
SARS Coronavirus-2 Microneutralisation and Commercial Serological Assays Correlated Closely for Some but Not All Enzyme Immunoassays

 , , , , , , ,
, , , , , , ,
Abstract
:1. Introduction
2. Methods
2.1. Sample Collection and Testing
2.2. Virus Microneutralisation Assay
2.3. Cobas Elecsys Anti-SARS-CoV-2
2.4. Vitros Immunodiagnostic Anti-SARS-CoV-2
2.5. Abbott Architect SARS-CoV-2 IgG
2.6. Euroimmun Anti-SARS-CoV-2 ELISA
2.7. In-House RBD Assay
2.8. Statistical Analyses
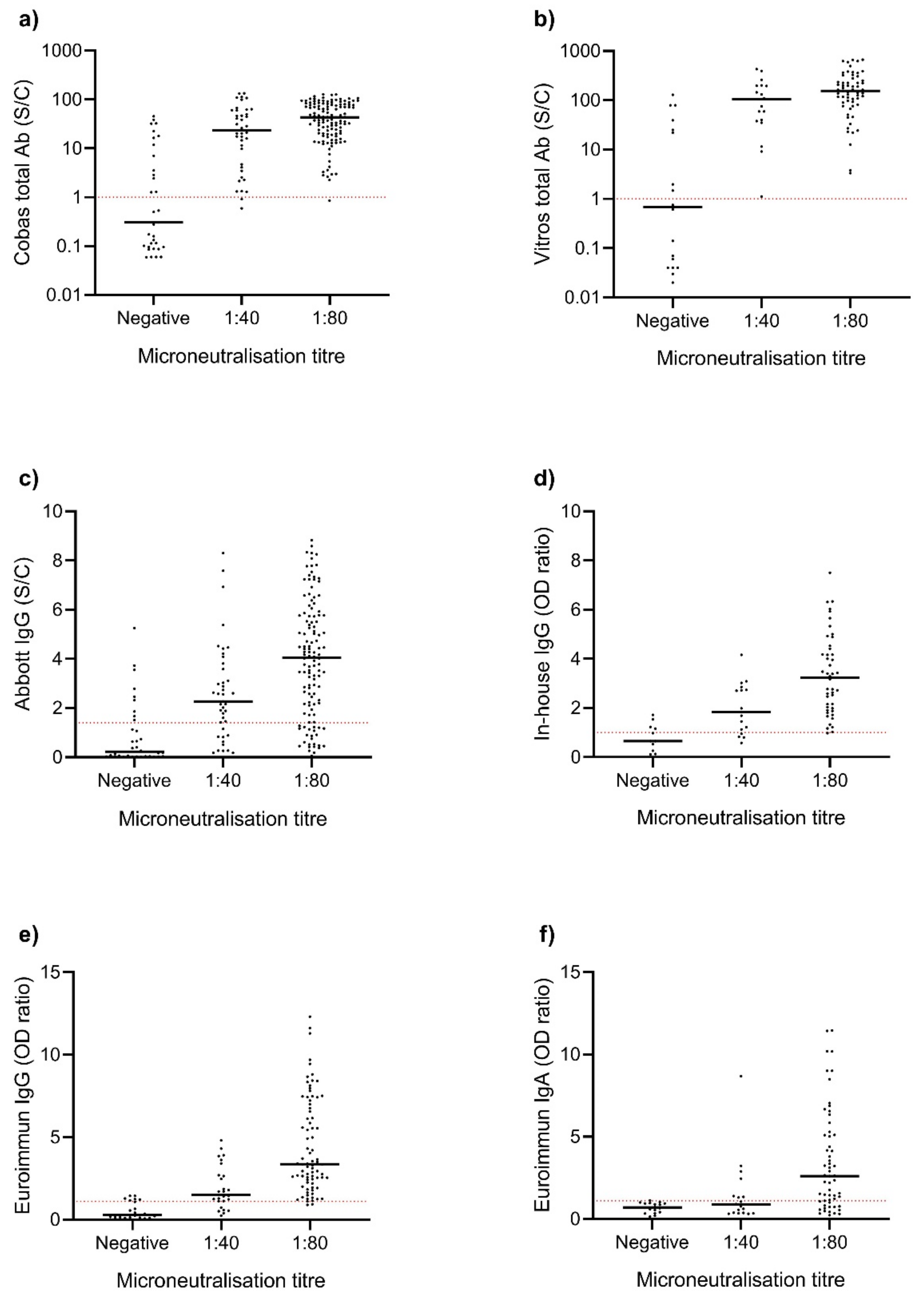
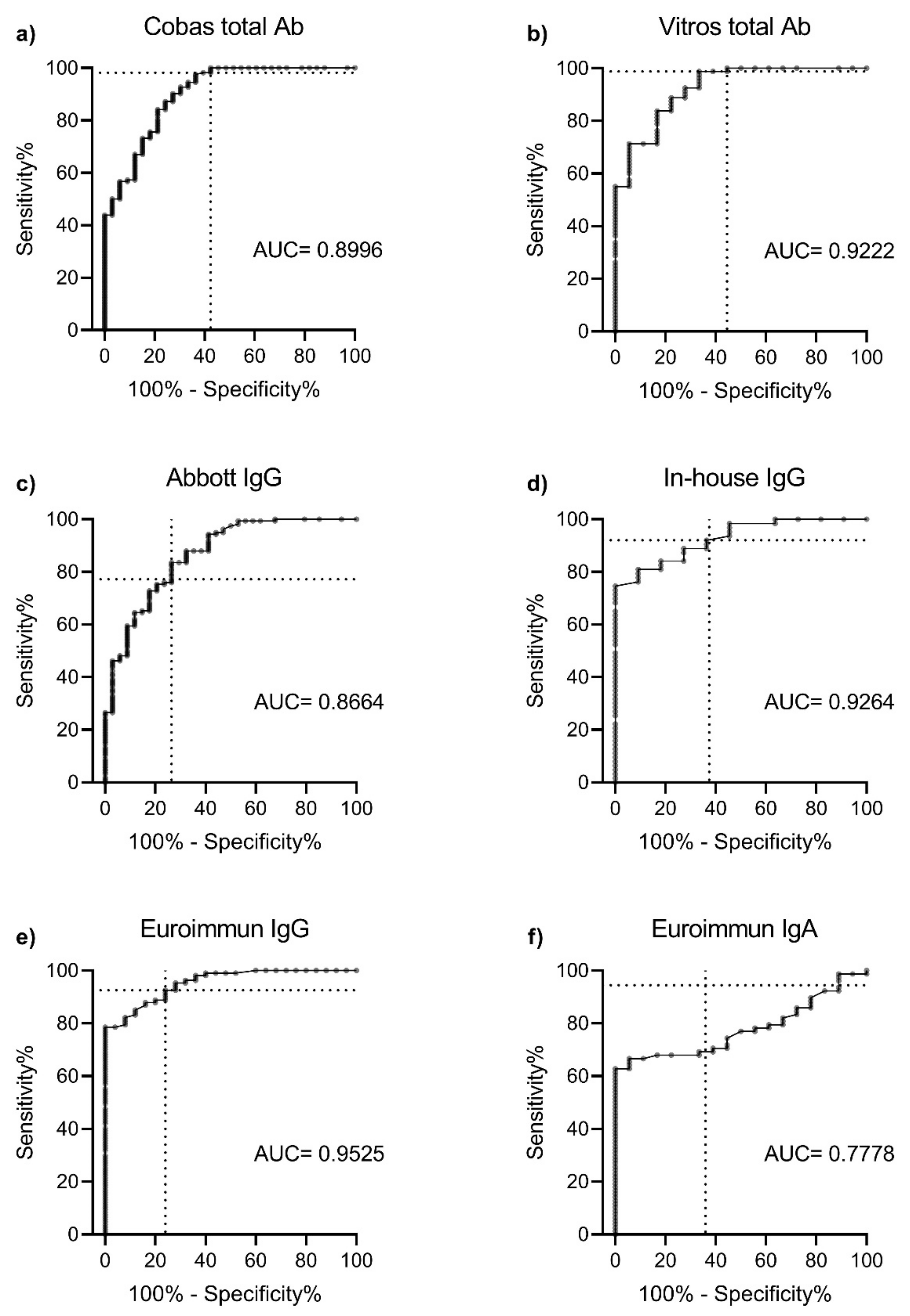
3. Results
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Petherick, A. Developing antibody tests for SARS-CoV-2. Lancet 2020, 395, 1101–1102. [Google Scholar] [CrossRef]
- Krammer, F.; Simon, V. Serology assays to manage COVID-19. Science 2020, 368, 1060–1061. [Google Scholar] [CrossRef]
- Peeling, R.W.; Wedderburn, C.J.; Garcia, P.J. Serology testing in the COVID-19 pandemic response. Lancet Infect. Dis. 2020, 20, e245–e249. [Google Scholar] [CrossRef]
- Maor, Y.; Cohen, D.; Paran, N. Compassionate use of convalescent plasma for treatment of moderate and severe pneumonia in COVID-19 patients and association with IgG antibody levels in donated plasma. EClinicalMedicine 2020, 26, 100525. [Google Scholar] [CrossRef]
- Henderson, J.R.; Taylor, R.M. Arthropod-Borne Virus Plaques in Agar Overlaid Tube Cultures. Proc. Soc. Exp. Biol. Med. 1959, 101, 257–259. [Google Scholar] [CrossRef]
- Stelzer-Braid, S.; Walker, G.J.; Aggarwal, A. Virus isolation of severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) for diagnostic and research purposes. Pathology 2020, 52, 760–763. [Google Scholar] [CrossRef] [PubMed]
- D’Cruz, R.J.; Currier, A.W.; Sampson, V.B. Laboratory Testing Methods for Novel Severe Acute Respiratory Syndrome-Coronavirus-2 (SARS-CoV-2). Front. Cell Dev. Biol. 2020, 8, 468. [Google Scholar] [CrossRef]
- Tan, C.W.; Chia, W.N.; Qin, X. A SARS-CoV-2 surrogate virus neutralization test based on antibody-mediated blockage of ACE2-spike protein-protein interaction. Nat. Biotechnol. 2020, 38, 1073–1078. [Google Scholar] [CrossRef]
- Klasse, P.J. Neutralization of Virus Infectivity by Antibodies: Old Problems in New Perspectives. Adv. Biol. 2014, 2014, 157895. [Google Scholar] [CrossRef] [Green Version]
- Houlihan, C.F.; Beale, R. The complexities of SARS-CoV-2 serology. Lancet Infect. Dis. 2020, 20, 1350–1351. [Google Scholar] [CrossRef]
- GeurtsvanKessel, C.H.; Okba, N.M.A.; Igloi, Z. An evaluation of COVID-19 serological assays informs future diagnostics and exposure assessment. Nat. Commun. 2020, 11, 3436. [Google Scholar] [CrossRef]
- Henss, L.; Scholz, T.; von Rhein, C. Analysis of humoral immune responses in SARS-CoV-2 infected patients. J. Infect. Dis. 2020, 223, 56–61. [Google Scholar] [CrossRef] [PubMed]
- Luchsinger, L.L.; Ransegnola, B.; Jin, D. Serological Assays Estimate Highly Variable SARS-CoV-2 Neutralizing Antibody Activity in Recovered COVID19 Patients. J. Clin. Microbiol. 2020, 58, 12. [Google Scholar] [CrossRef]
- Patel, E.U.; Bloch, E.M.; Clarke, W. Comparative performance of five commercially available serologic assays to detect antibodies to SARS-CoV-2 and identify individuals with high neutralizing titers. J. Clin. Microbiol. 2020, 59, e02257. [Google Scholar] [CrossRef] [PubMed]
- Weidner, L.; Gänsdorfer, S.; Unterweger, S. Quantification of SARS-CoV-2 antibodies with eight commercially available immunoassays. J. Clin. Virol. 2020, 129, 104540. [Google Scholar] [CrossRef] [PubMed]
- Jääskeläinen, A.J.; Kuivanen, S.; Kekäläinen, E. Performance of six SARS-CoV-2 immunoassays in comparison with microneutralisation. J. Clin. Virol. 2020, 129, 104512. [Google Scholar] [CrossRef]
- Brigger, D.; Horn, M.P.; Pennington, L.F. Accuracy of serological testing for SARS-CoV-2 antibodies: First results of a large mixed-method evaluation study. Allergy 2020. [Google Scholar] [CrossRef]
- Kohmer, N.; Westhaus, S.; Rühl, C.; Ciesek, S.; Rabenau, H.F. Brief clinical evaluation of six high-throughput SARS-CoV-2 IgG antibody assays. J. Clin. Virol. 2020, 129, 104480. [Google Scholar] [CrossRef]
- Kohmer, N.; Westhaus, S.; Rühl, C.; Ciesek, S.; Rabenau, H.F. Clinical performance of different SARS-CoV-2 IgG antibody tests. J. Med. Virol. 2020, 92, 2243–2247. [Google Scholar] [CrossRef]
- Marklund, E.; Leach, S.; Axelsson, H. Serum-IgG responses to SARS-CoV-2 after mild and severe COVID-19 infection and analysis of IgG non-responders. PLoS ONE 2020, 15, e0241104. [Google Scholar] [CrossRef]
- Lumley, S.F.; Eyre, D.W.; McNaughton, A.L. SARS-CoV-2 antibody prevalence, titres and neutralising activity in an antenatal cohort, United Kingdom, 14 April to 15 June 2020. Eurosurveillance 2020, 25, 2001721. [Google Scholar] [CrossRef]
- Meschi, S.; Colavita, F.; Bordi, L. Performance evaluation of Abbott ARCHITECT SARS-CoV-2 IgG immunoassay in comparison with indirect immunofluorescence and virus microneutralization test. J. Clin. Virol. 2020, 129, 104539. [Google Scholar] [CrossRef]
- Okba, N.M.A.; Müller, M.; Li, W. Severe Acute Respiratory Syndrome Coronavirus 2−Specific Antibody Responses in Coronavirus Disease Patients. Emerg. Infect. Dis. J. 2020, 26, 1478. [Google Scholar] [CrossRef]
- Grzelak, L.; Temmam, S.; Planchais, C. A comparison of four serological assays for detecting anti-SARS-CoV-2 antibodies in human serum samples from different populations. Sci. Transl. Med. 2020, 12, 559. [Google Scholar] [CrossRef]
- Padoan, A.; Bonfante, F.; Sciacovelli, L.; Cosma, C.; Basso, D.; Plebani, M. Evaluation of an ELISA for SARS-CoV-2 antibody testing: Clinical performances and correlation with plaque reduction neutralization titer. Clin. Chem. Lab. Med. 2020, 58, e247. [Google Scholar] [CrossRef]
- Peterhoff, D.; Glück, V.; Vogel, M. A highly specific and sensitive serological assay detects SARS-CoV-2 antibody levels in COVID-19 patients that correlate with neutralization. Infection 2020, 49, 75–82. [Google Scholar] [CrossRef]
- Robbiani, D.F.; Gaebler, C.; Muecksch, F. Convergent antibody responses to SARS-CoV-2 in convalescent individuals. Nature 2020, 584, 437–442. [Google Scholar] [CrossRef]
- Beavis, K.G.; Matushek, S.M.; Abeleda, A.P.F. Evaluation of the EUROIMMUN Anti-SARS-CoV-2 ELISA Assay for detection of IgA and IgG antibodies. J. Clin. Virol. 2020, 129, 104468. [Google Scholar] [CrossRef]
- Haselmann, V.; Kittel, M.; Gerhards, C. Comparison of test performance of commercial anti-SARS-CoV-2 immunoassays in serum and plasma samples. Clin. Chim. Acta 2020, 510, 73–78. [Google Scholar] [CrossRef]
- Charlton, C.L.; Kanji, J.N.; Johal, K. Evaluation of six commercial mid to high volume antibody and six point of care lateral flow assays for detection of SARS-CoV-2 antibodies. J. Clin. Microbiol. 2020, 58, e01361. [Google Scholar] [CrossRef]
- Hsueh, P.R.; Huang, L.M.; Chen, P.J.; Kao, C.L.; Yang, P.C. Chronological evolution of IgM, IgA, IgG and neutralisation antibodies after infection with SARS-associated coronavirus. Clin. Microbiol. Infect. 2004, 10, 1062–1066. [Google Scholar] [CrossRef] [Green Version]
- Ainsworth, M.; Andersson, M.; Auckland, K. Performance characteristics of five immunoassays for SARS-CoV-2: A head-to-head benchmark comparison. Lancet Infect. Dis. 2020, 20, 1390–1400. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Microneutralisation | Cobas Total Ab | Vitros Total Ab | Abbott IgG | In-House IgG | Euroimmun IgG | Euroimmun IgA | |
|---|---|---|---|---|---|---|---|
| Platform | Cell culture | ECLIA | CLIA | CMIA | ELISA | ELISA | ELISA |
| Antigen | - | N | S1 | N | RBD | S1 | S1 |
| All COVID-19 samples | |||||||
| Total | 200 | 197 | 98 | 199 | 94 | 132 | 96 |
| Positive | 166 | 175 | 88 | 139 | 79 | 106 | 51 |
| Negative | 34 | 22 | 10 | 60 | 11 | 24 | 32 |
| Equivocal | - | - | - | - | 4 | 2 | 13 |
| Positivity (%) | 83.0 | 88.8 | 89.8 | 69.8 | 87.8 | 81.5 | 61.4 |
| Sensitivity 1 (%) | - | 98.2 | 100.0 | 78.8 | 96.1 | 94.3 | 69.4 |
| Convalescent samples 2 | |||||||
| Total | 167 | 167 | 73 | 167 | 74 | 109 | 73 |
| Positive | 151 | 160 | 72 | 123 | 65 | 93 | 40 |
| Negative | 16 | 70 | 1 | 43 | 6 | 66 | 24 |
| Equivocal | - | - | - | - | 3 | 2 | 9 |
| Positivity (%) | 90.4 | 95.8 | 98.6 | 73.7 | 91.5 | 86.9 | 62.5 |
| Sensitivity 1 (%) | - | 98.7 | 100.0 | 76.8 | 95.3 | 93.6 | 65.0 |
| Negative samples | |||||||
| Total | 100 | 100 | 99 | 100 | 100 | 100 | 100 |
| Positive | 0 | 0 | 0 | 0 | 4 | 0 | 6 |
| Negative | 100 | 100 | 99 | 100 | 96 | 100 | 92 |
| Equivocal | - | - | - | - | - | - | 2 |
| Specificity 1 (%) | 100.0 | 100.0 | 100.0 | 100.0 | 96.0 | 100.0 | 93.9 |
| PPV (%) | - | 93.7 | 90.9 | 93.5 | 89.2 | 94.3 | 87.7 |
| NPV (%) | - | 97.5 | 100.0 | 78.1 | 97.2 | 95.1 | 77.3 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Walker, G.J.; Naing, Z.; Ospina Stella, A.; Yeang, M.; Caguicla, J.; Ramachandran, V.; Isaacs, S.R.; Agapiou, D.; Bull, R.A.; Stelzer-Braid, S.; et al. SARS Coronavirus-2 Microneutralisation and Commercial Serological Assays Correlated Closely for Some but Not All Enzyme Immunoassays. Viruses 2021, 13, 247. https://doi.org/10.3390/v13020247
Walker GJ, Naing Z, Ospina Stella A, Yeang M, Caguicla J, Ramachandran V, Isaacs SR, Agapiou D, Bull RA, Stelzer-Braid S, et al. SARS Coronavirus-2 Microneutralisation and Commercial Serological Assays Correlated Closely for Some but Not All Enzyme Immunoassays. Viruses. 2021; 13(2):247. https://doi.org/10.3390/v13020247
Chicago/Turabian StyleWalker, Gregory J., Zin Naing, Alberto Ospina Stella, Malinna Yeang, Joanna Caguicla, Vidiya Ramachandran, Sonia R. Isaacs, David Agapiou, Rowena A. Bull, Sacha Stelzer-Braid, and et al. 2021. "SARS Coronavirus-2 Microneutralisation and Commercial Serological Assays Correlated Closely for Some but Not All Enzyme Immunoassays" Viruses 13, no. 2: 247. https://doi.org/10.3390/v13020247