
High Incidence and Early Onset of Urinary Tract Cancers in Patients with BK Polyomavirus Associated Nephropathy

 and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients and Definitions
2.2. Statistical Analysis
3. Results
3.1. Patient Characteristics
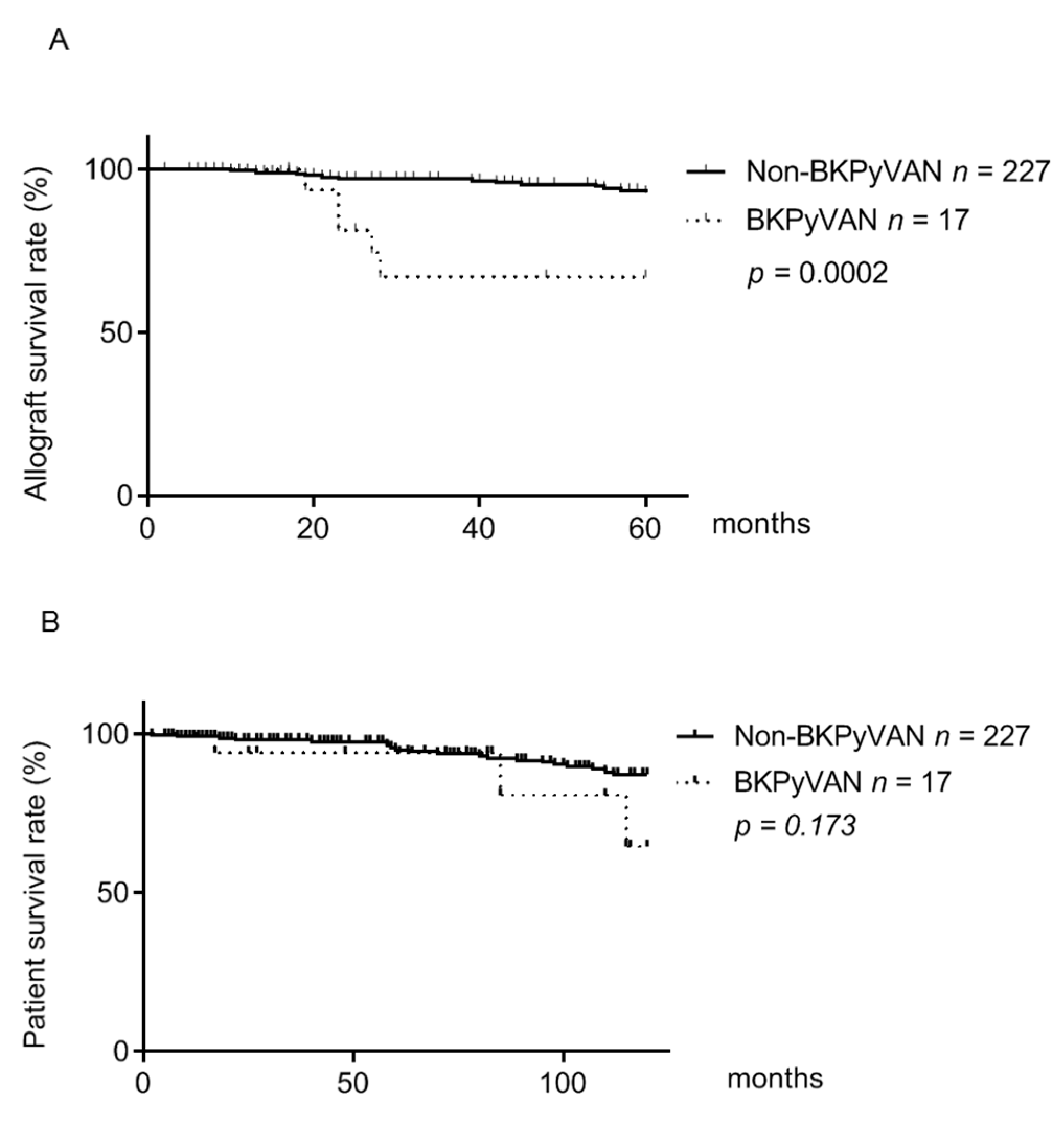
3.2. The Worst Allograft Outcome in Patients with BKPyVAN
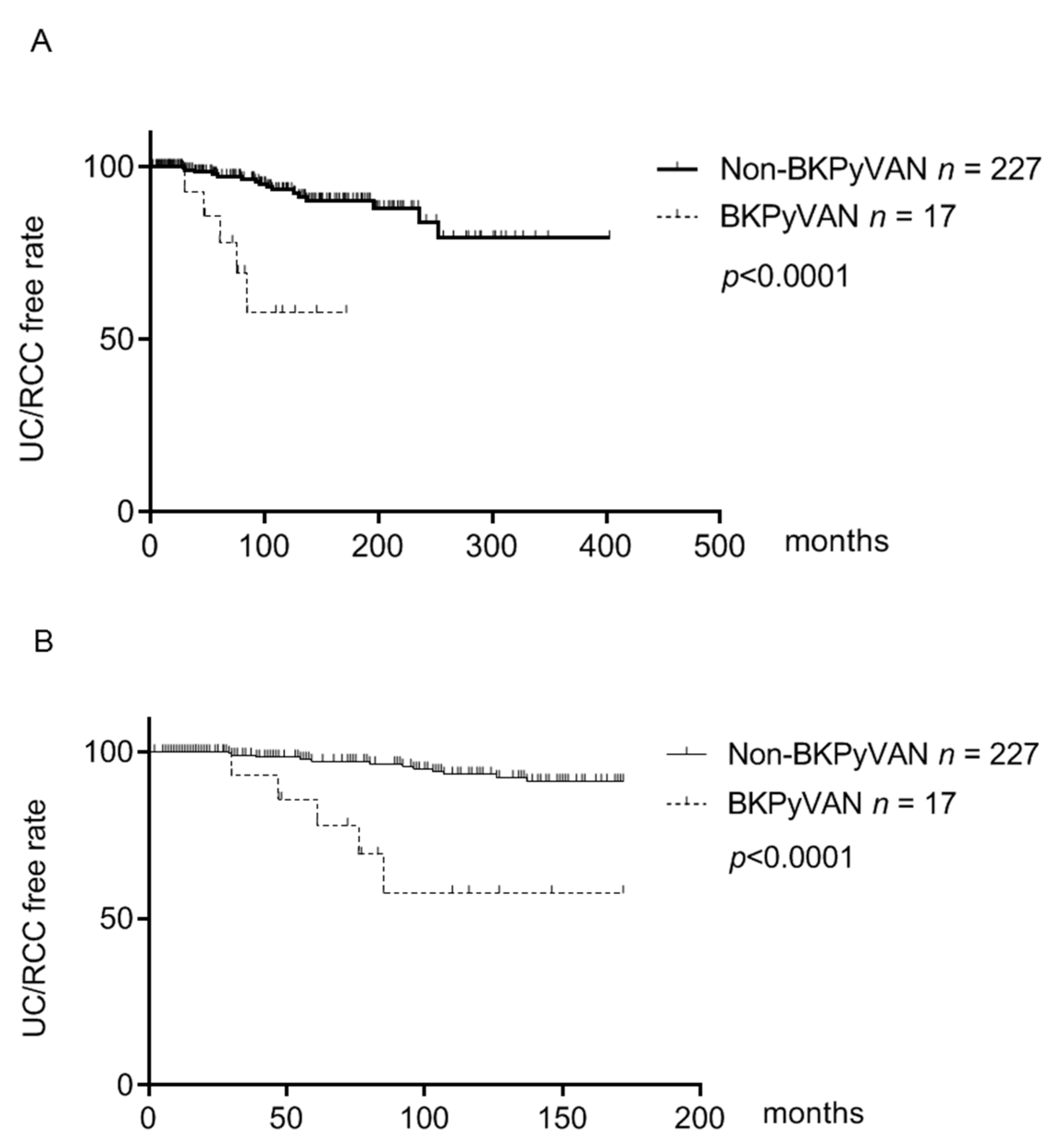
3.3. Increased Incidence of Urinary Tract Cancers in Patients with BKPyVAN
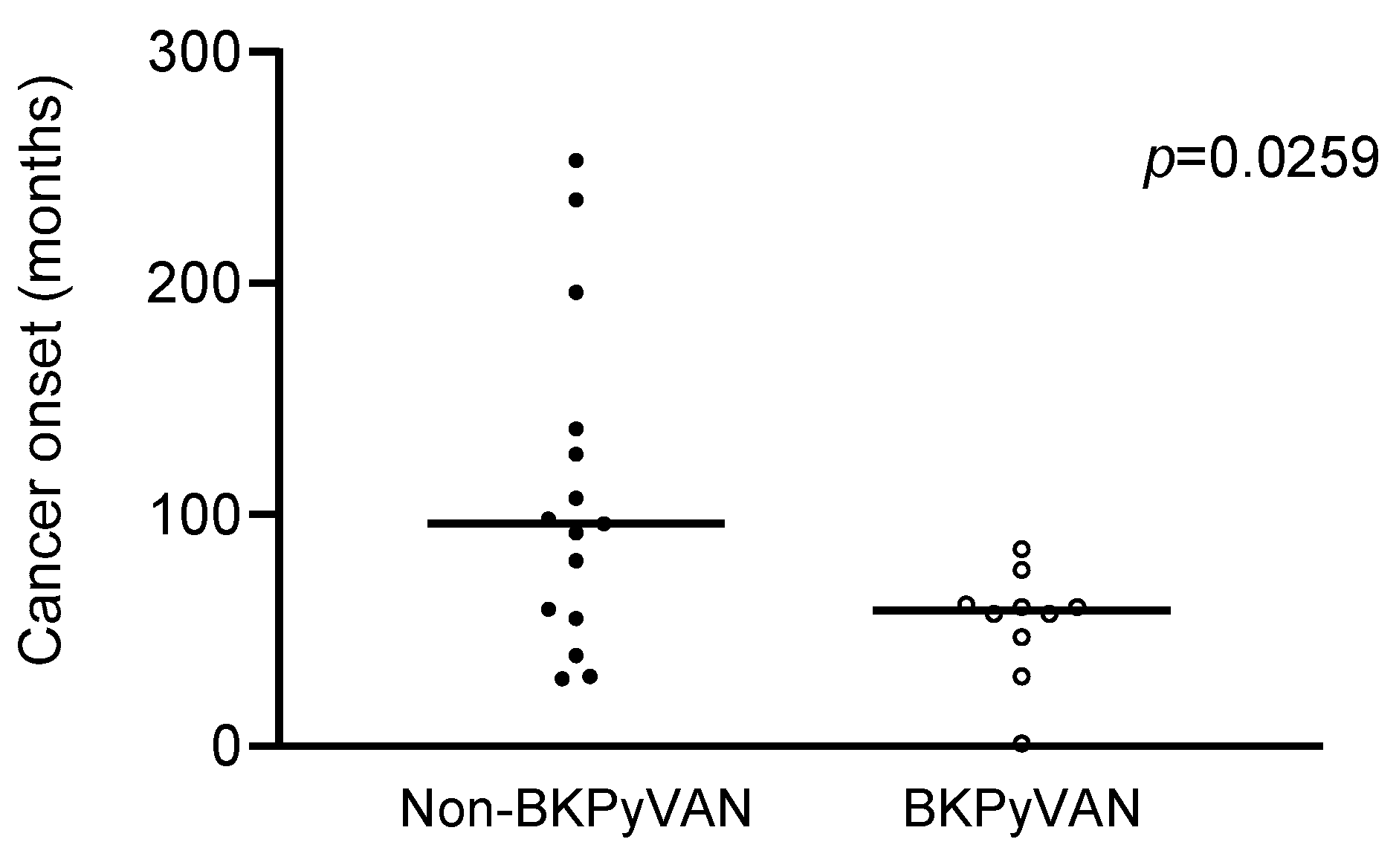
3.4. Earlier Onset of Urinary Tract Cancers in Patients with BKPyVAN
3.5. Association of BKPyVAN and Urinary Tract Cancers
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Murray, S.L.; O’Leary, E.; De Bhailis, A.M.; Deady, S.; Daly, F.E.; O’Kelly, P.; Williams, Y.; O’Neill, J.P.; Sexton, D.J.; Conlon, P.J. Cancer survival in kidney transplant recipients in Ireland. Nephrol. Dial. Transpl. 2020, 35, 1802–1810. [Google Scholar] [CrossRef]
- Au, E.; Wong, G.; Chapman, J.R. Cancer in kidney transplant recipients. Nat. Rev. Nephrol. 2018, 14, 508–520. [Google Scholar] [CrossRef]
- Chiu, H.F.; Chung, M.C.; Chung, C.J.; Yu, T.M.; Shu, K.H.; Wu, M.J. Prognosis of Kidney Transplant Recipients With Pretransplantation Malignancy: A Nationwide Population-Based Cohort Study in Taiwan. Transpl. Proc. 2016, 48, 918–920. [Google Scholar] [CrossRef]
- Tsai, H.I.; Lee, C.W.; Kuo, C.F.; See, L.C.; Liu, F.C.; Chiou, M.J.; Yu, H.P. De novo malignancy in organ transplant recipients in Taiwan: A nationwide cohort population study. Oncotarget 2017, 8, 36685–36695. [Google Scholar] [CrossRef] [Green Version]
- Li, W.H.; Chen, Y.J.; Tseng, W.C.; Lin, M.W.; Chen, T.J.; Chu, S.Y.; Hwang, C.Y.; Chen, C.C.; Lee, D.D.; Chang, Y.T.; et al. Malignancies after renal transplantation in Taiwan: A nationwide population-based study. Nephrol. Dial. Transpl. 2012, 27, 833–839. [Google Scholar] [CrossRef] [Green Version]
- de Martel, C.; Georges, D.; Bray, F.; Ferlay, J.; Clifford, G.M. Global burden of cancer attributable to infections in 2018: A worldwide incidence analysis. Lancet Glob. Health 2020, 8, e180–e190. [Google Scholar] [CrossRef] [Green Version]
- Zapatka, M.; Borozan, I.; Brewer, D.S.; Iskar, M.; Grundhoff, A.; Alawi, M.; Desai, N.; Sultmann, H.; Moch, H.; Pathogens, P.; et al. The landscape of viral associations in human cancers. Nat. Genet. 2020, 52, 320–330. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chang, Y.; Moore, P.S. Merkel cell carcinoma: A virus-induced human cancer. Annu. Rev. Pathol. 2012, 7, 123–144. [Google Scholar] [CrossRef] [Green Version]
- Moore, P.S.; Chang, Y. Why do viruses cause cancer? Highlights of the first century of human tumour virology. Nat. Rev. Cancer 2010, 10, 878–889. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rotondo, J.C.; Mazzoni, E.; Bononi, I.; Tognon, M.; Martini, F. Association Between Simian Virus 40 and Human Tumors. Front. Oncol. 2019, 9, 670. [Google Scholar] [CrossRef] [PubMed]
- Sadeghi, F.; Salehi-Vaziri, M.; Ghodsi, S.M.; Alizadeh, A.; Bokharaei-Salim, F.; Saroukalaei, S.T.; Mirbolouk, M.; Monavari, S.H.; Keyvani, H. Prevalence of JC polyomavirus large T antigen sequences among Iranian patients with central nervous system tumors. Arch. Virol. 2015, 160, 61–68. [Google Scholar] [CrossRef]
- Mou, X.; Chen, L.; Liu, F.; Lin, J.; Diao, P.; Wang, H.; Li, Y.; Lin, J.; Teng, L.; Xiang, C. Prevalence of JC virus in Chinese patients with colorectal cancer. PLoS ONE 2012, 7, e35900. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pina-Oviedo, S.; De Leon-Bojorge, B.; Cuesta-Mejias, T.; White, M.K.; Ortiz-Hidalgo, C.; Khalili, K.; Del Valle, L. Glioblastoma multiforme with small cell neuronal-like component: Association with human neurotropic JC virus. Acta Neuropathol. 2006, 111, 388–396. [Google Scholar] [CrossRef]
- Kean, J.M.; Rao, S.; Wang, M.; Garcea, R.L. Seroepidemiology of human polyomaviruses. PLoS Pathog. 2009, 5, e1000363. [Google Scholar] [CrossRef] [Green Version]
- Li, Y.J.; Chen, Y.C.; Lai, P.C.; Fang, J.T.; Yang, C.W.; Chiang, Y.J.; Chu, S.H.; Wu, M.J.; Tian, Y.C. A direct association of polyomavirus BK viruria with deterioration of renal allograft function in renal transplant patients. Clin. Transplant. 2009, 23, 505–510. [Google Scholar] [CrossRef] [PubMed]
- Wang, R.Y.; Li, Y.J.; Lee, W.C.; Wu, H.H.; Lin, C.Y.; Lee, C.C.; Chen, Y.C.; Hung, C.C.; Yang, C.W.; Tian, Y.C. The association between polyomavirus BK strains and BKV viruria in liver transplant recipients. Sci. Rep. 2016, 6, 28491. [Google Scholar] [CrossRef]
- Levican, J.; Acevedo, M.; Leon, O.; Gaggero, A.; Aguayo, F. Role of BK human polyomavirus in cancer. Infect. Agents Cancer 2018, 13, 12. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Huang, Y.; Chen, X.T.; Yang, S.C.; Yang, H.F.; Hou, X.T.; Chen, W.F.; Li, J.; Deng, R.H.; Luo, J.Q.; Wang, J.Y.; et al. Detection of Proximal Tubule Involvement by BK Polyomavirus in Kidney Transplant Recipients With Urinary Sediment Double-Immunostaining. Front. Immunol. 2020, 11, 582678. [Google Scholar] [CrossRef]
- Yen, C.L.; Tian, Y.C.; Wu, H.H.; Weng, C.H.; Chen, Y.C.; Tu, K.H.; Liu, S.H.; Lee, C.C.; Lai, P.C.; Fang, J.T.; et al. Conversion to mTOR-inhibitors with calcineurin inhibitor elimination or minimization reduces urinary polyomavirus BK load in kidney transplant recipients. J. Med. Assoc. 2016, 115, 539–546. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, Y.J.; Wu, H.H.; Weng, C.H.; Chen, Y.C.; Hung, C.C.; Yang, C.W.; Wang, R.Y.; Sakamoto, N.; Tian, Y.C. Cyclophilin A and Nuclear Factor of Activated T Cells Are Essential in Cyclosporine-Mediated Suppression of Polyomavirus BK Replication. Am. J. Transplant. 2012, 12, 2348–2362. [Google Scholar] [CrossRef]
- Li, Y.J.; Weng, C.H.; Lai, W.C.; Wu, H.H.; Chen, Y.C.; Hung, C.C.; Yang, C.W.; Tian, Y.C. A Suppressive Effect of Cyclosporine A on Replication and Noncoding Control Region Activation of Polyomavirus BK Virus. Transplantation 2010, 89, 299–306. [Google Scholar] [CrossRef]
- Hirsch, H.H.; Drachenberg, C.B.; Steiger, J.; Ramos, E. Polyomavirus-associated nephropathy in renal transplantation: Critical issues of screening and management. Adv. Exp. Med. Biol. 2006, 577, 160–173. [Google Scholar] [PubMed]
- Zeng, Y.; Sun, J.; Bao, J.; Zhu, T. BK polyomavirus infection promotes growth and aggressiveness in bladder cancer. Virol. J. 2020, 17, 139. [Google Scholar] [CrossRef]
- Papadimitriou, J.C.; Randhawa, P.; Rinaldo, C.H.; Drachenberg, C.B.; Alexiev, B.; Hirsch, H.H. BK Polyomavirus Infection and Renourinary Tumorigenesis. Am. J. Transpl. 2016, 16, 398–406. [Google Scholar] [CrossRef]
- Borgogna, C.; Albertini, S.; Martuscelli, L.; Poletti, F.; Volpe, A.; Merlotti, G.; Cantaluppi, V.; Boldorini, R.; Gariglio, M. Evidence of BK Polyomavirus Infection in Urothelial but not Renal Tumors from a Single Center Cohort of Kidney Transplant Recipients. Viruses 2021, 13, 56. [Google Scholar] [CrossRef] [PubMed]
- Sirohi, D.; Vaske, C.; Sanborn, Z.; Smith, S.C.; Don, M.D.; Lindsey, K.G.; Federman, S.; Vankalakunti, M.; Koo, J.; Bose, S.; et al. Polyoma virus-associated carcinomas of the urologic tract: A clinicopathologic and molecular study. Mod. Pathol. 2018, 31, 1429–1441. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chu, Y.H.; Zhong, W.; Rehrauer, W.; Pavelec, D.M.; Ong, I.M.; Arjang, D.; Patel, S.S.; Hu, R. Clinicopathologic Characterization of Post-Renal Transplantation BK Polyomavirus-Associated Urothelial CarcinomaSingle Institutional Experience. Am. J. Clin. Pathol. 2020, 153, 303–314. [Google Scholar] [CrossRef] [PubMed]
- Kenan, D.J.; Mieczkowski, P.A.; Latulippe, E.; Cote, I.; Singh, H.K.; Nickeleit, V. BK Polyomavirus Genomic Integration and Large T Antigen Expression: Evolving Paradigms in Human Oncogenesis. Am. J. Transplant. 2017, 17, 1674–1680. [Google Scholar] [CrossRef] [Green Version]
- Kenan, D.J.; Mieczkowski, P.A.; Burger-Calderon, R.; Singh, H.K.; Nickeleit, V. The oncogenic potential of BK-polyomavirus is linked to viral integration into the human genome. J. Pathol. 2015, 237, 379–389. [Google Scholar] [CrossRef]
- Wang, H.H.; Liu, K.L.; Chu, S.H.; Tian, Y.C.; Lai, P.C.; Chiang, Y.J. BK virus infection in association with posttransplant urothelial carcinoma. Transpl. Proc. 2009, 41, 165–166. [Google Scholar] [CrossRef]
- Dao, M.; Pecriaux, A.; Bessede, T.; Durrbach, A.; Mussini, C.; Guettier, C.; Ferlicot, S. BK virus-associated collecting duct carcinoma of the renal allograft in a kidney-pancreas allograft recipient. Oncotarget 2018, 9, 15157–15163. [Google Scholar] [CrossRef] [Green Version]
- Yin, W.Y.; Lee, M.C.; Lai, N.S.; Lu, M.C. BK virus as a potential oncovirus for bladder cancer in a renal transplant patient. J. Med. Assoc. 2015, 114, 373–374. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gupta, G.; Kuppachi, S.; Kalil, R.S.; Buck, C.B.; Lynch, C.F.; Engels, E.A. Treatment for presumed BK polyomavirus nephropathy and risk of urinary tract cancers among kidney transplant recipients in the United States. Am. J. Transplant. 2018, 18, 245–252. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liu, S.; Chaudhry, M.R.; Berrebi, A.A.; Papadimitriou, J.C.; Drachenberg, C.B.; Haririan, A.; Alexiev, B.A. Polyomavirus Replication and Smoking Are Independent Risk Factors for Bladder Cancer After Renal Transplantation. Transplantation 2017, 101, 1488–1494. [Google Scholar] [CrossRef]
- Elfadawy, N.; Yamada, M.; Sarabu, N. Management of BK Polyomavirus Infection in Kidney and Kidney-Pancreas Transplant Recipients: A Review Article. Infect. Dis. Clin. North. Am. 2018, 32, 599–613. [Google Scholar] [CrossRef]
- Drachenberg, C.B.; Papadimitriou, J.C.; Chaudhry, M.R.; Ugarte, R.; Mavanur, M.; Thomas, B.; Cangro, C.; Costa, N.; Ramos, E.; Weir, M.R.; et al. Histological Evolution of BK Virus-Associated Nephropathy: Importance of Integrating Clinical and Pathological Findings. Am. J. Transplant. 2017, 17, 2078–2091. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nankivell, B.J.; Renthawa, J.; Sharma, R.N.; Kable, K.; O’Connell, P.J.; Chapman, J.R. BK Virus Nephropathy: Histological Evolution by Sequential Pathology. Am. J. Transplant. 2017, 17, 2065–2077. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Huang, G.; Wu, L.W.; Yang, S.C.; Fei, J.G.; Deng, S.X.; Li, J.; Chen, G.D.; Fu, Q.; Deng, R.H.; Qiu, J.; et al. Factors Influencing Graft Outcomes Following Diagnosis of Polyomavirus -Associated Nephropathy after Renal Transplantation. PLoS ONE 2015, 10, e0142460. [Google Scholar] [CrossRef] [Green Version]
- Vasudev, B.; Hariharan, S.; Hussain, S.A.; Zhu, Y.R.; Bresnahan, B.A.; Cohen, E.P. BK virus nephritis: Risk factors, timing, and outcome in renal transplant recipients. Kidney Int. 2005, 68, 1834–1839. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, M.; Zhou, Q.; Wang, H.; Chen, Y.; Chen, J. An application of the 2018 Banff Classification for BK polyomavirus-associated nephropathy in renal transplantation. Transpl. Infect. Dis. 2020, e13557. [Google Scholar]
- Chapman, J.R.; Webster, A.C. Cancer after renal transplantation: The next challenge. Am. J. Transplant. 2004, 4, 841–842. [Google Scholar] [CrossRef] [PubMed]
- Kapoor, A. Malignancy in kidney transplant recipients. Drugs 2008, 68, 11–19. [Google Scholar] [CrossRef] [PubMed]
- Chung, M.C.; Wu, M.J.; Chang, C.H.; Muo, C.H.; Yu, T.M.; Ho, H.C.; Shu, K.H.; Chung, C.J. Increased risk of post-transplant malignancy and mortality in transplant tourists: A nationwide population-based cohort study in Taiwan. Med. (Baltim.) 2014, 93, e344. [Google Scholar] [CrossRef]
- Collett, D.; Mumford, L.; Banner, N.R.; Neuberger, J.; Watson, C. Comparison of the incidence of malignancy in recipients of different types of organ: A UK Registry audit. Am. J. Transplant. 2010, 10, 1889–1896. [Google Scholar] [CrossRef]
- Matsuzaki, K.; Murata, M.; Yoshida, K.; Sekimoto, G.; Uemura, Y.; Sakaida, N.; Kaibori, M.; Kamiyama, Y.; Nishizawa, M.; Fujisawa, J.; et al. Chronic inflammation associated with hepatitis C virus infection perturbs hepatic transforming growth factor beta signaling, promoting cirrhosis and hepatocellular carcinoma. Hepatology 2007, 46, 48–57. [Google Scholar] [CrossRef] [PubMed]
- Vedham, V.; Verma, M. Cancer-associated infectious agents and epigenetic regulation. Methods Mol. Biol. 2015, 1238, 333–354. [Google Scholar]
- Khoury, J.D.; Tannir, N.M.; Williams, M.D.; Chen, Y.; Yao, H.; Zhang, J.; Thompson, E.J.; Network, T.; Meric-Bernstam, F.; Medeiros, L.J.; et al. Landscape of DNA virus associations across human malignant cancers: Analysis of 3,775 cases using RNA-Seq. J. Virol. 2013, 87, 8916–8926. [Google Scholar] [CrossRef] [PubMed] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Total n = 244 | BKPyVAN n = 17 | Non-BKPyVAN n = 227 | p Value | |
|---|---|---|---|---|
| Gender (male) | 124 (50.8%) | 12 (70.6%) | 112 (49.3%) | 0.13 |
| Age (years old) | 55.2 ± 13.1 | 48.4 ± 13.0 | 55.7 ± 12.9 | 0.038 |
| Diabetes | 65 (26.6%) | 4 (23.5%) | 61 (26.9%) | 1.0 |
| Living related donor | 65 (26.6%) | 3 (17.6%) | 62 (27.3%) | 0.57 |
| Dialysis duration (year) | 4.3 ± 4.3 | 5.8 ± 6.0 | 4.1 ± 4.1 | 0.284 |
| Hepatitis virus B | 21 (8.6%) | 0 (0%) | 21 (9.3%) | 0.38 |
| Hepatitis virus C | 31 (12.7%) | 2 (11.8%) | 29 (12.8%) | 1.0 |
| Creatinine (mg/dL) | 3.3 ± 3.1 | 5.7 ± 3.1 | 3.1 ± 3.0 | 0.002 |
| eGFR (mL/min/1.73 m2) | 40 ± 32 | 16 ± 15 | 41 ± 32 | <0.0001 |
| Acute rejection episode | 67 (27.5%) | 1 (5.9%) | 66 (29.1%) | 0.047 |
| Allograft loss | 55 (22.5%) | 9 (52.9%) | 46 (20.3%) | 0.004 |
| Urinary tract cancers a | 20 (8.2%) | 5 (29.4%) | 15 (6.6%) | 0.007 |
| Cancers other than urinary tract cancers | 11 (4.5%) | 0 (0%) | 11 (4.8%) | 1.0 |
| Any cancer | 31 (12.7%) | 5 (29.4%) | 26 (11.5%) | 0.048 |
| Mortality b | 38 (15.6%) | 3 (17.6%) | 35 (15.4%) | 0.734 |
| Total n = 244 | BKPyVAN n = 17 | Non-BKPyVAN n = 227 | |
|---|---|---|---|
| Urinary tract cancer | |||
| Renal cell carcinoma | 3 | 1 | 2 |
| Pelvis/ureter | 1 | 0 | 1 |
| Bladder | 16 | 4 | 12 |
| Prostate | 0 | 0 | 0 |
| Total | 20 (8.2%) | 5 (29.4%) | 15 (6.6%) |
| Other cancers | |||
| Hepatocellular carcinoma | 2 | 0 | 2 |
| Lymphoma | 2 | 0 | 2 |
| Cervical cancer | 2 | 0 | 2 |
| Endometrial cancer | 1 | 0 | 1 |
| Breast cancer | 1 | 0 | 1 |
| Colon cancer | 1 | 0 | 1 |
| Lung cancer | 1 | 0 | 1 |
| Kaposi sarcoma | 1 | 0 | 1 |
| Total | 11 (4.5%) | 0 (0%) | 11 (4.8%) |
| Factor | RR | Hazard Ratio (95% CI) | p Value |
|---|---|---|---|
| Univariate logistic regression | |||
| Sex (male) | 0.775 | 0.309–1.044 | 0.588 |
| Age | 1.036 | 0.995–1.079 | 0.085 |
| Living donor | 0.668 | 0.215–2.077 | 0.486 |
| Pre-transplant dialysis duration | 1.049 | 0.945–1.164 | 0.369 |
| Diabetes | 0.461 | 0.131–1.628 | 0.229 |
| HBV | 1.000 | 0.998 | |
| HCV | 1.823 | 0.568–5.860 | 0.313 |
| eGFR | 0.980 | 0.961–1.000 | 0.053 |
| Acute rejection | 0.441 | 0.125–1.557 | 0.203 |
| BKPyVAN | 5.889 | 1.833–18.923 | 0.003 |
| Multivariate logistic regression | |||
| Age | 1.062 | 1.006–1.122 | 0.030 |
| BKPyVAN | 6.459 | 1.131–36.889 | 0.036 |
| Factor | OR | Hazard Ratio (95% CI) | p Value |
|---|---|---|---|
| Univariate logistic regression | |||
| Sex (male) | 0.798 | 0.237–2.689 | 0.716 |
| Age | 1.030 | 0.977–1.085 | 0.269 |
| Living donor | 0.000 | 0.997 | |
| Pre-transplant dialysis duration | 1.048 | 0.906–1.213 | 0.529 |
| Diabetes | 0.264 | 0.033–2.105 | 0.209 |
| HBV | 4.479 | 1.092–18.372 | 0.037 |
| HCV | 0.677 | 0.084–5.477 | 0.714 |
| eGFR | 0.993 | 0.973–1.015 | 0.539 |
| Acute rejection | 0.990 | 0.255–3.849 | 0.989 |
| BKPyVAN | 0.000 | 1.833–18.923 | 0.999 |
| Multivariate logistic regression | |||
| HBV | 5.205 | 0.782–34.649 | 0.088 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Li, Y.-J.; Wu, H.-H.; Chen, C.-H.; Wang, H.-H.; Chiang, Y.-J.; Hsu, H.-H.; Pang, S.-T.; Wang, R.Y.L.; Tian, Y.-C. High Incidence and Early Onset of Urinary Tract Cancers in Patients with BK Polyomavirus Associated Nephropathy. Viruses 2021, 13, 476. https://doi.org/10.3390/v13030476
Li Y-J, Wu H-H, Chen C-H, Wang H-H, Chiang Y-J, Hsu H-H, Pang S-T, Wang RYL, Tian Y-C. High Incidence and Early Onset of Urinary Tract Cancers in Patients with BK Polyomavirus Associated Nephropathy. Viruses. 2021; 13(3):476. https://doi.org/10.3390/v13030476
Chicago/Turabian StyleLi, Yi-Jung, Hsin-Hsu Wu, Cheng-Hsu Chen, Hsu-Han Wang, Yang-Jen Chiang, Hsiang-Hao Hsu, See-Tong Pang, Robert Y. L. Wang, and Ya-Chung Tian. 2021. "High Incidence and Early Onset of Urinary Tract Cancers in Patients with BK Polyomavirus Associated Nephropathy" Viruses 13, no. 3: 476. https://doi.org/10.3390/v13030476