
Iron Related Biomarkers Predict Disease Severity in a Cohort of Portuguese Adult Patients during COVID-19 Acute Infection

 , , , , , ,
, , , , , ,  and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Patient Stratification
2.3. Laboratory Determinations
2.4. Statistical Analysis
3. Results
3.1. Baseline Characterization of the Patients
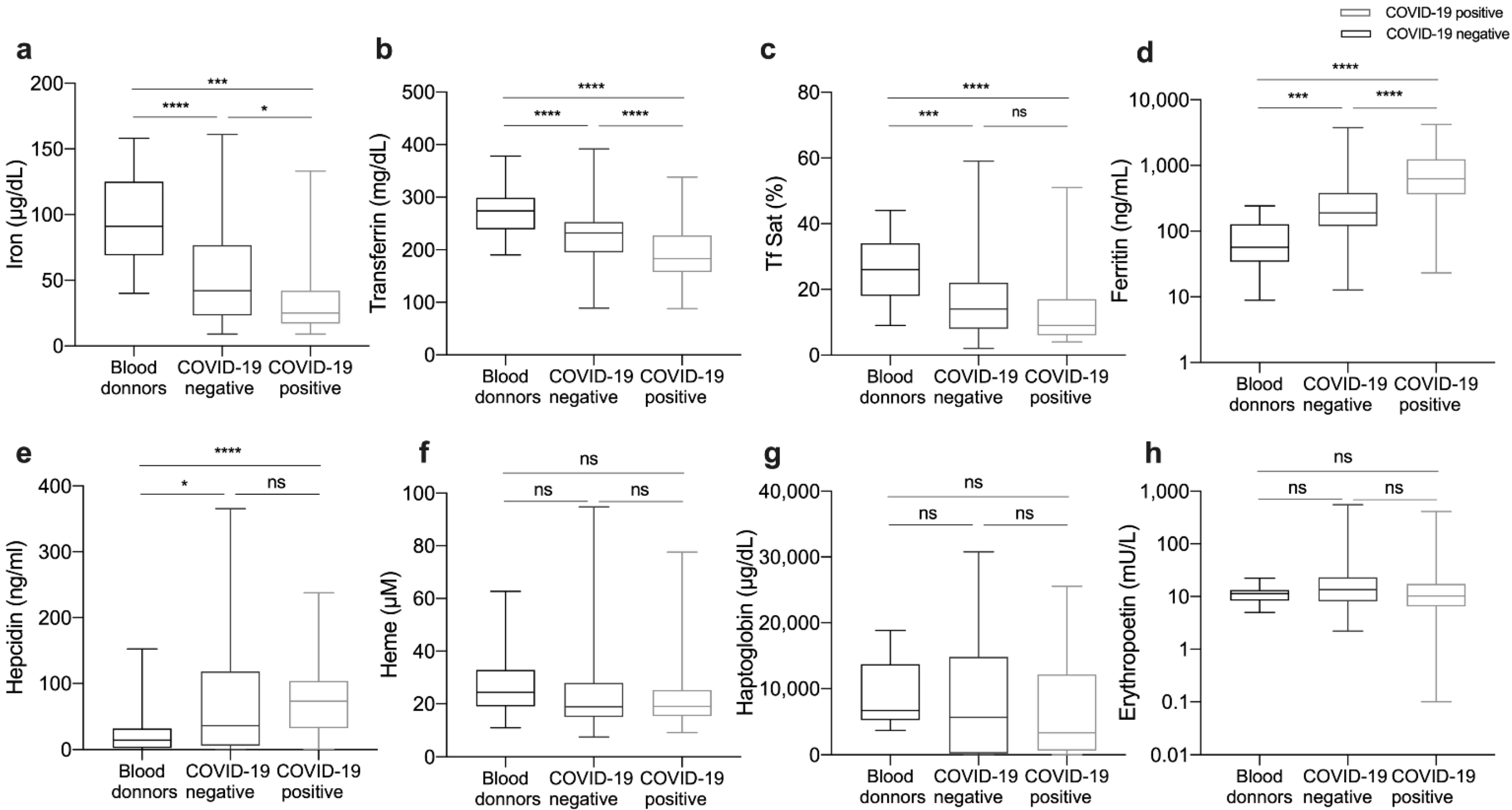
3.2. Impact of COVID-19 in Iron-Related and Hematological Parameters
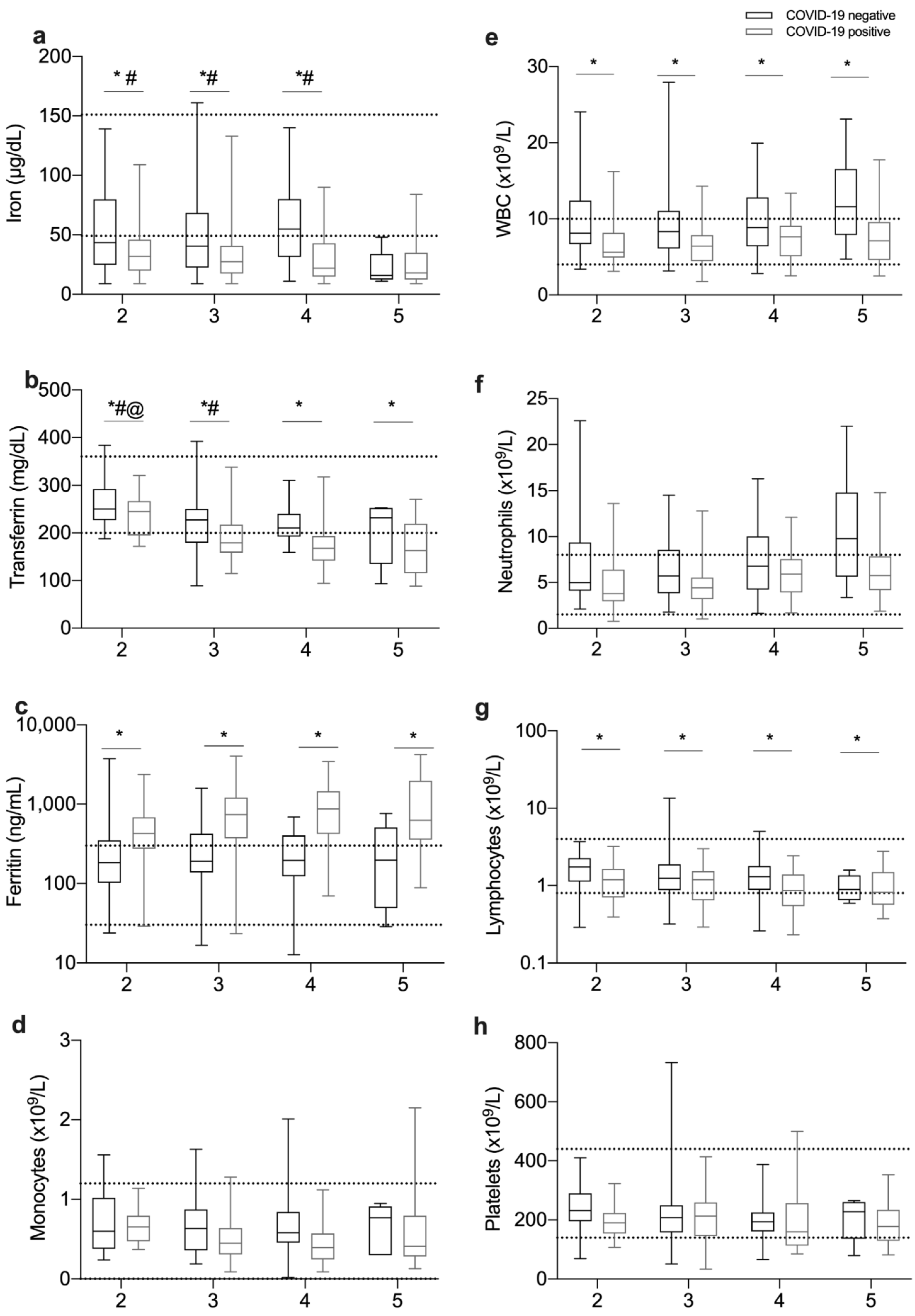
3.3. Relationship between Iron-Related Parameters and Disease Severity
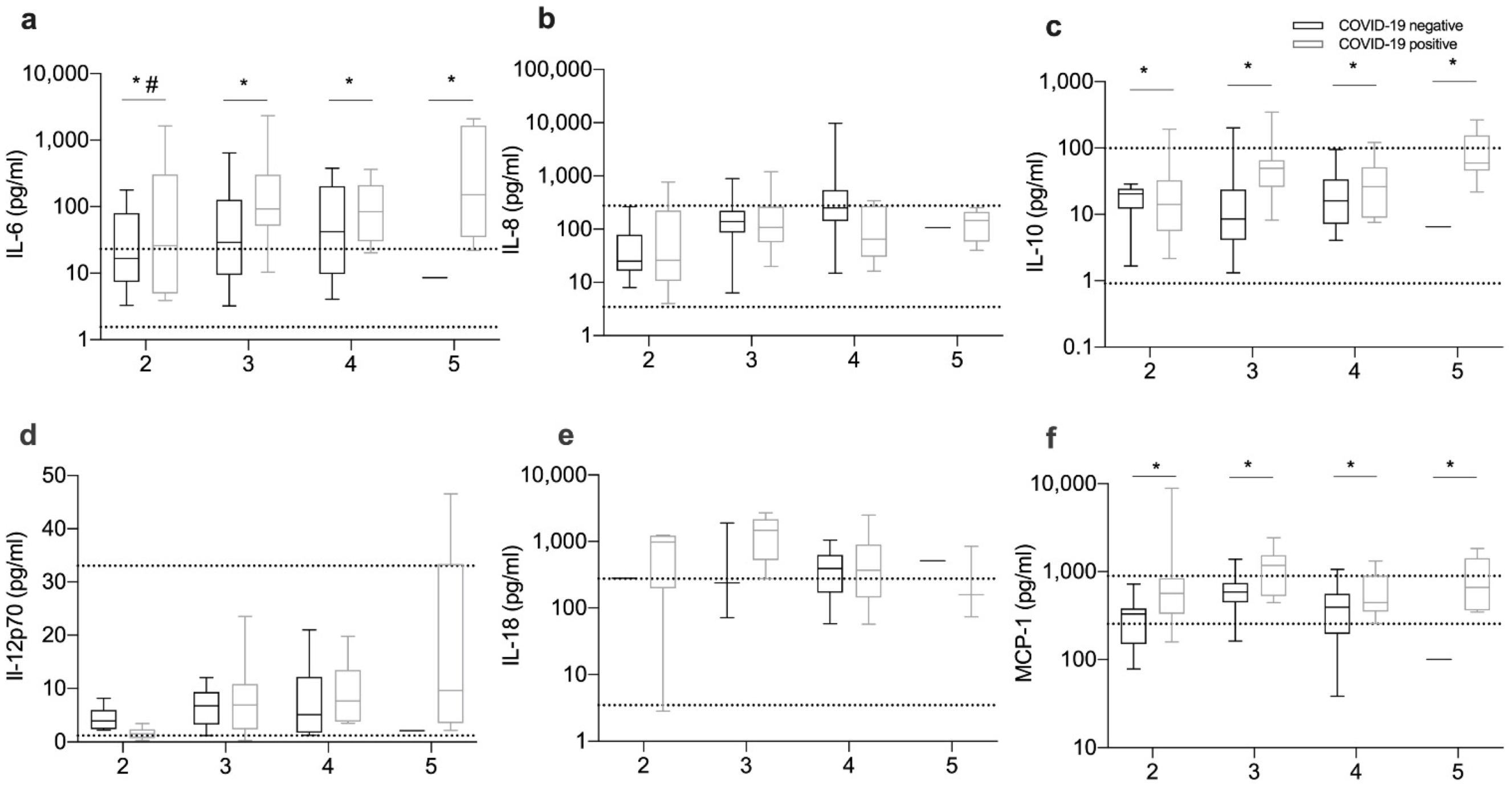
3.4. Inflammation and Immune Response Markers
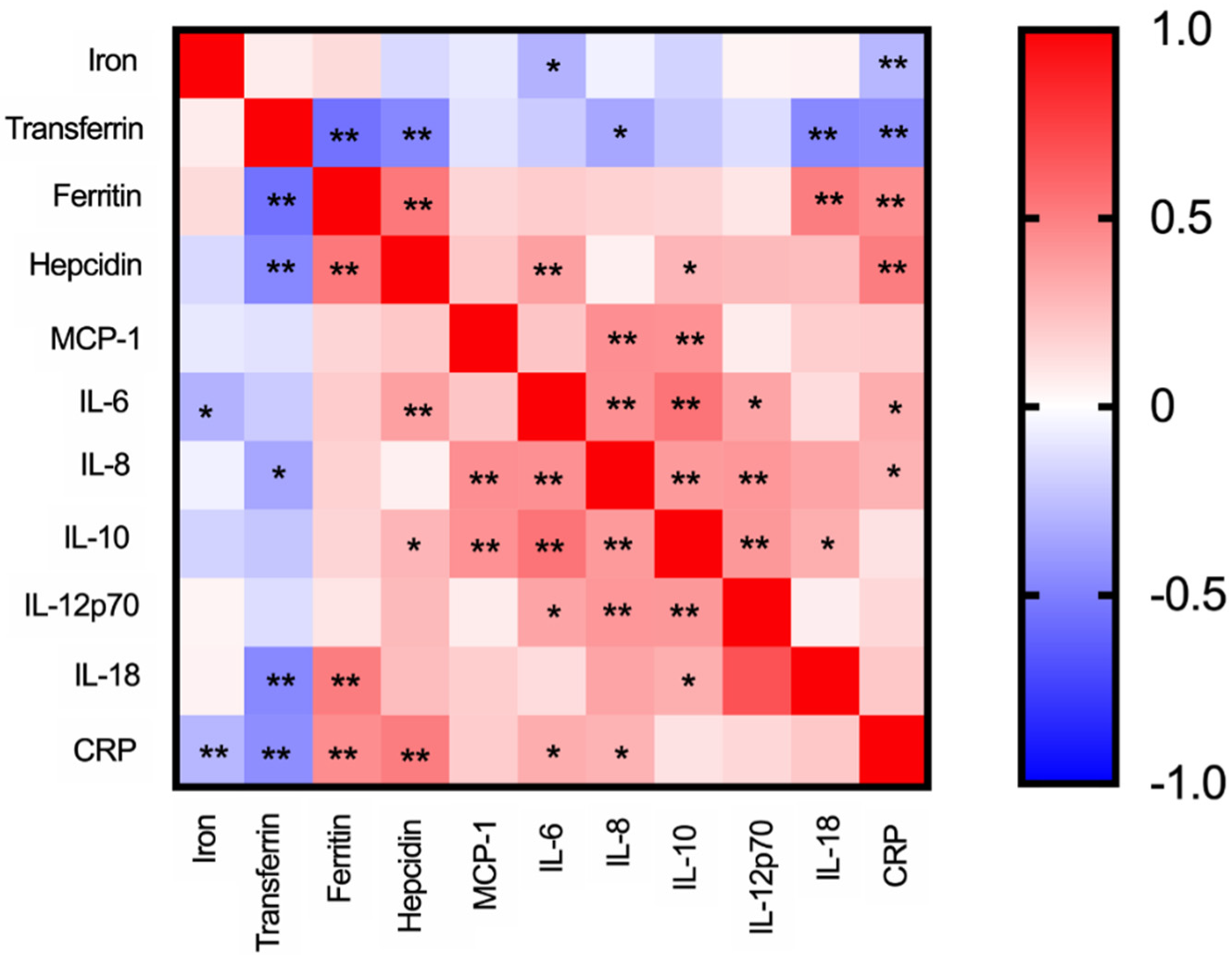
3.5. Correlations between Iron Parameters and Cytokine Levels
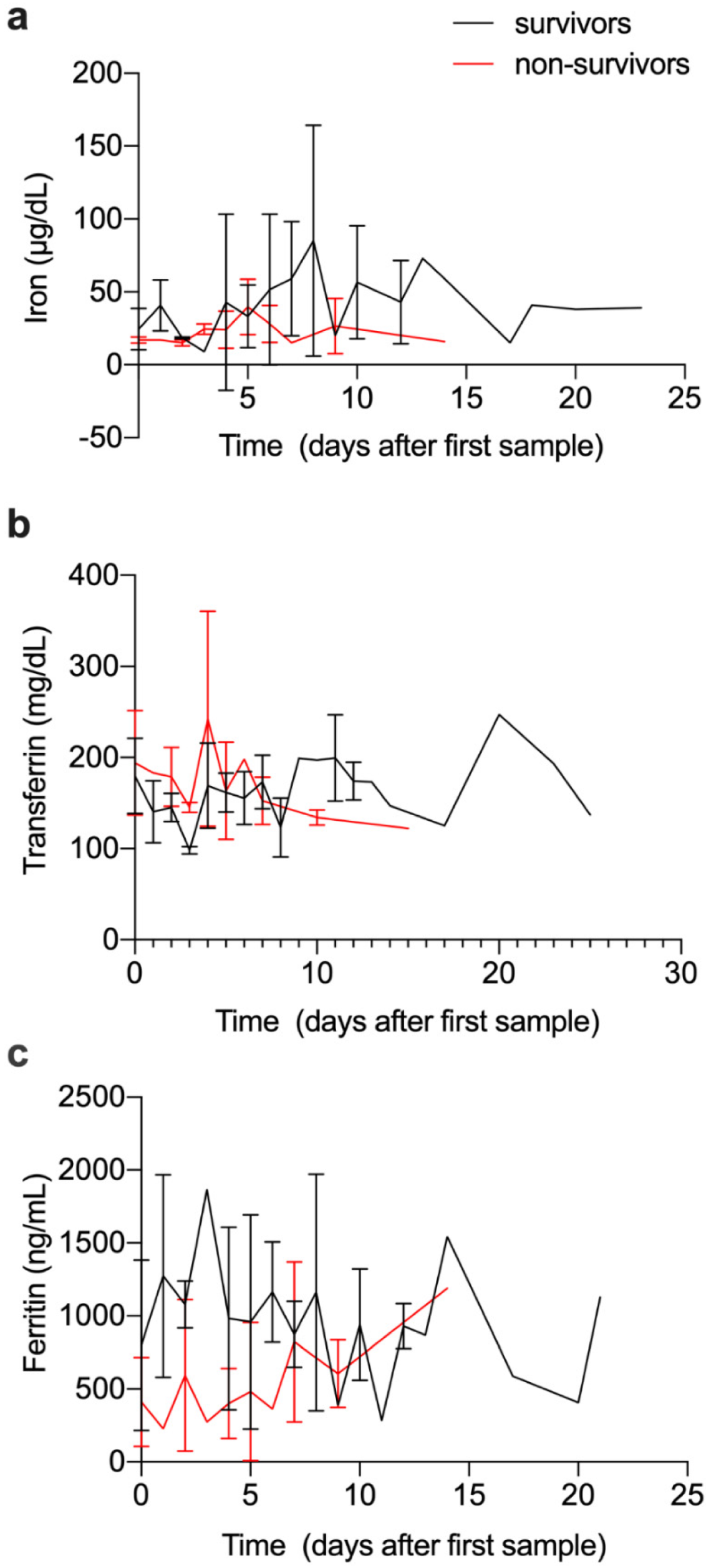
3.6. Evolution of Iron and Immune Parameters over Time
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Chen, G.; Wu, D.; Guo, W.; Cao, Y.; Huang, D.; Wang, H.; Wang, T.; Zhang, X.; Chen, H.; Yu, H.; et al. Clinical and immunological features of severe and moderate coronavirus disease 2019. J. Clin. Investig. 2020, 130, 2620–2629. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ko, J.Y.; Danielson, M.L.; Town, M.; Derado, G.; Greenlund, K.J.; Kirley, P.D.; Alden, N.B.; Yousey-Hindes, K.; Anderson, E.J.; Ryan, P.A.; et al. Risk Factors for Coronavirus Disease 2019 (COVID-19)-Associated Hospitalization: COVID-19-Associated Hospitalization Surveillance Network and Behavioral Risk Factor Surveillance System. Clin. Infect. Dis. 2021, 72, e695–e703. [Google Scholar] [CrossRef]
- Gomes, A.C.; Moreira, A.C.; Mesquita, G.; Gomes, M.S. Modulation of Iron Metabolism in Response to Infection: Twists for All Tastes. Pharmaceuticals 2018, 11, 84. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gomes-Pereira, S.; Rodrigues, P.N.; Appelberg, R.; Gomes, M.S. Increased susceptibility to Mycobacterium avium in hemochromatosis protein HFE-deficient mice. Infect. Immun. 2008, 76, 4713–4719. [Google Scholar] [CrossRef] [Green Version]
- Vale-Costa, S.; Gomes-Pereira, S.; Teixeira, C.M.; Rosa, G.; Rodrigues, P.N.; Tomás, A.; Appelberg, R.; Gomes, M.S. Iron overload favors the elimination of Leishmania infantum from mouse tissues through interaction with reactive oxygen and nitrogen species. PLoS Negl. Trop. Dis. 2013, 7, e2061. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hippchen, T.; Altamura, S.; Muckenthaler, M.U.; Merle, U. Hypoferremia is Associated With Increased Hospitalization and Oxygen Demand in COVID-19 Patients. Hemasphere 2020, 4, e492. [Google Scholar] [CrossRef]
- Shah, A.; Frost, J.N.; Aaron, L.; Donovan, K.; Drakesmith, H.; Collaborators. Systemic hypoferremia and severity of hypoxemic respiratory failure in COVID-19. Crit. Care 2020, 24, 320. [Google Scholar] [CrossRef] [PubMed]
- Zhao, K.; Huang, J.; Dai, D.; Feng, Y.; Liu, L.; Nie, S. Serum Iron Level as a Potential Predictor of Coronavirus Disease 2019 Severity and Mortality: A Retrospective Study. Open Forum Infect. Dis. 2020, 7, ofaa250. [Google Scholar] [CrossRef] [PubMed]
- Camaschella, C.; Nai, A.; Silvestri, L. Iron metabolism and iron disorders revisited in the hepcidin era. Haematologica 2020, 105, 260–272. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nai, A.; Lorè, N.I.; Pagani, A.; De Lorenzo, R.; Di Modica, S.; Saliu, F.; Cirillo, D.M.; Rovere-Querini, P.; Manfredi, A.A.; Silvestri, L. Hepcidin levels predict Covid-19 severity and mortality in a cohort of hospitalized Italian patients. Am. J. Hematol. 2021, 96, E32–E35. [Google Scholar] [CrossRef] [PubMed]
- Sonnweber, T.; Boehm, A.; Sahanic, S.; Pizzini, A.; Aichner, M.; Sonnweber, B.; Kurz, K.; Koppelstätter, S.; Haschka, D.; Petzer, V.; et al. Persisting alterations of iron homeostasis in COVID-19 are associated with non-resolving lung pathologies and poor patients’ performance: A prospective observational cohort study. Respir. Res. 2020, 21, 276. [Google Scholar] [CrossRef]
- Tojo, K.; Sugawara, Y.; Oi, Y.; Ogawa, F.; Higurashi, T.; Yoshimura, Y.; Miyata, N.; Hayami, H.; Yamaguchi, Y.; Ishikawa, Y.; et al. The U-shaped association of serum iron level with disease severity in adult hospitalized patients with COVID-19. Sci. Rep. 2021, 11, 13431. [Google Scholar] [CrossRef]
- Yağcı, S.; Serin, E.; Acicbe, Ö.; Zeren, M.; Odabaşı, M.S. The relationship between serum erythropoietin, hepcidin, and haptoglobin levels with disease severity and other biochemical values in patients with COVID-19. Int. J. Lab. Hematol. 2021, 43 (Suppl. 1), 142–151. [Google Scholar] [CrossRef]
- Zhou, C.; Chen, Y.; Ji, Y.; He, X.; Xue, D. Increased Serum Levels of Hepcidin and Ferritin Are Associated with Severity of COVID-19. Med. Sci. Monit. 2020, 26, e926178. [Google Scholar] [CrossRef] [PubMed]
- Biamonte, F.; Botta, C.; Mazzitelli, M.; Rotundo, S.; Trecarichi, E.M.; Foti, D.; Torti, C.; Viglietto, G.; Torella, D.; Costanzo, F. Combined lymphocyte/monocyte count, D-dimer and iron status predict COVID-19 course and outcome in a long-term care facility. J. Transl. Med. 2021, 19, 79. [Google Scholar] [CrossRef]
- Henry, B.M.; de Oliveira, M.H.S.; Benoit, S.; Plebani, M.; Lippi, G. Hematologic, biochemical and immune biomarker abnormalities associated with severe illness and mortality in coronavirus disease 2019 (COVID-19): A meta-analysis. Clin. Chem. Lab. Med. 2020, 58, 1021–1028. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lv, Y.; Chen, L.; Liang, X.; Liu, X.; Gao, M.; Wang, Q.; Wei, Q.; Liu, L. Association between iron status and the risk of adverse outcomes in COVID-19. Clin. Nutr. 2021, 40, 3462–3469. [Google Scholar] [CrossRef] [PubMed]
- Saúde, D.-D.G.D. Prescrição e Determinação do Hemograma. 2011, 2011. 63. Available online: https://nocs.pt/prescricao-determinacao-hemograma/ (accessed on 1 January 2021).
- Rodrigues, A.M.; Gregório, M.J.; Sousa, R.D.; Dias, S.S.; Santos, M.J.; Mendes, J.M.; Coelho, P.S.; Branco, J.C.; Canhão, H. Challenges of Ageing in Portugal: Data from the EpiDoC Cohort. Acta Med. Port. 2018, 31, 80–93. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Maguire, D.; Richards, C.; Woods, M.; Dolan, R.; Wilson Veitch, J.; Sim, W.M.J.; Kemmett, O.E.H.; Milton, D.C.; Randall, S.L.W.; Bui, L.D.; et al. The systemic inflammatory response and clinicopathological characteristics in patients admitted to hospital with COVID-19 infection: Comparison of 2 consecutive cohorts. PLoS ONE 2021, 16, e0251924. [Google Scholar] [CrossRef]
- Ekregbesi, P.; Shankar-Hari, M.; Bottomley, C.; Riley, E.M.; Mooney, J.P. Relationship between Anaemia, Haemolysis, Inflammation and Haem Oxygenase-1 at Admission with Sepsis: A pilot study. Sci. Rep. 2018, 8, 11198. [Google Scholar] [CrossRef]
- Gomes, A.C.; Moreira, A.C.; Silva, T.; Neves, J.V.; Mesquita, G.; Almeida, A.A.; Barreira-Silva, P.; Fernandes, R.; Resende, M.; Appelberg, R.; et al. IFN-gamma-Dependent Reduction of Erythrocyte Life Span Leads to Anemia during Mycobacterial Infection. J. Immunol. 2019, 203, 2485–2496. [Google Scholar] [CrossRef]
- Mathew, D.; Giles, J.R.; Baxter, A.E.; Oldridge, D.A.; Greenplate, A.R.; Wu, J.E.; Alanio, C.; Kuri-Cervantes, L.; Pampena, M.B.; D’Andrea, K.; et al. Deep immune profiling of COVID-19 patients reveals distinct immunotypes with therapeutic implications. Science 2020, 369, eabc8511. [Google Scholar] [CrossRef] [PubMed]
- DePalma, R.G.; Hayes, V.W.; O’Leary, T.J. Optimal serum ferritin level range: Iron status measure and inflammatory biomarker. Metallomics 2021, 13, mfab030. [Google Scholar] [CrossRef] [PubMed]
- Sabaka, P.; Koščálová, A.; Straka, I.; Hodosy, J.; Lipták, R.; Kmotorková, B.; Kachlíková, M.; Kušnírová, A. Role of interleukin 6 as a predictive factor for a severe course of Covid-19: Retrospective data analysis of patients from a long-term care facility during Covid-19 outbreak. BMC Infect. Dis. 2021, 21, 308. [Google Scholar] [CrossRef]
- Santa Cruz, A.; Mendes-Frias, A.; Oliveira, A.I.; Dias, L.; Matos, A.R.; Carvalho, A.; Capela, C.; Pedrosa, J.; Castro, A.G.; Silvestre, R. Interleukin-6 Is a Biomarker for the Development of Fatal Severe Acute Respiratory Syndrome Coronavirus 2 Pneumonia. Front. Immunol. 2021, 12, 613422. [Google Scholar] [CrossRef]
- Angriman, F.; Ferreyro, B.L.; Burry, L.; Fan, E.; Ferguson, N.D.; Husain, S.; Keshavjee, S.H.; Lupia, E.; Munshi, L.; Renzi, S.; et al. Interleukin-6 receptor blockade in patients with COVID-19: Placing clinical trials into context. Lancet Respir. Med. 2021, 9, 655–664. [Google Scholar] [CrossRef]
- WHO. WHO Recommends Life-Saving Interleukin-6 Receptor Blockers for COVID-19 and Urges Producers to Join Efforts to Rapidly Increase Access; WHO: Geneva, Switzerland, 2021. [Google Scholar]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| COVID19-Negative | COVID19-Positive | ||
|---|---|---|---|
| Blood Donors | Patients | ||
| Number of patients | 35 | 176 | 127 |
| Median age (P25–P75) a | 46 (42–59) | 65 (50–78) | 72 (61–81) |
| Number of males (%) | 16 (45.7) | 102 (58.0) | 78 (61.4) |
| Number of comorbidities, median (P25–P75) a | 4.0 (2–6) | 4.0 (2–6) | |
| Frequency of comorbidities (%): | |||
| Hypertension (*) | 52.8 | 65.4 | |
| Dyslipidemia (ns) | 44.3 | 44.1 | |
| Diabetes (**) | 26.1 | 40.9 | |
| Obesity (ns) | 23.3 | 24.4 | |
| Chronic kidney disease (ns) | 15.3 | 14.2 | |
| Chronic respiratory disease (ns) | 13.6 | 14.2 | |
| Iron supplementation (ns) | 10.8 | 5.5 | |
| Hypocoagulation (ns) | 9.7 | 8.7 | |
| Anemia (ns) | 3.4 | 3.1 | |
| Normal Range | COVID-19-Negative | COVID-19-Positive | ||
|---|---|---|---|---|
| Red blood cells (1012/L) Males Females | 4.31–6.4 3.85–5.20 | 4.44 (3.99–4.94) 4.20 (3.55–4.53) | 4.54 (4.05–4.98) 4.35 (4.00–4.68) | ns * |
| Hemoglobin (g/dL) Males Females | 13.6–18 11.5–16 | 13.3 (11.30–15.23) 12.6 (10.80–13.50) | 13.6 (12.30–15.2) 13.2 (12.10–13.90) | ns ns |
| Hematocrit (%) Males Females | 39.8–52 34.7–46 | 39.95 (34.80–44.80) 37.6 (32.90–40.50) | 40.09 (36.35–43.65) 38.9 (36.80–41.70) | ns * |
| Mean corpuscular volume (fL) | 80–97 | 89.7 ± 6.28 | 90.1 ± 5.55 | ns |
| Mean corpuscular hemoglobin (pg) | 26–34 | 30.0 ± 2.49 | 30.2 ± 2.14 | ns |
| Mean corpuscular hemoglobin concentration (g/dL) | 32–36 | 33.5 ± 1.43 | 33.6 ± 1.15 | ns |
| Red blood cell distribution width-CV (%) | 11.5–15 | 14.2 ± 1.68 | 13.8 ± 1.60 | ns |
| Red blood cell distribution width-SD (fL) | 37–54 | 46.1 ± 5.99 | 45.4 ± 5.38 | ns |
| White blood cells (×109/L) | 4.0–10.0 | 8.44 (6.35–11.49) | 6.48 (4.77–8.32) | *** |
| Neutrophils (×109/L) | 1.5–8 | 5.97 (4.05–9.14) | 4.49 (3.17–6.81) | *** |
| Lymphocytes (×109/L) | 0.8–4 | 1.41 (0.92–1.95) | 1.02 (0.63–1.49) | *** |
| Monocytes (×109/L) | 0.0–1.2 | 0.60 (0.38–0.87) | 0.50 (0.32–0.71) | *** |
| Platelets (109/L) | 140–440 | 216.0 (167.0–257.5) | 191.5 (144.0–251.5) | * |
| Mean platelet volume (fL) | 10.8 ± 1.01 | 10.9 ± 1.03 | ns | |
| Platelet distribution width (fL) | 12.8 ± 2.42 | 13.1 ± 2.37 | ns | |
| CRP a (mg/L) | <3 | 8.10 (2.33–63.93) | 64.2 (21.40–133.83) | ** |
| AST a (U/L) | 10–37 | 30.00 (22.00–43.00) | 35.00 (25.00–57.25) | ns |
| ALT a (U/L) | 10–37 | 24.00 (16.00–35.5) | 25.00 (16.00–47.00) | ns |
| Gamma GT a (U/L) | 10–49 | 30.00 (18.00–56.75) | 48.00 (25.00–88.00) | ns |
| Total Protein (g/L) | 64–83 | 68.1 ± 9.95 | 69.1 ± 9.32 | ns |
| Number | Minimum O2 Saturation a | Pneumonia (%) | ||
|---|---|---|---|---|
| All | ||||
| COVID-19-negative | 176 | 93.0 ± 7.3 | 15.3% | |
| COVID-19-positive | 127 | 88.3 ± 7.9 | 60.6% | |
| 1 | Asymptomatic | |||
| COVID-19-negative | 15 | 96.8 ± 2.1 | --- | |
| COVID-19-positive | 0 | --- | --- | |
| 2 | Ambulatory | |||
| COVID-19-negative | 40 | 95.1 ± 3.4 | 15.0% | |
| COVID-19-positive | 28 | 94.4 ± 2.5 | 14.3% | |
| 3 | General inward | |||
| COVID-19-negative | 72 | 92.9 ± 5.6 | 20.8% | |
| COVID-19-positive | 48 | 89.1 ± 6.9 | 60.4% | |
| 4 | Intensive care | |||
| COVID-19-negative | 43 | 93.0 ±7.2 | 9.3% | |
| COVID-19-positive | 32 | 86.4 ± 7.0 | 84.4% | |
| 5 | Fatalities | |||
| COVID-19-negative | 6 | 77.3 ± 18.4 | 33.3% | |
| COVID-19-positive | 19 | 81.2 ± 10.0 | 89.5% |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Moreira, A.C.; Teles, M.J.; Silva, T.; Bento, C.M.; Alves, I.S.; Pereira, L.; Guimarães, J.T.; Porto, G.; Oliveira, P.; Gomes, M.S. Iron Related Biomarkers Predict Disease Severity in a Cohort of Portuguese Adult Patients during COVID-19 Acute Infection. Viruses 2021, 13, 2482. https://doi.org/10.3390/v13122482
Moreira AC, Teles MJ, Silva T, Bento CM, Alves IS, Pereira L, Guimarães JT, Porto G, Oliveira P, Gomes MS. Iron Related Biomarkers Predict Disease Severity in a Cohort of Portuguese Adult Patients during COVID-19 Acute Infection. Viruses. 2021; 13(12):2482. https://doi.org/10.3390/v13122482
Chicago/Turabian StyleMoreira, Ana C., Maria Jose Teles, Tânia Silva, Clara M. Bento, Inês Simões Alves, Luisa Pereira, João Tiago Guimarães, Graça Porto, Pedro Oliveira, and Maria Salomé Gomes. 2021. "Iron Related Biomarkers Predict Disease Severity in a Cohort of Portuguese Adult Patients during COVID-19 Acute Infection" Viruses 13, no. 12: 2482. https://doi.org/10.3390/v13122482