
Bacteriophages as an Alternative Method for Control of Zoonotic and Foodborne Pathogens


Abstract
:1. Introduction
1.1. General Characteristics of Bacteriophages
1.2. History of Bacteriophages
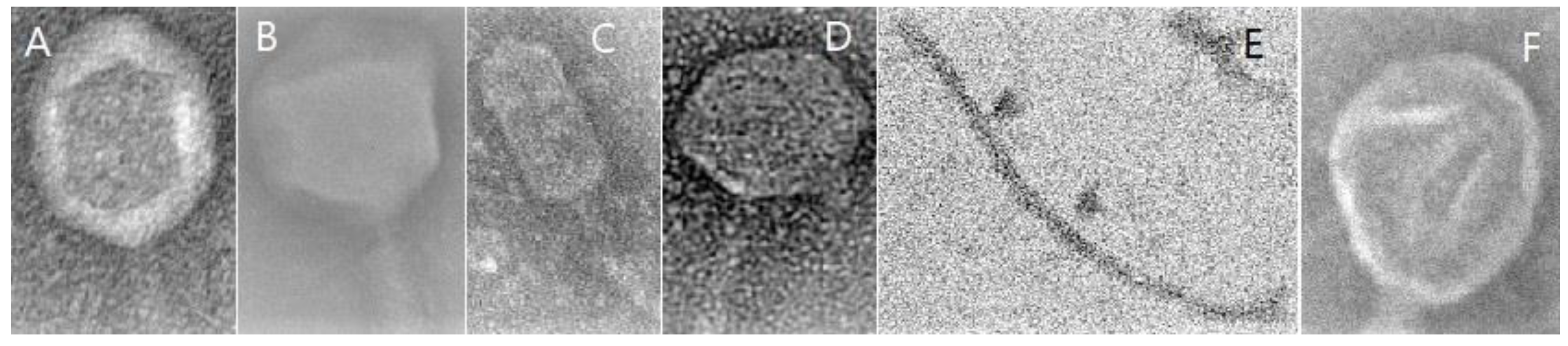
1.3. Classification of Bacteriophages
1.4. Life Cycles of Phages
2. The Spectrum of Use of Bacteriophages
Bacteriophage Interactions during Phage Therapy
- lysis of bacteria usually highly resistant to antibiotic therapy, living in a biofilm;
- high degree of safety for commensal and symbiotic flora;
- possibility of use with other bacteriophages as a cocktail or with other antibacterials;
- complete biodegradability of bacteriophages, making them safe for the organism and the environment [17].
- repeating phage administration two or more times, because bacteriophages can multiply at the site of application during infection of the host bacteria;
- increasing the phage concentration in the solution, because a high level of phages protects against complete destruction by neutralizing antibodies;
- using different phages, especially during the second and subsequent cycles of application during treatment, because resistance differs from one phage to another [27]. In addition to the increase in neutralizing antibodies during phage therapies, the concentration of class M and G immunoglobulins increases as well and continues to increase with subsequent applications of phage preparations [83,84].
3. Commercial Products with Bacteriophages for Elimination of Foodborne Zoonotic Pathogens
4. Advantages and Disadvantages of Bacteriophage Therapy
- Because the mechanism of action of phages against the host bacteria is different to that of antibiotics, they are highly effective against many pathogens, especially against multidrug-resistant bacteria [36].
- Phages replicate at the site of infection even after a single application, because they multiply inside the bacterial cell and therefore are released at the site of infection [101].
- Bacteriophages are resistant to stress factors during food production [91].
- There is no withdrawal period in livestock due to the lack of residue in tissues as soon as therapy is completed [103].
- There are no side effects or allergic reactions because most bacteriophages consist mainly of proteins and genetic material (DNA or RNA).
- Due to their high specificity for a single type of bacteria, bacteriophages have a narrow host range [104].
- Bacteriophages may neutralize antibodies, which may prevent a portion of the administered phage dose from adhering to the target bacteria [104].
- Only lytic phages are admissible in phage therapy because lysogenic (temporary) phages may be a source of horizontal transfer of bacterial toxins or antibiotic resistance [31].
- The duration of survival of phages is varied, depending in part on the presence of the host bacteria. Their activity is also influenced by the environment within the organism in which it is administered, and therefore the survival of phages must be monitored at the site of administration in order to assess their antimicrobial activity [99].
- Information about the kinetics of phages remains insufficient, especially the degree of adsorption, the number of replications necessary for a therapeutic effect, the latent period, and their elimination from the body by phagocytic cells [106].
5. Bacteriophage Efficacy in Experimental Models
6. Conclusions
Author Contributions
Funding
Conflicts of Interest
Abbreviations
| AMPs | antimicrobial peptides |
| ATCC | American Type Culture Collection |
| BALB | Bagg Albino Mouse |
| BAVS | Bacterial and Archaeal Viruses Subcommittee |
| CD | cluster of differentiation |
| CFU | colony-forming unit |
| EFSA | European Food Safety Authority |
| EHEC | Enterohaemorrhagic Escherichia coli |
| ETEC | Enterotoxigenic Escherichia coli |
| EFSA | European Food Safety Authority |
| EIBMV | Eliava Institute of Bacteriophages, Microbiology, and Virology |
| HF | Holstein–Friesian |
| HIIET | Hirszfeld Institute of Immunology and Experimental Therapy |
| HGT | horizontal gene transfer |
| Hp | haptoglobin |
| ICR | Institute of Cancer Research |
| ICTV | International Committee on Taxonomy of Viruses |
| IFNγ | Interferon gamma |
| Ig | immunoglobulin |
| i.p | intraperitoneally |
| i.n | intranasal |
| INSDC | International Nucleotide Sequence Database Collaboration |
| IL | interleukin |
| LAB | lactic acid bacteria |
| LPS | lipopolysaccharide |
| MAC-T | mammary alveolar cells |
| MDR | multidrug-resistant |
| MHC | major histocompatibility complex |
| MOI | multiplicity of infection |
| NF-κB | nuclear factor kappa-light-chain-enhancer of activated B cells |
| NK | Natural killer |
| PFU | plaque-forming units |
| PMN | polymorphonuclear |
| RBPs | receptor-binding proteins |
| ROS | reactive oxygen species |
| mRNA | messenger RNA |
| SAA | serum amyloid A |
| ssRNA | single-stranded ribonucleic acid |
| dsRNA | double-stranded ribonucleic acid |
| ssDNA | single-stranded deoxyribonucleic acid |
| dsDNA | double-stranded deoxyribonucleic acid |
| SPF | specific free pathogens |
| stx | Shiga toxin |
| TEM | transmission electron microscopy |
| TNF-α | tumour necrosis factor α |
| UV | ultraviolet |
| WHO | World Health Organization |
References
- Ssekatawa, K.; Byarugabaa, D.K.; Katoa, C.D.; Wampandea, E.M.; Ejobia, F.; Tweyongyerea, R.; Nakavumaa, J.L. A review of phage mediated antibacterial applications. Alexandria J. Med. 2021, 57, 1–20. [Google Scholar] [CrossRef]
- World Health Organization. World Health Organization Estimates of the Global Burden of Foodborne Diseases; WHO: Geneva, Switzerland, 2015; Available online: http://apps.who.int (accessed on 22 November 2021).
- Alali, W.Q.; Thakur, S.; Berghaus, R.D.; Martin, M.P.; Gebreyes, W.A. Prevalence anddistribution of Salmonella in organic andconventional broiler poultry farms. Foodborne Pathog. Dis. 2010, 7, 1363–1371. [Google Scholar] [CrossRef] [Green Version]
- Sillankorva, S.M.; Oliveira, H.; Azeredo, J. Bacteriophages and their role in food safety. Inter. J. Microbiol 2012, 2012, 863945. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Niu, Y.D.; Cook, S.R.; Wang, J.; Klima, C.L.; Hsu, Y.; Kropinski, A.M.; Turner, D.; McAllister, T.A. Comparative analysis of multiple inducible phages from Mannheimia haemolytica. BMC Microbiol. 2015, 15, 175. [Google Scholar] [CrossRef] [Green Version]
- European Food Safety Authority (EFSA). The European Union summary report on antimicrobial resistance in zoonotic and indicator bacteria from humans, animals and food in 2017. EFSA J. 2018, 17, e05598. [Google Scholar]
- Eichenberger, E.M.; Thaden, J.T. Epidemiology and mechanisms of resistance of extensively drug resistant Gram-negative bacteria. Antibiotics 2019, 8, 37. [Google Scholar] [CrossRef] [Green Version]
- Donkor, E.S.; Newman, M.J.; Yeboah-Manu, D. Epidemiological aspects of non-human antibiotic usage and resistance: Implications for the control of antibiotic resistance in Ghana. Trop. Med. Int. Health 2012, 17, 462–468. [Google Scholar] [CrossRef]
- Żbikowska, K.; Michalczuk, M.; Dolka, B. The use of bacteriophages in the poultry industry. Animals 2020, 10, 872. [Google Scholar] [CrossRef]
- Regulation (EU) 2019/6 Of The European Parliament And Of The Council of 11 December 2018 on veterinary medicinal products and repealing Directive 2001/82/EC. Offical J. EU.Union. 2019, pp. 43–167. Available online: https://eur-lex.europa.eu/eli/reg/2019/6/oj (accessed on 22 November 2021).
- Orlova, E. Bacteriophages and Their Structural Organisation, 1st ed.; IntechOpen: London, UK, 2012; pp. 3–30. [Google Scholar]
- Lenski, R.E. Dynamics of interactions between bacteria and virulent bacteriophage. In Advances in Microbial Ecology; Springer: Chicago, IL, USA, 1988; pp. 1–44. [Google Scholar]
- Batinovic, S.; Wassef, F.; Knowler, S.A.; Rice, D.T.F.; Stanton, C.R.; Rose, J.; Tucci, J.; Nittami, T.; Vinh, A.; Drummond, G.R.; et al. Bacteriophages in natural and artificial environments. Pathogens 2019, 8, 100. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brüssow, H. Bacteria between protists and phages: From antipredation strategies to the evolution of pathogenicity. Mol. Microbiol. 2007, 65, 583–589. [Google Scholar] [CrossRef]
- Vikram, A.; Tokman, J.I.; Woolston, J.; Sulakvelidze, A. Phage Biocontrol Improves Food Safety by Significantly Reducing the Level and Prevalence of Escherichia coli O157:H7 in Various Foods. J. Food Prot. 2021, 83, 668–676. [Google Scholar] [CrossRef] [PubMed]
- Viazis, S.; Akhtar, M.; Feirtag, J.; Brabban, A.D.; Diez-Gonzalez, F. Isolation and characterization of lytic bacteriophages against enterohaemorrhagic Escherichia coli. J. Appl. Microbiol. 2011, 110, 1323–1331. [Google Scholar] [CrossRef]
- Dec, M.; Wernicki, A.; Urban-Chmiel, R. Efficacy of experimental phage therapies in livestock. Anim. Health Res. Rev. 2020, 21, 69–83. [Google Scholar] [CrossRef] [PubMed]
- De Jonge, P.A.; Nobrega, F.L.; Brouns, S.J.; Dutilh, B.E. Molecular and evolutionary determinants of bacteriophage host range. Trends Microb. 2019, 27, 51–63. [Google Scholar] [CrossRef]
- Dunne, M.; Rupf, B.; Tala, M.; Qabrati, X.; Ernst, P.; Shen, Y.; Sumrall, E.; Heeb, L.; Plückthun, P.; Loessner, M.J.; et al. Reprogramming Bacteriophage Host Range through Structure-Guided Design of Chimeric Receptor Binding Proteins. Cell Reports 2019, 29, 1336–1350. [Google Scholar] [CrossRef] [Green Version]
- Twort, F.W. An investigation on the nature of ultramicroscopic viruses. Lancet 1915, 186, 1241–1243. [Google Scholar] [CrossRef] [Green Version]
- d’Herelle, F. Sur un microbe invisible antagoniste des bacilles dysentériques. Comptes Rendus de l’Académie Sci. Paris 1917, 165, 173–175. [Google Scholar]
- d’Herelle, F. Sur le role du microbe bacteriophage dans la typhose aviare. C. R. Acad. Sci. 1919, 169, 932–934. [Google Scholar]
- Duckworth, D.H. Who discovered bacteriophage? Bacteriol. Rev. 1976, 40, 793. [Google Scholar] [CrossRef]
- Abedon, S.T.; Thomas-Abedon, C.; Thomas, A.; Mazure, H. Bacteriophage prehistory: Is or is not Hankin, 1896, a phage reference. Bacteriophage 2011, 1, 174–178. [Google Scholar] [CrossRef] [Green Version]
- Opal, S.M. The evolution of the understanding of sepsis, infection, and the host response: A brief history. Crit. Care Clin. 2009, 25, 637–663. [Google Scholar] [CrossRef] [PubMed]
- Rello, J.; Bunsow, E.; Perez, A. What if there were no new antibiotics? A look at alternatives. Expert Rev. Clin. Pharmacol. 2016, 9, 1547–1555. [Google Scholar] [CrossRef] [PubMed]
- Sulakvelidze, A.; Alavidze, Z.; Morris, J.G. Bacteriophage therapy. Antimicrob Agents Chemother. 2001, 45, 649–659. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kutter, E.; De Vos, D.; Gvasalia, G.; Alavidze, Z.; Gogokhia, L.; Kuhl, S.; Abedon, S.T. Phage therapy in clinical practice: Treatment of human infections. Curr. Pharm. Biotechnol. 2010, 11, 69–86. [Google Scholar] [CrossRef]
- Górski, A.; Miedzybrodzki, R.; Weber-Da˛browska, B.; Fortuna, W.; Letkiewicz, S.; Rogóż, P.; Jończyk-Matysiak, E.; Dabrowska, K.; Majewska, J.; Borysowski, J. Phage Therapy: Combating Infections with Potential for Evolving from Merely a Treatment for Complications to Targeting Diseases. Front. Microbiol. 2016, 7, 1515. [Google Scholar] [CrossRef] [Green Version]
- International Nucleotide Sequence Database Collaboration. Available online: https://www.insdc.org/ (accessed on 28 October 2021).
- Wittebole, X.; De Roock, S.; Opal, S.M. A historical overview of bacteriophage therapy as an alternative to antibiotics for the treatment of bacterial pathogens. Virulence 2014, 5, 226–235. [Google Scholar] [CrossRef]
- Adriaenssens, E.M.; Krupovic, M.; Knezevic, P.; Ackermann, H.W.; Barylski, J.; Brister Clokie, R.M.C.; Duffy, S.; Dutilh, B.E.; Edwards, R.A.; Enault, F.; et al. Taxonomy of prokaryotic viruses: 2016 update from the ICTV bacterial and archaeal viruses subcommittee. Archiv. Virol. 2017, 162, 1153–1157. [Google Scholar] [CrossRef] [Green Version]
- Pyzik, E.; Radzki, R.P.; Urban-Chmiel, R. Experimental Phage Therapies in Companion Animals with A Historical Rewiev. Curr. Clin. Pharmacol. 2021, 16, 17–29. [Google Scholar]
- García, P.; Rodríguez, L.; Rodríguez, A.; Martínez, B. Food biopreservation: Promising strategies using bacteriocins, bacteriophages and endolysins. Trends Food Sci. Technol. 2010, 21, 373–382. [Google Scholar] [CrossRef] [Green Version]
- Rakhuba, D.V.; Kolomiets, E.I.; Dey, E.S.; Novik, G.I. Bacteriophage receptors, mechanisms of phage adsorption and penetration into host cell. Pol. J. Microbiol. 2010, 59, 145–155. [Google Scholar] [CrossRef]
- Hanlon, G.W. Bacteriophages: An appraisal of their role in the treatment of bacterial infections. Int. J. Antimicrob. Agen. 2007, 30, 118–128. [Google Scholar] [CrossRef]
- Wernicki, A.; Nowaczek, A.; Urban-Chmiel, R. Bacteriophage therapy to combat bacterial infections in poultry. Virol. J. 2017, 14, 179. [Google Scholar] [CrossRef] [PubMed]
- Clark, D.P.; Pazdernik, N.J. Chapter 7. Cloning Genes for Analysis. In Molecular Biology, 2nd ed.; Academic Cell Update Edition; Elsevier Inc.: Waltham, MA, USA, 2013; pp. 194–226. [Google Scholar]
- Hyman, P.; Abedon, S.T. Bacteriophage Host Range and Bacterial Resistance, in Advances in Applied Microbiology; Elsevier: Amsterdam, The Netherlands, 2010; pp. 217–248. [Google Scholar]
- Clokie, M.R.; Millard, A.D.; Letarov, A.V.; Heaphy, S. Phages in nature. Bacteriophage 2011, 1, 31–45. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alomari, M.M.M.; Dec, M.; Nowaczek, A.; Puchalski, A.; Wernicki, A.; Kowalski, C.J.; Urban-Chmiel, R. Therapeutic and Prophylactic Effect of the Experimental Bacteriophage Treatment to Control Diarrhea Caused by E. coli in Newborn Calves. ACS Infect. Dis. 2021, 7, 2093–2101. [Google Scholar] [CrossRef] [PubMed]
- Wagenaar, J.A.; Van Bergen, M.A.; Mueller, M.A.; Wassenaar, T.M.; Carlton, R.M. Phage therapy reduces Campylobacter jejuni colonization in broilers. Vet. Microbiol. 2005, 109, 275–283. [Google Scholar] [CrossRef]
- Ahmadi, M.; Karimi Torshizi, M.A.; Rahimi, S.; Dennehy, J.J. Prophylactic bacteriophage administration more effective than post-infection Administration in Reducing Salmonella enterica serovar Enteritidis shedding in quail. Front. Microbiol. 2016, 7, 1253. [Google Scholar] [CrossRef] [Green Version]
- Kazi, M.; Annapure, U.S. Bacteriophage biocontrol of foodborne pathogens. J. Food Sci. Tech. 2016, 53, 1355–1362. [Google Scholar] [CrossRef] [Green Version]
- Silva, J.; Sauvageau, D. Bacteriophages as antimicrobial agents against bacterial contaminants in yeast fermentation processes. J. Biotech. Biof. 2014, 7, 123. [Google Scholar] [CrossRef]
- Roy, B.; Ackermann, H.W.; Pandian, S.; Picard, G.; Goulet, J. Biological inactivation of adhering Listeria monocytogenes by listeriaphages and a quaternary ammonium compound. Appl. Environ. Microbiol. 1993, 59, 2914–2917. [Google Scholar] [CrossRef] [Green Version]
- Ho, Y.H.; Tseng, C.C.; Wang, L.S.; Chen, Y.T.; Ho, G.J.; Lin, T.Y.; Wang, L.Y.; Chen, L.K. Application of bacteriophage-containing aerosol against nosocomial transmission of carbapenem-resistant acinetobacter baumannii in an intensive care unit. PLoS ONE 2016, 11, e0168380. [Google Scholar]
- Le, T.S.; Southgate, P.C.; O’Connor, W.; Poole, S.; Kurtböke, D.I. Bacteriophages as biological control agents of enteric bacteria contaminating edible oysters. Curr. Microbiol. 2018, 75, 611–619. [Google Scholar] [CrossRef]
- Sieiro, C.; Areal-Hermida, L.; Pichardo-Gallardo, Á.; Almuiña-González, R.; de Miguel, T.; Sánchez, S.; Sánchez-Pérez, Á.; Villa, T.G. A Hundred Years of Bacteriophages: Can Phages Replace Antibiotics in Agriculture and Aquaculture? Antibiotics 2020, 9, 493. [Google Scholar] [CrossRef] [PubMed]
- Bai, J.; Kim, Y.T.; Ryu, S.; Lee, J.H. Biocontrol and rapid detection of food-borne pathogens using bacteriophages and endolysins. Front. Microbiol. 2016, 7, 1–15. [Google Scholar] [CrossRef]
- Sultan, I.; Rahman, S.; Jan, A.T.; Siddiqui, M.T.; Mondal, A.H.; Haq, Q.M.R. Antibiotics, resistome and resistance mechanisms: A bacterial perspective. Front. Microbiol. 2018, 9, 2066. [Google Scholar] [CrossRef] [Green Version]
- Park, K.; Cha, K.E.; Myung, H. Observation of inflammatory responses in mice orally fed with bacteriophage T 7. J. Appl. Microb. 2014, 117, 627–633. [Google Scholar] [CrossRef]
- Van Belleghem, J.D.; Clement, F.; Merabishvili, M.; Lavigne, R.; Vaneechoutte, M. Pro-and anti-inflammatory responses of peripheral blood mononuclear cells induced by Staphylococcus aureus and Pseudomonas aeruginosa phages. Sci. Rep. 2017, 7, 1–13. [Google Scholar]
- Zhang, L.; Hou, X.; Sun, L.; He, T.; Wei, R.; Pang, M.; Wang, R. Staphylococcus aureus bacteriophage suppresses LPS-induced inflammation in MAC-T bovine mammary epithelial cells. Front. Microbiol. 2018, 9, 1614. [Google Scholar] [CrossRef] [Green Version]
- Smith, H.W.; Huggins, M.B.; Shaw, K.M. Factors influencing the survival and multiplication of bacteriophages in calves and in their environment. J. Gen. Microbiol. 1987, 133, 1127–1135. [Google Scholar] [CrossRef] [Green Version]
- Cooper, R.A.; Bjarnsholt, T.; Alhede, M. Biofilms in wounds: A review of present knowledge. J. Wound. Care 2014, 23, 570–580. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Reardon, S. Phage therapy gets revitalized: The rise of antibiotic resistance rekindles interest in a century-old virus treatment. Nature 2014, 510, 15–17. [Google Scholar] [CrossRef] [Green Version]
- Kutter, E.M.; Kuhl, S.J.; Abedon, S.T. Re-establishing a place for phage therapy in western medicine. Future Microbiol. 2015, 10, 685–688. [Google Scholar] [CrossRef] [Green Version]
- Alomari, M.M.M.; Nowaczek, A.; Dec, M.; Urban-Chmiel, R. Antibacterial activity of bacteriophages isolated from poultry against Shiga-toxic strains of Esherichia coli isolated from calves. Med. Weter. 2016, 72, 699–703. [Google Scholar] [CrossRef] [Green Version]
- Cisek, A.A.; Dąbrowska, I.; Gregorczyk, K.P.; Wyżewski, Z. Phage therapy in bacterial infections treatment: One hundred years after the discovery of bacteriophages. Curr. Microbiol. 2017, 74, 1–7. [Google Scholar] [CrossRef] [Green Version]
- Podlacha, M.; Grabowski, Ł.; Kosznik-Kawśnicka, K.; Zdrojewska, K.; Stasiłojć, M.; Węgrzyn, G.; Alicja Węgrzyn, A. Interactions of Bacteriophages with Animal and Human Organisms—Safety Issues in the Light of Phage Therapy. Int. J. Mol. Sci. 2021, 22, 8937. [Google Scholar] [CrossRef]
- Ann, T.W.; Kim, S.J.; Lee, Y.D.; Park, J.H.; Chang, H.I. The Immune-Enhancing Effect of the Cronobacter Sakazakii ES2 Phage Results in the Activation of Nuclear Factor-KB and Dendritic Cell Maturation via the Activation of IL-12p40 in the Mouse Bone Marrow. Immunol. Lett. 2014, 157, 1–8. [Google Scholar] [CrossRef]
- Van Belleghem, J.D.; Dąbrowska, K.; Vaneechoutte, M.; Barr, J.J.; Bollyky, P.L. Interactions between Bacteriophage, Bacteria, and the Mammalian Immune System. Viruses 2019, 11, 10. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Geier, M.R.; Trigg, M.E.; Merril, C.R. Fate of bacteriophage lambda in non-immune germ-free mice. Nature 1973, 246, 221–223. [Google Scholar] [CrossRef] [PubMed]
- Tiwari, B.R.; Kim, S.; Rahman, M.; Kim, J. Antibacterial efficacy of lytic Pseudomonas bacteriophage in normal and neutropenic mice models. J. Microbiol. 2011, 49, 994–999. [Google Scholar] [CrossRef]
- Tóthová, L.; Celec, P.; Bábíˇcková, J.; Gajdošová, J.; Al-Alami, H.; Kamodyova, N.; Drahovská, H.; Liptáková, A.; Tur ˇna, J.; Hodosy, J. Phage Therapy of Cronobacter-Induced Urinary Tract Infection in Mice. Med. Sci. Monit. 2011, 17, 173–178. [Google Scholar] [CrossRef]
- Reyes, A.; Semenkovich, N.P.; Whiteson, K.; Rohwer, F.; Gordon, J.I. Going viral: Next generation sequencing applied to human gut phage populations. Nat. Rev. Microbiol. 2012, 10, 607–610. [Google Scholar] [CrossRef] [PubMed]
- Dabrowska, K.; Switała-Jelen, K.; Opolski, A.; Weber-Dabrowska, B.; Gorski, A. Bacteriophage penetration in vertebrates. J. Appl. Microbiol. 2005, 98, 7–13. [Google Scholar] [CrossRef] [PubMed]
- Sarker, S.A.; McCallin, S.; Barretto, C.; Berger, B.; Pittet, A.C.; Sultana, S.; Krause, L.; Huq, S.; Bibiloni, R.; Bruttin, A.; et al. Oral T4-like phage cocktail application to healthy adult volunteers from Bangladesh. Virology 2012, 434, 222–232. [Google Scholar] [CrossRef] [Green Version]
- Wright, A.; Hawkins, C.H.; Änggård, E.E.; Harper, D.R. A controlled clinical trial of a therapeutic bacteriophage preparation in chronic otitis due to antibiotic-resistant Pseudomonas aeruginosa; a preliminary report of efficacy. Clin. Otolaryngol. 2009, 34, 349–357. [Google Scholar] [CrossRef]
- Górski, A.; Miedzybrodzki, R.; Borysowski, J.; Dabrowska, K.; Wierzbicki, P.; Ohams, M.; Korczak-Kowalska, G.; Olszowska-Zaremba, N.; Łusiak-Szelachowska, M.; KŁak, M.; et al. Phage as a Modulator of Immune Responses: Practical Implications for Phage Therapy. Adv. Virus Res. 2012, 83, 41–71. [Google Scholar] [PubMed]
- Przerwa, A.; Zimecki, M.; Switała-Jelen, K.; Dabrowska, K.; Krawczyk, E.; Łuczak, M.; Weber-Dabrowska, B.; Syper, D.; Miedzybrodzki, R.; Górski, A. Effects of bacteriophages on free radical production and phagocytic functions. Med. Microbiol. Immunol. 2006, 195, 143–150. [Google Scholar] [CrossRef]
- Ly-Chatain, M.H. The factors affecting effectiveness of treatment in phages therapy. Front. Microbiol. 2014, 18, 51. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sulakvelidze, A.; Kutter, E. Bacteriophage Therapy in Humans. Bacteriophages: Biology and Applications; CRC Press: Boca Raton, FL, USA, 2004; pp. 381–436. [Google Scholar]
- Roach, D.R.; Leung, C.Y.; Henry, M.; Morello, E.; Singh, D.; Di Santo, J.P. Synergy between the host immune system and bacteriophage is essential for successful phage therapy against an acute respiratory pathogen. Cell Host Microb. 2017, 22, 38.e–47.e. [Google Scholar] [CrossRef]
- Miernikiewicz, P.; Dąbrowska, K.; Piotrowicz, A.; Owczarek, B.; Wojas-Turek, J.; Kicielińska, J.; Rossowska, J.; Pajtasz-Piasecka, E.; Hodyra, K.; Macegoniuk, K.; et al. T4 phage and its head surface proteins do not stimulate inflammatory mediator production. PLoS ONE 2013, 8, e71036. [Google Scholar]
- Pajtasz-Piasecka, E.; Rossowska, J.; Duś, D.; Weber-Dabrowska, B.; Zabłocka, A.; Górski, A. Bacteriophages support anti-tumor response initiated by DC-based vaccine against murine transplantable colon carcinoma. Immunol. Lett. 2008, 116, 24–32. [Google Scholar] [CrossRef]
- Yıldızlı, G.; Coral, G.; Ayaz, F. Immunostimulatory Activities of Coliphages on In Vitro Activated Mammalian Macrophages. Inflammation 2020, 43, 595–604. [Google Scholar] [CrossRef]
- Srivastava, A.S.; Kaido, T.; Carrier, E. Immunological factors that affect the in vivo fate of T7 phage in the mouse. J. Virol. Meth. 2004, 115, 99–104. [Google Scholar] [CrossRef]
- Gogokhia, L.; Buhrke, K.; Bell, R.; Hoffman, B.; Brown, D.G.; Hanke-Gogokhia, C.; Ajami, N.J.; Wong, M.C.; Ghazaryan, A.; John, F.; et al. Expansion of Bacteriophages Is Linked to Aggravated Intestinal Inflammation and Colitis. Cell Host Microb. 2019, 25, 285–299. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Majewska, J.; Kaźmierczak, Z.; Lahutta, K.; Lecion, D.; Szymczak, A.; Miernikiewicz, P.; Drapała, J.; Harhala, M.; Marek-Bukowiec, K.; Jędruchniewicz, N.; et al. Induction of Phage-Specific Antibodies by Two Therapeutic Staphylococcal Bacteriophages Administered per os. Front. Immunol. 2019, 10, 2607. [Google Scholar] [CrossRef]
- Anand, T.; Virmani, N.; Kumar, S.; Mohanty, A.K.; Pavulraj, S.; Bera, B.C.; Vaid, R.K.; Ahlawat, U.; Tripathi, B.N. Phage therapy for treatment of virulent Klebsiella pneumoniae infection in a mouse model. J. Glob. Antimicrob. Resist. 2020, 21, 34–41. [Google Scholar] [CrossRef]
- Biswas, B.; Adhya, S.; Washart, P.; Paul, B.; Trostel, A.N.; Powell, B.; Troste, A.N.; Powell, B.; Carlton, R.; Merril, C.R. Bacteriophage therapy rescues mice bacteremic from a clinical isolate of vancomycin-resistant Enterococcus faecium. Infect. Immun. 2002, 70, 204–210. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Capparelli, R.; Nocerino, N.; Iannaccone, M.; Ercolini, D.; Parlato, M.; Chiara, M.; Iannelli, D. Bacteriophage therapy of Salmonella enterica: A fresh appraisal of bacteriophage therapy. J. Infect. Dis. 2010, 201, 52–61. [Google Scholar] [CrossRef] [Green Version]
- Langbeheim, H.; Teitelbaum, D.; Arnon, R. Cellular immune response toward MS-2 phage and a synthetic fragment of its coat protein. Cell Immunol. 1978, 38, 193–197. [Google Scholar] [CrossRef]
- Górski, A.; Ważna, E.; Dąbrowska, B.W.; Dąbrowska, K.; Świtała-Jeleń, K.; Międzybrodzki, R. Bacteriophage translocation. FEMS Immunol. Med. Microbiol. 2006, 46, 313–319. [Google Scholar] [CrossRef]
- Moye, Z.D.; Woolston, J.; Sulakvelidze, A. Bacteriophage applications for food production and processing. Viruses 2018, 10, 205. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Abedon, S.T. Ecology of anti-biofilm agents II. Bacteriophage exploitation and biocontrol of biofilm bacteria. Pharmaceuticals 2015, 8, 559–589. [Google Scholar] [CrossRef] [Green Version]
- Soffer, N.; Abuladze, T.; Woolston, J.; Li, M.; Hanna, L.F.; Heyse, S.; Charbonneau, D.; Sulakvelidze, A. Bacteriophages safely reduce Salmonella contamination in pet food and raw pet food ingredients. Bacteriophage 2016, 6, e1220347. [Google Scholar] [CrossRef] [Green Version]
- Food Safety. Available online: https://www.intralytix.com/index.php?page=food (accessed on 28 October 2021).
- Połaska, M.; Sokołowska, B. Bacteriophages—a new hope or a huge problem in the food industry. AIMS Microbiol. 2019, 5, 324–346. [Google Scholar] [CrossRef] [PubMed]
- Agricultural Biocontrol Applications. Available online: https://www.brimrosetechnology.com/biocontrol (accessed on 28 October 2021).
- Sommer, J.; Trautner, C.; Witte, A.K.; Fister, S.; Schoder, D.; Rossmanith, P.; Mester, P.J. Don’t shut the stable door after the phage has bolted—the importance of bacteriophage inactivation in food environments. Viruses 2019, 11, 468. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- PhageGuard. Available online: www.phageguard.com (accessed on 28 October 2021).
- Vikram, A.; Woolston, J.; Sulakvelidze, A. Phage biocontrol applications in food production and processing. Curr. Iss. Mol. Biol. 2020, 40, 267–302. [Google Scholar]
- U. S. Food & Drug. Available online: https://fda.report/media/111308/GRAS-Notice-000724 (accessed on 28 October 2021).
- Mai, V.; Ukhanova, M.; Reinhard, M.K.; Li, M.; Sulakvelidze, A. Bacteriophage administration significantly reduces Shigella colonization and shedding by Shigella-challenged mice without deleterious side effects and distortions in the gut microbiota. Bacteriophage 2015, 5, e1088124. [Google Scholar] [CrossRef] [Green Version]
- EFSA BIOHAZ Panel (EFSA Panel on Biological Hazards): Scientific opinion on the evaluation of the safety and efficacy of Listex TM P100 for reduction of pathogens on different ready-to-eat (RTE) food products. EFSA J. 2016, 14, 1–94.
- Chhibber, S.; Kumari, S. Application of Therapeutic Phages in Medicine, Bacteriophages, Ipek Kurtboke, IntechOpen. 2012. Available online: https://www.intechopen.com/chapters/32283 (accessed on 22 November 2021). [CrossRef] [Green Version]
- Barrow, P.A.; Soothill, J.S. Bacteriophage therapy and prophylaxis: Rediscovery and renewed assessment of potential. Trends Microbiol. 1997, 5, 268–271. [Google Scholar] [CrossRef]
- Matsuzaki, S.; Rashel, M.; Uchiyama, J.; Sakurai, S.; Ujihara, T.; Kuroda, M.; Ikeuchi, M.; Tani, T.; Fujieda, M.; Wakiguchi, H.; et al. Bacteriophage therapy: A revitalized therapy against bacterial infectious diseases. J. Infect. Chemother. 2005, 11, 211–219. [Google Scholar] [CrossRef]
- Loc-Carrillo, C.; Abedon, S.T. Pros and cons of phage therapy. Bacteriophage 2011, 1, 111–114. [Google Scholar] [CrossRef] [Green Version]
- Elbreki, M.; Ross, R.P.; Hill, C.; O’Mahony, J.; McAuliffe, O.; Coffey, A. Bacteriophages and their derivatives as biotherapeutic agents in disease prevention and treatment. J. Viruses 2014, 2014, 382539. [Google Scholar] [CrossRef] [Green Version]
- Oliveira, J.; Castilho, F.; Cunha, A.; Pereira, M.J. Bacteriophage therapy as a bacterial control strategy in aquaculture. Aquaculture Inter. 2012, 20, 879–910. [Google Scholar] [CrossRef]
- Iriarte, F.B.; Balogh, B.; Momol, M.T.; Smith, L.M.; Wilson, M.; Jones, J.B. Factors affecting survival of bacteriophage on tomato leaf surfaces. Appl. Environ. Microbiol. 2007, 73, 1704–1711. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pirnay, J.P.; Blasdel, B.G.; Bretaudeau, L.; Buckling, A.; Chanishvili, N.; Jason, R.; Corte-Real, S.; Debarbieux, L.; Dublanchet, A.; De VosJérôme, D.; et al. Quality and safety requirements for sustainable phage therapy products. Pharm. Res. 2015, 32, 2173–2179. [Google Scholar] [CrossRef] [Green Version]
- Ryan, E.M.; Gorman, S.P.; Donnelly, R.F.; Gilmore, B.F. Recent advances in bacteriophage therapy: How delivery routes, formulation, concentration and timing influence the success of phage therapy. J. Pharm. Pharmacol. 2011, 63, 1253–1264. [Google Scholar] [CrossRef] [PubMed]
- Babalova, E.G.; Katsitadze, K.T.; Sakvarelidze, L.A.; Imnaishvili, N.S.; Sharashidze, T.G.; Badashvili, V.A.; Kiknadze, G.P.; Meipariani, A.N.; Gendzekhadze, N.D.; Machavariani, E.V.; et al. Preventive value of dried dysentery bacteriophage. Zhurnal Mikrobiol. 1968, 45, 143–145. [Google Scholar]
- Litvinova, A.M.; Chtetsova, V.M.; Kavtreva, I.G. Evaluation of efficacy of the use of coli-Proteus bacteriophage in intestinal dysbacteriosis in premature infants. Voprosy Okhrany Materinstva i Detstva 1978, 23, 42–44. [Google Scholar]
- Meladze, G.D.; Mebuke, M.G.; Chkhetia, N.S.; Kiknadze, N.I.; Koguashvili, G.G.; Timoshuk, I.I.; Larionova, N.G.; Vasadze, G.K. The efficacy of staphylococcal bacteriophage in treatment of purulent diseases of lungs and pleura. Grudn. Khir. 1982, 1, 53–56. [Google Scholar]
- Bogovazova, G.G.; Voroshilova, N.N.; Bondarenko, V.M. The efficacy of Klebsiella pneumoniae bacteriophage in the therapy of experimental Klebsiella infection. Zhurnal Mikrobiol. Epidemiol. Immunobiol. 1991, 4, 5–8. [Google Scholar]
- Johnson, R.P.; Gyles, C.L.; Huff, W.E.; Ojha, S.; Huff, G.R.; Rath, N.C.; Donoghue, A.M. Bacteriophages for prophylaxis and therapy in cattle, poultry and pigs. Anim. Health Res. Rev. 2008, 9, 201–215. [Google Scholar] [CrossRef]
- Smith, H.W.; Huggins, M.B. Effectiveness of phages in treating experimental Escherichia coli diarrhoea in calves, piglets and lambs. J. Gen. Microbiol. 1983, 129, 2659–2675. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- O’Flaherty, S.; Ross, R.P.; Meaney, W.; Fitzgerald, G.F.; Elbreki, M.F.; Coffey, A. Potential of the polyvalent anti-Staphylococcus bacteriophage K for control of antibiotic-resistant staphylococci from hospitals. Appl. Environ. Microb. 2005, 71, 1836–1842. [Google Scholar] [CrossRef] [Green Version]
- Ngassam-Tchamba, C.; Duprez, J.N.; Fergestad, M.; De Visscher, A.; L’Abee-Lund, T.; De Vliegher, S.; Wasteson, Y.; Touzain, F.; Blanchard, Y.; Lavigne, R.; et al. In Vitro and in Vivo Assessment of Phage Therapy against Staphylococcus Aureus Causing Bovine Mastitis. J. Glob. Antimicrob. Resist. 2020, 22, 762–770. [Google Scholar] [CrossRef] [PubMed]
- Meira, E.B.S.; Rossi, R.S.; Teixeira, A.G.; Kaçar, C.; Oikonomou, G.; Gregory, L. Bicalho, R.C. The effect of prepartum intravaginal bacteriophage administration on the incidence of retained placenta and metritis. J. Dairy Sci. 2013, 96, 7658–7665. [Google Scholar] [CrossRef] [PubMed]
- Titze, I.; Lehnherr, T.; Lehnherr, H.; Krömker, V. Efficacy of bacteriophages against Staphylococcus aureus isolates from bovine mastitis. Pharmaceuticals 2020, 13, 35. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mendes, J.J.; Leandro, C.; Corte-Real, S.; Barbosa, R.; Cavaco-Silva, P.; Melo-Cristino, J.; Górski, A.; Garcia, M. Wound healing potential of topical bacteriophage therapy on diabetic cutaneous wounds. Wound Repair. Regen. 2013, 21, 595–603. [Google Scholar] [CrossRef] [PubMed]
- Wall, S.K.; Zhang, J.; Rostagno, M.H.; Ebner, P.D. Phage therapy to reduce preprocessing Salmonella infections in market-weight swine. Appl. Environ. Microbiol. 2010, 76, 48–53. [Google Scholar] [CrossRef] [Green Version]
- Jamalludeen, N.; Johnson, R.P.; Shewen, P.E.; Gyles, C.L. Evaluation of bacteriophages for prevention and treatment of diarrhea due to experimental enterotoxigenic Escherichia coli O149 infection of pigs. Vet. Microbiol. 2009, 136, 135–141. [Google Scholar] [CrossRef] [PubMed]
- Saez, A.C.; Zhang, J.; Rostagno, M.H.; Ebner, P.D. Direct Feeding of Microencapsulated Bacteriophages to Reduce Salmonella Colonization in Pigs. Foodborne Pathog. Dis. 2011, 8, 1269–1274. [Google Scholar] [CrossRef]
- Seo, B.J.; Song, E.T.; Lee, K.; Kim, J.W.; Jeong, C.G.; Moon, S.H.; Son, J.S.; Kang, S.H.; Cho, H.S.; Jung, B.Y.; et al. Evaluation of the broad-spectrum lytic capability of bacteriophage cocktails against various Salmonella serovars and their effects on weaned pigs infected with Salmonella Typhimurium. J. Vet. Med. Sci. 2018, 80, 851–860. [Google Scholar] [CrossRef] [Green Version]
- Drilling, A.; Morales, S.; Boase, S.; Jervis-Bardy, J.; James, C.; Jardeleza, C.; Tan, N.C.; Cleland, E.; Speck, P.; Vreugde, S.; et al. Safety and efficacy of topical bacteriophage and ethylenediaminetetraacetic acid treatment of Staphylococcus aureus infection in a sheep model of sinusitis. Int. Forum Allergy Rhinol. 2014, 4, 176–186. [Google Scholar] [CrossRef]
- Bach, S.J.; Johnson, R.P.; Stanford, K.; McAllister, T.A. Bacteriophages reduce Escherichia coli O157: H7 levels in experimentally inoculated sheep. Can. J. Anim. Sci. 2009, 89, 285–293. [Google Scholar] [CrossRef] [Green Version]
- Atterbury, R.J.; Van Bergen, M.A.P.; Ortiz, F.; Lovell, M.A.; Harris, J.A.; De Boer, A.; Wagenaar, J.A.; Allen, V.M.; Barrow, P.A. Bacteriophage Therapy To Reduce Salmonella Colonization of Broiler Chickens. Appl. Environ. Microbiol. 2007, 73, 4543–4549. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ma, Y.-H.; Islam, G.S.; Wu, Y.; Sabour, P.M.; Chambers, J.R.; Wang, Q.; Wu, S.X.Y.; Griffiths, M.W. Temporal distribution of encapsulated bacteriophages during passage through the chick gastrointestinal tract. Poultry Sci. 2016, 95, 2911–2920. [Google Scholar] [CrossRef] [PubMed]
- Hammerl, J.A.; Jäckel, C.; Alter, T.; Janzcyk, P.; Stingl, K.; Knüver, M.T.; Hertwing, S. Reduction of Campylobacter jejuni in Broiler Chicken by Successive Application of Group II and Group III Phages. PLoS ONE 2014, 9, e114785. [Google Scholar]
- Goode, D.; Allen, V.M.; Barrow, P.A. Reduction of experimental Salmonella and Campylobacter contamination of chicken skin by application of lytic bacteriophages. Appl. Environ. Microbiol. 2003, 69, 5032–5036. [Google Scholar] [CrossRef] [Green Version]
- Colom, J.; Cano-Sarabia, M.; Otero, J.; Aríñez-Soriano, J.; Cortés, P.; Maspoch, D.; Llagostera, M. Microencapsulation with alginate/CaCO 3: A strategy for improved phage therapy. Sci. Rep. 2017, 7, 1–10. [Google Scholar]
- El-Gohary, F.A.; Huff, W.E.; Huff, G.R.; Rath, N.C.; Zhou, Z.Y.; Donoghue, A.M. Environmental augmentation with bacteriophage prevents colibacillosis in broiler chickens1. Poult. Sci. 2014, 93, 2788–2792. [Google Scholar] [CrossRef]
- Bhandare, S.; Colom, J.; Baig, A.; Ritchie, J.M.; Bukhari, H.; Shah, M.A.; Sarkar, B.L.; Su, J.; Wren, B.; Barrow, P.; et al. Reviving Phage Therapy for the Treatment of Cholera. J. Infect. Dis. 2019, 219, 786–794. [Google Scholar] [CrossRef]
- Trigo, G.; Martins, T.G.; Fraga, A.G.; Longatto-Filho, A.; Castro, A.G.; Azeredo, J.; Pedrosa, J. Phage therapy is effective against infection by Mycobacterium ulcerans in a murine footpad model. PLoS Negl. Trop Dis. 2013, 7, e2183. [Google Scholar] [CrossRef] [Green Version]
- El-Aziz, A.M.A.; Elgaml, A.; Ali, Y.M. Bacteriophage Therapy Increases Complement-Mediated Lysis of Bacteria and Enhances Bacterial Clearance After Acute Lung Infection With Multidrug-Resistant Pseudomonas aeruginosa. J. Infect. Dis. 2019, 219, 1439–1447. [Google Scholar] [CrossRef] [PubMed]
- Jeon, J.; Ryu, C.-M.; Lee, J.-Y.; Park, J.-H.; Yong, D.; Lee, K. In Vivo Application of Bacteriophage as a Potential Therapeutic Agent To Control OXA-66-Like Carbapenemase-Producing Acinetobacter baumannii Strains Belonging to Sequence Type 357. Appl. Environ. Microbiol. 2016, 82, 4200–4208. [Google Scholar] [CrossRef] [Green Version]
- Chadha, P.; Katare, O.P.; Chhibber, S. In vivo efficacy of single phage versus phage cocktail in resolving burn wound infection in BALB/c mice. Microb. Pathogen. 2016, 99, 68–77. [Google Scholar] [CrossRef] [PubMed]
- Prazak, J.; Iten, M.; Cameron, D.R.; Save, J.; Grandgirard, D.; Resch, G.; Goepfert, C.; Leib, S.L.; Takala, J.; Jakob, S.M.; et al. Bacteriophages Improve Outcomes in Experimental Staphylococcus aureus Ventilator-associated Pneumonia. Am. J. Respir. Crit. Care Med. 2019, 200, 1126–1133. [Google Scholar] [CrossRef] [PubMed]
- Yen, M.; Cairns, L.S.; Camilli, A. A cocktail of three virulent bacteriophages prevents Vibrio cholerae infection in animal models. Nature Comm. 2017, 8, 1–7. [Google Scholar] [CrossRef] [Green Version]
- Schmelcher, M.; Powell, A.M.; Camp, M.J.; Pohl, C.S.; Donovan, D.M. Synergistic streptococcal phage λSA2 and B30 endolysins kill streptococci in cow milk and in a mouse model of mastitis. Appl. Micorb. Biotechnol. 2015, 99, 8475–8486. [Google Scholar] [CrossRef]


{kind=link}
| Scope of Use | Example | Host Pathogens | References |
|---|---|---|---|
| Treatment of human and animals | Gastroenteric, respiratory, urinary tract and skin infections, otitis, keratitis | E. coli, Salmonella spp., S. aureus, Pseudomonas spp., Enterococcus spp., Acinetobacter baumanni | [1] |
| Prophylaxis and treatment | Neonatal diarrhoeal infections in calves; | E. coli, | [41] |
| Campylobacter infections in broiler chickens; | Campylobacter jejuni | [42] | |
| Salmonella infections in chickens | Salmonella spp. | [43] | |
| Decontaminants | Biocontrol agents against food- and beverage-borne pathogens | Control of LAB growth during ethanol fermentation | [44,45] |
| Biosanitization | On equipment surfaces to eradicate biofilms in food production; on plastic, glass, and ceramic surfaces in hospitals | S. aureus, E. coli, P. aeruginosa, L. monocytogenes Acinetobacter baumannii | [46,47] |
| Bio-preservation | Highly processed products with a short shelf life | Listeria monocytogenes; Campylobacter spp. | [48] |
| Agriculture | Biocontrol of plant pathogens, i.e., potato and tomato diseases; onion scab; lettuce and leek diseases; fruit tree diseases; cultivated mushrooms | Pseudomonas spp., Xanthomonas spp., Erwinia spp., Ralstonia spp., Agrobacterium spp., Xylella spp., Pectobacterium spp., Dickeya spp. Pleurotus ostreatus | [49] |
| Aquaculture | Biocontrol of fish pathogens in commercial fish farming | Mainly to Vibrio spp., less to Edwardsiella spp., Lactococcus spp., Pseudomonas spp., Aeromonas spp., Flavobacterium spp. | [49] |
| Kind of Phage | Form of Application | Animal Model | Influence on Immune Parameters | References |
|---|---|---|---|---|
| Pseudomonas spp. bacteriophage (PA1Ø) | 100 µL of PA1Ø (5 × 104 PFU; 5 × 107 PFU (10 MOI) or 5 × 108 PFU (100 MOI) in a single i.p. dose | 4–5-week-old male ICR mice weighing 24–26 g | Increase in phagocytosis (killing effect of PA1Ø + PMN up to 6 h after application) | [65] |
| Pseudomonas aeruginosa phage PAK_P1 | Intranasally at a curative dose of 1.0 × 108 PFU or 1.0 × 109 PFU | Wild-type BALB/c (C), wild-type C57Bl6/J (B6) | Increase in neutrophil activity, NK cells; reduced production of IFNγ and TNFα | [75] |
| Cronobacter sakazakii ES2 phage | Phage suspension 106 PFU·mL−1 in vitro | 6–8-week-old C57BL/6 mice | Increase in expression of maturation markers CD86, CD40, and MHC II; stimulation of induction of NF-κBp65-mediated-IL-12p40; stimulation of IL-12 expression; suppression of IL-6, TNF-α, IL-1β, and IFN-γ | [62] |
| E. coli T4 phage | Intraperitoneal injection at 20 µg/mouse | Female C57Bl6/J (6–8-week-old) mice | No effect on production of cytokines IL-1α, IL-6, IL-12, and TNF-α; minor changes in expression of MHC II, CD40, CD86, and CD80 | [76] |
| E.coli T4 bacteriophages | T4 phages 5 × 108 PFU/mL | 8–12-week-old female C57BL/6 mice | Inhibition of specific antibody response; reduction in bacteria-induced ROS production by phagocytic cells; antitumour response; activation of T cells for IFN-γ production | [77] |
| E. coli P1 and P2 phages | 106 PFU/mL in vitro | Mice | Stimulation of TNFα; stimulation of macrophage activity in vitro | [78] |
| Wild-type E. coli T7 phage | 109 PFU/mL injected in vitro into tail vein of mice | Adult female C57BL/6J, SCID (C57BL/6J-Prkdcscid), B-cell-deficient (C57BL/10-Igh-6tm1Cgn) and T-cell deficient (C57BL/6J-Hfh11nu) mice | Spontaneous antibodies, mainly IgM, observed in sera; slight effect on NK activation; anti-inflammatory effect—ROS suppression | [79] |
| Wild-type E.coli φ26, φ27, φ29 | 107–108 PFU/mL for 5 days per rectum as suppositories | 25 newborn HF calves aged 1 d to 2 weeks | Significant increase in IgG and IgA production stimulation of nonspecific immune response—IFNγ, lysozyme; activation of acute phase response SAA and HP | [41] |
| Wild-type E.coli phage and bacteriophage genomes NC-A: MK310182; NC-B: MK310183; NC-G: MK310184 | 3 × 107 PFU/mL of phage mixture with drinking water | 8-week-old germ-free Swiss Webster mice | Whole bacteriophages and phage DNA stimulated IFN-γ via nucleotide-sensing receptor TLR9 | [80] |
| S. aureus vB_SauM_JS25 phage | MAC-T cells pre-treated with vB_SauM_JS25 phage 108 PFU/well for 3 h | In vitro MAC-T bovine mammary epithelial cells | Reduction in TNF-α, IL-1β, IL-6, IL-8, and IL-10 | [54] |
| Staphylococcus spp. bacteriophage A3R or 676Z | 3 doses of 1010 PFU/mouse in drinking water and peritoneally | C57BL/6J normal male mice | Induction of specific antibodies in blood (IgM, IgG, IgA) | [81] |
| Klebsiella pneumoniae MTCC109 bacteriophage PA43 | Intranasal application of 109 PFU BPA43 phage after 2 h of bacterial infection | BALB/c mice, 6–8 weeks old, weight 20–25 g | Suppression of local inflammatory reaction in lungs; suppression of migration of lymphocytes and macrophages | [82] |
| Commercial Phage Product | Target Bacteria | Company | Target Food Products | Country Approving Product | References |
|---|---|---|---|---|---|
| SalmoLyse® | Salmonella spp. | Intralytix, Inc., USA | Raw pet food ingredients; meat products: chicken, tuna, turkey; plant products: cantaloupe, lettuce | USA | [89] |
| SalmoFreshTM | Salmonella spp. | Intralytix Inc., USA | Poultry, fish and shellfish, fresh and processed fruits and vegetables | USA, Canada, Israel | [90] |
| PhageGuard S SalmonelexTM | Salmonella spp. | Micreos Food Safety/Nederlands | Fresh poultry meat | USA, Canada, Australia, Israel | [91] |
| Bafasal® | Salmonella spp., Aeromonas spp. Pseudomonas spp., Yersinia spp. | Proteon Pharmaceuticals (Łódź, Poland) | Regulatory-approved poultry feed | Poland | [9] |
| EnkoPhagum | Salmonella spp., Shigella spp.; enteropathogenic E. coli; Staphylococcus spp. | Brimrose Technology Corporation (Sparks Glencoe, MD, USA) | Meat products | Georgia | [92] |
| BacWash TM | Salmonella spp. | OmniLytics Inc. (Sandy, UT, USA) | For disinfection of skin of live animals prior to slaughter | USA | [4] |
| Biotector® S | Salmonella Gallinarum S. Pullorum | CJ CheilJedang Research Institute of Biotechnology (Seoul, Korea) | In animal feed to control Salmonella in poultry | South Korea | [93] |
| PhageGuard STM | Salmonella | Micreos Food Safety BV (Wageningen, The Netherlands) | Fresh poultry meat | Netherlands, Australia, Canada, USA | [87,94] |
| EcoShield TM | Escherichia coli O157:H7 | Intralytix Inc. (Columbia, MD, USA) | Kosher meat (ground beef); vegetables (tomatoes, broccoli, spinach); lettuce and cantaloupe; leafy greens | USA | [9,91,95] |
| Secure Shield E1 | Escherichia coli O157:H7 | FINK TEC GmbH (Hamm, Germany) | Beef carcasses | USA | [96] |
| EcoShield PX™ | Stx Escherichia coli O157:H7 | Intralytix, Inc., Baltimore, MD, USA | Fresh-cut leafy greens; foods of plant origin, beef, chicken | USA, Canada, Israel | [90,95] |
| ShigaShield™ (ShigActive™) | Shigella spp. | Intralytix, Inc., Baltimore, MD, USA | Beef, poultry, dairy products, including cheese; fruit and vegetable surfaces | USA | [90,97] |
| ListShield™ | Listeria monocytogenes | Intralytix, Inc., Baltimore, MD, USA | Food biopreservative in meat and poultry products | USA, Canada, Israel | [9,87,90] |
| Listex P100 PhageGuard Listex™ | Listeria monocytogenes | Micreos Food Safety, Wageningen, Netherlands | Beef and turkey meat; fish and shellfish; dairy products; red smear soft cheese, smoked salmon and fresh salmon; frozen vegetables | USA, Australia, New Zealand, Israel, Switzerland, the Netherlands | [87,98] |
| ListPhage™ | Listeria monocytogenes | Intralytix, Inc., Baltimore, MD, USA | Pet food | USA, EU | [91] |
| Agriphage™ | Xanthomonas campestris pv. vesicatoria, Pseudomonas syringae pv. tomato | OmniLytics Inc., USA | Foods of plant origin, especially tomatoes and peppers | USA | [91] |
| Agriphage-Fire Blight | Erwinia amylovora | OmniLytics Inc., USA | Surfaces of apples and pears | USA | [91] |
| Biolyse™ | Erwinia, Pectobacterium, Pseudomonas | APS Biocontrol Ltd./Dundee, UK | Vegetables, including potatoes | UK, Europe | [91] |
| Animal Species | Pathogen Species | Phage Treatment | Results | Treatment Procedure | References |
|---|---|---|---|---|---|
| Cattle–newborn Holstein-Friesian heifers | E. coli O9:K30.99 106 CFU mL−1 | Oral administration of phage cocktail (B44/1 and B44/2), 1011 PFU mL−1 | 100 % reduction of mortality in calves; Significant reduction (93%) of morbidity of bacterial diarrhoea; high protection against ETEC infections | Treatment of diarrhoea | [113] |
| Cattle–Holstein-Friesian dairy cows | Staphylococcus aureus | Direct infusions into teats with bacteriophage K cocktail (CS1, DW2) (108 PFU ml−1) | About 10,000-fold reduction of S. aureus in udder; lower presence of somatic cells in milk | Treatment of subclinical mastitis | [114] |
| 20 female BALB/cJRj (SPF) mice | Staphylococcus aureus causing mastitis in cows | Inoculation with 108 PFU of ISP phage mixture into mammary glands | Significant reduction of bacterial count; reduction or lack of clinical changes in mammary glands | Antibacterial activity and therapeutic effect | [115] |
| 280 Holstein-Friesian lactating cows with metritis during the first and second lactations | Escherichia coli strains causing metritis | Intravaginal administration of 20 mL 10-phage cocktail 109 PFU mL−1 at 230, 260 and 275 days of gestation | Lack of antibacterial effect; no prophylactic effect in prevention of metritis; increased incidence of retained placenta | Failure of therapeutic and prophylactic effect in metritis | [116] |
| 25 newborn Holstein-Friesian heifers aged 0–14 days old | E. coli causing diarrhoea in newborn calves | Rectal application as suppositories of phage cocktail (26, 27, 29 at 107 to 109 PFU mL−1) mixed with Lactobacillus spp. strains for 5 days | Significant reduction of clinical signs and duration of diarrhoea <24h; significant reduction of ETEC content in faeces 2 log10 CFU/mL; protection against re-infection for 3 weeks after treatment; immunomodulatory effect | Prophylactic and therapeutic effect against diarrhoea | [41] |
| Holstein-Friesian dairy cows with clinical or subclinical mastitis | S. aureus strains obtained from cows with subclinical and clinical mastitis, pig farm and human infections | 0.1 mL phage cocktail (STA1.ST29, EB1.ST11, and 27) 1.2 × 108 PFU/mL or 1.2 × 109 PFU/mL against S. aureus inoculated into about 5.0 mL of milk obtained from cows with mastitis | Significant reduction of S. aureus in milk–2 log10 CFU/mL in vitro | Antibacterial activity | [117] |
| 3 female Yorkshire pigs weighing~60 kg | S. aureus ulcers | S. aureus F44/10 and F125/10, inoculated topically at 108 to 109 PFU | Slight reduction of S. aureus strains, reduction of ulcerous changes | Therapeutic effect on skin ulcers | [118] |
| 16 small pigs 3 to 4 weeks old | Salmonella enterica ser. Typhimurium at 5 × 108 CFU mL | Microencapsulated alginate beads containing 16-phage cocktail (SEP-1, SGP-1, STP-1, SS3eP-1, STP-2, SChP-1, SAP-1, SAP-2), ∼109 to 1010 PFU/mL by gavage | Significant early reduction (99%) in concentration of S. Typhimurium 2 to 3 log10 CFU/g in the ileum, caecum and tonsils; significant influence on health status and AWG of pigs | Prophylactic and therapeutic effect | [119] |
| 3-week-old weaned pigs | E. coli (ETEC); O149:H10:F4 | Oral administration of phage cocktail GJ1–GJ7 or mono-phage: prophylactic 1010 PFU/pig or therapeutic 108 PFU/pig | Significant reduction of diarrhoea; reduction of duration of diarrhoea <2 days, mean diarrhoea score, and mean composite diarrhoea score significant reduction of ETEC strains; protection against diarrhoea | Prophylactic and therapeutic effect against diarrhoea | [120] |
| Weaned pigs >4 weeks old | Oral challenge with 5 mL of 109 CFU/mL Salmonella Typhimurium | Microencapsulated phage cocktail in feed (5 × 1011 PFU) for 5 days before challenge with Salmonella Typhimurium | Reduction of S. Typhimurium in ileum and caecum by about 1 log10 CFU/g | Therapeutic and prophylactic effect | [121] |
| 4-week-old weaned pigs | Salmonella enterica serovar Typhimurium | 5 mL of a 8- phage cocktail at 109 PFU/mL (SEP-1, SGP-1, STP-1, SS3eP-1, STP-2, SChP-1, SAP-1, SAP-2) | Significant reduction of Salmonella Typhimurium; 100% lytic activity against 34 Salmonella reference strains and 92.5% lytic activity against 107 wild strains | Therapeutic effect in diarrhoea | [122] |
| Merino cross wethers sheep (1 year of age) | S. aureus strain ATCC 25923 | Phage cocktail CTSA 2 × 108 PFU/mL applied to right and left sinuses | Reduction of tissue damage; reduction of S. aureus colonization | Therapeutic and antibacterial activity | [123] |
| 20 Canadian Arcott rams weighing 50 kg | E. coli O157:H7(109 CFU/mL | Oral administration of E. coli phage cocktail P5, P8 and P11 (1010 PFU) administered orally 5 times using a sterile 60-mL syringe and stomach tube | Significant reduction~2 log10 CFU of intestinal E. coli O157:H7 in sheep; total elimination of bacteria in 30% of animals | Prophylactic and therapeutic effect | [124] |
| Ross broiler chickens at 34 d of age | S. enterica ser. Enteritidis P125109; S. enterica serotype Typhimurium 4/74; S. enterica serotype Hadar 18 | Bacteriophage suspensions as antacid administered by oral gavage 9.0 or 11.0 log10 PFU of φ151 (S. enterica ser. Enteritidis), φ25 (S. enterica ser. Hadar), or φ10 (S. enterica ser. Typhimurium) | Significant reduction of S. enterica ser. Enteritidis and Typhimurium caecal colonization by ≥4.2 log10 CFU within 24 h | Therapeutic and prophylactic effect | [125] |
| Young chicks | Salmonella Typhimurium DT104 | Single oral dose of phage FO1 of 109 (PFU)/chick in encapsulated form | Reduction of Salmonella Typhimurium strains in caecum | Antibacterial effect | [126] |
| Vrolix chicks aged 20 days | Campylobacter jejuni | 3-bacteriophage cocktail 5 × 108 PFU of CP14, CP81 or CP68 | Reduction of C. jejuni strains in caeca by approx. 3 log10 CFU units | Antibacterial and protective effect | [127] |
| Chickens | Campylobacter jejuni; S. enterica serovar Enteritidis | Direct inoculation onto chicken skin, C. jejuni typing phage 12673 at 106 PFU/cm2 of skin; S. enterica serovar Enteritidis phage P22, phage 29C, 103 PFU/cm2 of skin | Significant reduction of Campylobacter up to 2 log10 per unit area of skin within 48 h; reduction of C. jejuni ~2 log10 on experimentally contaminated chicken skin after phage application | Therapeutic and antibacterial effect | [128] |
| Ross strain 308 commercial chicken broilers | Salmonella enterica | 3-phage cocktail, liposome/alginate, encapsulated, 1010 PFU/animal for 9 days | Significant decrease in Salmonella spp. concentration (~50%) in caeca | Antibacterial activity | [129] |
| Broiler chickens (Cobb 500) at 1 d of age | E. coli ser 02 | Sprayed with 200 mL of 8 × 108 PFU/mL phage SPR02 | Significant reduction of mortality by >10% | Antibacterial and protective effect | [130] |
| 8-day-old quail | Oral challenge with 100 μL of 1.2 × 109 CFU ml−1 S. Enteritidis | Oral application of 100 μL of 106 PFU ml−1 bacteriophage for 3 days | Reduction of S. Enteritidis in caecal tonsils of Japanese quails to 33.3 and 20%, 24 h and 7 days after application; prophylactic effect against S. Enteritidis colonization, increase in resistance against Salmonella challenge | Prophylactic effect | [43] |
| 2-day-old New Zealand White rabbits | Oral infection with Vibrio cholerae 8 × 108 CFU | Oral application of 3 phages (Phi_2, 24 and X29) 109 PFU | Reduction of bacteria count up to 4 log10 CFU/g; full protection against clinical signs of disease | Prophylactic and therapeutic effects | [131] |
| 120 eight-week-old female BALB/c mice | Mycobacterium ulcerans as ulcerous infections | Single dose of mycobacteriophage D29 108 PFU/mouse administered 33 days post infection | Progressive reduction of footpad swelling by day 150 post-infection significant reduction of M. ulcerans~1.5–2 log10 CFU/ml | Therapeutic effect and antipathogenic activity effect | [132] |
| Mice | Pseudomonas aeruginosa | Bacteriophage PAK_P1 intranasally at curative dose of 1.0 × 108 PFU/mL or prophylactic dose of 1.0 × 109 PFU (MOI 100) | Prophylaxis of acute respiratory infections caused by P. aeruginosa; significant reduction of clinical signs; resistance to infection; stimulation of immune response | Therapeutic and prophylactic effect | [75] |
| BALB-C female mice aged 10 weeks | Pseudomonas aeruginosa | Single dose of phage MMI-Ps1 107 PFU suspension by intranasal application | Prophylaxis against P. aeruginosa infection; significant reduction of bacterial content in lungs about 2 log10 | Protective and antibacterial effect | [133] |
| Female mice C57BL/6 mice, aged 7 to 8 weeks | Acinetobacter baumanni | A. baumanni phage Bϕ-C62 inoculated intranasally (1 × 1010 PFU/ml | 100% survival after challenge with A. baumanni | Therapeutic effect, slight immunostimulatory effect | [134] |
| BALB/c mice aged 6–8 weeks | Klebsiella pneumonia-induced pneumonia | Bacteriophage suspension 2 × 109 PFU/mouse applied in a single dose i.n. | Significant decrease in duration of illness and microscopic lesions; suppression of necrosis, bronchiolitis, and infiltration of inflammatory cells | Therapeutic effect | [82] |
| BALB/c mice | Klebsiella pneumoniae B5055 | 50 μL of 108 PFU/mL single and 5-phage cocktail applied topically at wound site (Kpn1, Kpn2, Kpn3, Kpn4 and Kpn5) | Significant reduction of K. pneumoniae load to 4.32, 4.64, 4.42, 4.11 and 4.27 log CFU/mL; rapid healing of wounds in all phage-treated groups | Therapeutic and antibacterial activity | [135] |
| Male Wistar rats; 9–10 weeks old | Staphylococcus aureus-associated pneumonia | Intravenous application of cocktail of 4 phages (2–3 × 109 PFU/mL of 2003, 2002, 3A, and K | Increase in survival from 0% to 58% significant reduction of bacterial content in the lung (1.2 × 106 CFU/g of tissue for survivors vs. 1.2 × 109 CFU/g for nonsurviving animals); reduction of lung damage | Therapeutic and immunomodulatory effect; antibacterial activity | [136] |
| New Zealand White infant rabbits (aged 3 days) and CD-1 infant mice (aged 4 and 5 days) | Vibrio cholerae; oral administration of 5 × 108 CFU/rabbit or mouse | Oral administration of phage cocktail (3 × 107 or 108 PFU/rabbit or mouse) | Protective effect against cholera via significant reduction of caecal colonization by V. cholerae; protection against cholera-like diarrhoea | Prophylactic and therapeutic effect | [137] |
| New Zealand White rabbits 2-day-old | Vibrio cholera 5 × 108 CFU per animal | Phage Phi_1 at 1 × 109 PFU/animal orally administered either 6 h before or 6 h after bacterial challenge | Protection against clinical signs of cholera; lack of diarrhoea; significant reduction of 2–4 log10 CFU/g V. cholera | Prophylactic and therapeutic effect | [131] |
| Female C57BL6/SJL mice as cow mastitis infection model | Streptococcus dysgalactiae NRRL B-65273, S. agalactiae NRRL B-65272, and S. uberis NRRL B-65274 | Direct application into mammary gland: Streptococcus spp. phage endolysins 25 μg/gland for λSA2, 250 μg/gland for B30, and 12.5 (λSA2) + 125 (B30) μg/gland | Significant reduction of S. dysgalactiae content by 3.5 log10 CFU; S. agalactiae (2 log); S. uberis (4 log); protection against clinical signs of mastitis | Therapeutic effect and antibacterial activity | [138] |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Alomari, M.M.M.; Dec, M.; Urban-Chmiel, R. Bacteriophages as an Alternative Method for Control of Zoonotic and Foodborne Pathogens. Viruses 2021, 13, 2348. https://doi.org/10.3390/v13122348
Alomari MMM, Dec M, Urban-Chmiel R. Bacteriophages as an Alternative Method for Control of Zoonotic and Foodborne Pathogens. Viruses. 2021; 13(12):2348. https://doi.org/10.3390/v13122348
Chicago/Turabian StyleAlomari, Mohammed Mijbas Mohammed, Marta Dec, and Renata Urban-Chmiel. 2021. "Bacteriophages as an Alternative Method for Control of Zoonotic and Foodborne Pathogens" Viruses 13, no. 12: 2348. https://doi.org/10.3390/v13122348