 100% |
| Economopoulou et al. (2019) Ohio, USA [40] | NR | 22/14 | Blood (CtC) | HPV16 E6/E7 mRNA qPCR | p16 IHC, staining > 70% and HPV DNA qPCR | 3 | 0 | 11 (7 HPV16) | 8 | NR |
| Chera et al. (2019) North Carolina, USA [41] | 2016 –2018 | 103/103. 155 controls (55 healty controls and 60 non-HPV malignancies (not OPSCC)) | Plasma | DNA, ddPCR | p16 IHC, staining > 70% | 84 | Control: 3 | 19 | Control: 112 | Sen: 89%; Spe: 97% |
| Ren et al. (2019) China [42] | 2007–2017 | 783/611 | Plasma | HPV16 E6 antibody advanced multiplex analysis/ELISA | p16 IHC, staining >70% | 545 | 8 | 66 | 164 | Sen: 89% (95%CI 86–92); Spe: 95% (95%CI 91–98) |
| Damerla et al. New York, USA (2019) [43] | NR | 97/97. (HPV- group: 7 HPV- HNC and 20 healthy controls) | Plasma | HPV16 and HPV33 ddPCR | p16 IHC, staining >70% or DNA ISH, or RNA ISH | 90 | 0 | 7 | 27 | Sen: 92.8%; Spe: 100% |
| Hanna et al. (2018) Boston, USA [44] | 2017–2018 | 17/15 | Blood (Obtained at any time during treatment) | DNA ddPCR | p16 IHC, staining >70% and DNA ISH or PCR | 14 | 1 | 1 | 1 | Sen: 93.3% (95%CI 68.0–99.8); Spe: 50% (95%CI 1.3–98.7) |
| Kuhs et al. (2017) Pittsburgh, USA [45] | 2003–2013 | 112/87 | Serum | HPV16 E6 multiplex serology | p16 IHC, staining >70% and DNA ISH | 78 | 1 | 9 | 24 | Sen: 89.7% (95%CI, 81.3–95.2); Spe: 96.0% (95% CI, 79.6–99.9) |
| Holzinger et al. (2017) Germany and Italy [46] | NR | 120/66 | Serum | HPV16 E6 antibody ELISA | HPV16 DNA, RT-PCR | 63 | 1 | 3 | 53 | Sen: 96% (95%CI 88–98); Spe: 98% (95%CI 90–100) |
| Mazurek et al. (2016) Poland [47] | 2011–2013 | 51/29 | Plasma | HPV16 DNA, RT-PCR | HPV16 DNA qPCR | 21 | 0 | 8 | 22 | Sen: 72%; Spe: 100%. |
| Number of Studies Included in Meta-Analysis | References: | Sensitivity (95% CI) | Specificity (95% CI) | |
|---|---|---|---|---|
| RNA ISH | 5 | p16 IHC: 3 studies DNA PCR: 2 studies | 93.1 (87.4–96.4) | 91.9 (78.8–97.2) |
| DNA ISH | 4 | p16 IHC: 2 studies DNA PCR: 3 studies | 81.1 (71.9–87.8) | 94.9 (79.1–98.9) |
| DNA PCR | 5 | p16 IHC: 3 studies RNA: 2 studies | 90.4 (81.4–95.3) | 81.1 (71.9–87.8) |
| p16 IHC | 4 | RNA: 2 studies DNA PCR: 2 studies | 83.3 (69.0–91.8) | 93.5 (88.4–96.5) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jakobsen, K.K.; Carlander, A.-L.F.; Bendtsen, S.K.; Garset-Zamani, M.; Lynggaard, C.D.; Grønhøj, C.; von Buchwald, C. Diagnostic Accuracy of HPV Detection in Patients with Oropharyngeal Squamous Cell Carcinomas: A Systematic Review and Meta-Analysis. Viruses 2021, 13, 1692. https://doi.org/10.3390/v13091692
Jakobsen KK, Carlander A-LF, Bendtsen SK, Garset-Zamani M, Lynggaard CD, Grønhøj C, von Buchwald C. Diagnostic Accuracy of HPV Detection in Patients with Oropharyngeal Squamous Cell Carcinomas: A Systematic Review and Meta-Analysis. Viruses. 2021; 13(9):1692. https://doi.org/10.3390/v13091692
Chicago/Turabian StyleJakobsen, Kathrine Kronberg, Amanda-Louise Fenger Carlander, Simone Kloch Bendtsen, Martin Garset-Zamani, Charlotte Duch Lynggaard, Christian Grønhøj, and Christian von Buchwald. 2021. "Diagnostic Accuracy of HPV Detection in Patients with Oropharyngeal Squamous Cell Carcinomas: A Systematic Review and Meta-Analysis" Viruses 13, no. 9: 1692. https://doi.org/10.3390/v13091692