1. Introduction
SARS-CoV-2 spread globally, and in March 2021, the total number of infections in the world exceeded 123 million, with more than 2.7 million deaths [
1]. Given that COVID-19 poses a serious threat to public health and the economy around the world, an urgent need exists for a new effective drugs for the treatment and prophylaxis of SARS-CoV-2 infections. The SARS-CoV-2 replication inhibitor favipiravir (Avifavir
®) [
2,
3], together with Hydroxychloroquine, umifenovir, and lopinavir+ritonavir, were among the first drugs repurposed and recommended by the Russian Ministry of Health for the treatment of COVID-19 [
4].
Previously, we demonstrated the efficacy of Avifavir
® in the treatment of patients with moderate COVID-19 [
3]. However, taking into account the complex nature of the SARS-CoV-2 pathogenesis and multiorgan involvement, a combination of direct virus-acting and host-targeted drugs could be clinically beneficial for the therapy of COVID-19. One of the promising drug candidates for the combination therapy of COVID-19 is aprotinin, a natural protease inhibitor with a long history of clinical use since the 1960s, a good safety profile, and anti-inflammatory activity [
5,
6,
7]. Recently, it was demonstrated that aprotinin inhibits transmembrane serine protease 2 (TMPRSS2), a host cell protease responsible for the cleavage and activation of the spike protein of SARS-CoV-2 [
8,
9], and downregulates cellular proteases during replication cycles [
10]. Thus, in addition to an anti-inflammatory effect, it is suggested that aprotinin can prevent SARS-CoV-2 penetration into susceptible cells and inhibits its replication. Our preliminary case series demonstrated a good potential of aprotinin for prevention [
11] and as a part of combination therapy for the treatment [
12] of COVID-19.
Therefore, we evaluated the efficacy of aprotinin in combination with drugs recommended by the Russian Ministry of Health for the treatment of COVID-19: HCQ and Avifavir®. Here, we report the results of a pilot noncomparative clinical study of the efficacy and safety of a combination therapy of aprotinin with Avifavir® or HCQ for moderate COVID-19 patients.
2. Materials and Methods
2.1. Ethics
This study was conducted at the Smolensk Clinical Hospital, Russia from June (11 June 2020—1st patient was included) to August 2020. The COVID-19-aprotinin-01 study protocol and the amendment to the protocol were approved by the Independent Ethics Committee of Smolensk Clinical Hospital (protocols NO. 38 from 2 June and 2 July 2020, respectively) and registered at the U.S. National Library of Medicine (NCT04527133). All patients participated in this study provided their written informed consent. The informed consent form was approved by a local ethics committee (Independent Ethics Committee of Smolensk Clinical Hospital #1) before the study was started at the research site.
2.2. Study Design and Patients
This was an open noncomparative study of the safety and efficacy of aprotinin on the patients hospitalized with COVID-19. Characteristics of the patients and exclusion criteria are presented in the
Appendix A.
Participants were divided into 3 cohorts of 10 patients in each: cohort 1—combination of aprotinin (IV) (Gordox® 1,000,000 KIU daily, 3 days), HCQ (400/200 mg, twice a day, 5 to 6 days), and standard of care (SOC); cohort 2—combinations of inhaled aprotinin (Gordox® 625 KIU four times per day, 5 days), HCQ (400/200 mg, twice a day, 5 to 6 days), and SOC; and cohort 3—combinations of aprotinin (IV) (Gordox® 1,000,000 KIU daily, 5 days), oral Avifavir® (2000 mg twice on the first day, then 800 mg twice a day, 10 days), and SOC. Patients in cohorts 1–3 received thromboembolic prophylaxis with an anticoagulant enoxaparin (40 mg, once a day, 14 to 15 days). Patients with a score of 4 on the WHO-OSCI had supportive oxygen therapy via nasal cannula or face mask. None of the patients had invasive or NIV mechanical ventilation at the baseline.
2.3. Efficacy Endpoints
The primary efficacy endpoint of the study was time to normalization of the following parameters: elimination of SARS-CoV-2 (defined as two negative results from a RT-PCR assay with at least a 24-h interval), CRP, and D-dimer concentrations.
Key secondary clinical endpoints were: time to body temperature normalization (<37 °C) and changes from baseline of the laboratory parameters during 14 days, which included hematology: CRP values and coagulogram; changes from the baseline of lung parenchyma on a tomography chest CT scan on days 7 and 14; frequency of the clinical status improvement by 2 scores in accordance with the WHO Ordinal scale of clinical improvement (WHO-OSCI) or discharge from the hospital before day 14; frequency of transfer to the ICU, frequency of the NIV, and frequency of the invasive ventilation; mortality rate; and frequency of adverse events and serious adverse events of various severities according to subjective complaints, physical examination, vital signs, laboratory tests, and electrocardiogram.
2.4. Procedures
Clinical manifestations, including persistent fever >38 °C, respiratory rate, oxygen saturation, and oxygen therapy requirement, and biological parameters, including CRP, D-dimer, neutrophil, lymphocyte and platelet counts, INR, prothrombin, and fibrinogen, were recorded at the baseline and at discharge from the hospital. The median time to improve the clinical state by 2 points was determined according to the WHO-OSCI. Chest CT was done with a single inspiratory phase with patients in the supine position. Radiologists classified the CT scan as typical, equivocal, or negative for COVID-19 and described the main CT features: ground glass opacity, crazy-paving pattern, and consolidation. A semi-quantitative scoring system was used to estimate the pulmonary involvement of the observed abnormalities based on the area involved: mild (<25%), moderate (25–50%), severe (51–75%), or diffuse (>75%) [
13].
2.5. Statistical Analysis
The sample size was based on the exact single-stage Phase II assessment at one-sided α = 0.05 and 80% power [
14]. Continuous variables with a normal distribution were expressed as the mean (SD) and with a non-normal distribution as the median with interquartile range (IQR) and compared using a 2-tailed, paired
t-test for parametric data and Wilcoxon rank-sum test for nonparametric data. The categorical variables were presented as the absolute and relative (in percentage) frequencies and compared using a chi-square test. The efficacy endpoints (time to viral clearance, time to CRP normalization (≤10 mg/L), time to D-dimer normalization (<253 ng/mL), time to temperature normalization (<37 °C), and time to improvement in clinical status) were estimated using Kaplan–Meier curves. For groups, a comparison log-rank test was used (
p-value ˂ 0.05 was considered significant).
3. Results
The cohorts were generally comparable, while some differences existed; the proportions of males and females were higher in cohort 3 as compared to cohorts 1 and 2, and some of the patients in cohort 1 had a score of 3 (according to the WHO-OSCI), while all the patients in cohorts 2 and 3 had a score of 4 (requiring oxygen therapy;
Appendix A).
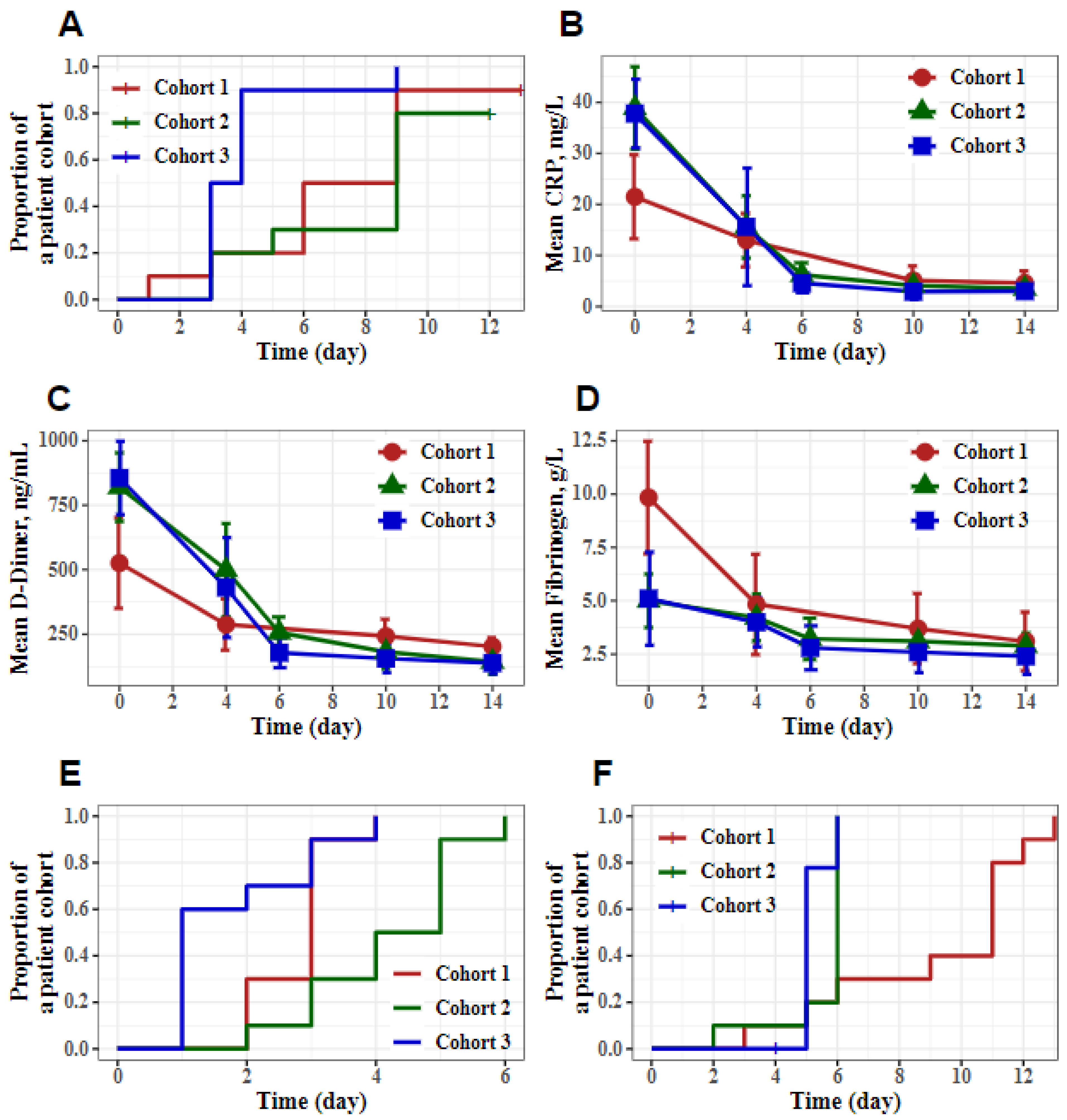
An analysis of the primary and secondary efficacy points revealed that combination therapy with aprotinin (IV) + Avifavir in association with SOC was beneficial for COVID-19 patients (
Table 1). In particular, the median time to SARS-CoV-2 elimination was 3.5 (IQR 3–4) days for cohort 3 and 7.5 (IQR 6–9) and 9 (IQR 5–9) days for cohorts 1 and 2, respectively (the difference was significant,
p = 0.019 and
p = 0.006 as compared to patients from cohorts 3,
Figure 1A). The median time to CRP normalization was 3.5 (IQR 3–5) days for cohort 3 and 6 (IQR 6–6) and 4 (IQR 3–5) days for cohorts 1 and 2, respectively. The difference in this parameter between cohorts 1 and 3 was significant (
p < 0.001,
Figure 1B).
The efficacy of the aprotinin combinations on the normalization of thrombosis markers (D-dimer and fibrinogen) in the patients’ blood are presented in
Figure 1C,D. The increased D-dimer levels quickly returned to normal values with a median of 4.5 (IQR 3–6), 9 (IQR 5–9), and 5 (IQR 4–5) days for cohorts 1, 2, and 3, respectively (
Figure 1C). The difference in this parameter between cohorts 2 and 3 was significant (
p = 0.002). The elevated baseline fibrinogen levels returned to normal values on day 4, presumably as a result of the therapy (
Figure 1D).
The dynamics of the INR and prothrombin changes were used to monitor blood-thinning anticoagulants and to check blood-clotting problems. Both the INR and Quick prothrombin tests were defined as normal at admission and discharge of the patients from the hospital. The patients presented normal values for neutrophils and leukocytes when admitted to the hospital and when discharged from the hospital after the aprotinin combination therapy.
The median time to normalization of the body temperatures of the patients in cohorts 1–3 was 3 (IQR 2–3), 4.5 (IQR 3–5), and 1 (IQR 1–3) days, respectively. The difference in this parameter between cohorts 2 and 3 was significant (
p < 0.001). The median time to improve the clinical state by two points was 11 (IQR 6–11), 6 (IQR 6–6), and 5 (IQR 5–5) days for cohorts 1–3, respectively (
Figure 1E,F). This parameter differed significantly between cohorts 1 and 2 and from that in cohort 3 (
p = 0.004 and
p = 0.036, respectively).
Importantly, none of the participants in cohorts 1–3 of the administered aprotinin combinations were transferred to the ICU for ALV or NIV. All the patients in cohorts 1–3 were discharged from the hospital, and no adverse events were recorded.
For the retrospective comparison, our results from two historical cohorts with COVID-19 patients treated with Avifavir
® + SOC (
n = 40, cohort 4) or HCQ + SOC (
n = 20, cohort 5) were added to
Table 1 (the study was conducted in six Russian hospitals from 27 April to 4 July 2020) [
3].
4. Discussion
In this study, we evaluated the efficacy of aprotinin in combination with HCQ and Avifavir
® in patients admitted to the hospital due to COVID-19-associated pneumonia. HCQ and Avifavir
® are recommended by the Russian Ministry of Health for the treatment of the new coronavirus infection COVID-19 [
4]. Retrospectively, we compared these results with our data from the Phase II/III clinical trials of Avifavir
® among hospitalized patients with moderate COVID-19 pneumonia [
3]. It is important to mention that, while HCQ was recommended for the therapy of COVID-19 patients in Russia at the time when this study was conducted, later results demonstrated that it does not improve the clinical status of the patients hospitalized with COVIV-19 compared to the standard care [
15,
16]. It allowed us to consider HCQ+SOC as SOC and helped us to better interpret the effects of aprotinin by comparing the median time to SARS-CoV-2 elimination in cohorts 1 and 2 vs. 5; we could see that, at the studied doses, aprotinin did not affect the replication of SARS-CoV-2, but it significantly reduced the level of CRP (comparing the median time to CRP normalization in cohorts 1 and 2 vs. 5 and cohort 3 vs. 4), which was in agreement with its known anti-inflammatory activity [
17].
As we hypothesized, the most significant results were demonstrated with a combination of aprotinin and Avifavir
®. It reduced the time to normalization of the CRP and D-dimer concentrations in the patients’ blood and overall improved the clinical outcome and the median time to SARS-CoV-2 elimination, and the body temperature normalization was shorter compared to cohorts 1 and 2; the elevated fibrinogen levels returned to normal concentrations on day 4. As it was previously demonstrated, Avifavir
® itself enabled SARS-CoV-2 viral clearance in 62.5% of patients within 4 days of therapy but had little effect on the concentration of CRP, which is a marker of the severity of COVID-19 [
3]. Taking into account the results from our historical cohorts, we can hypothesize that the better median time to SARS-CoV-2 elimination in cohort 3 was due to the effect of Avifavir
®, but the improved recovery from the infection was most likely due to the actions of aprotinin.
Despite the limitations of this pilot clinical study, such as the low number of patients per cohort and absence of prospective cohorts with aprotinin+SOC, Avifavir®+SOC, and SOC, this clinical study revealed, for the first time, the potency of aprotinin combination therapy for patients hospitalized with moderate COVID-19 pneumonia and requiring oxygen therapy. Significantly, none of the patients in cohorts 1–3 treated with the aprotinin combinations were transferred to the ICU for ALV or NIV, no adverse events were recorded, and all the patients were discharged from the hospital.
Taken together, these results can be considered as a promising first step in the evaluation of aprotinin and open the possibility for the initiation of a multicenter, randomized trial of combination aprotinin therapy in patients with moderate and severe COVID-19.
5. Conclusions
Our findings demonstrates that therapy with a combination of aprotinin with Avifavir® showed promising results in preventing disease progression in patients hospitalized with COVID-19-associated pneumonia and requiring oxygen therapy, as none of the patients were transferred to the ICU for mechanical ventilation or noninvasive ventilation, and their hospital stays were shortened.
Author Contributions
O.S.R. and E.N.S. were the principal investigators responsible for the recruitment of patients, study treatment, and data collection in compliance with the Protocol. A.A.I., V.G.L., E.V.Y., M.A.T. and A.V.I. conceived this project, suggested the variants of its organization, and controlled the implementation. V.N.A., N.P.S., S.V.P., and A.N.E. developed the clinical trial protocol and worked on the statistical aspects of the study and the analysis of the results. E.A.M. and N.V.K. organized the clinical trial and collection of the data. R.N.K. developed the preclinical study design, organized its implementation, did the literature search, and edited the manuscript. D.V.K. developed the technology and coordinated the production of the substance. A.V.I. carried out the scientific management of the project and wrote and edited the manuscript. The manuscript was written with contributions from all the authors. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The COVID-19-aprotinin-01 study protocol and the amendment to the protocol were approved by the Independent Ethics Committee of Smolensk Clinical Hospital #1 (protocols No. 38 from 2 June and 2 July 2020, respectively).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study. An informed consent form was used to obtain patient’s informed consent for participation in the study prior to any other protocol procedures being implemented. The informed consent form was approved by a local ethics committee (Independent Ethics Committee of Smolensk Clinical Hospital #1) before the study was started at the research site.
Data Availability Statement
The datasets used and/or analyzed during the current study are available from the corresponding author upon reasonable request.
Conflicts of Interest
AAI, NPS, and AVI are the founders of ChemDiv. AAI, AVI, NPS, and DVK reporting patent RU 2731932 (09.09.2020). The other authors declare no competing interests.
Appendix A
Table A1.
Demographic and baseline characteristics of the patients.
Table A1.
Demographic and baseline characteristics of the patients.
| Characteristic | Cohort 1 | Cohort 2 | Cohort 3 |
|---|
| Age |
| Years, mean (SD) | 44.9 (11.2) | 48.2 (10.4) | 46.7 (10.6) |
| Age category, no. (%) |
| 18–44 | 4 (40) | 4 (40) | 4 (40) |
| 45–59 | 6 (60) | 3 (30) | 5 (50) |
| ≥60 | 0 | 3 (30) | 1 (10) |
| Male, no. (%) | 3 (30) | 1 (10) | 8 (80) |
| Female, no. (%) | 7 (70) | 9 (90) | 2 (20) |
| Body mass, kg (SD) | 74.3 (4.7) | 76.7 (6.4) | 80.7 (6) |
| Body-mass index, kg/m2 (SD) | 25.9 (1.7) | 26.9 (2.1) | 26.4 (1.5) |
| Positive swab by RT- PCR, % | 100 | 100 | 100 |
| Duration of illness, days (SD) | 3.4 (1.1) | 2.7 (0.7) | 3.4 (0.8) |
| ≤7 days, no. (%) | 10 (100) | 10 (100) | 10 (100) |
| >7 days, no. (%) | 0 | 0 | 0 |
| WHO Ordinal scale of clinical improvement (WHO-OSCI, score 0 to 8) |
| Score 3, no. (%) | 4 (40) | 0 | 0 |
| Score 4, no. (%) | 6 (60) | 10 (100) | 10 (100) |
| Oxygen saturation, % (SD) | 96.7 (1.1) | 94.3 (0.7) | 95.0 (0.9) |
| SpO2 ≥ 95%, no. (%) | 10 (100) | 6 (60) | 6 (60) |
| SpO2 < 95%, no. (%) | 0 | 4 (40) | 4 (40) |
| Fever, °C (SD) | 38.3 (0.1) | 38.3 (0.3) | 38.5 (0.4) |
| <37 °C, no. (%) | 0 | 0 | 0 |
| 37–38 °C, no. (%) | 0 | 1 (10) | 1 (10) |
| >38 °C, no. (%) | 10 (100) | 9 (90) | 9 (90) |
Respiratory rate, min (SD)
(normal range 16–20 min) | 21.4 (1.6) | 22.6 (0.7) | 21.8 (1) |
| ≤22 min, no. (%) | 8 (80) | 5 (50) | 7 (70) |
| >22 min, no (%) | 2 (20) | 5 (50) | 3 (30) |
CRP, mg/L (SD)
(normal < 5 mg/L) | 21.5 (8.2) | 38.9 (8.1) | 37.8 (6.7) |
D-dimer, ng/mL (SD)
(normal < 243 ng/mL) | 525.4 (175.7) | 820.1 (133.1) | 855.5 (142.5) |
| Neutrophil count × 109 cells per L, no. (SD) (normal range 1.8–6.5) | 3.0 (0.5) | 2.2 (0.4) | 2.7 (1.0) |
| Leukocyte count × 109 cells per L, no. (SD) (normal range 3.2–10.6) | 4.4 (0.7) | 3.4 (0.4) | 3.9 (1.5) |
INR *, no. (SD)
(normal range 0.85–1.15) | 1.0 (0.2) | 1.0 (0.1) | 1.1 (0.1) |
Prothrombin, % (SD)
(quick test, normal range 95–105%) | 103.3 (8.1) | 78.5 (5.7) | 78.2 (8.7) |
Fibrinogen, g/L (SD)
(normal range 2–4) | 9.8 (2.6) | 5.0 (1.2) | 5.1 (2.2) |
| Involvement of the lung parenchyma, % (SD) | 28.3 (7.6) | 20.6 (6.8) | 21.8 (6.1) |
| Chest CT 1 (< 25% abnormality), no. (%) | 4 (40) | 3 (30) | 6 (60) |
| Chest CT 2 (25% –50% abnormality), no. (%) | 6 (60) | 7 (70) | 4 (40) |
Exclusion criteria were the following: refusal of the patient to participate; patients with respiratory rates >35 per min that did not decrease after their body temperature dropped to normal or sub-febrile values; blood oxygen saturation ≤93% at rest; partial pressure of oxygen in arterial blood (SpO2) <60 mm Hg; oxygenation index, SpO2 per fraction of inspired oxygen (SpO2/FiO2) ≤200 mm Hg; septic shock; chronic liver and kidneys diseases in terminal stage; refusal of other organs requiring control and treatment in the ICU; patients with HIV; using aprotinin within 6 months prior to screening; hypersensitivity to any of the components of the study therapy; patients participating in other clinical trials or taking other investigational drugs within 28 days of screening; pregnant or lactating women or women planning a pregnancy during the clinical study; women capable of childbirth who do not use adequate methods of contraception; patients unable to read or write or unwilling to understand and follow research protocol procedures; noncompliance with the regimen of taking medications or performing procedures, which, in the opinion of the investigator, may affect the results of the study or the safety of the patient and prevented the patient’s further participation in the study; and patients with any other comorbid medical or serious mental health conditions that rendered them ineligible for participation in clinical research, limited their ability to obtain informed consent, or affected their ability to participate in the research.
References
- COVID-19 Dashboard by the Center for Systems Science and Engineering (CSSE) at Johns Hopkins University; 22 March 2021, COVID-19 Map—Johns Hopkins Coronavirus Resource Center (jhu.edu); Available online: https://publichealthupdate.com/jhu/ (accessed on 12 June 2021).
- Scavone, C.; Brusco, S.; Bertini, M.; Sportiello, L.; Rafaniello, C.; Zoccoli, A.; Berrino, L.; Racagni, G.; Rossi, F.; Capuano, A. Current pharmacological treatments for COVID-19: What’s next? Br. J. Pharmacol. 2020, 177, 4813–4824. [Google Scholar] [CrossRef] [PubMed]
- Ivashchenko, A.A.; Dmitriev, K.A.; Vostokova, N.V.; Azarova, V.N.; Blinow, A.A.; Egorova, A.N.; Gordeev, I.G.; Ilin, A.P.; Karapetian, R.N.; Kravchenko, D.V.; et al. AVIFAVIR for Treatment of Patients with Moderate Coronavirus Disease 2019 (COVID-19): Interim Results of a Phase II/III Multicenter Randomized Clinical Trial. Clin. Infect. Dis. 2020, 9, 1176. [Google Scholar] [CrossRef] [PubMed]
- Ministry of Health of the Russian Federation. Temporary methodological recommendations. In Prevention, Diagnostics and Treatment of New Coronavirus Infection COVID-19; Version 7 (Russian language); June 3d 2020, 03062020_MR_COVID-19_v7.pdf (rosminzdrav.ru). Available online: https://journal.pulmonology.ru/pulm/article/view/1249?locale=en_US (accessed on 12 June 2021).
- Scheule, A.M.; Beierlein, W.; Wendel, H.P.; Jurmann, M.J.; Eckstein, F.S.; Ziemer, G. Aprotinin in fibrin tissue adhesives induces specific antibody re-sponse and increases antibody response of high-dose intravenous application. J. Thorac. Cardiovasc. Surg. 1999, 118, 348–353. [Google Scholar] [CrossRef] [Green Version]
- Ascenzi, P.; Bocedi, A.; Bolognesi, M.; Spallarossa, A.; Coletta, M.; Cristofaro, R.D.; Menegatti, E. The bovine basic pancreatic trypsin inhibitor (Kunitz inhibitor): A milestone protein. Curr Protein Pept Sci 2003, 4, 231–251. [Google Scholar] [CrossRef]
- Engles, L. Review and application of serine protease inhibition in coronary artery bypass graft surgery Am. J. Health-Syst. Pharm. 2005, 62, S9–S14. [Google Scholar] [CrossRef] [PubMed]
- Solun, B.; Shoenfeld, Y. Inhibition of metalloproteinases in therapy for severe lung injury due to COVID-19. Med. Drug Discov. 2020, 7, 100052. [Google Scholar] [CrossRef]
- Hoffmann, M.; Kleine-Weber, H.; Schroeder, S.; Krüger, N.; Herrler, T.; Erichsen, S.; Schiergens, T.S.; Herrler, G.; Wu, N.; Nitsche, A.; et al. SARS-CoV-2 Cell Entry Depends on ACE2 and TMPRSS2 and Is Blocked by a Clinically Proven Protease Inhibitor. Cell 2020, 18, 271–280. [Google Scholar] [CrossRef]
- Bojkova, D.; Bechtel, M.; McLaughlin, K.-M.; McGreig, J.E.; Klann, K.; Bellinghausen, C.; Rohde, G.; Jonigk, D.; Braubach, P.; Ciesek, S.; et al. Aprotinin Inhibitors SARS-CoV-2 Replication. Cells 2020, 9, 2377. [Google Scholar] [CrossRef]
- Ivashchenko, A.A.; Svistunov, A.A.; Khorobryh, T.V.; Loginov, V.G.; Karapetian, R.N.; Mishchenko, N.P.; Poyarkov, S.V.; Volgin, M.V.; Yakubova, E.V.; Topr, M.P.; et al. Aprotinin—A New Drug Candidate for The Prevention of SARS-CoV-2 (COVID-19). COVID19-Prepr. 2020. Aprotinin—A New Drug Candidate for The Prevention of SARS-CoV-2 (COVID-19)—REPRINTS.RU (microbe.ru). Available online: https://covid19-preprints.microbe.ru/article/117 (accessed on 12 June 2021).
- Ivashchenko, A.A.; Svistunov, A.A.; Khorobryh, T.V.; Loginov, V.G.; Karapetian, R.N.; Mishchenko, N.P.; Poyarkov, S.V.; Volgin, M.V.; Yakubova, E.V.; Topr, M.P.; et al. Aprotinin—A New Multi-Target Drug Candidate or “Magic Shotgun” for the Therapy of COVID-19. COVID19-Prepr. 2020. Aprotinin—A new multi-target drug candidate or “magic shotgun” for the therapy of COVID-19—REPRINTS.RU (microbe.ru). Available online: https://covid19-preprints.microbe.ru/article/125 (accessed on 12 June 2021).
- Chang, Y.C.; Yu, C.J.; Chang, S.C.; Galvin, J.R.; Liu, H.M.; Hsiao, C.H.; Yang, P.C. Pulmonary sequelae in convalescent patients after severe acute respiratory syndrome: Evaluation with thin-section CT. Radiology 2005, 236, 1067–1075. [Google Scholar] [CrossRef] [PubMed]
- A’Hern, R.P. Sample size tables for exact single-stage phase II designs. Stat. Med. 2001, 20, 859–866. [Google Scholar] [CrossRef]
- Cavalcanti, A.B.; Zampieri, F.G.; Rosa, R.G.; Azevedo, L.C.; Veiga, V.C.; Avezum, A.; Damiani, L.P.; Marcadenti, A.; Kawano-Dourado, L.; Lisboa, T.; et al. Hydroxychloroquine with or without Azithromycin in Mild-to-Moderate Covid-19. N. Engl. J. Med. 2020, 383, 2041–2052. [Google Scholar] [CrossRef]
- Self, W.H.; Semler, M.W.; Leither, L.M.; Casey, J.D.; Angus, D.C.; Brower, R.G.; Chang, S.Y.; Collins, S.P.; Eppensteiner, J.C.; Filbin, M.R.; et al. Effect of Hydroxychloroquine on Clinical Status at 14 Days in Hospitalized Patients With COVID-19. JAMA 2020, 324, 2165–2176. [Google Scholar] [CrossRef] [PubMed]
- Mojcik, C.F.; Levy, J.H. Aprotinin and the systemic inflammatory response after cardiopulmonary bypass. Ann. Thorac. Surg. 2001, 71, 745–754. [Google Scholar] [CrossRef]
| Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).


 ,
, 
{kind=link}
