
Distribution of Human Papillomavirus (HPV) Genotypes in HIV-Negative and HIV-Positive Women with Cervical Intraepithelial Lesions in the Eastern Cape Province, South Africa


Abstract
:1. Introduction
2. Material and Methods
2.1. Study Population
2.2. Detection of HPV Genotypes
2.3. Data Analysis
3. Results
3.1. Description of Study Participants
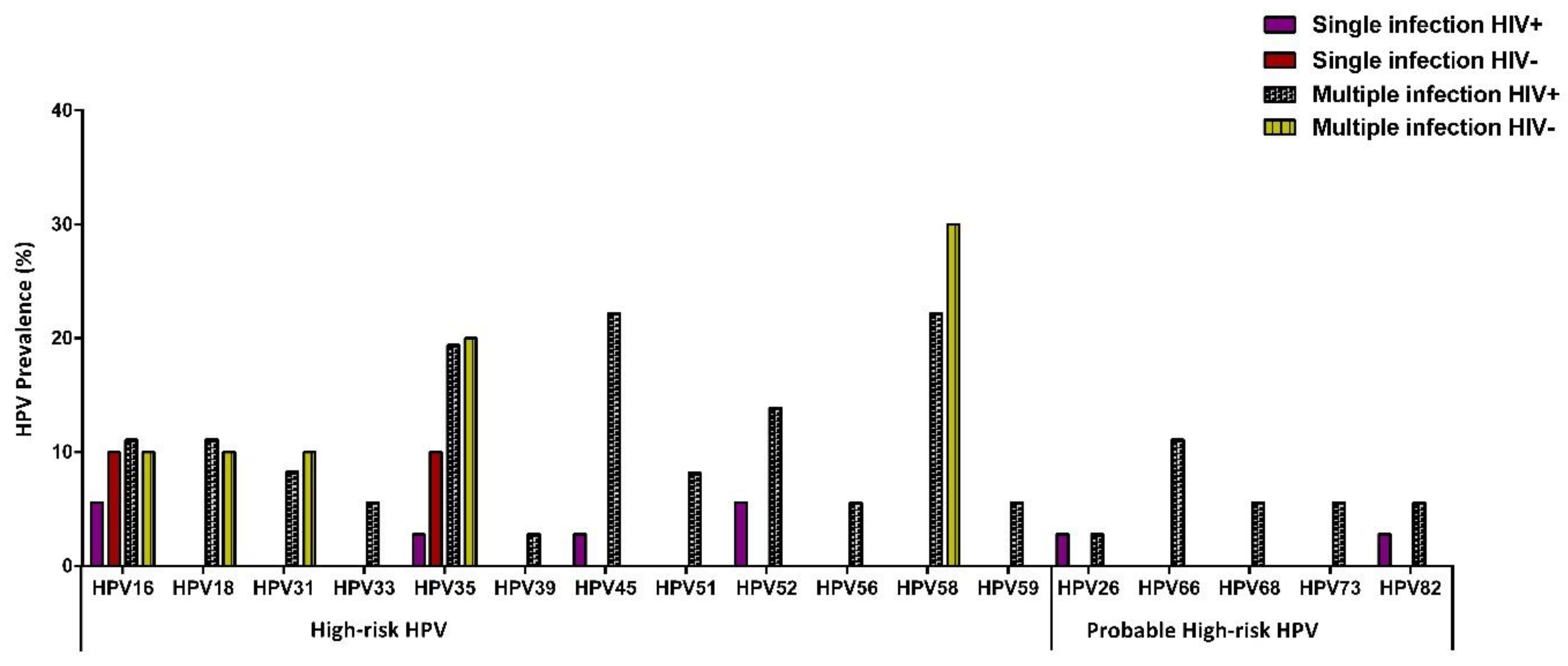
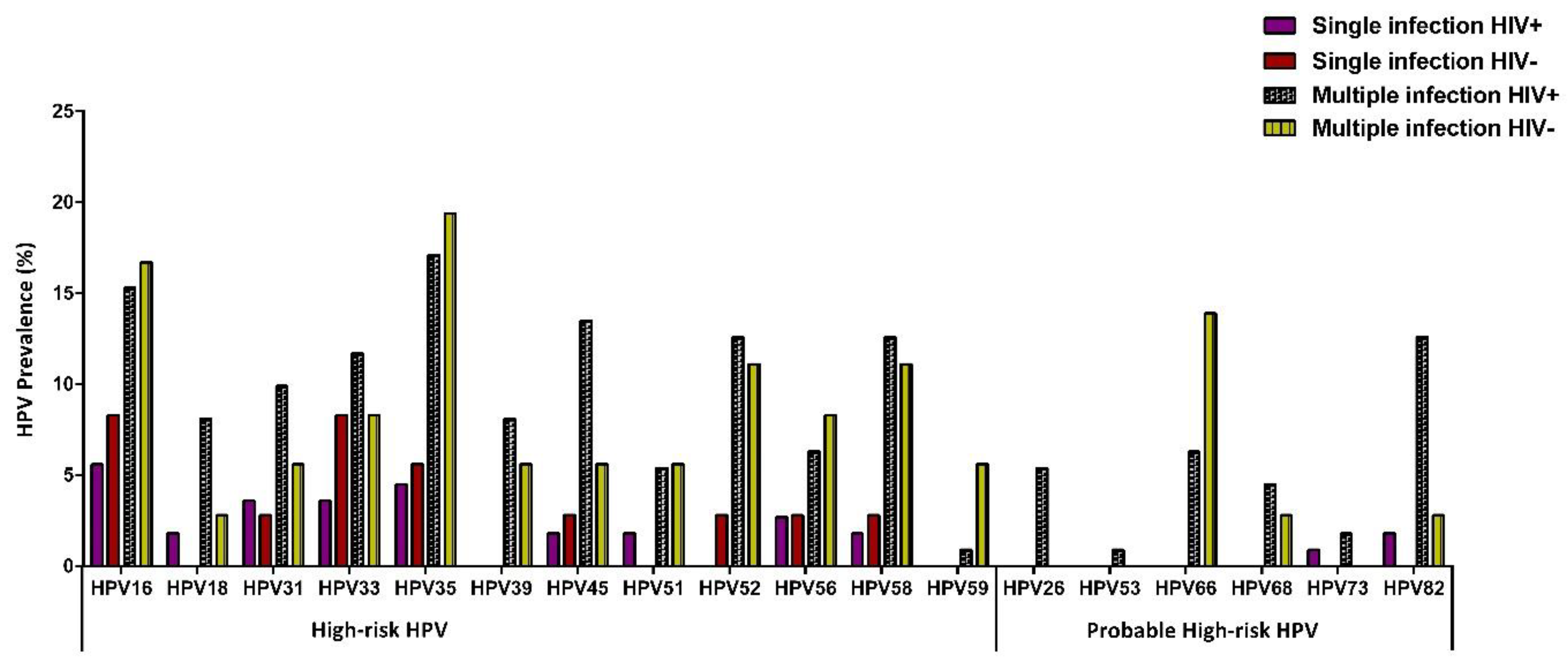
3.2. HPV Prevalence According to HIV Status
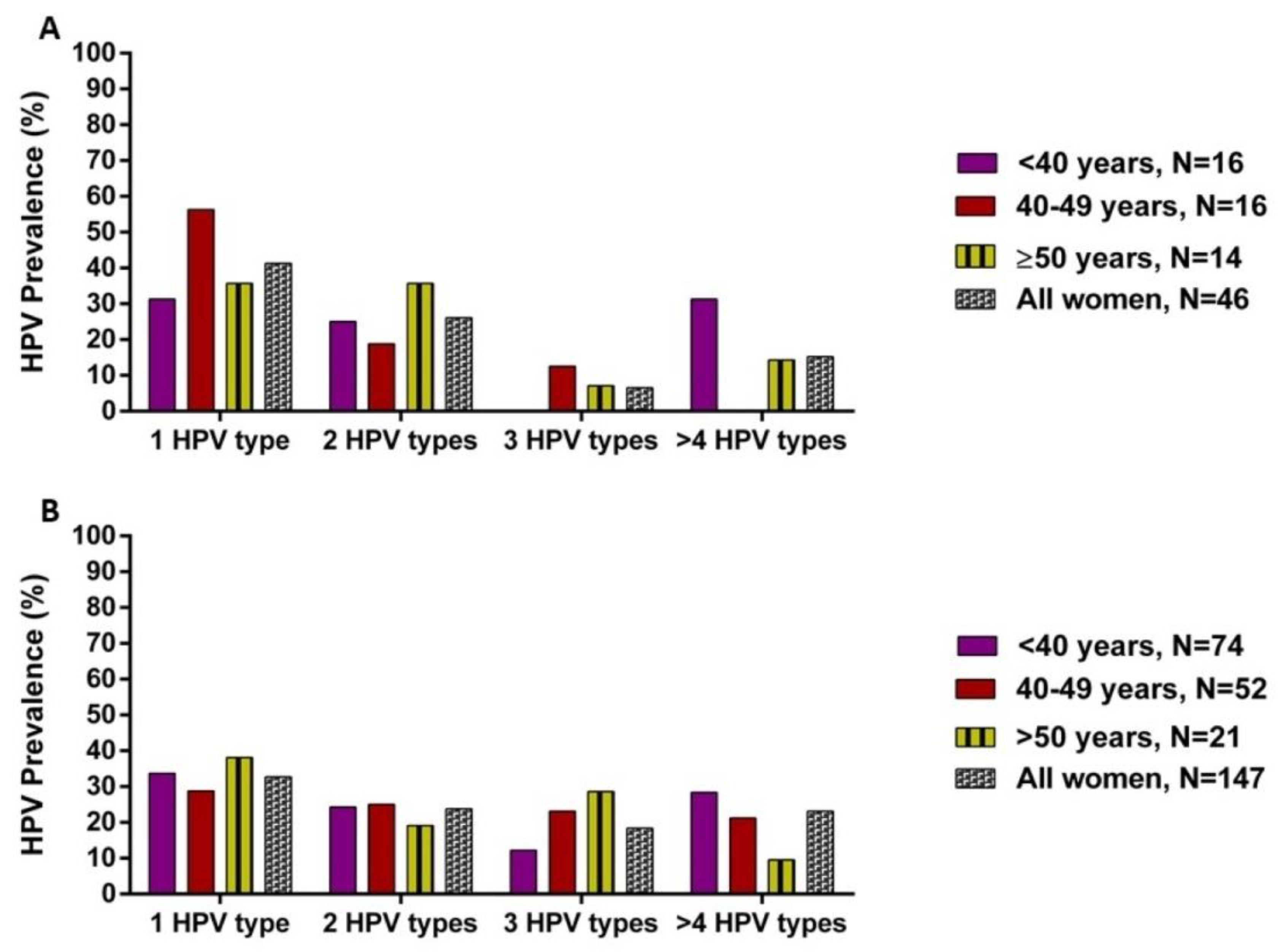
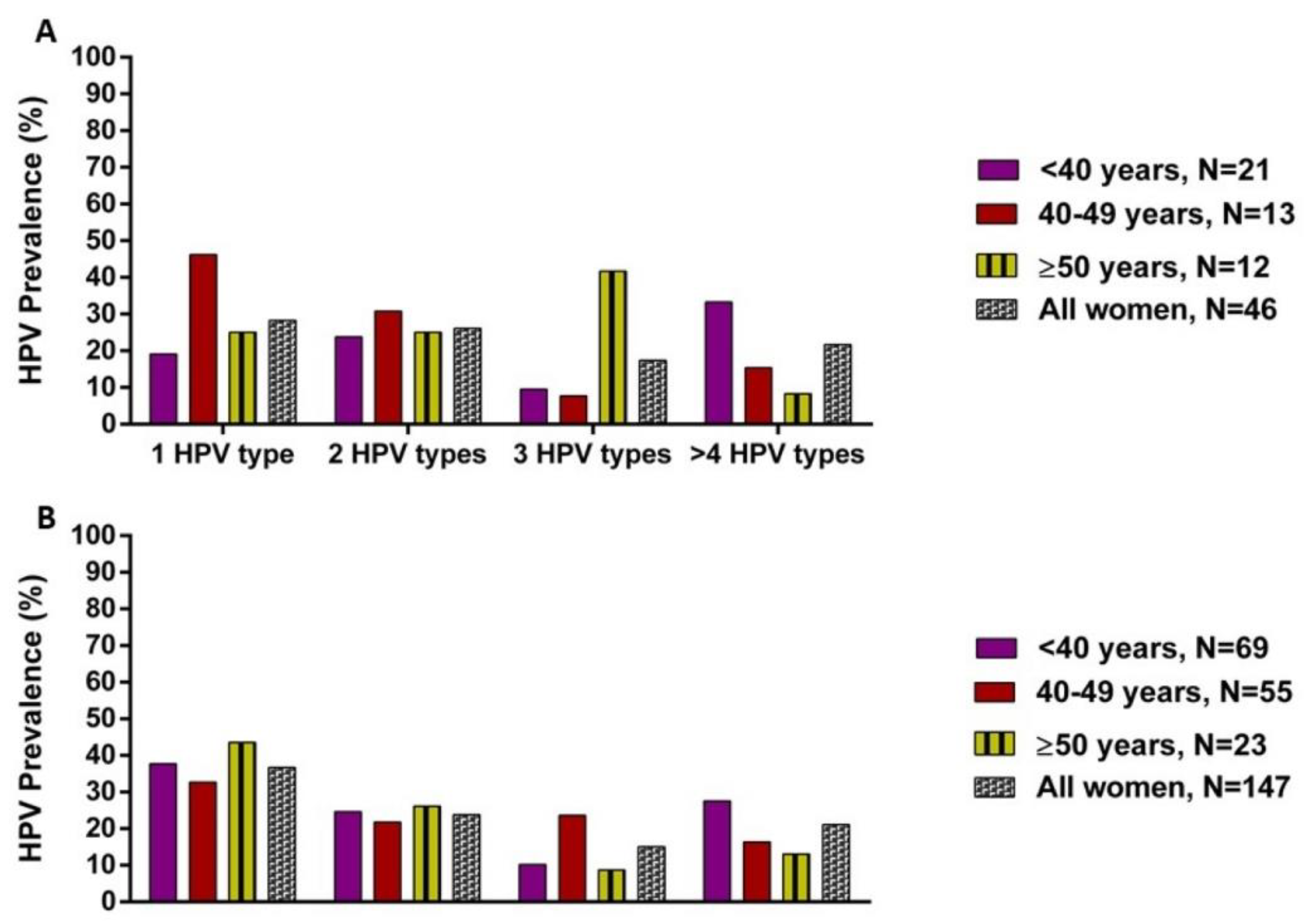
3.3. HPV Distribution According to Cervical Intraepithelial Lesions and HIV Status
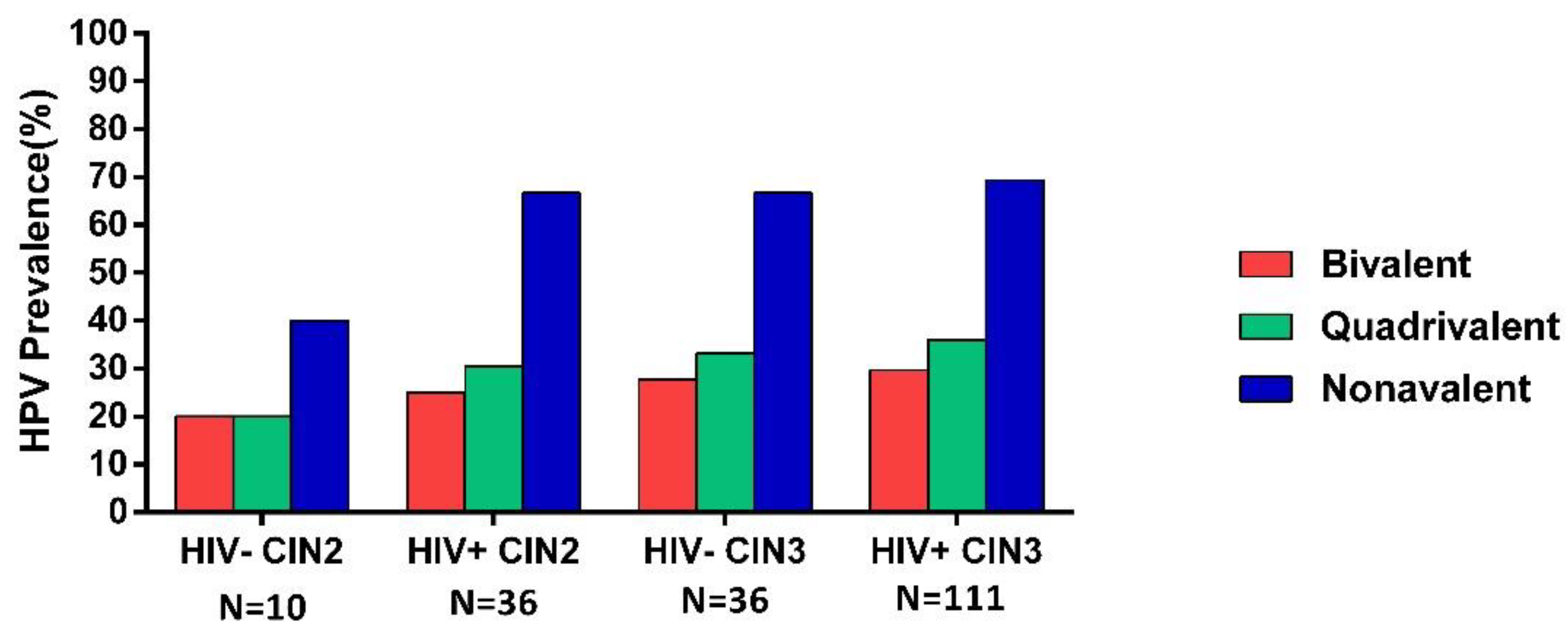
3.4. HPV Prevalence According to Vaccine HPV Types
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
References
- Avert. HIV and AIDS in East and Southern Africa Regional Overview. 2019. Available online: https://wwwavertorg/printpdf/node/393 (accessed on 31 October 2020).
- WHO. HIV/AIDS: Data and Statistics. 2019. Available online: https://wwwwhoint/hiv/data/en/ (accessed on 31 October 2020).
- UNAIDS. Aidsinfo. 2019. Available online: http://aidsinfounaidsorg/ (accessed on 31 October 2020).
- Human Sciences Research Council H. The Fifth South African National HIV Prevalence, Incidence, Behaviour and Communication Survey; HIV Impact Assessment Summary Report Cape Town; HSRC Press: Cape Town, South Africa, 2018. [Google Scholar]
- Blattner, W.A.; Nowak, R.G. Epidemiology of AIDS-Defining Malignancies. In Encyclopedia of AIDS; Hope, T.J., Stevenson, M., Richman, D., Eds.; Springer: New York, NY, USA, 2013; pp. 1–12. [Google Scholar]
- Stelzle, D.; Tanaka, L.F.; Lee, K.K.; Khalil, A.I.; Baussano, I.; Shah, A.S.V.; McAllister, D.A.; Gottlieb, S.L.; Klug, S.J.; Winkler, A.S.; et al. Estimates of the global burden of cervical cancer associated with HIV. Lancet Glob. Health 2020, 9, e161–e169. [Google Scholar] [CrossRef]
- Rohner, E.; Sengayi, M.; Goeieman, B.; Michelow, P.; Firnhaber, C.; Maskew, M.; Bohlius, J. Cervical cancer risk and impact of Pap-based screening in HIV-positive women on antiretroviral therapy in Johannesburg, South Africa. Int. J. Cancer 2017, 141, 488–496. [Google Scholar] [CrossRef] [Green Version]
- Zur Hausen, H. Papillomaviruses and cancer: From basic studies to clinical application. Nat. Rev. Cancer 2002, 2, 342–350. [Google Scholar] [CrossRef]
- Jemal, A.; Bray, F.; Center, M.M.; Ferlay, J.; Ward, E.; Forman, D. Global cancer statistics. CA Cancer J. Clin. 2011, 61, 69–90. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liu, G.; Sharma, M.; Tan, N.; Barnabas, R.V. HIV-positive women have higher risk of human papilloma virus infection, precancerous lesions, and cervical cancer. AIDS 2018, 32, 795–808. [Google Scholar] [CrossRef] [PubMed]
- Marembo, T.; Mandishora, R.D.; Borok, M. Use of Multiplex Polymerase Chain Reaction for Detection of High-Risk Human Papillomavirus Genotypes in Women Attending Routine Cervical Cancer Screening in Harare. Intervirology 2019, 62, 90–95. [Google Scholar] [CrossRef] [PubMed]
- Kriek, J.-M.; Jaumdally, S.Z.; Masson, L.; Little, F.; Mbulawa, Z.; Gumbi, P.P.; Barnabas, S.L.; Moodley, J.; Denny, L.; Coetzee, D.; et al. Female genital tract inflammation, HIV co-infection and persistent mucosal Human Papillomavirus (HPV) infections. Virology 2016, 493, 247–254. [Google Scholar] [CrossRef]
- Schettino, M.T.; Ammaturo, F.P.; Grimaldi, E.; Legnante, A.; Marcello, A.; Donnarumma, G.; Colacurci, N.; Torella, D. Persistent papillomavirus type-31 and type-45 infections predict the progression to squamous intraepithelial lesion. Taiwan J. Obstet. Gynecol. 2014, 53, 494–497. [Google Scholar] [CrossRef] [Green Version]
- Khan, M.J.; Castle, P.E.; Lorincz, A.T.; Wacholder, S.; Sherman, M.; Scott, D.R.; Rush, B.B.; Glass, A.G.; Schiffman, M. The Elevated 10-Year Risk of Cervical Precancer and Cancer in Women With Human Papillomavirus (HPV) Type 16 or 18 and the Possible Utility of Type-Specific HPV Testing in Clinical Practice. J. Natl. Cancer Inst. 2005, 97, 1072–1079. [Google Scholar] [CrossRef]
- Joura, E.A.; Giuliano, A.R.; Iversen, O.-E.; Bouchard, C.; Mao, C.; Mehlsen, J.; Moreira, E.D.; Ngan, Y.; Petersen, L.K.; Lazcano-Ponce, E.; et al. A 9-Valent HPV Vaccine against Infection and Intraepithelial Neoplasia in Women. N. Engl. J. Med. 2015, 372, 711–723. [Google Scholar] [CrossRef]
- Harper, D.M.; Vierthaler, S.L. Next Generation Cancer Protection: The Bivalent HPV Vaccine for Females. ISRN Obstet. Gynecol. 2011, 2011, 1–20. [Google Scholar] [CrossRef] [Green Version]
- Markowitz, L.E.; Tsu, V.; Deeks, S.L.; Cubie, H.; Wang, S.A.; Vicari, A.S.; Brotherton, J.M. Human Papillomavirus Vaccine Introduction—The First Five Years. Vaccine 2012, 30 (Suppl. 5), F139–F148. [Google Scholar] [CrossRef]
- Delany-Moretlwe, S.; Kelley, K.F.; James, S.; Scorgie, F.; Subedar, H.; Dlamini, N.R.; Pillay, Y.; Naidoo, N.; Chikandiwa, A.; Rees, H. Human Papillomavirus Vaccine Introduction in South Africa: Implementation Lessons From an Evaluation of the National School-Based Vaccination Campaign. Glob. Health Sci. Pract. 2018, 6, 425–438. [Google Scholar] [CrossRef] [Green Version]
- Botha, M.; Van Der Merwe, F.H.; Snyman, L.C.; Dreyer, G. The vaccine and cervical cancer screen (VACCS) project: Acceptance of human papillomavirus vaccination in a school-based programme in two provinces of South Africa. S. Afr. Med. J. 2015, 105, 40. [Google Scholar] [CrossRef]
- Segondy, M.; Kelly, H.; Magooa, M.P.; Djigma, F.; Ngou, J.; Gilham, C.; Omar, T.; Goumbri-Lompo, O.; Michelow, P.; Doutre, S.; et al. Performance of careHPV for detecting high-grade cervical intraepithelial neoplasia among women living with HIV-1 in Burkina Faso and South Africa: HARP study. Br. J. Cancer 2016, 115, 425–430. [Google Scholar] [CrossRef] [Green Version]
- Cuzick, J.; Myers, O.; Hunt, W.C.; Saslow, D.; Castle, P.E.; Kinney, W.; Waxman, A.; Robertson, M.; Wheeler, C.M.; on Behalf of the New Mexico HPV Pap Registry Steering Committee. Human papillomavirus testing 2007–2012: Co-testing and triage utilization and impact on subsequent clinical management. Int. J. Cancer 2015, 136, 2854–2863. [Google Scholar] [CrossRef] [Green Version]
- Firnhaber, C.; Mayisela, N.; Mao, L.; Williams, S.; Swarts, A.; Faesen, M.; Levin, S.; Michelow, P.; Omar, T.; Hudgens, M.G.; et al. Validation of Cervical Cancer Screening Methods in HIV Positive Women from Johannesburg South Africa. PLoS ONE 2013, 8, e53494. [Google Scholar] [CrossRef] [Green Version]
- Ronco, G.; Dillner, J.; Elfström, K.M.; Tunesi, S.; Snijders, P.J.F.; Arbyn, M.; Kitchener, H.; Segnan, N.; Gilham, C.; Giorgi-Rossi, P.; et al. Efficacy of HPV-based screening for prevention of invasive cervical cancer: Follow-up of four European randomised controlled trials. Lancet 2014, 383, 524–532. [Google Scholar] [CrossRef]
- Taku, O.; Meiring, T.L.; Gustavsson, I.; Phohlo, K.; Garcia-Jardon, M.; Mbulawa, Z.Z.A.; Businge, C.B.; Gyllensten, U.; Williamson, A.-L. Acceptability of self- collection for human papillomavirus detection in the Eastern Cape, South Africa. PLoS ONE 2020, 15, e0241781. [Google Scholar] [CrossRef] [PubMed]
- Gustavsson, I.; Sanner, K.; Lindell, M.; Strand, A.; Olovsson, M.; Wikström, I.; Wilander, E.; Gyllensten, U. Type-specific detection of high-risk human papillomavirus (HPV) in self-sampled cervicovaginal cells applied to FTA elute cartridge. J. Clin. Virol. 2011, 51, 255–258. [Google Scholar] [CrossRef] [PubMed]
- Herraez-Hernandez, E.; Alvarez, M.; Navarro-Bustos, G.; Esquivias, J.; Alonso, S.; Aneiros-Fernández, J.; Lacruz-Pelea, C.; Sanchez-Aguera, M.; Santamaria, J.S.; De Antonio, J.C.; et al. HPV Direct Flow CHIP: A new human papillomavirus genotyping method based on direct PCR from crude-cell extracts. J. Virol. Methods 2013, 193, 9–17. [Google Scholar] [CrossRef] [Green Version]
- Ramogola-Masire, D.; McGrath, C.M.; Barnhart, K.T.; Friedman, H.M.; Zetola, N.M. Subtype Distribution of Human Papillomavirus in HIV-Infected Women With Cervical Intraepithelial Neoplasia Stages 2 and 3 in Botswana. Int. J. Gynecol. Pathol. 2011, 30, 591–596. [Google Scholar] [CrossRef] [Green Version]
- McDonald, A.C.; Tergas, A.; Kuhn, L.; Denny, L.; Wright, T.C., Jr. Distribution of Human Papillomavirus Genotypes among HIV-Positive and HIV-Negative Women in Cape Town, South Africa. Front. Oncol. 2014, 4, 48. [Google Scholar] [CrossRef] [Green Version]
- Van Aardt, M.C.; Dreyer, G.; Snyman, L.C.; Richter, K.L.; Becker, P.; Mojaki, S.M. Oncogenic and incidental HPV types associated with histologically confirmed cervical intraepithelial neoplasia in HIV-positive and HIV-negative South African women. S. Afr. Med. J. 2016, 106. [Google Scholar] [CrossRef]
- Guan, P.; Howell-Jones, R.; Li, N.; Bruni, L.; De Sanjosé, S.; Franceschi, S.; Clifford, G.M. Human papillomavirus types in 115,789 HPV-positive women: A meta-analysis from cervical infection to cancer. Int. J. Cancer 2012, 131, 2349–2359. [Google Scholar] [CrossRef]
- Menon, S.; Wusiman, A.; Boily, M.C.; Kariisa, M.; Mabeya, H.; Luchters, S.; Forland, F.; Rossi, R.; Callens, S.; Broeck, D.V. Epidemiology of HPV Genotypes among HIV Positive Women in Kenya: A Systematic Review and Meta-Analysis. PLoS ONE 2016, 11, e0163965. [Google Scholar] [CrossRef]
- Sweet, K.; Bosire, C.; Sanusi, B.; Sherrod, C.J.; Kwatampora, J.; Waweru, W.; Mugo, N.; Kimani, J.; Ting, J.; Clark, J.; et al. Prevalence, incidence, and distribution of human papillomavirus types in female sex workers in Kenya. Int. J. STD AIDS 2020, 31, 109–118. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dovey de la Cour, C.; Guleria, S.; Nygård, M.; Trygvadóttir, L.; Sigurdsson, K.; Liaw, K.L.; Hortlund, M.; Lagheden, C.; Hansen, B.T.; Munk, C.; et al. Human papillomavirus types in cervical high-grade lesions or cancer among Nordic women-Potential for prevention. Cancer Med. 2019, 8, 839–849. [Google Scholar] [CrossRef] [Green Version]
- Pinheiro, M.; Gage, J.C.; Clifford, G.M.; Demarco, M.; Cheung, L.C.; Chen, Z.; Yeager, M.; Cullen, M.; Boland, J.F.; Chen, X.; et al. Association of HPV35 with cervical carcinogenesis among women of African ancestry: Evidence of viral-host interaction with implications for disease intervention. Int. J. Cancer 2020, 147, 2677–2686. [Google Scholar] [CrossRef] [PubMed]
- Howitt, B.E.; Herfs, M.; Tomoka, T.; Kamiza, S.; Gheit, T.; Tommasino, M.; Delvenne, P.; Crum, C.P.; Milner, D. Comprehensive Human Papillomavirus Genotyping in Cervical Squamous Cell Carcinomas and Its Relevance to Cervical Cancer Prevention in Malawian Women. J. Glob. Oncol. 2017, 3, 227–234. [Google Scholar] [CrossRef]
- Castellsagué, X.; Klaustermeier, J.; Carrilho, C.; Albero, G.; Sacarlal, J.; Quint, W.; Kleter, B.; Lloveras, B.; Ismail, M.R.; De Sanjosé, S.; et al. Vaccine-related HPV genotypes in women with and without cervical cancer in Mozambique: Burden and potential for prevention. Int. J. Cancer 2008, 122, 1901–1904. [Google Scholar] [CrossRef]
- Okolo, C.A.; Franceschi, S.; Adewole, I.F.; Thomas, J.; Follen, M.; Snijders, P.J.F.; Meijer, C.J.L.M.; Clifford, G.M. Human papillomavirus infection in women with and without cervical cancer in Ibadan, Nigeria. Infect. Agents Cancer 2010, 5, 24. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Denny, L.; Adewole, I.; Anorlu, R.; Dreyer, G.; Moodley, M.; Smith, T.; Snyman, L.C.; Wiredu, E.; Molijn, A.; Quint, W.; et al. Human papillomavirus prevalence and type distribution in invasive cervical cancer in sub-Saharan Africa. Int. J. Cancer 2014, 134, 1389–1398. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Clifford, G.M.; De Vuyst, H.; Tenet, V.; Plummer, M.; Tully, S.; Franceschi, S. Effect of HIV Infection on Human Papillomavirus Types Causing Invasive Cervical Cancer in Africa. JAIDS J. Acquir. Immune Defic. Syndr. 2016, 73, 332–339. [Google Scholar] [CrossRef] [Green Version]
- Van der Marel, J.; Berkhof, J.; Ordi, J.; Torné, A.; Del Pino, M.; van Baars, R.; Schiffman, M.; Wentzensen, N.; Jenkins, D.; Quint, W.G. Attributing oncogenic human papillomavirus genotypes to high-grade cervical neoplasia: Which type causes the lesion? Am. J. Surg. Pathol. 2015, 39, 496–504. [Google Scholar] [CrossRef]
- Schmitt, M.; Depuydt, C.E.; Benoy, I.; Bogers, J.P.; Antoine, J.; Arbyn, M.; Pawlita, M.; on behalf of the VALGENT Study Group. Multiple Human Papillomavirus Infections with High Viral Loads Are Associated with Cervical Lesions but Do Not Differentiate Grades of Cervical Abnormalities. J. Clin. Microbiol. 2013, 51, 1458–1464. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kaliff, M.; Sorbe, B.; Mordhorst, L.B.; Helenius, G.; Karlsson, M.G.; Lillsunde-Larsson, G. Findings of multiple HPV genotypes in cervical carcinoma are associated with poor cancer-specific survival in a Swedish cohort of cervical cancer primarily treated with radiotherapy. Oncotarget 2018, 9, 18786–18796. [Google Scholar] [CrossRef] [PubMed]
- Munagala, R.; Donà, M.G.; Rai, S.N.; Jenson, A.B.; Bala, N.; Ghim, S.J.; Gupta, R.C. Significance of multiple HPV infection in cervical cancer patients and its impact on treatment response. Int. J. Oncol. 2009, 34, 263–271. [Google Scholar] [PubMed]
- De Vuyst, H.; Chung, M.H.; Baussano, I.; Mugo, N.R.; Tenet, V.; van Kemenade, F.J.; Rana, F.S.; Sakr, S.R.; Meijer, C.J.; Snijders, P.J.; et al. Comparison of HPV DNA testing in cervical exfoliated cells and tissue biopsies among HIV-positive women in Kenya. Int. J. Cancer 2013, 133, 1441–1446. [Google Scholar] [CrossRef] [Green Version]
- Bruni, L.; Diaz, M.; Castellsagué, X.; Ferrer, E.; Bosch, F.X.; De Sanjosé, S. Cervical Human Papillomavirus Prevalence in 5 Continents: Meta-Analysis of 1 Million Women with Normal Cytological Findings. J. Infect. Dis. 2010, 202, 1789–1799. [Google Scholar] [CrossRef] [Green Version]
- Monsonego, J.; Cox, J.T.; Behrens, C.; Sandri, M.; Franco, E.L.; Yap, P.-S.; Huh, W. Prevalence of high-risk human papilloma virus genotypes and associated risk of cervical precancerous lesions in a large U.S. screening population: Data from the ATHENA trial. Gynecol. Oncol. 2015, 137, 47–54. [Google Scholar] [CrossRef] [Green Version]
- Tornesello, M.L.; Giorgi Rossi, P.; Buonaguro, L.; Buonaguro, F.M. Human Papillomavirus Infection and Cervical Neoplasia among Migrant Women Living in Italy. Front. Oncol. 2014, 4, 31. [Google Scholar] [CrossRef] [Green Version]
- Hildesheim, A.; Wang, S.S. Host and viral genetics and risk of cervical cancer: A review. Virus Res. 2002, 89, 229–240. [Google Scholar] [CrossRef]
- Serrano, B.; Alemany, L.; De Ruíz, P.A.; Tous, S.; Lima, M.A.; Bruni, L.; Jain, A.; Clifford, G.M.; Qiao, Y.L.; Weiss, T.; et al. Potential impact of a 9-valent HPV vaccine in HPV-related cervical disease in 4 emerging countries (Brazil, Mexico, India and China). Cancer Epidemiol. 2014, 38, 748–756. [Google Scholar] [CrossRef] [Green Version]
- Garland, S.M.; Pitisuttithum, P.; Ngan, H.Y.S.; Cho, C.-H.; Lee, C.-Y.; Chen, C.-A.; Yang, Y.C.; Chu, T.-Y.; Twu, N.-F.; Samakoses, R.; et al. Efficacy, Immunogenicity, and Safety of a 9-Valent Human Papillomavirus Vaccine: Subgroup Analysis of Participants From Asian Countries. J. Infect. Dis. 2018, 218, 95–108. [Google Scholar] [CrossRef]
- Huh, W.K.; Joura, E.A.; Giuliano, A.R.; Iversen, O.-E.; De Andrade, R.P.; Ault, K.A.; Bartholomew, D.; Cestero, R.M.; Fedrizzi, E.N.; Hirschberg, A.L.; et al. Final efficacy, immunogenicity, and safety analyses of a nine-valent human papillomavirus vaccine in women aged 16–26 years: A randomised, double-blind trial. Lancet 2017, 390, 2143–2159. [Google Scholar] [CrossRef]
- Ruiz-Sternberg, Á.M.; Moreira, E.D., Jr.; Restrepo, J.A.; Lazcano-Ponce, E.; Cabello, R.; Silva, A.; Andrade, R.; Revollo, F.; Uscanga-Sánchez, S.R.; Victori, A.; et al. Efficacy, immunogenicity, and safety of a 9-valent human papillomavirus vaccine in Latin American girls, boys, and young women. Papillomavirus Res. 2018, 5, 63–74. [Google Scholar] [CrossRef]
- Kreimer, A.R.; Struyf, F.; Del Rosario-Raymundo, M.R.; Hildesheim, A.; Skinner, S.R.; Wacholder, S.; Garland, S.M.; Herrero, R.; David, M.P.; Wheeler, C.M.; et al. Efficacy of fewer than three doses of an HPV-16/18 AS04-adjuvanted vaccine: Combined analysis of data from the Costa Rica Vaccine and PATRICIA Trials. Lancet Oncol. 2015, 16, 775–786. [Google Scholar] [CrossRef] [Green Version]
- Skinner, S.R.; Apter, D.; De Carvalho, N.; Harper, D.M.; Konno, R.; Paavonen, J.; Romanowski, B.; Roteli-Martins, C.; Burlet, N.; Mihalyi, A.; et al. Human papillomavirus (HPV)-16/18 AS04-adjuvanted vaccine for the prevention of cervical cancer and HPV-related diseases. Expert Rev. Vaccines 2016, 15, 367–387. [Google Scholar] [CrossRef]
- Malagón, T.; Drolet, M.; Boily, M.-C.; Franco, E.L.; Jit, M.; Brisson, J.; Brisson, M. Cross-protective efficacy of two human papillomavirus vaccines: A systematic review and meta-analysis. Lancet Infect. Dis. 2012, 12, 781–789. [Google Scholar] [CrossRef]
- Bogaards, J.A.; Van Der Weele, P.; Woestenberg, P.J.; Van Benthem, B.H.B.; King, A.J. Bivalent Human Papillomavirus (HPV) Vaccine Effectiveness Correlates With Phylogenetic Distance From HPV Vaccine Types 16 and 18. J. Infect. Dis. 2019, 220, 1141–1146. [Google Scholar] [CrossRef]
- Tsang, S.H.; Sampson, J.N.; Schussler, J.; Porras, C.; Wagner, S.; Boland, J.; Cortes, B.; Lowy, D.R.; Schiller, J.T.; Schiffman, M.; et al. Durability of Cross-Protection by Different Schedules of the Bivalent HPV Vaccine: The CVT Trial. J. Natl. Cancer Inst. 2020, 112, 1030–1037. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brown, D.R.; Kjaer, S.K.; Sigurdsson, K.; Iversen, O.; Hernandez-Avila, M.; Wheeler, C.M.; Perez, G.; Koutsky, L.A.; Tay, E.H.; Garcia, P.; et al. The Impact of Quadrivalent Human Papillomavirus (HPV; Types 6, 11, 16, and 18) L1 Virus-Like Particle Vaccine on Infection and Disease Due to Oncogenic Nonvaccine HPV Types in Generally HPV-Naive Women Aged 16–26 Years. J. Infect. Dis. 2009, 199, 926–935. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | % (n/N) |
|---|---|
| Age in years: Median (IQR) | 40 (33–48) |
| HIV Status | |
| No | 23.8% (46/193) |
| Yes | 76.2% (147/193) |
| Age categories | |
| 18–29 years | 11.4% (22/193) |
| 30–39 years | 35.2% (68/193) |
| 40–49 years | 35.2% (68/193) |
| ≥50 years | 18.1% (35/193) |
| Highest level of education attained | |
| Never/primary | 29.5% (57/193) |
| High school/university | 70.5% (136/193) |
| Household income | |
| <$139.36 | 75.1% (145/193) |
| ≥$139.36 | 22.8% (44/193) |
| Smoking status | |
| Never | 93.3% (180/193) |
| Former/current smoker | 6.2% (12/193) |
| Age at first sexual experience | |
| <16 years | 21.2% (41/193) |
| 16–18 years | 53.9% (104/193) |
| ≥18 years | 24.9% (48/193) |
| Lifetime sexual partners | |
| 1 | 15.0% (29/193) |
| 2 | 21.8% (42/193) |
| ≥3 | 62.7% (121/193) |
| Cytology | |
| ASCUS/ASCU-H/AGC-NOS | 13.5% (26/193) |
| LSIL | 9.3% (18/193) |
| HSIL | 75.1% (145/193) |
| Variables | HIV-Negative, N = 46 | HIV-Positive, N = 147 | OR (95%CI) | p-Value |
|---|---|---|---|---|
| Any type | 89.1% (41/46) | 98.0% (144/147) | 0.17 (0.039–0.745) | 0.012 |
| Single infection | 41.3% (19/46) | 32.7% (48/147) | 1.45 (0.735–2.867) | 0.282 |
| Multiple infection | 47.8% (22/46) | 65.3% (96/147) | 0.49 (0.249–0.953) | 0.034 |
| HR-HPV types | 82.6% (38/46) | 87.1% (128/147) | 0.71 (0.286–1.738) | 0.446 |
| Probable HR-HPV types | 17.4% (8/46) | 30.6% (45/147) | 0.60 (0.260–1.394) | 0.233 |
| LR-HPV | 39.1% (18/46) | 44.2% (65/147) | 0.81 (0.413–1.594) | 0.543 |
| HPV Types | All Women % (n/N) | CIN2 % (n/N) | CIN3 % (n/N) |
|---|---|---|---|
| 16 | 20.7% (40/193) | 17.4% (8/46) | 21.8% (32/147) |
| 18 | 8.8% (17/193) | 10.9% (5/46) | 8.8% (12/147) |
| 31 | 11.4% (22/193) | 8.7% (4/46) | 12.2% (18/147) |
| 33 | 13.0% (25/193) | 4.4% (2/46) | 15.6% (23/147) |
| 35 | 22.8% (44/193) | 23.9% (11/46) | 22.5% (33/147) |
| 39 | 6.2% (12/193) | 2.2% (1/46) | 7.5% (11/147) |
| 45 | 15.0% (29/193) | 19.6% (9/46) | 13.6% (20/147) |
| 51 | 6.7% (13/193) | 6.5% (3/46) | 6.8% (10/147) |
| 52 | 13.5% (26/193) | 15.2% (7/46) | 12.9% (19/147) |
| 56 | 8.3% (16/193) | 4.4% (2/46) | 9.5% (14/147) |
| 58 | 16.6% (32/193) | 23.9% (11/46) | 14.3% (21/147) |
| 59 | 2.6% (5/193) | 4.4% (2/46) | 2.0% (3/147) |
| 26 | 4.1% (8/193) | 4.4% (2/46) | 4.1% (6/147) |
| 53 | 0.5% (1/193) | 0.0% (0/46) | 0.7% (1/147) |
| 66 | 8.3% (16/193) | 8.7% (4/46) | 8.2% (12/147) |
| 68 | 4.1% (8/193) | 4.4% (2/46) | 4.1% (6/147) |
| 73 | 2.6% (5/193) | 4.4% (2/46) | 2.0% (3/147) |
| 82 | 10.4% (20/193) | 6.5% (3/46) | 11.6% (17/147) |
| 6 | 6.2% (12/193) | 6.5% (3/46) | 6.1% (9/147) |
| 11 | 4.7% (9/193) | 0.0% (0/46) | 6.1% (9/147) |
| 40 | 3.6% (7/193) | 2.2% (1/46) | 4.1% (6/147) |
| 42 | 7.3% (14/193) | 8.7% (4/46) | 6.8% (10/147) |
| 43 | 2.1% (4/193) | 0.0% (0/46) | 2.7% (4/147) |
| 44/55 | 10.9% (21/193) | 17.4% (8/46) | 8.8% (13/147) |
| 54 | 3.6% (7/193) | 6.5% (3/46) | 2.7% (4/147) |
| 61 | 0.5% (1/193) | 0.0% (0/46) | 1.4% (1/147) |
| 62/81 | 15.0% (29/193) | 19.6% (9/46) | 13.6% (20/147) |
| 70 | 4.1% (8/193) | 6.5% (3/46) | 3.4% (5/147) |
| 71 | 4.7% (9/193) | 2.2% (1/46) | 5.4% (8/147) |
| 72 | 3.6% (7/193) | 6.5% (3/46) | 2.7% (4/147) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Taku, O.; Mbulawa, Z.Z.A.; Phohlo, K.; Garcia-Jardon, M.; Businge, C.B.; Williamson, A.-L. Distribution of Human Papillomavirus (HPV) Genotypes in HIV-Negative and HIV-Positive Women with Cervical Intraepithelial Lesions in the Eastern Cape Province, South Africa. Viruses 2021, 13, 280. https://doi.org/10.3390/v13020280
Taku O, Mbulawa ZZA, Phohlo K, Garcia-Jardon M, Businge CB, Williamson A-L. Distribution of Human Papillomavirus (HPV) Genotypes in HIV-Negative and HIV-Positive Women with Cervical Intraepithelial Lesions in the Eastern Cape Province, South Africa. Viruses. 2021; 13(2):280. https://doi.org/10.3390/v13020280
Chicago/Turabian StyleTaku, Ongeziwe, Zizipho Z. A. Mbulawa, Keletso Phohlo, Mirta Garcia-Jardon, Charles B. Businge, and Anna-Lise Williamson. 2021. "Distribution of Human Papillomavirus (HPV) Genotypes in HIV-Negative and HIV-Positive Women with Cervical Intraepithelial Lesions in the Eastern Cape Province, South Africa" Viruses 13, no. 2: 280. https://doi.org/10.3390/v13020280