
Seroprevalence of SARS-CoV-2, Symptom Profiles and Sero-Neutralization in a Suburban Area, France

 , ,
, ,
Abstract
:1. Background
2. Materials and Methods
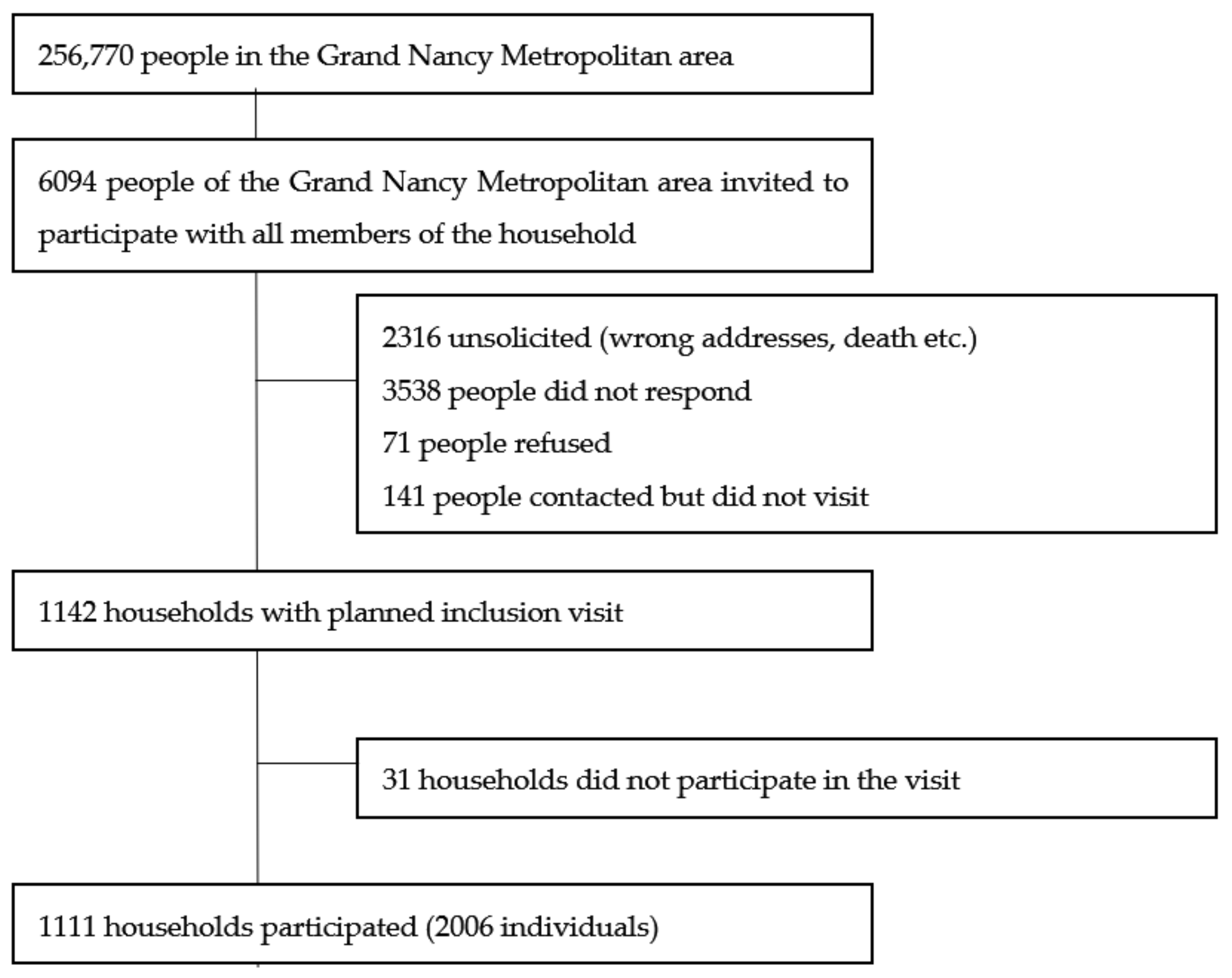
2.1. Sampling
- –
- socio-demographic characteristics: age, sex, socio-professional category, education level;
- –
- Evaluation of Deprivation and Inequalities in Health Examination Centres (EPICES) questionnaire (for adults) [22], a composite index commonly used to measure individual deprivation. A score is calculated on the basis of 11 weighted questions related to material and social deprivation, ranging from 0 to 100 (>30 associated with social deprivation).
- –
- health characteristics: body mass index, smoking status, influenza vaccination, health problems, pregnancy;
- –
- potential contacts with a person with COVID-19: perception of infection with the virus, relatives infected;
- –
- symptoms experienced since mid-February: fever, cough, runny nose, chest pain, anosmia or ageusia, sore throat, muscle pain, aches, fatigue, headaches, skin rashes, appetite loss, shortness of breath, diarrhea, loss of balance, abdominal pain, nausea, and irritated eyes. According to the European Center for Disease Prevention and Control [23], at least one symptom among fever, cough, anosmia or ageusia, and shortness of breath indicates COVID-19.
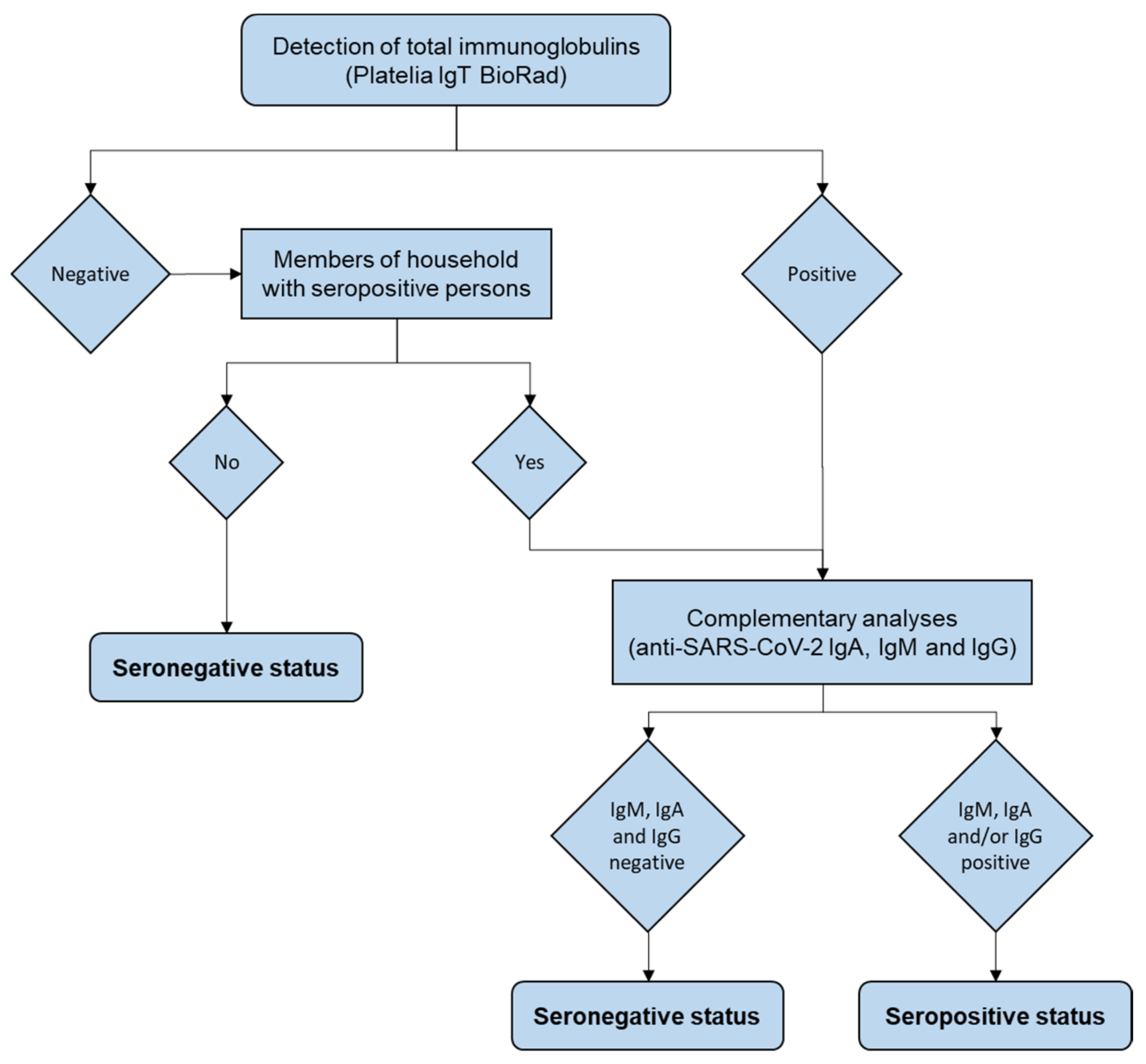
2.2. Serology
2.3. Microneutralization Assay
2.4. Statistical Analysis
3. Results
3.1. Sample Description
3.2. General Seroprevalence
3.3. Seroprevalence by Age and Socioeconomic Status
3.4. Seroprevalence with Other Factors
3.5. Symptoms
3.6. Seroneutralization Assay
3.7. Consequences of Low Anti-SARS-CoV-2 Prevalence on the Epidemic Evolution
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
- –
- the Département Méthodologie, Promotion, Investigation, Mehdi SIAGHY, Nathalie THILLY, Marjorie STARCK and Louise GEND for their support.
- –
- the Centre d’Investigation Clinique Epidémiologie Clinique members for their contribution to organization, blood samples and data collection, data entry and management, activity reporting, and logistic with Sylvie KLEIN Marie SPONGA, Jean-Marc VIRION, Laurence EMPORTE, Sandrine GRANDCLERE, Emilie JACQUOT, Sylvie RONCHETTI Agathe BOCHNAKIAN, Heloise BRIANCON, Alfousseyni COLY, Marie Rita LETOURNEUR, Sandrine GERSET, Nathalie DUMONT, Nathalie PIERREZ, Nina THIAVILLE, Sandrine TYRODE, Véronique VOGEL, Christelle DUJON, Nicole KOEBEL, Philippe MELCHIOR and Samia MAHMOUDI.
- –
- the Centre d’Investigation Clinique Pluridisciplinaire members for their contribution to organization and realization of blood samples: Patrick ROSSIGNOL, Nicolas GIRERD, Edith DAUCHY, Helene COYARD, Evelyne MICOR, Agnes PEZZI, Lydie POINSIGNON and Jonathan UDOT.
- –
- the Unité d’Investigation Clinique for their contribution to organization and realization of blood samples: Nathalie THILLY, Valerie BOUAZIZ and Marie Alexandra PAQUOT et Nelly FRANCOIS.
- –
- the Hôpital d’Enfant, Cyril SCHWEITZER, Valerie RATAJCZAK, Herve LEROY and the pediatric nurses for the realization of child blood samples.
- –
- the technical and management teams of the Laboratories for the realization of SARS-CoV-2 serology and samples management, Mihayl VARBANOV and Stéphanie PHILIPPOT of the L2CM Laboratory (Nancy) for the cell model of culture of SARS-CoV-2 and Jonathan MAYER (medical student) for his contribution to the performance of sero-neutralization analyzes.
- –
- Direction des Soins, in particular Mireille GAUDRON, Sandrine HAYO VILLENEUVE, Sandrine JORAY et Julie THOUVENIN-GALANTI.
- –
- Centre de Ressources Biologiques (CRB) Lorrain of Nancy BB-0033-00035 for managing patient samples: Catherine MALAPLATE and Sandra LOMAZZI.
- –
- Communication members Laurence VERGER and David KOZON.
- –
- the Direction des Services Informatiques in particularly Lionel SCHWEITZER.
Conflicts of Interest
References
- World Health Organization. Population-Based Age-Stratified Seroepidemiological Investigation Protocol for Coronavirus 2019 (COVID-19) Infection. 26 May 2020. Available online: https://apps.who.int/iris/handle/10665/332188 (accessed on 28 May 2020).
- Younas, A.; Waheed, S.; Khawaja, S.; Imam, M.; Borhany, M.; Shamsi, T. Seroprevalence of SARS-CoV-2 antibodies among healthy blood donors in Karachi, Pakistan. Transfus. Apher. Sci. 2020, 59, 102923. [Google Scholar] [CrossRef] [PubMed]
- McLaughlin, C.C.; Doll, M.K.; Morrison, K.T.; McLaughlin, W.L.; O’Connor, T.; Sholukh, A.M.; Bossard, E.L.; Phasouk, K.; Ford, E.S.; Diem, K.; et al. High Community SARS-CoV-2 Antibody Seroprevalence in a Ski Resort Community, Blaine County, Idaho, US. Preliminary Results. medRxiv 2020. [Google Scholar] [CrossRef]
- Percivalle, E.; Cambiè, G.; Cassaniti, I.; Nepita, E.V.; Maserati, R.; Ferrari, A.; di Martino, R.; Isernia, P.; Mojoli, F.; Bruno, R.; et al. Prevalence of SARS-CoV-2 specific neutralising antibodies in blood donors from the Lodi Red Zone in Lombardy, Italy, as at 06 April 2020. Eurosurveillance 2020, 25, 2001031. [Google Scholar] [CrossRef] [PubMed]
- Pagani, G.; Conti, F.; Giacomelli, A.; Bernacchia, D.; Rondanin, R.; Prina, A.; Scolari, V.; Gandolfi, C.E.; Castaldi, S.; Marano, G.; et al. Seroprevalence of SARS-CoV-2 significantly varies with age: Preliminary results from a mass population screening. J. Infect. 2020, 81, e10. [Google Scholar] [CrossRef] [PubMed]
- Naranbhai, V.; Chang, C.C.; Beltran, W.F.G.; Miller, T.E.; Astudillo, M.G.; Villalba, J.A.; Yang, D.; Gelfand, J.; Bernstein, B.E.; Feldman, J.; et al. High Seroprevalence of Anti-SARS-CoV-2 Antibodies in Chelsea, Massachusetts. J. Infect. Dis. 2020, 22, 1955–1959. [Google Scholar] [CrossRef] [PubMed]
- Borges, L.P.; Martins, A.F.; de Melo, M.S.; de Oliveira, M.G.B.; Neto, J.M.d.; Dósea, M.B.; Cabral, B.C.M.; Menezes, R.F.; Santos, A.A.; Matos, I.L.S.; et al. Seroprevalence of SARS-CoV-2 IgM and IgG antibodies in an asymptomatic population in Sergipe, Brazil. Rev. Panam. Salud Publica 2020, 4, e108. [Google Scholar] [CrossRef] [PubMed]
- Kawachi, I. COVID-19 and the ‘rediscovery’ of health inequities. Int. J. Epidemiol. 2020, 49, 1415–1418. [Google Scholar] [CrossRef] [PubMed]
- Hallal, P.C.; Hartwig, F.P.; Horta, B.L.; Silveira, M.F.; Struchiner, P.J.; Vidaletti, L.P.; Neumann, N.A.; Pellanda, P.C.; Dellagostin, P.A.; Burattini, M.N.; et al. SARS-CoV-2 antibody prevalence in Brazil: Results from two successive nationwide serological household surveys. Lancet Glob. Health 2020, 8, e1390–e1398. [Google Scholar] [CrossRef]
- Liu, W.; Liu, L.; Kou, G.; Zheng, Y.; Ding, Y.; Ni, W.; Wang, Q.; Tan, L.; Wu, W.; Tang, S.; et al. Evaluation of nucleocapsid and spike protein-based enzyme-linked immunosorbent assays for detecting antibodies against SARS-CoV-2. J. Clin. Microbiol. 2020, 58. [Google Scholar] [CrossRef] [Green Version]
- Flehmig, B.; Schindler, M.; Ruetalo, N.; Businger, R.; Bayer, M.; Haage, A.; Kirchner, T.; Klingel, K.; Normann, A.; Pridzun, L.; et al. Persisting Neutralizing Activity to SARS-CoV-2 over Months in Sera of COVID-19 Patients. Viruses 2020, 12, 1357. [Google Scholar] [CrossRef]
- Stefanelli, P.; Bella, A.; Fedele, G.; Pancheri, S.; Leone, P.; Vacca, P.; Neri, A.; Carannante, A.; Fazio, C.; Benedetti, E.; et al. Prevalence of SARS-CoV-2 IgG antibodies in an area of northeastern Italy with a high incidence of COVID-19 cases: A population-based study. Clin. Microbiol Infect. 2021, 27, e1–e7. [Google Scholar] [CrossRef]
- Zost, S.J.; Gilchuk, P.; Chen, R.E.; Case, J.B.; Reidy, J.X.; Trivette, A.; Nargi, R.S.; Sutton, R.E.; Suryadevara, N.; Chen, E.C.; et al. Rapid isolation and profiling of a diverse panel of human monoclonal antibodies targeting the SARS-CoV-2 spike protein. bioRxiv 2020, 26, 1422–1427. [Google Scholar]
- Dogan, M.; Kozhaya, L.; Placek, L.; Gunter, C.L.; Yigit, M.; Hardy, R.; Plassmeyer, M.; Coatney, P.; Lillard, K.; Bukhari, Z.; et al. Novel SARS-CoV-2 specific antibody and neutralization assays reveal wide range of humoral immune response during COVID-19. medRxiv 2020. [Google Scholar] [CrossRef]
- Mazzini, L.; Martinuzzi, D.; Hyseni, I.; Mazzini, L.; Martinuzzi, D.; Hyseni, I.; Benincasa, L.; Molesti, E.; Casa, E.; Lapini, G.; et al. Comparative analyses of SARS-CoV-2 binding (IgG, IgM, IgA) and neutralizing antibodies from human serum samples. J. Immunol. Methods 2021, 489, 112937. [Google Scholar] [CrossRef]
- Klingler, J.; Weiss, S.; Itri, V.; Liu, X.; Oguntuyo, K.Y.; Stevens, C.; Ikegame, S.; Hung, C.-T.; Enyindah-Asonye, G.; Amanat, F.; et al. Role of IgM and IgA Antibodies in the Neutralization of SARS-CoV-2. medRxiv 2020. [Google Scholar] [CrossRef]
- Sholukh, A.M.; Fiore-Gartland, A.; Ford, E.S.; Hou, Y.J.; Tse, V.; Kaiser, H.; Park, A.; Lempp, F.A.; Germain, R.S.; Bossard, E.; et al. Evaluation of SARS-CoV-2 neutralization assays for antibody monitoring in natural infection and vaccine trials. medRxiv 2020. [Google Scholar] [CrossRef]
- Stoecklin, S.B.; Rolland, P.; Silue, Y.; Mailles, A.; Campese, C.; Simondon, A.; Mechain, M.; Meurice, L.; Nguyen, M.; Bassi, C.; et al. First cases of coronavirus disease 2019 (COVID-19) in France: Surveillance, investigations and control measures, January 2020. Eurosurveillance 2020, 25, 2000094. [Google Scholar]
- Oussalah, A.; Gleye, S.; Clerc Urmes, I.; Laugel, E.; Callet, J.; Barbé, F.; Orlowski, S.; Malaplate, C.; Aimone-Gastin, I.; Caillierez, B.M.; et al. Long-term ACE Inhibitor/ARB Use Is Associated With Severe Renal Dysfunction and Acute Kidney Injury in Patients With Severe COVID-19: Results From a Referral Center Cohort in the Northeast of France. Clin. Infect. Dis Off. Publ Infect. Dis Soc. Am. 2020, 71, 2447–2456. [Google Scholar] [CrossRef]
- Pornet, C.; Delpierre, C.; Dejardin, O.; Grosclaude, P.; Launay, L.; Guittet, L.; Lang, T.; Launoy, G. Construction of an adaptable European transnational ecological deprivation index: The French version. J. Epidemiol. Community Health 2012, 66, 982–989. [Google Scholar] [CrossRef]
- Salje, H.; Tran Kiem, C.; Lefrancq, N.; Courtejoie, N.; Bosetti, P.; Paireau, J.; Andronico, A.; Hozé, N.; Richet, J.; Dubost, C.-L.; et al. Estimating the burden of SARS-CoV-2 in France. Science 2020, 369, 208–211. [Google Scholar] [CrossRef]
- Labbe, E.; Moulin, J.J.; Gueguen, R.; Sass, C.; Chatain, C.; Gerbaud, L. Un indicateur de mesure de la précarité et de la « santé sociale » : Le score EPICES: L’expérience des Centres d’examens de santé de l’Assurance maladie. Rev. Ires. 2007, 53, 3. [Google Scholar] [CrossRef] [Green Version]
- Case Definition for Coronavirus Disease 2019 (COVID-19), as of 3 December 2020. European Centre for Disease Prevention and Control. Available online: https://www.ecdc.europa.eu/en/covid-19/surveillance/case-definition (accessed on 21 January 2021).
- INSEE. Population par sexe et groupe d’âges [Internet]. Available online: https://www.insee.fr/fr/statistiques/2381474 (accessed on 28 May 2020).
- Chavent, M.; Kuentz-Simonet, V.; Liquet, B.; Saracco, J. ClustOfVar: An R Package for the Clustering of Variables. J. Stat. Softw. 2012, 50. [Google Scholar] [CrossRef] [Green Version]
- Siegel, S.; Castellan, N.J. Nonparametric Statistics for the Behavioral Sciences; McGraw-Hill: New York, NY, USA, 1988; p. 440. [Google Scholar]
- Naqvi, A.A.T.; Fatima, K.; Mohammad, T.; Fatima, U.; Singh, I.K.; Singh, A.; Atif, S.M.; Hariprasad, G.; Hasan, G.M.; Hassan, M.I. Insights into SARS-CoV-2 genome, structure, evolution, pathogenesis and therapies: Structural genomics approach. Biochim. Biophys. Acta BBA—Mol. Basis Dis. 2020, 1866, 165878. [Google Scholar] [CrossRef]
- Simula, E.R.; Manca, M.A.; Jasemi, S.; Uzzau, S.; Rubino, S.; Manchia, P.; Bitti, A.; Palermo, M.; Sechi, L.A. HCoV-NL63 and SARS-CoV-2 Share Recognized Epitopes by the Humoral Response in Sera of People Collected Pre- and during CoV-2 Pandemic. Microorganisms 2020, 8, 1993. [Google Scholar] [CrossRef]
- Guo, L.; Ren, L.; Yang, S.; Xiao, M.; Chang, D.; Yang, F.; Cruz, C.S.D.; Wang, Y.; Wu, C.; Xiao, Y.; et al. Profiling Early Humoral Response to Diagnose Novel Coronavirus Disease (COVID-19). Clin. Infect. Dis. 2020, 71, 778–785. [Google Scholar] [CrossRef] [Green Version]
- Poston, D.; Weisblum, Y.; Wise, H.; Templeton, K.; Jenks, S.; Hatziioannou, T.; Bieniasz, P. Absence of SARS-CoV-2 neutralizing activity in pre-pandemic sera from individuals with recent seasonal coronavirus infection. Clin Infect Dis. 2020, ciaa1803. [Google Scholar] [CrossRef]
- Gaebler, C.; Wang, Z.; Lorenzi, J.C.C.; Muecksch, F.; Finkin, S.; Tokuyama, M.; Cho, A.; Jankovic, M.; Schaefer-Babajew, D.; Oliveira, T.Y.; et al. Evolution of Antibody Immunity to SARS-CoV-2. Nature. 2021, 591, 639–644. [Google Scholar] [CrossRef] [PubMed]
- Bao, Y.; Ling, Y.; Chen, Y.; Tian, D.; Zhao, G.; Zhang, X.; Hong, H.; Li, Y.; Su, B.; Lu, H.; et al. Dynamic Anti-Spike Protein Antibody Profiles in COVID-19 Patients. Int. J. Infect. Dis. 2020, 103, 540–548. [Google Scholar] [CrossRef] [PubMed]
- Von Rhein, C.; Scholz, T.; Henss, L.; Kronstein-Wiedemann, R.; Schwarz, T.; Rodionov, R.N.; Corman, V.M.; Tonn, T.; Schnierle, B.S. Comparison of potency assays to assess SARS-CoV-2 neutralizing antibody capacity in COVID-19 convalescent plasma. J. Virol. Methods 2021, 288, 114031. [Google Scholar] [CrossRef] [PubMed]
- Wiens, K.E.; Mawien, P.N.; Rumunu, J.; Slater, D.; Jones, F.K.; Moheed, S.; Caflish, A.; Bior, B.K.; Jacob, I.A.; Lako, R.L.L.; et al. Seroprevalence of anti-SARS-CoV-2 IgG antibodies in Juba, South Sudan: A population-based study. medRxiv 2021. [Google Scholar] [CrossRef]
- Shaw, J.A.; Meiring, M.; Cummins, T.; Chegou, N.N.; Claassen, C.; Plessis, N.D.; Flinn, M.; Hiemstra, A.; Kleynhans, L.; Leukes, V.; et al. Higher SARS-CoV-2 seroprevalence in workers with lower socioeconomic status in Cape Town, South Africa. PLoS ONE 2021, 16, e0247852. [Google Scholar] [CrossRef]
- Sykes, W.; Mhlanga, L.; Swanevelder, R.; Glatt, T.N.; Grebe, E.; Coleman, C.; Pieterson, N.; Cable, R.; Welte, A.; van den Berg, K.; et al. Prevalence of anti-SARS-CoV-2 antibodies among blood donors in Northern Cape, KwaZulu-Natal, Eastern Cape, and Free State provinces of South Africa in January 2021. Res. Sq. 2021. [Google Scholar] [CrossRef]
- Boonyaratanakornkit, J.; Morishima, C.; Selke, S.; Zamora, D.; McGuffin, S.A.; Shapiro, A.E.; Campbell, V.L.; McClurkan, C.L.; Jing, L.; Gross, R.; et al. Clinical, laboratory, and temporal predictors of neutralizing antibodies to SARS-CoV-2 among COVID-19 convalescent plasma donor candidates. J. Clin. Investig. 2021, 131, e144930. [Google Scholar] [CrossRef]
- Planas, D.; Bruel, T.; Grzelak, L.; Guivel-Benhassine, F.; Staropoli, I.; Porrot, F.; Planchais, C.; Buchrieser, J.; Rajah, M.M.; Bishop, E.; et al. Sensitivity of infectious SARS-CoV-2 B.1.1.7 and B.1.351 variants to neutralizing antibodies. Nat. Med. 2021, 27, 917–924. [Google Scholar] [CrossRef]
- Shon, J.-L.P.K.; Robertson, G. Determinants of Electoral Non-Registration and Sensitive Neighbourhoods in France. Population 2004, 59, 143–156. [Google Scholar] [CrossRef]
- Martin, J.; Klapsa, D.; Wilton, T.; Zambon, M.; Bentley, E.; Bujaki, E.; Fritzsche, M.; Mate, R.; Majumdar, M. Tracking SARS-CoV-2 in Sewage: Evidence of Changes in Virus Variant Predominance during COVID-19 Pandemic. Viruses 2020, 12, 1144. [Google Scholar] [CrossRef]
- Altmann, D.M.; Boyton, R.J.; Beale, R. Immunity to SARS-CoV-2 variants of concern. Science 2021, 371, 1103–1104. [Google Scholar] [CrossRef]
- West, R.; Kobokovich, A.; Connell, N.; Gronvall, G.K. COVID-19 Antibody Tests: A Valuable Public Health Tool with Limited Relevance to Individuals. Trends Microbiol. 2021, 29, 214–223. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| n | IgT | IgM | IgA | IgG | Serological Status | Seroneutralization Capacity (n) |
|---|---|---|---|---|---|---|
| 1923 | Negative | NR | NR | NR | Seronegative | NE |
| 32 | Negative | Negative | Negative | Negative | Seronegative * | NE |
| 8 | Positive | Negative | Negative | Negative | Seronegative | NE |
| 2 | Negative | Negative | Positive | Positive | Seropositive * | 0 |
| 14 | Positive | Positive | Positive | Positive | Seropositive | 11 |
| 0 | Positive | Positive | Positive | Negative | Seropositive | NE |
| 3 | Positive | Positive | Negative | Positive | Seropositive | 1 |
| 17 | Positive | Negative | Positive | Positive | Seropositive | 15 |
| 0 | Positive | Positive | Negative | Negative | Seropositive | NE |
| 0 | Positive | Negative | Positive | Negative | Seropositive | NE |
| 7 | Positive | Negative | Negative | Positive | Seropositive | 4 |
| 2006 | Total |
| Modalities | Positive/Total | % | % CI | OR | OR CI | p |
|---|---|---|---|---|---|---|
| Age | ||||||
| 05–19 | 2/203 | 1.0 | 0.1–3.5 | 0.7 | 0.1–3.2 | 0.65 |
| 20–34 | 10/215 | 4.7 | 2.3–8.4 | 3.4 | 1.2–10.9 | 0.03 |
| 35–49 | 5/350 | 1.4 | 0.5–3.3 | ref | ||
| 50–64 | 16/553 | 2.9 | 1.7–4.7 | 2.1 | 0.8–6.3 | 0.16 |
| 65–79 | 9/573 | 1.6 | 0.7–3.0 | 1.1 | 0.4–3.6 | 0.86 |
| 80+ | 1/112 | 0.9 | 0.0–4.9 | 0.7 | 0.0–3.9 | 0.67 |
| Gender | ||||||
| Female | 24/1104 | 2.2 | 1.4–3.2 | ref | ||
| Male | 19/902 | 2.1 | 1.3–3.3 | 1.0 | 0.5–1.8 | 0.92 |
| Quintile EDI | ||||||
| 1–2 | 6/615 | 1.0 | 0.4–0.2 | ref | ||
| 3–4-5 | 37/1391 | 2.7 | 1.9–3.7 | 2.8 | 1.3–7.3 | 0.02 |
| Household Size | ||||||
| 1 | 9/364 | 2.5 | 1.1–4.6 | ref | ||
| 2 | 19/882 | 2.2 | 1.3–3.3 | 0.9 * | 0.4–2.0 | 0.74 |
| >=3 | 15/760 | 2.0 | 1.1–3.2 | 0.6 | 0.2–1.5 | 0.24 |
| Educational Level: Baccalaureate | ||||||
| Yes | 33/1266 | 2.6 | 1.8–3.6 | ref | ||
| No | 8/586 | 1.4 | 0.6–2.7 | 0.5 | 0.2–1.1 | 0.1 |
| missing | 154 | |||||
| Smoking status | ||||||
| Non-Smoker | 38/1583 | 2.4 | 0.2–3.3 | ref | ref | |
| Smoker | 4/338 | 1.2 | 0.3–3.0 | 0.5 | 0.1–1.2 | 0.17 |
| Missing | 85 | |||||
| Body Mass Index | ||||||
| <25 | 22/1162 | 1.9 | 1.2–2.9 | ref | ||
| 25–30 | 15/551 | 2.7 | 1.5–4.5 | 1.5 | 0.7–2.8 | 0.27 |
| >=30 | 6/284 | 2.1 | 0.8–4.5 | 1.1 | 0.4–2.6 | 0.81 |
| missing | 9 | |||||
| Comorbidity | ||||||
| No | 38/1726 | 2.20 | 1.6–3.0 | ref | ||
| Yes | 5/280 | 1.78 | 0.6–4.1 | 0.8 | 0.3–1.9 | 0.65 |
| Precariousness (Adjusted on Age, Sex and EDI) | ||||||
| EPICES <= 30 | 35/1428 | 2.5 | 1.7–3.4 | ref | ||
| EPICES > 30 | 4/388 | 1.0 | 0.3–2.6 | 0.4 | 0.1–1.0 | 0.1 |
| Clinical Criterion | Seropositive | Seronegative | p-Value |
|---|---|---|---|
| n | 43 | 2006 | |
At least one symptom | % 83.7 | % 47.6 | 3 × 10−6 |
| At least one intense symptom | 60.5 | 13.1 | 1 × 10−18 |
| Clinical criteria poss Covid-19 * | 74.4 | 23.8 | 3 × 10−14 |
| Fever | 62.8 | 14.7 | 1 × 10−17 |
| Cough | 53.5 | 12.1 | 1 × 10−15 |
| Fatigue | 48.8 | 10.9 | 6 × 10−11 |
| Shortness of breath | 46.5 | 6.6 | 6 × 10−13 |
| Aches | 41.9 | 8.2 | 2 × 10−14 |
| Anosmia/ageusia | 39.5 | 2.3 | 5 × 10−44 |
| Muscle pain | 37.2 | 10.4 | 3 × 10−8 |
| Sore throat | 34.9 | 14.7 | 3 × 10−4 |
| Headaches | 32.6 | 10.1 | 2 × 10−6 |
| Rhinorrhea | 30.2 | 16.6 | 0.02 |
| Chest pain | 25.6 | 6.3 | 6 × 10−17 |
| Diarrhea | 23.30 | 8.4 | 0.0006 |
| Abdominal pain | 20.9 | 6.8 | 0.0004 |
| Loss of balance | 14.0 | 4.0 | 0.001 |
| Nausea | 14.0 | 3.8 | 0.0009 |
| Appetite loss | 11.6 | 1.1 | 2 × 10−9 |
| Skin rashes | 7.0 | 4.9 | 0.52 |
| Irritated eyes | 4.7 | 6.0 | 0.70 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gégout Petit, A.; Jeulin, H.; Legrand, K.; Jay, N.; Bochnakian, A.; Vallois, P.; Schvoerer, E.; Guillemin, F. Seroprevalence of SARS-CoV-2, Symptom Profiles and Sero-Neutralization in a Suburban Area, France. Viruses 2021, 13, 1076. https://doi.org/10.3390/v13061076
Gégout Petit A, Jeulin H, Legrand K, Jay N, Bochnakian A, Vallois P, Schvoerer E, Guillemin F. Seroprevalence of SARS-CoV-2, Symptom Profiles and Sero-Neutralization in a Suburban Area, France. Viruses. 2021; 13(6):1076. https://doi.org/10.3390/v13061076
Chicago/Turabian StyleGégout Petit, Anne, Hélène Jeulin, Karine Legrand, Nicolas Jay, Agathe Bochnakian, Pierre Vallois, Evelyne Schvoerer, and Francis Guillemin. 2021. "Seroprevalence of SARS-CoV-2, Symptom Profiles and Sero-Neutralization in a Suburban Area, France" Viruses 13, no. 6: 1076. https://doi.org/10.3390/v13061076