
Hepatitis E Virus in People Who Use Crack-Cocaine: A Cross-Sectional Study in a Remote Region of Northern Brazil

 , , , ,
, , , ,  , , , , and
, , , , and
Abstract
:1. Introduction
2. Materials and Methods
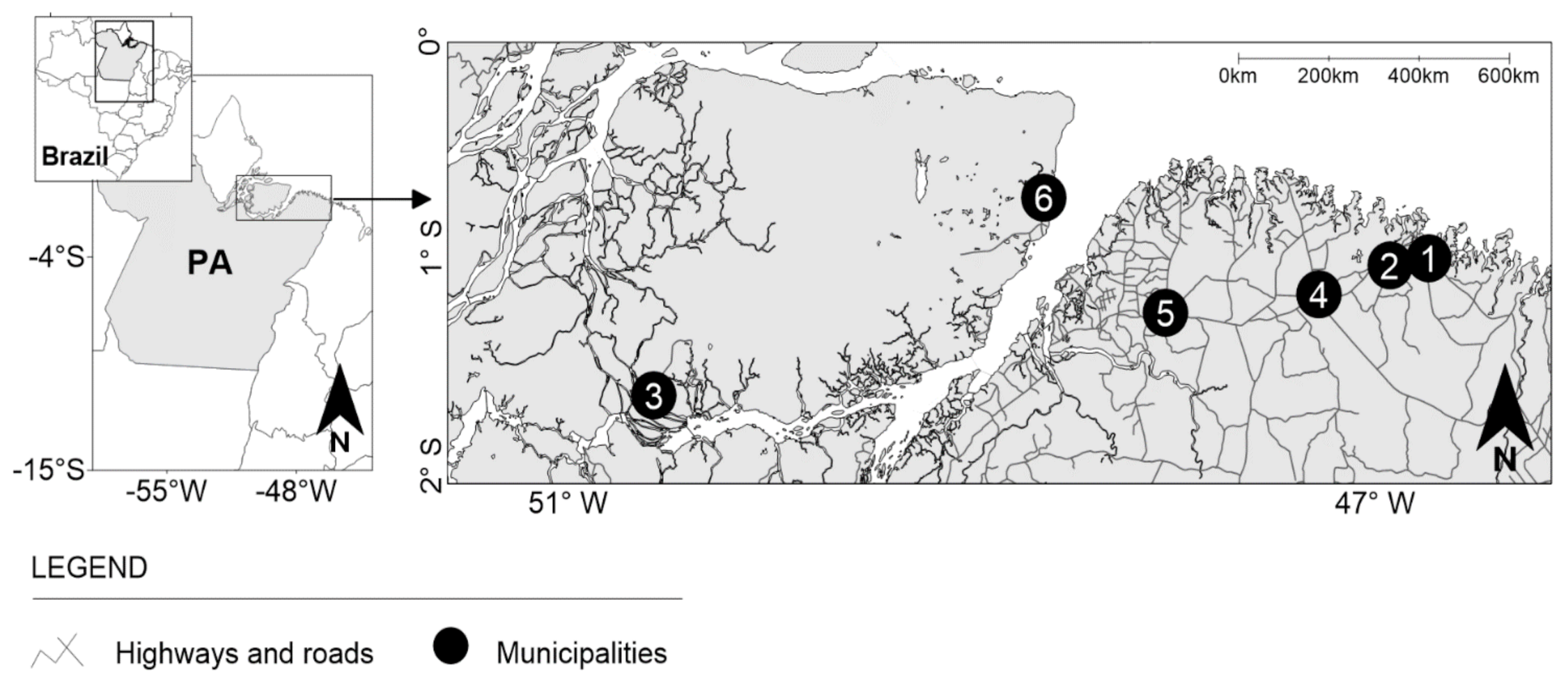
2.1. Study Area
2.2. Study Design
2.3. Sample Size
2.4. Sample Collection and Laboratory Tests
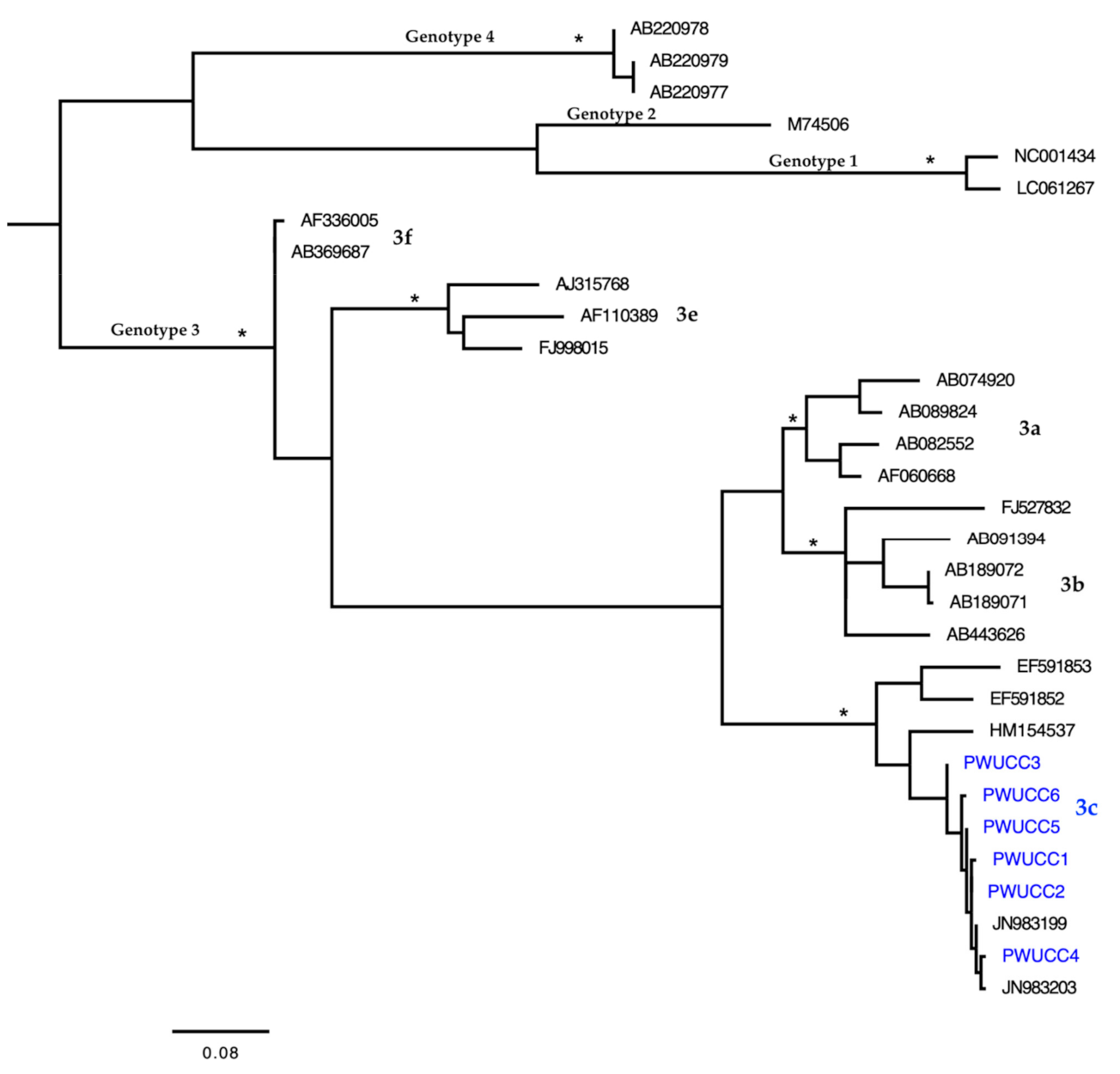
2.5. Phylogenetic Analysis and Genotyping
2.6. Statistical Analysis
3. Results
3.1. Sample Size
3.2. Characteristics of the PWUCC
3.3. Laboratory Markers and HEV Genotypes
3.4. Factors Associated with HEV Exposure
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Denner, J. Hepatitis E virus (HEV)—The Future. Virus 2019, 11, 251. [Google Scholar] [CrossRef] [Green Version]
- Van der Poel, W.H. Food and environmental routes of Hepatitis E virus transmission. Curr. Opin. Virol. 2014, 4, 91–96. [Google Scholar] [CrossRef]
- Smith, D.B.; Izopet, J.; Nicot, F.; Simmonds, P.; Jameel, S.; Meng, X.J.; Norder, H.; Okamoto, H.; Van der Poel, W.H.M.; Reuter, G.; et al. Update: Proposed reference sequences for subtypes of hepatitis E virus (species Orthohepevirus A). J. Gen. Virol. 2020, 101, 692–698. [Google Scholar] [CrossRef] [PubMed]
- Melgaço, J.G.; Gardinali, N.R.; de Mello, V.D.M.; Leal, M.; Lewis-Ximenez, L.L.; Pinto, M.A. Hepatitis E: Update on Prevention and Control. BioMed Res. Int. 2018. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, G.H.; Tan, B.H.; Teo, E.C.; Lim, S.G.; Dan, Y.Y.; Wee, A.; Aw, P.P.; Zhu, Y.; Hibberd, M.L.; Tan, C.K.; et al. Chronic Infection With Camelid Hepatitis E Virus in a Liver Transplant Recipient Who Regularly Consumes Camel Meat and Milk. Gastroenterology 2016, 150, 355–357. [Google Scholar] [CrossRef] [Green Version]
- Kamar, N.; Izopet, J.; Pavio, N.; Aggarwal, R.; Labrique, A.; Wedemeyer, H.; Dalton, H.R. Hepatitis E virus infection. Clin. Microbiol. Rev. 2017, 3. [Google Scholar] [CrossRef]
- Khuroo, M.S.; Khuroo, M.S.; Khuroo, N.S. Transmission of Hepatitis E Virus in Developing Countries. Virus 2016, 8, 253. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- WHO. Hepatitis E. Available online: https://www.who.int/news-room/fact-sheets/detail/hepatitis-e (accessed on 27 July 2020).
- Sayed, I.M.; El-Mokhtar, M.A.; Mahmoud, M.; Elkhawaga, A.A.; Gaber, S.; Seddek, N.H.; Abdel-Wahid, L.; Ashmawy, A.M.; Alkareemy, E. Clinical Outcomes and Prevalence of Hepatitis E Virus (HEV) Among Non-A-C Hepatitis Patients in Egypt. Infect. Drug Resist. 2021, 14, 59–69. [Google Scholar] [CrossRef]
- Sayed, I.M.; Elkhawaga, A.A.; El-Mokhtar, M.A. Circulation of hepatitis E virus (HEV) and/or HEV-like agent in non-mixed dairy farms could represent a potential source of infection for Egyptian people. Int. J. Food Microbiol. 2020, 317, 108479. [Google Scholar] [CrossRef]
- El-Mokhtar, M.A.; Elkhawaga, A.A.; Sayed, I.M. Assessment of hepatitis E virus (HEV) in the edible goat products pointed out a risk for human infection in Upper Egypt. Int. J. Food Microbiol. 2020, 330, 108784. Available online: http://j.ijfoodmicro.2020.108784 (accessed on 1 May 2021). [CrossRef]
- Pisano, M.B.; Martinez-Wassaf, M.G.; Mirazo, S.; Fantilli, A.; Arbiza, J.; Debes, J.D.; Ré, V.E. Hepatitis E virus in South America: The current scenario. Liver Int. 2018, 38, 1536–1546. [Google Scholar] [CrossRef] [Green Version]
- Hering, T.; Passos, A.M.; Perez, R.M.; Bilar, J.; Fragano, D.; Granato, C.; Medina-Pestana, J.O.; Ferraz, M.L. Past and current hepatitis E virus infection in renal transplant patients. J. Med. Virol. 2014, 86, 948–953. [Google Scholar] [CrossRef] [PubMed]
- Gonçales, N.S.; Pinho, J.R.; Moreira, R.C.; Saraceni, C.P.; Spina, A.M.; Stucchi, R.B.; Filho, A.D.; Magna, L.A.; Gonçales Júnior, F.L. Hepatitis E virus immunoglobulin G antibodies in different populations in Campinas, Brazil. Clin. Diagn. Lab. Immunol. 2000, 7, 813–816. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vitral, C.L.; da Silva-Nunes, M.; Pinto, M.A.; de Oliveira, J.M.; Gaspar, A.M.; Pereira, R.C.; Ferreira, M.U. Hepatitis A and E seroprevalence and associated risk factors: A community-based cross-sectional survey in rural Amazonia. BMC Infect. Dis. 2014, 14. [Google Scholar] [CrossRef]
- Oliveira-Filho, E.F.; Lopes, K.G.S.; Cunha, D.S. Risk Analysis and Occurrence of Hepatitis E Virus (HEV) in Domestic Swine in Northeast Brazil. Food Environ. Virol. 2017, 9, 256–259. [Google Scholar] [CrossRef]
- Moss da Silva, C.; Oliveira, J.M.; Mendoza-Sassi, R.A.; Figueiredo, A.S.; Mota, L.D.D.; Nader, M.M.; Gardinali, N.R.; Kevorkian, Y.B.; Salvador, S.B.S.; Pinto, M.A.; et al. Detection and characterization of hepatitis E virus genotype 3 in HIV-infected patients and blood donors from southern Brazil. Int. J. Infect. Dis. 2019, 86, 114–121. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bricks, G.; Senise, J.F.; Pott Junior, H.; Grandi, G.; Passarini, A.; Caldeira, D.B.; Carnaúba Junior, D.; Moraes, H.A.B.; Granato, C.F.H.; Castelo, A. Seroprevalence of hepatitis E virus in chronic hepatitis C in Brazil. Braz. J. Infect. Dis. 2018, 22, 85–91. [Google Scholar] [CrossRef]
- Bezerra, L.A.; de Oliveira-Filho, E.F.; Silva, J.V.J., Jr.; Morais, V.M.S.; Gonçales, J.P.; da Silva, D.M.; Duarte Coêlho, M.R.C. Risk analysis and seroprevalence of HEV in people living with HIV/AIDS in Brazil. Acta Trop. 2019, 189, 65–68. [Google Scholar] [CrossRef]
- Castro, V.O.L.; Tejada-Strop, A.; Weis, S.M.S.; Stábile, A.C.; de Oliveira, S.M.V.L.; Teles, S.A.; Kamili, S.; Motta-Castro, A.R.C. Evidence of hepatitis E virus infections among persons who use crack cocaine from the Midwest region of Brazil. J. Med. Virol. 2019, 91, 151–154. [Google Scholar] [CrossRef] [Green Version]
- Passos, A.M.; Heringer, T.P.; Medina-Pestana, J.O.; Ferraz, M.L.; Granato, C.F. First report and molecular characterization of hepatitis E virus infection in renal transplant recipients in Brazil. J. Med. Virol. 2013, 85, 615–619. [Google Scholar] [CrossRef]
- Dualibi, L.B.; Ribeiro, M.; Laranjeira, R. Profile of cocaine and crack users in Brazil. Cad. Saude Publica 2008, 24, 545–557. [Google Scholar] [CrossRef] [Green Version]
- Santos Cruz, M.; Andrade, T.; Bastos, F.I.; Leal, E.; Bertoni, N.; Villar, L.M.; Tiesmaki, M.; Fischer, B. Key drug use, health and socio-economic characteristics of young crack users in two Brazilian cities. Int. J. Drug Policy 2013, 24, 432–438. [Google Scholar] [CrossRef] [PubMed]
- Halpern, S.C.; Scherer, J.N.; Roglio, V.; Faller, S.; Sordi, A.; Ornell, F.; Dalbosco, C.; Pechansky, F.; Kessler, F.; Diemen, L.V. Clinical and social vulnerabilities in crack users according to housing status: A multicenter study in six Brazilian state capitals. Cad. Saude Publica 2017, 33, 6. [Google Scholar] [CrossRef] [Green Version]
- Vernaglia, T.V.C.; Leite, T.H.; Faller, S.; Pechansky, F.; Kessler, F.H.P.; Cruz, M.S.; Group, B.C. The female crack users: Higher rates of social vulnerability in Brazil. Health Care Women Int. 2017, 38, 1170–1187. [Google Scholar] [CrossRef]
- Peiter, P.; Belmonte, P.; Teixeira, M.; Cobra, G.; Lacerda, A. Homeless crack cocaine users: Territories and territorialities in the constitution of social support networks for health. Soc. Sci. Med. 2019, 227, 111–118. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Oliveira-Filho, A.B.; Silva, F.Q.; Santosa, F.J.A.; Cardoso, Y.M.N.; Di Miceli, J.F.F.; Resque, R.L.; Silva-Oliveira, G.C.; Martins, L.C.; Pinheiro, L.M.L.; Machado, L.F.A.; et al. Prevalence and risk factors for HIV-1 infection in people who use illicit drugs in northern Brazil. Trans. R. Soc. Trop. Med. Hyg. 2020, 114, 121–213. [Google Scholar] [CrossRef] [PubMed]
- Oliveira-Filho, A.B.; Santos, F.J.A.; Silva, F.Q.; Raiol, N.C.; Costa, C.C.S.; Piauiense, J.N.F.; Martins, L.C.; Cardoso, Y.M.N.; Di Miceli, J.F.F.; Resque, R.L.; et al. Hepatitis C virus infection status and associated factors among a multi-site sample of people who used illicit drugs in the Amazon region. BMC Infect. Dis. 2019. [Google Scholar] [CrossRef]
- Piauiense, J.N.F.; Costa, C.C.S.; Silva, R.J.S.; Cardoso, Y.M.N.; Di Miceli, J.F.F.; Resque, R.L.R.; Lemos, J.A.R.; Fischer, B.; Pinho, J.R.R.; Kupek, E.; et al. Hepatitis B Virus Infection among People Who Use Illicit Drugs: Prevalence, Genotypes and Risk Factors in the State of Amapá, Northern Brazil. Sub. Use Misuse 2020, 55, 1633–1639. [Google Scholar] [CrossRef]
- Oliveira-Filho, A.B.; Araújo, A.P.S.; Souza, A.P.C.; Gomes, C.M.; Silva-Oliveira, G.C.; Martins, L.C.; Fischer, B.; Machado, L.F.A.; Vallinoto, A.C.R.; Ishak, R.; et al. Human T-lymphotropic virus 1 and 2 among people who used illicit drugs in the state of Pará, northern Brazil. Sci. Rep. 2019, 9. [Google Scholar] [CrossRef] [Green Version]
- Rodrigues, M.S.A.; Nascimento, R.S.; Fonseca, R.R.S.; Silva-Oliveira, G.C.; Machado, L.F.A.; Emil Kupek, E.; Fischer, B.; Oliveira-Filho, A.B. Oral HPV among people who use crack-cocaine: Prevalence, genotypes, risk factors, and key interventions in a remote Northern Brazilian region. Clin. Oral Investig. 2020, 25, 759–767. [Google Scholar] [CrossRef]
- De Souza, A.J.S.; Gomes-Gouvêa, M.S.; Soares, M.C.P.; Pinho, J.R.R.; Malheiros, A.P.; Carneiro, L.A.; Santos, D.R.L.; Pereira, W.L.A. HEV infection in swine from Eastern Brazilian Amazon: Evidence of co-infection by different subtypes. Comp. Immunol. Microbiol. Infect. Dis. 2012, 35, 477–485. [Google Scholar] [CrossRef] [PubMed]
- Souza, A.J.S.; Oliveira, C.M.A.; Sarmento, V.P.; Chagas, A.A.C.; Nonato, N.S.; Brito, D.C.N.; Barbosa, K.M.V.; Soares, M.C.P.; Nunes, H.M. Hepatitis E virus infection among rural Afro-descendant communities from the eastern Brazilian Amazon. Rev. Soc. Bras. Med. Trop. 2018, 51, 803–807. [Google Scholar] [CrossRef] [PubMed]
- Instituto Brasileiro de Geografia e Estatística (IBGE), Brasil. Panorama: Municípios do Pará. Brasil. Available online: https://cidades.ibge.gov.br/brasil/pa/panorama (accessed on 11 January 2021).
- da Costa, L.M.; Raiol, N.C.; Lisboa, B.L.A.; Frade, P.C.R.; Blandtt, L.D.S.; Silva-Oliveira, G.C.; Machado, L.F.A.; Martins, L.C.; Oliveira-Filho, A.B. Prevalence and Risk Factors for Human Immunodeficiency Virus Infection Among Female Sex Workers: Distinct Offers of Sexual Services in a Municipality of the Brazilian Amazon. AIDS Res. Hum. Retrovir. 2019, 35, 826–832. [Google Scholar] [CrossRef] [PubMed]
- Jothikumar, N.; Cromeans, T.L.; Robertson, B.H.; Meng, X.J.; Hill, V.R. A broadly reactive one-step real-time RT-PCR assay for rapid and sensitive detection of hepatitis E virus. J. Virol. Methods 2006, 131, 65–71. [Google Scholar] [CrossRef] [PubMed]
- Heldt, F.H.; Staggmeier, R.; Gularte, J.S.; Demoliner, M.; Henzel, A.; Spilki, F.R. Hepatitis E Virus in Surface Water, Sediments, and Pork Products Marketed in Southern Brazil. Food Environ. Virol. 2016, 8, 200–205. [Google Scholar] [CrossRef]
- Larsson, A. AliView: A fast and lightweight alignment viewer and editor for large datasets. Bioinformatics 2014, 30, 3276–3278. [Google Scholar] [CrossRef]
- Guindon, S.; Dufayard, J.F.; Lefort, V.; Anisimova, M.; Hordijk, W.; Gascuel, O. New algorithms and methods to estimate maximum-likelihood phylogenies: Assessing the performance of PhyML 3.0. Syst. Biol. 2010, 59, 307–321. [Google Scholar] [CrossRef] [Green Version]
- Lefort, V.; Longueville, J.E.; Gascuel, O. SMS: Smart Model Selection in PhyML. Mol. Biol. Evol. 2017, 34, 2422–2424. [Google Scholar] [CrossRef] [Green Version]
- Bartoloni, A.; Bartalesi, F.; Roselli, M.; Mantella, A.; Arce, C.C.; Paradisi, F.; Hall, A.J. Prevalence of antibodies against hepatitis A and E viruses among rural populations of the Chaco region, south-eastern Bolivia. Trop. Med. Int. Health 1999, 4, 596–601. [Google Scholar] [CrossRef]
- Blitz-Dorfman, L.; Monsalve, F.; Atencio, R.; Porto, L.; Monzon, M.; Favorov, M.O.; Fields, H.A.; Pujol, F.H.; Echevarría, J.M. Serological survey of markers of infection with viral hepatitis among the Yukpa Amerindians from western Venezuela. Ann. Trop. Med. Parasitol. 1996, 90, 655–657. [Google Scholar] [CrossRef]
- Cruells, M.R.; Mescia, G.; Gaibisso, R. Epidemiological study of hepatites A and E viruses in different populations in Uruguay. Gastroenterol. Hepatol. 1997, 20, 295–298. [Google Scholar] [PubMed]
- Fainboim, H.; González, J.; Fassio, E. Prevalence of hepatitis viruses in an anti-human immunodeficiency virus-positive population from Argentina. A multicentre study. J. Viral Hepat. 1999, 6, 53–57. [Google Scholar] [CrossRef] [PubMed]
- Gutiérrez-Vergara, C.; Quintero, J.; Duarte, J.F.; Suescún, J.P.; López-Herrera, A. Detection of hepatitis E virus genome in pig livers in Antioquia, Colombia. Genet. Mol. Res. 2015, 14, 2890–2899. [Google Scholar] [CrossRef] [PubMed]
- Ibarra, H.; Riedemann, S.; Toledo, C. Hepatitis A and E virus antibodies in Chilean children of low socioeconomic status: A year follow-up study. Rev. Med. Chil. 2006, 134, 139–144. [Google Scholar] [CrossRef] [Green Version]
- Ibarra, H.; Riedemann, S.; Reinhardt, G. Prevalence of hepatites E virus antibody in blood donors and other population groups in Southern Chile. Rev. Med. Chil. 1997, 125, 257–258. [Google Scholar]
- Vildosola, H.; Colichon, A.; Barreda, M.; Piscoya, M.; Palacios, O. Hepatitis E IgG antibodies seroprevalence in a Peruvian risk group. Rev. Gastroenterol. Peru 2000, 20, 111–116. [Google Scholar] [PubMed]
- Pepe, R.M.T.; Risso, G.W.M. Health Impacts Due to Deficient Water Access. Saude Soc. 2008, 17, 21–32. [Google Scholar] [CrossRef] [Green Version]
- Barreto, M.L.; Teixeira, M.G.; Bastos, F.I.; Ximenes, R.A.; Barata, R.B.; Rodrigues, L.C. Successes and failures in the control of infectious diseases in Brazil: Social and environmental context, policies, interventions, and research needs. Lancet 2011, 377, 1877–1889. [Google Scholar] [CrossRef]
- Nahas, M.I.P.; Moura, A.S.A.; Carvalho, R.C.; Heller, L. Inequality and discrimination in access to water and sanitation in the Belo Horizonte Metropolitan Region, Minas Gerais State, Brazil. Cad. Saude Publica 2019, 35. [Google Scholar] [CrossRef] [Green Version]
- Chaves, T.V.; Sanchez, Z.M.; Ribeiro, L.A.; Nappo, S.A. Crack cocaine craving: Behaviors and coping strategies among current and former users. Rev. Saude Publica 2011, 45, 1168–1175. [Google Scholar] [CrossRef] [Green Version]
- Ippagunta, S.K.; Naik, S.; Sharma, B.; Aggarwal, R. Presence of hepatitis E virus in sewage in Northern India: Frequency and seasonal pattern. J. Med. Virol. 2007, 79, 1827–1831. [Google Scholar] [CrossRef] [PubMed]
- Ishida, S.; Yoshizumi, S.; Ikeda, T.; Miyoshi, M.; Goto, A.; Matsubayashi, K.; Ikeda, H. Detection and molecular characterization of hepatitis E virus in clinical, environmental and putative animal sources. Arch. Virol. 2012, 157, 2363–2368. [Google Scholar] [CrossRef] [PubMed]
- Masclaux, F.G.; Hotz, P.; Friedli, D.; Savova-Bianchi, D.; Oppliger, A. High occurrence of hepatitis E virus in samples from wastewater treatment plants in Switzerland and comparison with other enteric viruses. Water Res. 2013, 47, 5101–5109. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- dos Santos, D.R.L.; de Paula, V.S.; de Oliveira, J.M.; Marchevsky, R.S.; Pinto, M.A. Hepatitis E virus in swine and effluent samples from slaughterhouses in Brazil. Vet. Microbiol. 2011, 149, 236–241. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Innis, B.L.; Lynch, J.A. Immunization against Hepatitis E. Cold Spring Harb. Perspect. Med. 2018, 8. [Google Scholar] [CrossRef]
- Vergara-Moragues, E.; Araos Gómez, P.; González-Saiz, F.; Rodríguez-Fonseca, F. Cocaine-induced psychotic symptoms in clinical setting. Psychiatry Res. 2014, 217, 115–120. [Google Scholar] [CrossRef]
- Narvaez, J.C.; Jansen, K.; Pinheiro, R.T.; Kapczinski, F.; Silva, R.A.; Pechansky, F.; Magalhães, P.V. Psychiatric and substance-use comorbidities associated with lifetime crack cocaine use in young adults in the general population. Comp. Psychiatry 2014, 55, 1369–1376. [Google Scholar] [CrossRef]
- Brasil, Ministério da Saúde. Centro de Atenção Psicossocial (CAPS). 2017. Available online: https://www.gov.br/saude/pt-br/acesso-a-informacao/acoes-e-programas/centro-de-atencao-psicossocial-caps (accessed on 8 March 2021).
- Guariento, C.F.; Torres, S.; Ecker, D.D. Prevenção e Promoção de Saúde no CAPS AD através de oficinas de psicoeducação. R. Eletr. Cient. Uergs. 2019, 5, 191–197. Available online: http://revista.uergs.edu.br/index.php/revuergs/article/view/1984 (accessed on 19 January 2021). [CrossRef]
- Pinho, R.J.; Pereira, A.P.F.B.; Lussi, I.A.O. Homeless, the world of work and the specialized reference centers for population in street situation (centro pop): Perspectives on actions for productive inclusion. Cad. Bras. Ter. Ocup. 2019, 27, 480–495. [Google Scholar] [CrossRef] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Characteristics | All | HEV+ (%) * | HEV− (%) | p-Value ** |
|---|---|---|---|---|
| Total | 437 | 79 (18.1) | 358 (81.9) | - |
| Sex | ||||
| Male | 314 | 52 (16.6) | 262 (83.4) | 0.19 |
| Female | 123 | 27 (22.0) | 96 (78.0) | |
| Age (years) | ||||
| 18–29 | 291 | 55 (18.9) | 236 (81.1) | 0.17 |
| 30–40 | 121 | 23 (19.0) | 98 (81.0) | |
| >40 | 25 | 1 (4.0) | 24 (96.0) | |
| Race/ethnicity (self-identified) | ||||
| White | 48 | 3 (6.3) | 45 (95.7) | 0.08 |
| Mixed race | 279 | 54 (19.4) | 225 (80.6) | |
| Black | 110 | 22 (20.0) | 108 (80.0) | |
| Marital status † | ||||
| Single | 344 | 67 (19.5) | 277 (80.5) | 0.19 |
| Separated or widowed | 63 | 10 (15.9) | 53 (84.1) | |
| Married or co-habiting | 30 | 2 (6.7) | 28 (93.3) | |
| Educational level | ||||
| No formal education (including illiterates) | 38 | 4 (10.5) | 34 (89.5) | 0.22 |
| Up to elementary school | 315 | 63 (20.0) | 252 (80.0) | |
| Up to high school/postgraduate | 84 | 12 (14.3) | 72 (85.7) | |
| Monthly income (Brazilian minimum wage) † | ||||
| ≤one minimum wage ‡ | 329 | 71 (21.6) | 258 (78.4) | <0.01 |
| 2–3 times the minimum wage | 83 | 7 (8.4) | 76 (91.6) | |
| >3 times the minimum wage | 25 | 1 (4.0) | 24 (96.0) | |
| Housing status † | ||||
| Live in your own home/with parents | 257 | 17 (6.6) | 240 (93.4) | |
| Lives house or rented room | 121 | 40 (33.1) | 81 (66.9) | <0.01 |
| Unstable housing (including homeless people) | 59 | 22 (37.3) | 37 (62.7) | |
| Crack-cocaine use history (months) | ||||
| Up to 20 | 51 | 2 (3.9) | 49 (96.1) | <0.01 |
| 21–50 | 282 | 28 (9.9) | 254 (90.1) | |
| >50 | 104 | 49 (47.1) | 55 (52.9) | |
| Sexual orientation | ||||
| Heterosexual | 396 | 75 (18.9) | 321 (81.1) | 0.15 |
| Same sex (including bisexual) | 41 | 4 (9.8) | 37 (90.2) | |
| Condom use during sex † | ||||
| Rarely + Never | 330 | 61 (18.5) | 269 (81.5) | 0.12 |
| Sometimes | 66 | 15 (22.7) | 51 (77.3) | |
| Always | 41 | 3 (7.3) | 38 (92.7) | |
| Number of sexual partners † | ||||
| More than 10 | 189 | 31 (16.4) | 158 (83.6) | 0.43 |
| Up to 10 | 248 | 48 (19.4) | 200 (80.6) | |
| Oral sex † | 281 | 47 (16.7) | 234 (83.3) | 0.32 |
| Anal sex † | 157 | 32 (20.4) | 125 (79.6) | 0.35 |
| Exchange of sex for money or illicit drug † | 124 | 24 (19.4) | 100 (80.6) | 0.66 |
| Shared use of crack-cocaine equipment † | 171 | 58 (33.9) | 113 (66.1) | <0.01 |
| HEV Diagnosis (Sample) | Positive/Total | % | 95% CI |
|---|---|---|---|
| Anti-HEV IgG (blood plasma) | 73/437 | 16.7 | 12.5–20.3 |
| Anti-HEV IgG + IgM (blood plasma) | 6/437 | 1.4 | 0.0–5.8 |
| HEV-RNA (blood plasma) | 2/79 | 2.5 | 0.0–6.6 |
| HEV-RNA (feces) | 6/79 | 7.6 | 3.4–11.3 |
| Exposure to HEV | 79/437 | 18.1 | 14.2–21.8 |
| Factors | Total | HEV+ (%) | Bivariate OR (95% CI) | Multivariate aOR (95% CI) |
|---|---|---|---|---|
| ≤1 vs. >1 minimum wage † | 329 | 71 (21.6) | 3.4 (1.6–7.4) | 3.8 (1.9–9.0) |
| Unstable (including homelessness) vs. stable housing † | 59 | 22 (37.3) | 3.7 (1.7–6.1) | 4.7 (1.6–7.4) |
| ≥40 months vs. <40 months use of crack-cocaine | 286 | 69 (24.1) | 4.6 (2.1–8.7) | 6.2 (2.3–11.3) |
| Shared vs. not shared crack-cocaine equipment † | 171 | 58 (33.9) | 5.7 (3.4–10.3) | 6.5 (3.5–12.4) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
do Nascimento, R.S.; Baia, K.L.N.; de Souza, S.B.; Fontoura, G.M.G.; Nunes, P.F.; Machado, L.F.A.; Kupek, E.; Fischer, B.; Martins, L.C.; Oliveira-Filho, A.B. Hepatitis E Virus in People Who Use Crack-Cocaine: A Cross-Sectional Study in a Remote Region of Northern Brazil. Viruses 2021, 13, 926. https://doi.org/10.3390/v13050926
do Nascimento RS, Baia KLN, de Souza SB, Fontoura GMG, Nunes PF, Machado LFA, Kupek E, Fischer B, Martins LC, Oliveira-Filho AB. Hepatitis E Virus in People Who Use Crack-Cocaine: A Cross-Sectional Study in a Remote Region of Northern Brazil. Viruses. 2021; 13(5):926. https://doi.org/10.3390/v13050926
Chicago/Turabian Styledo Nascimento, Raquel Silva, Karen Lorena N. Baia, Samara Borges de Souza, Guilherme Martins G. Fontoura, Patrícia Ferreira Nunes, Luiz Fernando A. Machado, Emil Kupek, Benedikt Fischer, Luísa Caricio Martins, and Aldemir B. Oliveira-Filho. 2021. "Hepatitis E Virus in People Who Use Crack-Cocaine: A Cross-Sectional Study in a Remote Region of Northern Brazil" Viruses 13, no. 5: 926. https://doi.org/10.3390/v13050926