
Bacteriophage Treatment: Critical Evaluation of Its Application on World Health Organization Priority Pathogens



Abstract
:1. Introduction
2. Material and Method
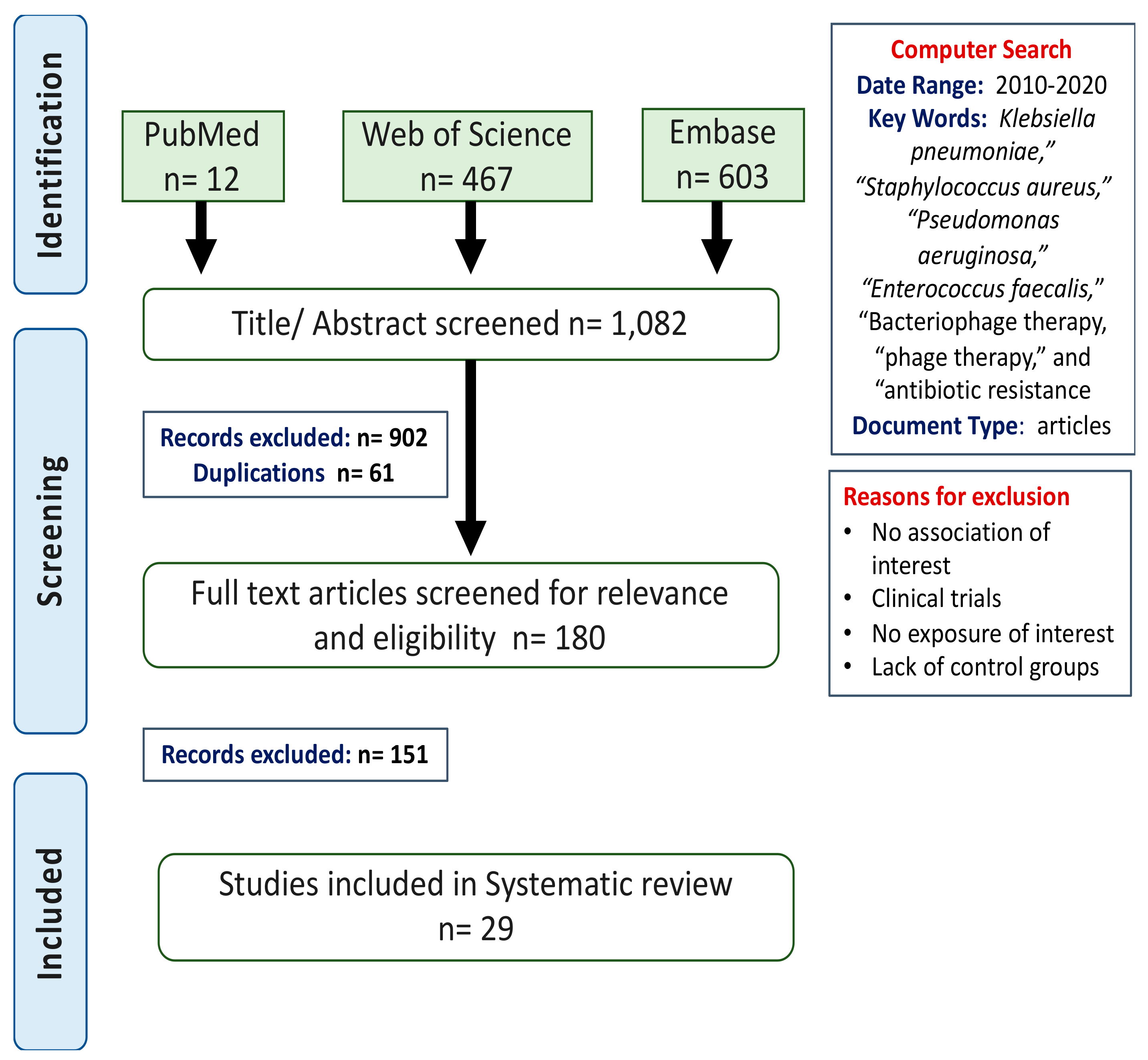
2.1. Search Methods
2.2. Study Selection and Data Collection
2.3. Critical Evaluation
3. Results
3.1. Study Characteristics
3.2. Characteristics of Model Used
3.3. Phage Isolation and Purification Protocol
3.4. Effectiveness of Phage Therapy as a Treatment Option
3.4.1. Pneumonia
3.4.2. Biofilm
3.4.3. Bloodstream Infections: Bacteremia and Sepsis
3.5. Phage Safety and Efficacy
4. Discussion
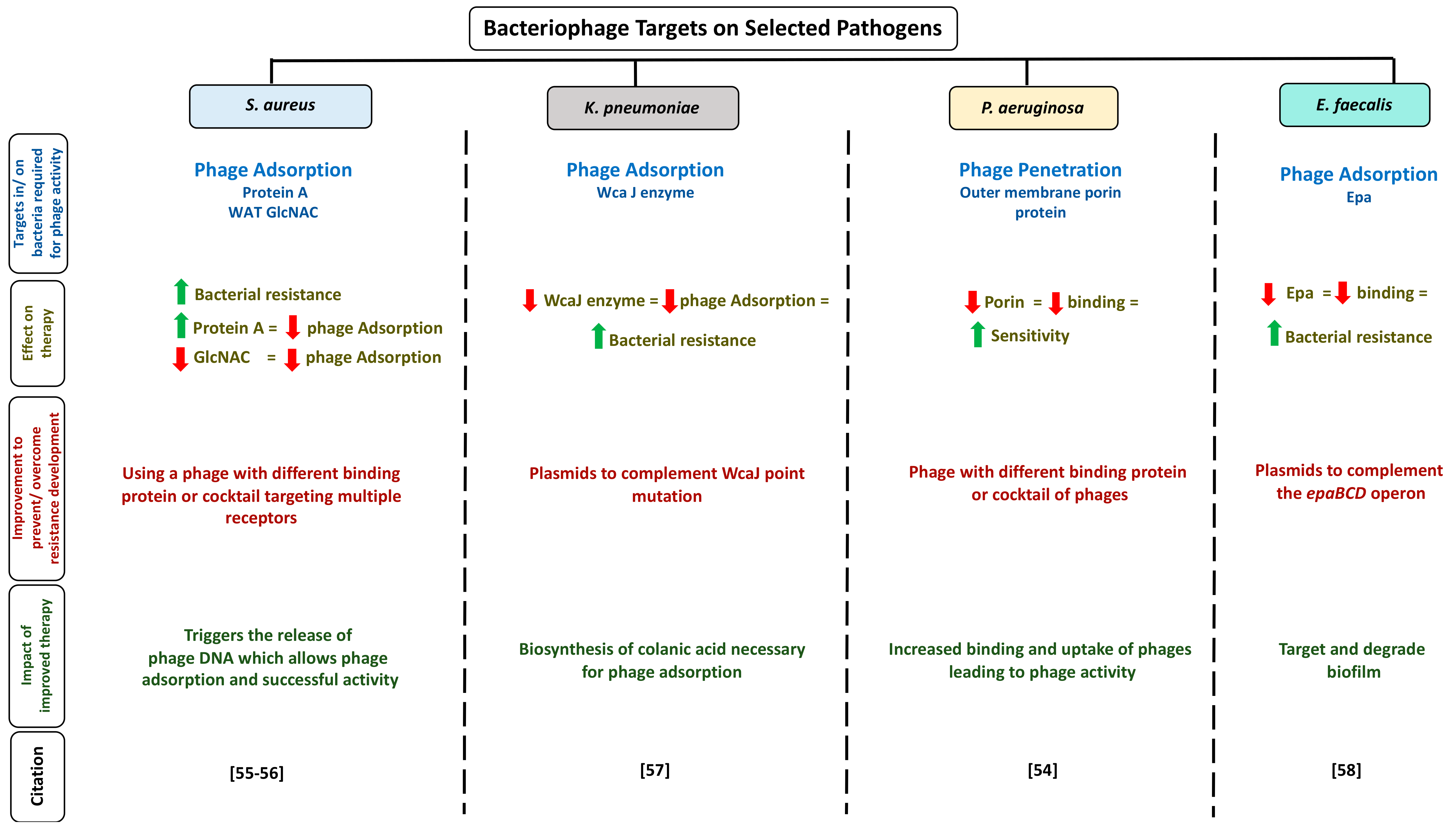
4.1. Appropriate Phage Selection for Therapy
4.2. Challenges of Phage Therapy
4.3. Recommendations for Successful Phage Therapy
4.4. Combination Therapy: Is It the Solution?
4.5. Immunological Aspects of Phage Therapy
4.6. Limitations
4.7. Future Directions
4.8. Clinical Trails Current Progress
4.9. Microbiome and Bacteriophages: Their Correlations?
5. Final Thoughts
Author Contributions
Funding
Conflicts of Interest
Abbreviations
| WHO | World Health Organization |
| S. aureus | Staphylococcus aureus |
| K. pneumoniae | Klebsiella pneumoniae |
| P. aeruginosa | Pseudomonas aeruginosa |
| E. faecalis | Enterococcus faecalis |
| PFU | Plaque forming unit |
| LB | Luria Burtani |
| CsCl | Caesium chloride |
| TNF-α | Tumour necrosis factor α |
| IL-B | Interleukin beta |
| IL-6 | Interleukin 6 |
| WAT GlcNac | Wall teichoic acid N-acetylglucosamine |
| WcaJ | Undecaprenyl-phosphate glycosyltransferase |
| EPS | Extracellular polymeric substances |
| PAS | Phage antibiotic synergy |
| ELISA | Enzyme-linked immunosorbent assay |
| DLA | Double layer agar |
References
- Sulakvelidze, A.; Alavidze, Z.; Morris, J.G., Jr. Bacteriophage therapy. Antimicrob. Agents Chemother. 2001, 45, 649–659. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Twort, F.W. An investigation on the nature of ultramicroscopic viruses. Lancet 1915, 186, 1241–1243. [Google Scholar] [CrossRef] [Green Version]
- Abedon, S.T.; Kuhl, S.J.; Blasdel, B.G.; Kutter, E.M. Phage treatment of human infections. Bacteriophage 2011, 1, 66–85. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Clokie, M.R.; Millard, A.D.; Letarov, A.V.; Heaphy, S. Phages in nature. Bacteriophage 2011, 1, 31–45. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- De Kraker, M.E.; Stewardson, A.J.; Harbarth, S. Will 10 Million People Die a Year due to Antimicrobial Resistance by 2050? PLoS Med. 2016, 13, e1002184. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kutter, E.; De Vos, D.; Gvasalia, G.; Alavidze, Z.; Gogokhia, L.; Kuhl, S.; Abedon, S.T. Phage therapy in clinical practice: Treatment of human infections. Curr. Pharm. Biotechnol. 2010, 11, 69–86. [Google Scholar] [CrossRef]
- Loc-Carrillo, C.; Abedon, S.T. Pros and cons of phage therapy. Bacteriophage 2011, 1, 111–114. [Google Scholar] [CrossRef] [Green Version]
- Lin, D.M.; Koskella, B.; Lin, H.C. Phage therapy: An alternative to antibiotics in the age of multi-drug resistance. World J. Gastrointest. Pharmacol. Ther. 2017, 8, 162–173. [Google Scholar] [CrossRef]
- Chan, B.K.; Turner, P.E.; Kim, S.; Mojibian, H.R.; Elefteriades, J.A.; Narayan, D. Phage treatment of an aortic graft infected with Pseudomonas aeruginosa. Evol. Med. Public Health 2018, 2018, 60–66. [Google Scholar] [CrossRef] [Green Version]
- Chan, B.K.; Sistrom, M.; Wertz, J.E.; Kortright, K.E.; Narayan, D.; Turner, P.E. Phage selection restores antibiotic sensitivity in MDR Pseudomonas aeruginosa. Sci. Rep. 2016, 6, 26717. [Google Scholar] [CrossRef]
- Booth, M.C.; Hatter, K.L.; Miller, D.; Davis, J.; Kowalski, R.; Parke, D.W.; Gilmore, M.S. Molecular epidemiology of Staphylococcus aureus and Enterococcus faecalis in endophthalmitis. Infect. Immun. 1998, 66, 356–360. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Furuno, J.P.; Perencevich, E.N.; Johnson, J.A.; Wright, M.O.; McGregor, J.C.; Morris, J.G.; Harris, A.D. Methicillin-resistant Staphylococcus aureus and vancomycin-resistant Enterococci co-colonization. Emerg. Infect. Dis. 2015, 11, 1539–1544. [Google Scholar] [CrossRef] [PubMed]
- Azimi, L.; Alaghehbandan, R.; Asadian, M.; Alinejad, F.; Lari, A.R. Multi-drug resistant Pseudomonas aeruginosa and Klebsiella pneumoniae circulation in a burn hospital, Tehran, Iran. GMS Hyg. Infect. Control 2019, 14, Doc01. [Google Scholar] [PubMed]
- Riquelme, S.A.; Ahn, D.; Prince, A. Pseudomonas aeruginosa and Klebsiella pneumoniae Adaptation to Innate Immune Clearance Mechanisms in the Lung. J. Innate Immun. 2018, 10, 442–454. [Google Scholar] [CrossRef]
- Bengoechea, J.A.; Sa Pessoa, J. Klebsiella pneumoniae infection biology: Living to counteract host defences. FEMS Microbiol. Rev. 2019, 43, 123–144. [Google Scholar] [CrossRef] [Green Version]
- Alves, D.R.; Gaudion, A.; Bean, J.E.; Esteban, P.P.; Arnot, T.C.; Harper, D.R.; Jenkins, A.T. Combined use of bacteriophage K and a novel bacteriophage to reduce Staphylococcus aureus biofilm formation. Appl. Environ. Microbiol. 2014, 80, 6694–6703. [Google Scholar] [CrossRef] [Green Version]
- Alvi, I.A.; Asif, M.; Tabassum, R.; Aslam, R.; Abbas, Z.; Rehman, S.U. RLP, a bacteriophage of the family Podoviridae, rescues mice from bacteremia caused by multi-drug-resistant Pseudomonas aeruginosa. Arch. Virol. 2020, 165, 1289–1297. [Google Scholar] [CrossRef]
- Anand, T.; Virmani, N.; Kumar, S.; Mohanty, A.K.; Pavulraj, S.; Bera, B.C.; Tripathi, B.N. Phage therapy for treatment of virulent Klebsiella pneumoniae infection in a mouse model. J. Glob. Antimicrob. Resist. 2020, 21, 34–41. [Google Scholar] [CrossRef]
- Cao, F.; Wang, X.; Wang, L.; Li, Z.; Che, J.; Wang, L.; Xu, Y. Evaluation of the efficacy of a bacteriophage in the treatment of pneumonia induced by multi-drug resistance Klebsiella pneumoniae in mice. Biomed. Res. Int. 2015, 2015, 752930. [Google Scholar] [CrossRef] [Green Version]
- Cheng, M.; Liang, J.; Zhang, Y.; Hu, L.; Gong, P.; Cai, R.; Gu, J. The Bacteriophage EF-P29 Efficiently Protects against Lethal Vancomycin-Resistant Enterococcus faecalis and Alleviates Gut Microbiota Imbalance in a Murine Bacteremia Model. Front. Microbiol. 2017, 8, 837. [Google Scholar] [CrossRef]
- Chopra, S.; Harjai, K.; Chhibber, S. Potential of combination therapy of endolysin MR-10 and minocycline in treating MRSA induced systemic and localized burn wound infections in mice. Int. J. Med. Microbiol. 2016, 306, 707–716. [Google Scholar] [CrossRef] [PubMed]
- D’Andrea, M.M.; Frezza, D.; Romano, E.; Marmo, P.; De Angelis, L.H.; Perini, N.; Di Lallo, G. The lytic bacteriophage vB_EfaH_EF1TV, a new member of the Herelleviridae family, disrupts biofilm produced by Enterococcus faecalis clinical strains. J. Glob. Antimicrob. Resist. 2020, 21, 68–75. [Google Scholar]
- De Melo, A.C.C.; da Mata Gomes, A.; Melo, F.L.; Ardisson-Araujo, D.M.P.; de Vargas, A.P.C.; Ely, V.L.; Wolff, J.L.C. Characterization of a bacteriophage with broad host range against strains of Pseudomonas aeruginosa isolated from domestic animals. BMC Microbiol. 2019, 19, 134. [Google Scholar] [CrossRef] [PubMed]
- Debarbieux, L.; Leduc, D.; Maura, D.; Morello, E.; Criscuolo, A.; Grossi, O.; Touqui, L. Bacteriophages can treat and prevent Pseudomonas aeruginosa lung infections. J. Infect. Dis. 2010, 201, 1096–1104. [Google Scholar] [CrossRef] [Green Version]
- Fu, W.; Forster, T.; Mayer, O.; Curtin, J.J.; Lehman, S.M.; Donlan, R.M. Bacteriophage cocktail for the prevention of biofilm formation by Pseudomonas aeruginosa on catheters in an in vitro model system. Antimicrob. Agents Chemother. 2010, 54, 397–404. [Google Scholar] [CrossRef] [Green Version]
- Golkar, Z.; Bagasra, O.; Jamil, N. Experimental Phage Therapy on Multiple Drug Resistant Pseudomonas aeruginosa Infection in Mice. Antivir. Antiretrovir. 2013, 10, S10-005. [Google Scholar] [CrossRef] [Green Version]
- Henry, M.; Lavigne, R.; Debarbieux, L. Predicting in vivo efficacy of therapeutic bacteriophages used to treat pulmonary infections. Antimicrob. Agents Chemother. 2013, 57, 5961–5968. [Google Scholar] [CrossRef] [Green Version]
- Horváth, M.; Kovács, T.; Koderivalappil, S. Identification of a newly isolated lytic bacteriophage against K24 capsular type, carbapenem resistant Klebsiella pneumoniae isolates. Sci. Rep. 2020, 10, 5891. [Google Scholar]
- Hung, C.H.; Kuo, C.F.; Wang, C.H.; Wu, C.M.; Tsao, N. Experimental phage therapy in treating Klebsiella pneumoniae-mediated liver abscesses and bacteremia in mice. Antimicrob. Agents Chemother. 2011, 55, 1358–1365. [Google Scholar] [CrossRef] [Green Version]
- Jeon, J.; Yong, D. Two Novel Bacteriophages Improve Survival in Galleria mellonella Infection and Mouse Acute Pneumonia Models Infected with Extensively Drug-Resistant Pseudomonas aeruginosa. Appl. Environ. Microbiol. 2019, 85, e02900-18. [Google Scholar] [CrossRef] [Green Version]
- Ji, Y.; Cheng, M.; Zhai, S.; Xi, H.; Cai, R.; Wang, Z.; Gu, J. Preventive effect of the phage VB-SavM-JYL01 on rabbit necrotizing pneumonia caused by Staphylococcus aureus. Vet. Microbiol. 2019, 229, 72–80. [Google Scholar] [CrossRef] [PubMed]
- Kaabi, S.A.G.; Musafer, H.K. An experimental mouse model for phage therapy of bacterial pathogens causing bacteremia. Microb. Pathog. 2019, 137, 103770. [Google Scholar] [CrossRef] [PubMed]
- Khalifa, L.; Brosh, Y.; Gelman, D.; Coppenhagen-Glazer, S.; Beyth, S.; Poradosu-Cohen, R.; Hazan, R. Targeting Enterococcus faecalis biofilms with phage therapy. Appl. Environ. Microbiol. 2015, 81, 2696–2705. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kifelew, L.G.; Warner, M.S.; Morales, S.; Thomas, N.; Gordon, D.L.; Mitchell, J.G.; Speck, P.G. Efficacy of Lytic Phage Cocktails on Staphylococcus aureus and Pseudomonas aeruginosa in Mixed-Species Planktonic Cultures and Biofilms. Viruses 2020, 12, 559. [Google Scholar] [CrossRef] [PubMed]
- Kolenda, C.; Josse, J.; Medina, M.; Fevre, C.; Lustig, S.; Ferry, T.; Laurent, F. Evaluation of the Activity of a Combination of Three Bacteriophages Alone or in Association with Antibiotics on Staphylococcus aureus Embedded in Biofilm or Internalized in Osteoblasts. Antimicrob. Agents Chemother. 2020, 64, e02231-19. [Google Scholar] [CrossRef] [PubMed]
- Li, G.; Shen, M.; Yang, Y.; Le, S.; Li, M.; Wang, J.; Lu, S. Adaptation of Pseudomonas aeruginosa to Phage PaP1 Predation via O-Antigen Polymerase Mutation. Front. Microbiol. 2018, 9, 1170. [Google Scholar] [CrossRef] [Green Version]
- Morris, J.L.; Letson, H.L.; Elliott, L.; Grant, A.L.; Wilkinson, M.; Hazratwala, K.; McEwen, P. Evaluation of bacteriophage as an adjunct therapy for treatment of peri-prosthetic joint infection caused by Staphylococcus aureus. PLoS ONE 2019, 14, e0226574. [Google Scholar] [CrossRef] [Green Version]
- Melo, L.D.R.; Ferreira, R.; Costa, A.R. Efficacy and safety assessment of two enterococci phages in an in vitro biofilm wound model. Sci. Rep. 2019, 9, 6643. [Google Scholar] [CrossRef] [Green Version]
- Prazak, J.; Iten, M.; Cameron, D.R.; Save, J.; Grandgirard, D.; Resch, G.; Haenggi, M. Bacteriophages Improve Outcomes in Experimental Staphylococcus aureus Ventilator-associated Pneumonia. Am. J. Respir. Crit. Care Med. 2019, 200, 1126–1133. [Google Scholar] [CrossRef]
- Pallavali, R.R.; Degati, V.L.; Lomada, D.; Reddy, M.C.; Durbaka, V.R.P. Isolation and in vitro evaluation of bacteriophages against MDR-bacterial isolates from septic wound infections. PLoS ONE 2017, 12, e0179245. [Google Scholar] [CrossRef] [Green Version]
- Sunagar, R.; Patil, S.A.; Chandrakanth, R.K. Bacteriophage therapy for Staphylococcus aureus bacteremia in streptozotocin-induced diabetic mice. Res. Microbiol. 2010, 161, 854–860. [Google Scholar] [CrossRef] [PubMed]
- Tinoco, J.M.; Liss, N.; Zhang, H.; Nissan, R.; Gordon, W.; Tinoco, E.; Stevens, R. Antibacterial effect of genetically-engineered bacteriophage varphiEf11/varphiFL1C(Delta36)P(nisA) on dentin infected with antibiotic-resistant Enterococcus faecalis. Arch. Oral. Biol. 2017, 82, 166–170. [Google Scholar] [CrossRef] [PubMed]
- Yilmaz, C.; Colak, M.; Yilmaz, B.C.; Ersoz, G.; Kutateladze, M.; Gozlugol, M. Bacteriophage therapy in implant-related infections: An experimental study. J. Bone Jt. Surg. Am. 2013, 95, 117–125. [Google Scholar] [CrossRef] [PubMed]
- Zhang, W.; Mi, Z.; Yin, X.; Fan, H.; An, X.; Zhang, Z.; Tong, Y. Characterization of Enterococcus faecalis phage IME-EF1 and its endolysin. PLoS ONE 2013, 8, e8043. [Google Scholar] [CrossRef]
- Cross, T.; Schoff, C.; Chudoff, D.; Graves, L.; Broomell, H.; Terry, K.; Dunbar, D. An optimized enrichment technique for the isolation of Arthrobacter bacteriophage species from soil sample isolates. J. Vis. Exp. 2015, 98, 52781. [Google Scholar] [CrossRef] [Green Version]
- Batinovic, S.; Wassef, F.; Knowler, S.A.; Rice, D.T.F.; Stanton, C.R.; Rose, J.; Franks, A.E. Bacteriophages in Natural and Artificial Environments. Pathogens 2019, 8, 100. [Google Scholar] [CrossRef] [Green Version]
- Furfaro, L.L.; Payne, M.S.; Chang, B.J. Bacteriophage Therapy: Clinical Trials and Regulatory Hurdles. Front. Cell. Infect. Microbiol. 2018, 8, 376. [Google Scholar] [CrossRef] [Green Version]
- Worthington, R.J.; Melander, C. Combination approaches to combat multidrug-resistant bacteria. Trends Biotechnol. 2013, 31, 177–184. [Google Scholar] [CrossRef] [Green Version]
- Altamirano, F.L.G.; Barr, J.J. Phage Therapy in the Postantibiotic Era. Clin. Microbiol. Rev. 2019, 32, e00066-18. [Google Scholar]
- Prasanth, M.; Ashok, T.; Sebastian, L.; Ramesh, N. Pharmacological and Immunological Aspects of Phage Therapy. Infect. Microbes Dis. 2019, 1, 34–42. [Google Scholar]
- Geier, M.R.; Trigg, M.E.; Merril, C.R. Fate of bacteriophage lambda in non-immune germ-free mice. Nature 1973, 246, 221–223. [Google Scholar] [CrossRef] [PubMed]
- Lusiak-Szelachowska, M.; Zaczek, M.; Weber-Dabrowska, B.; Miedzybrodzki, R.; Klak, M.; Fortuna, W.; Gorski, A. Phage neutralization by sera of patients receiving phage therapy. Viral Immunol. 2014, 27, 295–304. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Singla, S.; Harjai, K.; Raza, K.; Wadhwa, S.; Katare, O.P.; Chhibber, S. Phospholipid vesicles encapsulated bacteriophage: A novel approach to enhance phage biodistribution. J. Virol. Methods 2016, 236, 68–76. [Google Scholar] [CrossRef] [PubMed]
- Al-Wrafy, F.; Brzozowska, E.; Gorska, S.; Drab, M.; Strus, M.; Gamian, A. Identification and characterization of phage protein and its activity against two strains of multidrug-resistant Pseudomonas aeruginosa. Sci. Rep. 2019, 9, 13487. [Google Scholar] [CrossRef] [Green Version]
- Nordstrom, K.; Forsgren, A. Effect of protein A on adsorption of bacteriophages to Staphylococcus aureus. J. Virol. 1974, 14, 198–202. [Google Scholar] [CrossRef] [Green Version]
- Koc, C.; Xia, G.; Kuhner, P.; Spinelli, S.; Roussel, A.; Cambillau, C.; Stehle, T. Structure of the host-recognition device of Staphylococcus aureus phage varphi11. Sci. Rep. 2016, 6, 27581. [Google Scholar] [CrossRef]
- Tan, D.; Zhang, Y.; Qin, J.; Le, S.; Gu, J.; Chen, L.K.; Zhu, T. A Frameshift Mutation in wcaJ Associated with Phage Resistance in Klebsiella pneumoniae. Microorganisms 2020, 8, 378. [Google Scholar] [CrossRef] [Green Version]
- Al-Zubidi, M.; Widziolek, M.; Court, E.K.; Gains, A.F.; Smith, R.E.; Ansbro, K.; Stafford, G.P. Identification of Novel Bacteriophages with Therapeutic Potential That Target Enterococcus faecalis. Infect. Immun. 2019, 87, e00512-19. [Google Scholar] [CrossRef] [Green Version]
- Jault, P.; Leclerc, T.; Jennes, S.; Pirnay, J.P.; Que, Y.A.; Resch, G.; Gabard, J. Efficacy and tolerability of a cocktail of bacteriophages to treat burn wounds infected by Pseudomonas aeruginosa (PhagoBurn): A randomised, controlled, double-blind phase 1/2 trial. Lancet Infect. Dis. 2019, 19, 35–45. [Google Scholar] [CrossRef]
- Fabijan, A.P.; Team, W.B.T.; Lin, R.C.; Ho, J.; Maddocks, S.; Ben Zakour, N.L.; Iredell, J. Safety of bacteriophage therapy in severe Staphylococcus aureus infection. Nat. Microbiol. 2020, 5, 465–472. [Google Scholar] [CrossRef]
- Schooley, R.T.; Biswas, B.; Gill, J.J.; Hernandez-Morales, A.; Lancaster, J.; Lessor, L.; Hamilton, T. Development and Use of Personalized Bacteriophage-Based Therapeutic Cocktails to Treat a Patient with a Disseminated Resistant Acinetobacter baumannii Infection. Antimicrob. Agents Chemother. 2017, 61, e00954-17. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- El Haddad, L.; Harb, C.P.; Gebara, M.A.; Stibich, M.A.; Chemaly, R.F. A Systematic and Critical Review of Bacteriophage Therapy Against Multidrug-resistant ESKAPE Organisms in Humans. Clin. Infect. Dis. 2019, 69, 167–178. [Google Scholar] [CrossRef] [PubMed]
- McCallin, S.; Sarker, S.A.; Barretto, C.; Sultana, S.; Berger, B.; Huq, S.; Krause, L.; Bibiloni, R.; Schmitt, B.; Reuteler, G.; et al. Safety analysis of a Russian phage cocktail: From MetaGenomic analysis to oral applicationin healthy human subjects. Virology 2013, 443, 187–196. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Standard Treatment Associated with Phage Therapy Versus Placebo for Diabetic Foot Ulcers Infected by S. aureus (PhagoPied). Available online: https://clinicaltrials.gov/ct2/show/NCT02664740 (accessed on 19 November 2020).
- Bacteriophage Therapy in Patients with Urinary Tract Infections. Available online: https://clinicaltrials.gov/ct2/show/NCT04287478 (accessed on 26 October 2020).
- Phage Therapy for the Prevention and Treatment of Wound Infections in Burned Patients. Available online: https://clinicaltrials.gov/ct2/show/NCT04323475 (accessed on 26 October 2020).
- Antibacterial Treatment against Diarrhea in Oral Rehydration Solution. Available online: https://clinicaltrials.gov/ct2/show/NCT00937274 (accessed on 26 October 2020).
- Bacteriophages for Treating Urinary Tract Infections in Patients Undergoing Transurethral Resection of the Prostate. Available online: https://www.clinicaltrials.gov/ct2/show/NCT03140085 (accessed on 19 November 2020).
- Sutton, T.D.S.; Hill, C. Gut Bacteriophage: Current Understanding and Challenges. Front. Endocrinol. (Lausanne) 2019, 10, 784. [Google Scholar] [CrossRef]
- Hibbing, M.E.; Fuqua, C.; Parsek, M.R.; Peterson, S.B. Bacterial competition: Surviving and thriving in the microbial jungle. Nat. Rev. Microbiol. 2010, 8, 15–25. [Google Scholar] [CrossRef] [Green Version]
- Hsu, B.B.; Gibson, T.E.; Yeliseyev, V.; Liu, Q.; Lyon, L.; Bry, L.; Gerber, G.K. Dynamic Modulation of the Gut Microbiota and Metabolome by Bacteriophages in a Mouse Model. Cell Host Microbe 2019, 25, 803–814.e5. [Google Scholar] [CrossRef] [Green Version]
- Galtier, M.; De Sordi, L.; Maura, D.; Arachchi, H.; Volant, S.; Dillies, M.A.; Debarbieux, L. Bacteriophages to reduce gut carriage of antibiotic resistant uropathogens with low impact on microbiota composition. Environ. Microbiol. 2016, 18, 2237–2245. [Google Scholar] [CrossRef] [Green Version]



{kind=link}
{kind=link}
| Serial Number | Target Bacteria | Model Type/Age/ Gender | Phage/Cocktail Identification | Site/Type of Infection | Method of Inoculation | Follow Up Period | Therapy Dose | Method of Testing | Immune Markers | Outcome | Combination Therapy | Emergence of Resistance | Ref. |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | S. aureus (Methicillin resistant) | Plates | Phage K and DRA88 (Myoviridae family) from sewage alone and in a cocktail | Biofilm | Addition to plate | 1–48 h | 106–107 PFU/mL | Electron microscopy Genomic analysis Biofilm assays | Not assessed | Phage cocktail was able to disrupt biofilm | Not assessed | Not assessed | [16] |
| 2 | P. aeruginosa | Specific-pathogen-free (SPF) female mice, 6–8 weeks old | RLP phage from water body (Podoviridae family) | Bacteraemia | Intraperitoneal | 21 days | 1 × 109 PFU | Electron microscopy Genomic analysis Survival tests | Not assessed | Mice were rescued from bacteraemia (92% survival rate) | Not assessed | Not assessed | [17] |
| 3 | K. pneumoniae | BALB/c mice 6–8 weeks old | VTCCBPA43 from water body (Siphoviridae family) | Pneumonia | Intranasal | 10 days | 2 × 109 PFU | Nano-scale liquid chromatography–tandem mass spectrometry Electron microscopy Animal studies and histopathology | Not assessed | Significant reduction of bacterial load in lungs | Not assessed | Not assessed | [18] |
| 4 | K. pneumoniae | Webster female mice 7 weeks old | Phage 1513 (Siphoviridae family) | Pneumonia | Intranasal | 72 h | 2 × 109 PFU/mouse | Electron microscopy Histopathology ELISA | Lower TNF-α Lower IL-6 | Phage improved lung lesions and 80% survival rate | Not assessed | Not assessed | [19] |
| 5 | Vancomycin-resistant E. faecalis | BALB/c female mice 6–8 weeks old | EF-P29 phage from sewage (Siphoviridae family) | Bacteraemia | Intraperitoneal | 2 days | 4 × 105 PFU | Electron microscopy Genomic analysis Survival tests | Not assessed | Protection of all mice from bacteraemia (100% survival) | Not assessed | Not assessed | [20] |
| 6 | S. aureus (Methicillin resistant) | BALB/c female mice 4–6 weeks old | Endolysin from MR-10 phage | Systemic burn wound infection | Subcutaneously near the site of burn wound | 7 days | 50 ug/mL | Histopathology Survival tests | Not assessed | Combination therapy of endolysin plus antibiotic found to be effective against systemic infection (100% survival) | Minocycline | Not assessed | [21] |
| 7 | E. faecalis (multiple strains) | Plates | EF1TV phage from sewage (Herelleviridae family) | Biofilm | Addition to plate | 5 days | 109PFU | Electron microscopy Confocal microscopy Biofilm degradation | Not assessed | Exhibits anti-biofilm activity (9–68% reduction in different E. faecalis strains) | Not assessed | Yes | [22] |
| 8 | P. aeruginosa | Plates | BrSPI phage from sewage (Caudovirales family) | Culture | Addition to culture | 24 h | 106PFU/mL | Electron microscopy Genomic analysis Biological in vitro assays | Not assessed | Effective for controlling bacterial growth until 12 h post-infection | Not assessed | Yes | [23] |
| 9 | P. aeruginosa | Balb/c male mice 8 week old | PAK-P1 phage from sewage (Myoviridae family) | Pneumonia | Intranasal | 12 days | 108 PFU | Electron microscopy Inflammation analysis Genomic analysis Survival tests Luminescence assay | Lower TNF-α Lower IL-6 | Protection from lethal pneumonia (100% survival) | Not assessed | Not assessed | [24] |
| 10 | P. aeruginosa | Hydrogel-coated catheters. | Cocktail consisting of phages from sewage combined with phage M4 | Biofilm | Exposing the catheter lumen to phage lysate | 2 days | 7.0 × 109 PFU/mL | Biofilm degradation assay Electron microscopy | Not assessed | Phage cocktail pre-treatment significantly controls biofilm formation | Not assessed | Yes | [25] |
| 11 | P. aeruginosa (multidrug resistant) | BALB/c male mice 7 weeks old | Lytic phage PS5 from clinical specimen (Myoviridea family) | Acute and chronic wound infection model | Intraperitoneal and orally | 7 days | 9 × 108 PFU, administered 30 min after bacterial challenge and 24 h after the first injection, and then given a daily dose of phage orally (3 × 108) | Electron microscopy PCR Survival tests | Not assessed | Resolution of infection in acute wound model and complete recovery of the infected rodents in chronic wound infection model. | Not assessed | Not assessed | [26] |
| 12 | P. aeruginosa | BALB/c male mice 8 weeks old | Multiple bacteriophages from sewage tested individually (Myoviridea and Podoviridae family) | Pneumonia | Intranasal | 13 days | 106 PFU | Survival tests Genomic analysis Luminescence assay | Not assessed | 37–100% survival rate with seven of the nine tested phages at the indicated dosage in P. aeruginosa PAK-lumi strain. Two strains did not show sufficient activity. | Not assessed | Not assessed | [27] |
| 13 | K. pneumoniae (Carbapenem resistant) | Plates and BALB/c female mice 6–7 weeks old | vB_KpnS_Kp13 from sewage (Siphoviridae family) | Biofilm and in vivo infection model | For biofilm degradation assay, phages were added to the plates Intraperitoneal injection for mice | 2 days (biofilm) 10 days (in vivo) | 2 × 108 PFU/mL 1.75 × 108 PFU/mice | Electron microscopy Confocal microscopy Genomic analysis Biofilm degradation Survival assay | Not assessed | Phage was able to degrade 70% of biofilm Phage administration within 10 min of bacterial challenge resulted in 100% survival | Not assessed | Not assessed | [28] |
| 14 | K. pneumoniae | C57BL/6 male mice 6–7 weeks old | NK5 from sewage (Podoviridae family) | Liver abscess model and bacteraemia | Intraperitoneal (IP) Intragastric (IG) | 9 days | 2 × 107 PFU/mL (IP) 2 × 106 PFU/mL (IG) | Survival assay Inhibition assays | Lower TNF-α, MCP-1, IL-10 and IL-6 | Phage treatment 30 min after bacterial challenge protected mice from death (100% survival), no detectable bacteria in blood | Not assessed | Yes | [29] |
| 15 | P. aeruginosa (Extensively drug-resistant) | Female C57BL/6 mice 7–8 weeks old | B-R656 and B-R1836 (Siphoviridae family) from sewage tested individually | Pneumonia | Intraperitoneal | 12 days | 109 PFU/mL | Electron microscopy Histopathology Cytokines assay Survival assay | Lower TNF-α IL-6 | Both phages decreased bacterial load in lungs, increased survival rate (66% and 83% respectively) | Not assessed | Not assessed | [30] |
| 16 | S. aureus | Female rabbit | VB-SavM-JYlOI phage from sewage (Myoviridae family) | Rabbit necrotizing pneumonia model | Intranasal | 8 days | 3 × 109 PFU | Electron microscopy Histopathology Cytokines assay Genomic analysis Survival assay | Lower IFN-γ, TNF-α, IL-1α and IL-8 | Single dose of phage protected rabbit from pneumonia (survival rate 90% at 48 h) | Not assessed | Not assessed | [31] |
| 17 | K. pneumoniae and P. aeruginosa | Albino mice 1 month old | monovalent and polyvalent phage preparation | Bacteraemia | Intraperitoneal | 20 days | K. pneumoniae: 108 PFU P. aeruginosa:109 PFU | Dose ranging assay Delayed treatment Survival assays | Not assessed | Phage cocktails were effective in rescuing mice from death in 100% of mice in case of both monomicrobial and polymicrobial bacteremic mice | Not assessed | Not assessed | [32] |
| 18 | E. faecalis | Plates | EFDG1 from sewage (Myoviridae family) | Biofilm and ex vivo two chamber bacterial leakage model of human teeth | Addition to plate (biofilm) Teeth were irrigated with phages | 7 days (biofilms) 48 h (tooth model) | 1 × 107 PFU (biofilm) 1 × 108 PFU/mL (tooth irrigation) | Electron microscopy Confocal microscopy Biofilm degradation Viability assays | Not assessed | * Effective lytic activities against biofilm: 5-fold reduction in biomass and 5 log reduction in viable counts * protects root canals from infection: 7-log reduction in viable counts | Not assessed | Not assessed | [33] |
| 19 | S. aureus and P. aeruginosa mixed infection | Plates | Phage cocktails AB-SA01 consisting of staphylococcal phages designated J-Sa-36, Sa-83, and Sa-87 (Myoviridae family) and AB-PA01 consisting of Pa-193 and Pa-204 from Myoviridae family and Pa-222 and Pa-223 from Podoviridae family. | Biofilm | Addition to plate | 24 h | Not specified | Confocal microscopy Biofilm assay | Not assessed | * Individual phage cocktails and combination of the two phage cocktails produced significant biofilm biomass reduction in mixed species * Tetracycline was more effective than the phage therapy in reducing biofilm biomass. | Comparison of phage activity against Tetracycline | Not assessed | [34] |
| 20 | S. aureus (methicillin susceptible) | Plates | Cocktail of three phages: PP1493, PP1815, and PP1957 from sewage | Biofilm and in vitro model of osteoblast infection | Addition to plate | 24 h | 108 PFU | Biofilm assay | Not assessed | Cocktail active against mature biofilm with 3.6 log reduction in viable bacteria count -Synergistic effect between antibiotics and bacteriophages at lowed doses was observed -bacteriophages had no intracellular activity | Vancomycin/Rifampicin | Not assessed | [35] |
| 21 | P. aeruginosa | Liquid culture | PaPI phage | Liquid culture | Addition to culture | Not specified | 1010 PFU/mL | Biofilm assays Confocal microscopy Genomic analysis | Not assessed | Lysed cells | Not assessed | Yes | [36] |
| 22 | S. aureus (methicillin susceptible) | Sprague-Dawley male rats 20 weeks old | StaPhage cocktail consisting of 5 Myoviridae family phages: StaPh_1, StaPh_3, StaPh_4, StaPh_11 and StaPh_16 | Peri-prosthetic joint infection model | Intraperitoneal | 7 days | Three doses of 1.3 × 108 PFU; 8.9 × 105–1.9 × 106 and >104 PFU respectively | Bacterial load assay Cytokines assay | No significant difference in levels of TNF-𝛼, IFN-γ, MCP-1, IL-1ß, IL-12p70, IL-10, IL-6 and IL-4 between phage treatment and control groups in the joint tissue, MCP-1 was significantly lower in the phage plus vancomycin treatment group compared to controls | Phage cocktail treatment led to 5-fold reduction and combination treatment of phage with vancomycin led to 22.5-fold reduction in bacterial load in joint tissue compared to controls | Vancomycin | Yes | [37] |
| 23 | E. faecalis and E. faecium | Plates (biofilms) and 96 well plates (colonization assay) | Phage cocktail of vB_EfaS-Zip (Zip) (Siphovirus family) infecting E. faecium and vB_EfaP-Max (Max) (Podovirus family) infecting E. faecalis from sewage | Mixed infection collagen wound in vitro biofilm model and 3T3 cell colonization assay | Addition to plate | 1 day | 1 × 108 PFU of cocktail (biofilm) 1 × 107 PFU/mL of individual phages (colonization) | Electron microscopy Biofilm assays Cytotoxicity assays Mammalian cell infection assays | Not assessed | Dual species biofilms: phage cocktail led to reduction of cell concentration by 2.5 log CFU/mL 3T3 colonization assay: both phages individually in respective bacterial infections reduced viable bacterial cells by approx. 3 log CFU/mL in 6 h | Not assessed | Not assessed | [38] |
| 24 | S. aureus Methicillin resistant | Wistar male rats, 9–10 weeks old | Phage cocktail consisting of equal titers of phages 2003, 2002, 3A, and K | Ventilator associated pneumonia | Intravenous | 4 days | 2–3 × 109 PFU/mL; 5 doses | Survival assay Histopathology Cytokines assay | Reduced TNF-α IL-6 Levels | Significant improvement in survival rates (58%) compared to absolute mortality in controls, with reduced bacterial load and better histopathological outcomes | Teicoplanin: combination therapy of both phage and antibiotic did not improve results than single agent therapy alone | Not assessed | [39] |
| 25 | Multi drug resistant strains of P. aeruginosa, S. aureus and K. pneumoniae | ln vitro in flasks | K. pneumoniae phage: KP DP1 P. aeruginosa phage: PA DP4 S. aureus phage: SA DP1, all isolated from sewage | Liquid culture | Addition to flask | 1 day | 109 PFU/mL | Bacterial reduction assay in liquid medium | Not assessed | Phages applied on respective bacteria reduced bacterial load but bacteria could regrow after 14–16 h of phage therapy | Not assessed | Yes | [40] |
| 26 | S. aureus (methicillin sensitive) | BALB/c female mice six weeks old diabetic and non-diabetic mice | GRCS phage from raw sewage (Myoviridae family) | Bacteraemia | Intraperitoneal | 30 days | 2 × 109 PFU | Electron microscopy Survival tests | Not assessed | Protection from lethal bacteraemia (survival rate 90% in case of diabetic and 100% in case of non-diabetic bacteremic animals versus 0% for controls) | Oxacillin: phage therapy showed improved outcome compared to Oxacillin | Not assessed | [41] |
| 27 | E. faecalis vancomycin-sensitive and resistant strains | Two-chamber device containing human dentin segments | Genetically engineered phage, ϕEf11/ϕFL1C(Δ36)PnisA | In vitro infected-dentin models | Addition to root canals | 7 days | 5.8 × 109 PFU | Recovery and Inhibition assays | Not assessed | Titre of bacteria reduced by 18% in case of vancomycin sensitive strain and by 99% in case of vancomycin resistant infections | Not assessed | Not assessed | [42] |
| 28 | S. aureus (methicillin resistant); Pseudomonas aeruginosa (carbapenem sensitive) | Adult Sprague-Dawley albino male rats | Sb-1 phage for S. aureus and PAT14 phage for Pseudomonas aeruginosa | Biofilm (implant-related osteomyelitis model) | Injected through the skin | 15 days | 107 PFU | Biofilm assays Bactericidal test ELISA | Lower C-reactive protein | S. aureus: only bacteriophage plus antibiotic therapy significantly reduced bacterial load and prevented biofilm formation Pseudomonas aeruginosa: both bacteriophage, and bacteriophage plus antibiotic combination reduced bacterial load but did not impact biofilm | Teicoplanin for S. aureus and imipenem, cilastatin and amikacin for Pseudomonas aeruginosa | Not assessed | [43] |
| 29 | E. faecalis | BALB/c female mice 6–8 weeks old | IME-EF1 phage from sewage (Siphoviridae family) and purified endolysin | Sepsis | Intraperitoneal | 4 days | 2 × 1010 PFU/mL/0.2 mg of expressed endolysin | Electron microscopy Survival tests Lytic binding assay | Not assessed | Both phage and the endolysin reduced bacterial load and protected mice from lethal challenges (survival rate of 60–80%) | Not assessed | Not assessed | [44] |
| Serial Number | Trial Title | Medical Condition | Method of Intervention | Status | Country | References |
|---|---|---|---|---|---|---|
| 1 | Standard treatment Associated with Phage Therapy Versus Placebo for Diabetic Foot Ulcers Infected by S. aureus (PhagoPied) | Diabetic foot | Topical anti-Staphylococcus bacteriophage therapy | Not yet recruiting | France | [63,64] |
| 2 | Bacteriophage Therapy in Patients with Urinary Tract Infections (E. coli and K. pneumoniae) | Urinary tract infection | Biological: Bacteriophage Therapy (intravenous/intravesical route) | Not yet recruiting | United States of America | [65] |
| 3 | Phage Therapy for the Prevention and Treatment of Wound Infections in Burned Patients (S. aureus, P. aeruginosa, or K. pneumoniae) | Wound infection | Bacteriophage cocktail spray over burned area | Not yet recruiting | Australia | [66] |
| 4 | Antibacterial Treatment Against Diarrhea in Oral Rehydration Solution (E. coli) | Diarrhea | T4 phage cocktail-oral | Terminated | Bangladesh | [67] |
| 5 | Bacteriophages for Treating Urinary Tract Infections in Patients Undergoing Transurethral Resection of the Prostate | Urinary Tract Infections | PYO Phage (intravesical) installation) | Completed | Georgia | [68] |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
AL-Ishaq, R.K.; Skariah, S.; Büsselberg, D. Bacteriophage Treatment: Critical Evaluation of Its Application on World Health Organization Priority Pathogens. Viruses 2021, 13, 51. https://doi.org/10.3390/v13010051
AL-Ishaq RK, Skariah S, Büsselberg D. Bacteriophage Treatment: Critical Evaluation of Its Application on World Health Organization Priority Pathogens. Viruses. 2021; 13(1):51. https://doi.org/10.3390/v13010051
Chicago/Turabian StyleAL-Ishaq, Raghad Khalid, Sini Skariah, and Dietrich Büsselberg. 2021. "Bacteriophage Treatment: Critical Evaluation of Its Application on World Health Organization Priority Pathogens" Viruses 13, no. 1: 51. https://doi.org/10.3390/v13010051