Understanding Pediatric Norovirus Epidemiology: A Decade of Study among Ghanaian Children

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Sample Collection
2.2. Laboratory Analysis
2.2.1. Nucleic Acid Extraction and Norovirus RNA Amplification
2.2.2. DNA Purification and Nucleotide Sequencing
2.3. Data Analysis
Sequence Analysis and Norovirus Genotyping
2.4. Statistical Analysis
3. Results
3.1. Demographic and Clinical Characteristics of Study Subjects
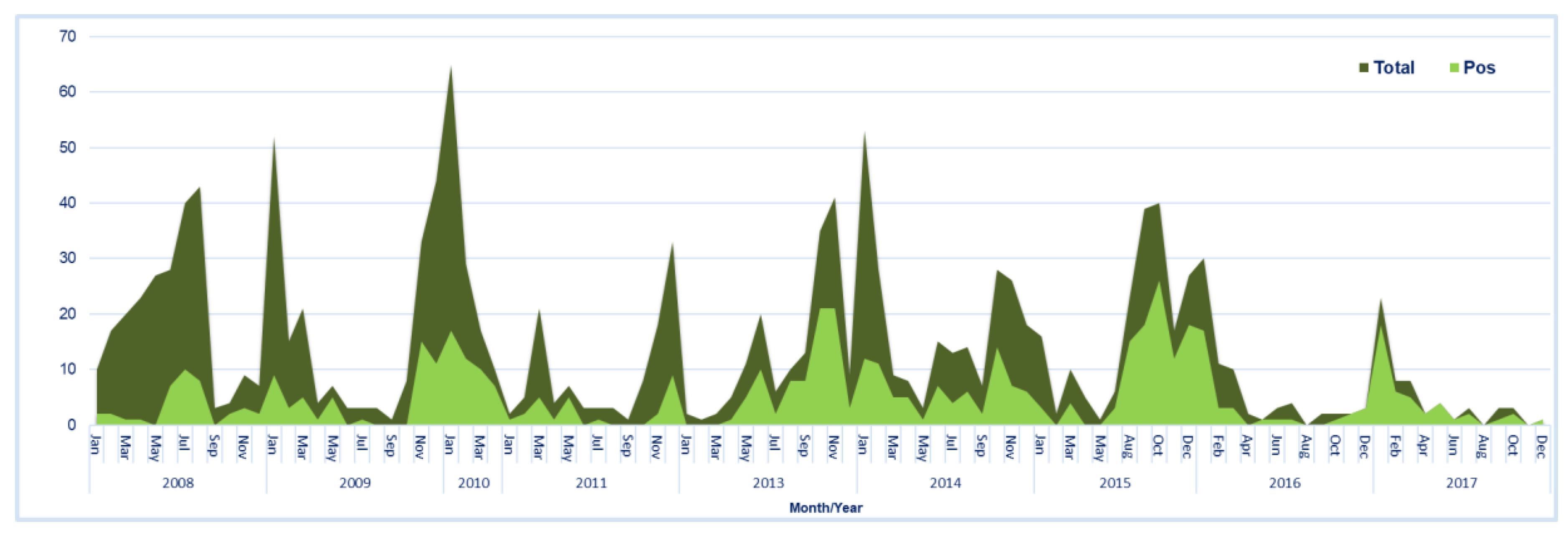
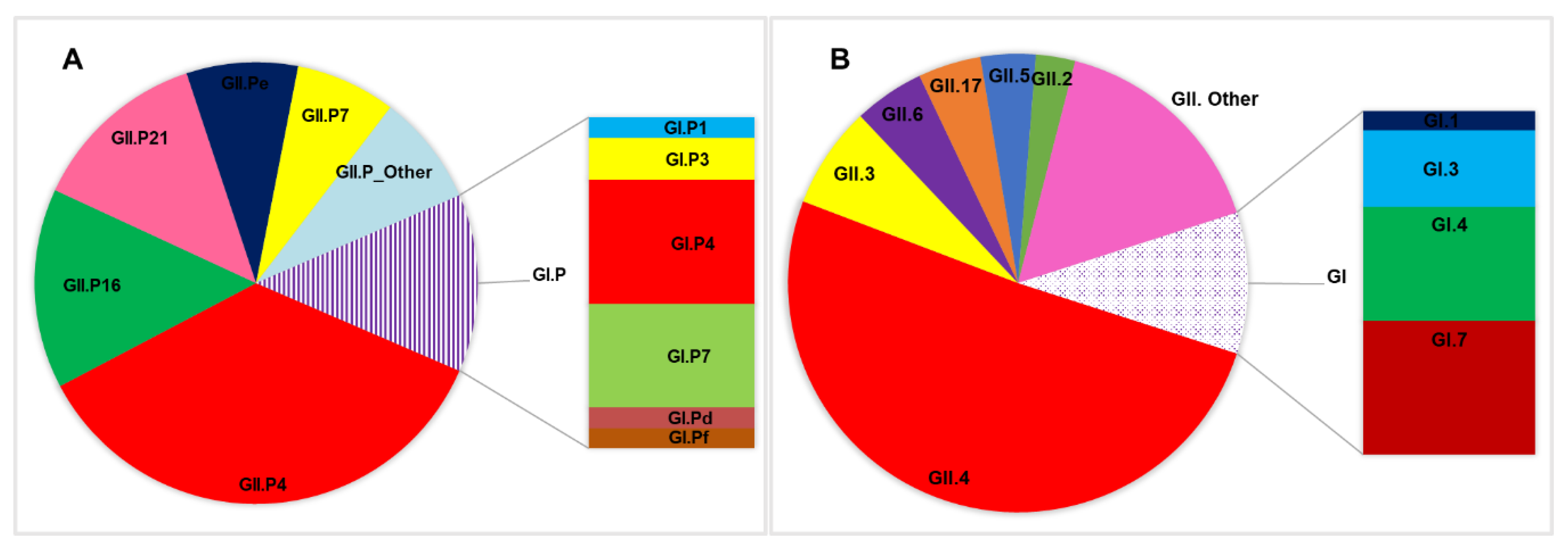
3.2. Norovirus Detection and Epidemiology
3.3. Clinical Characteristics of Norovirus Infection within the Study Population
3.4. Norovirus Genotype and Associated Disease Severity
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Troeger, C.; Blacker, B.; Khalil, I.; Rao, P.; Cao, S.; Zimsen, S.; Albertson, S.B.; Stanaway, J.D.; Deshpande, A.; Abebe, Z.; et al. Estimates of the global, regional, and national morbidity, mortality, and aetiologies of diarrhoea in 195 countries: A systematic analysis for the Global Burden of Disease Study 2016. Lancet Infect. Dis. 2018, 18, 1211–1228. [Google Scholar] [CrossRef] [Green Version]
- World Health Organisation. Children: Reducing Mortality. 2018. Available online: https://www.who.int/news-room/fact-sheets/detail/children-reducing-mortality (accessed on 18 June 2019).
- Mokdad, A. Despite Substantial Global Reduction in Diarrhea Deaths, Half a Million Children still Die from Diseases Each Year. 2017. Available online: http://www.healthdata.org/news-release/despite-substantial-global-reduction-diarrhea-deaths-half-million-children-still-die (accessed on 18 June 2019).
- Rheingans, R.D.; Antil, L.; Dreibelbis, R.; Podewils, L.J.; Bresee, J.S.; Parashar, U.D. Economic Costs of Rotavirus Gastroenteritis and Cost-Effectiveness of Vaccination in Developing Countries. J. Infect. Dis. 2009, 200, S16–S27. [Google Scholar] [CrossRef] [PubMed]
- Aliabadi, N.; Antoni, S.; Mwenda, J.M.; Weldegebriel, G.; Biey, J.N.M.; Cheikh, D.; Fahmy, K.; Teleb, N.; Ashmony, H.A.; Ahmed, H.; et al. Global impact of rotavirus vaccine introduction on rotavirus hospitalisations among children under 5 years of age, 2008 & 2013;16: Findings from the Global Rotavirus Surveillance Network. Lancet Glob. Health 2019, 7, e893–e903. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Burnett, E.; Jonesteller, C.L.; Tate, J.E.; Yen, C.; Parashar, U.D. Global Impact of Rotavirus Vaccination on Childhood Hospitalizations and Mortality from Diarrhea. J. Infect. Dis. 2017, 215, 1666–1672. [Google Scholar] [CrossRef]
- Armah, G.; Pringle, K.; Enweronu-Laryea, C.; Ansong, D.; Mwenda, J.; Diamenu, S.K.; Narh, C.; Lartey, B.; Binka, F.; Grytdal, S.; et al. Impact and Effectiveness of Monovalent Rotavirus Vaccine against Severe Rotavirus Diarrhea in Ghana. Clin. Infect. Dis. 2016, 62, S200–S207. [Google Scholar] [CrossRef] [Green Version]
- Enweronu-Laryea, C.; Armah, G.; Sagoe, K.; Ansong, D.; Addo-Yobo, E.; Diamenu, S.; Mwenda, J.M.; Parashar, U.D.; Tate, J.E. Sustained impact of rotavirus vaccine introduction on rotavirus gastroenteritis hospitalizations in children <5 years of age, Ghana, 2009–2016. Vaccine 2008, 36, 7131–7134. [Google Scholar] [CrossRef]
- Hallowell, B.D.; Parashar, U.D.; Hall, A.J. Epidemiologic challenges in norovirus vaccine development. Hum. Vaccines Immunother. 2019, 15, 1279–1283. [Google Scholar] [CrossRef]
- Chen, H.; Hu, Y. Molecular Diagnostic Methods for Detection and Characterization of Human Noroviruses. Open Microbiol. J. 2016, 10, 78–89. [Google Scholar] [CrossRef] [Green Version]
- Oude Munnink, B.B.; van der Hoek, L. Viruses Causing Gastroenteritis: The Known, The New and Those Beyond. Viruses 2016, 8, 42. [Google Scholar] [CrossRef]
- Stuempfig, N.D.; Seroy, J. Viral Gastroenteritis. In StatPearls; StatPearls Publishing: Treasure Island, FL, USA, 2020. Available online: https://www.ncbi.nlm.nih.gov/books/NBK518995/ (accessed on 20 October 2020).
- Koo, H.L.; Neill, F.H.; Estes, M.K.; Munoz, F.M.; Cameron, A.; DuPont, H.L.; Atmar, R.L. Noroviruses: The Most Common Pediatric Viral Enteric Pathogen at a Large University Hospital After Introduction of Rotavirus Vaccination. J. Pediatric Infect. Dis. Soc. 2013, 2, 57–60. [Google Scholar] [CrossRef] [Green Version]
- Lopman, B.; Grassly, N. Editorial Commentary: Pediatric Norovirus in Developing Countries: A Picture Slowly Comes Into Focus. Clin. Infect. Dis. 2016, 62, 1218–1220. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Centers for Disease Control and Prevention. Norovirus Worldwide. 2018. Available online: https://www.cdc.gov/norovirus/trends-outbreaks/worldwide.html (accessed on 19 June 2019).
- Mans, J. Norovirus Infections and Disease in Lower-Middle and Low-Income Countries, 1997–2018. Viruses 2019, 11, 341. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pires, S.M.; Fischer-Walker, C.L.; Lanata, C.F.; Devleesschauwer, B.; Hall, A.J.; Kirk, M.D.; Duarte, A.S.R.; Black, R.E.; Angulo, F.J. Aetiology-Specific Estimates of the Global and Regional Incidence and Mortality of Diarrhoeal Diseases Commonly Transmitted through Food. PLoS ONE 2015, 10, e0142927. [Google Scholar] [CrossRef] [PubMed]
- Bartsch, S.M.; Lopman, B.A.; Ozawa, S.; Hall, A.J.; Lee, B.Y. Global Economic Burden of Norovirus Gastroenteritis. PLoS ONE 2016, 11, e0151219. [Google Scholar] [CrossRef] [Green Version]
- Ahmed, S.; Hall, A.; Robinson, A.; Verhoef, L.; Premkumar, P.; Parashar, U.D.; Koopmans, M.; Lopman, B.A. Global prevalence of norovirus in cases of gastroenteritis: A systematic review and meta-analysis. Lancet Infect. Dis. 2014, 14, 725–730. [Google Scholar] [CrossRef] [Green Version]
- Lopman, B.A.; Steele, D.; Kirkwood, C.D.; Parashar, U.D. The Vast and Varied Global Burden of Norovirus: Prospects for Prevention and Control. PLoS Med. 2016, 13, e1001999. [Google Scholar] [CrossRef] [PubMed]
- Kreidieh, K.; Charide, R.; Dbaibo, G.; Melhem, N.M. The epidemiology of Norovirus in the Middle East and North Africa (MENA) region: A systematic review. Virol. J. 2017, 14, 220. [Google Scholar] [CrossRef]
- Ettayebi, K.; Crawford, S.E.; Murakami, K.; Broughman, J.R.; Karandikar, U.; Tenge, V.R.; Neill, F.H.; Blutt, S.E.; Zeng, X.-L.; Qu, L.; et al. Replication of human noroviruses in stem cell-derived human enteroids. Science 2016, 353, 1387–1393. [Google Scholar] [CrossRef]
- Jones, M.K.; Watanabe, M.; Zhu, S.; Graves, C.L.; Keyes, L.; Grau, K.R.; Gonzalez-Hernandez, M.B.; Lovine, N.M.; Wobus, C.E.; Vinjé, J.; et al. Enteric bacteria promote human and mouse norovirus infection of B cells. Science 2014, 346, 755–759. [Google Scholar] [CrossRef] [Green Version]
- Leroux-Roels, G.; Cramer, J.P.; Mendelman, P.M.; Sherwood, J.; Clemens, R.; Aerssens, A.; De Coster, I.; Borkowski, A.; Baehner, F.; Van Damme, P. Safety and Immunogenicity of Different Formulations of Norovirus Vaccine Candidate in Healthy Adults: A Randomized, Controlled, Double-Blind Clinical Trial. J. Infect. Dis. 2018, 217, 597–607. [Google Scholar] [CrossRef]
- Cannon, J.L.; Barclay, L.; Collins, N.R.; Wikswo, M.E.; Castro, C.J.; Magana, L.C.; Gregoricus, N.; Marine, R.L.; Chhabra, P.; Vinjé, J. Genetic and Epidemiologic Trends of Norovirus Outbreaks in the United States from 2013 to 2016 Demonstrated Emergence of Novel GII.4 Recombinant Viruses. J. Clin. Microbiol. 2017, 55, 2208–2221. [Google Scholar] [CrossRef] [Green Version]
- Ruuska, T.; Vesikari, T. Rotavirus Disease in Finnish Children: Use of Numerical Scores for Clinical Severity of Diarrhoeal Episodes. Scand. J. Infect. Dis. 1990, 22, 259–267. [Google Scholar] [CrossRef] [PubMed]
- Armah, G.E.; Gallimor, C.I.; Binka, F.N.; Asmah, R.H.; Green, J.; Ugoji, U.; Anto, F.; Brwon, D.W.G.; Gray, J.J. Characterisation of norovirus strains in rural Ghanaian children with acute diarrhoea. J. Med. Virol. 2006, 78, 1480–1485. [Google Scholar] [CrossRef] [PubMed]
- Reither, K.; Ignatius, R.; Weitzel, T.; Seidu-Korkor, A.; Anyidoho, L.; Saad, E.; Djie-Maletz, A.; Ziniel, P.; Amoo-Sakyi, F.; Danikuu, F.; et al. Acute childhood diarrhoea in northern Ghana: Epidemiological, clinical and microbiological characteristics. BMC Infect. Dis. 2007, 7, 104. [Google Scholar] [CrossRef] [Green Version]
- Chen, J.C.; Lartey, B.; Agbemabiese, C.; Mahmoud, A.; Armah, G.E. The Epidemiology of Noroviruses in Ghana A Case Study of Norovirus Detection. J. Glob. Health 2013, 3, 11–14. [Google Scholar]
- Munjita, S.M. Current Status of Norovirus Infections in Children in Sub-Saharan Africa. J. Trop. Med. 2015, 2015, 309648. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mans, J.; Armah, G.E.; Steele, A.D.; Taylor, M.B. Norovirus Epidemiology in Africa: A Review. PLoS ONE 2016, 11, e0146280. [Google Scholar] [CrossRef] [Green Version]
- Shioda, K.; Kambhampati, A.; Hall, A.J.; Lopman, B.A. Global age distribution of pediatric norovirus cases. Vaccine 2015, 33, 4065–4068. [Google Scholar] [CrossRef] [Green Version]
- Abugalia, M.; Cuevas, L.; Kirby, A.; Dove, W.; Nakagomi, O.; Nakagomi, T.; Kara, M.; Gweder, R.; Smeo, M.; Cunliffe, N. Clinical features and molecular epidemiology of rotavirus and norovirus infections in Libyan children. J. Med. Virol. 2011, 83, 1849–1856. [Google Scholar] [CrossRef]
- Ayolabi, C.; Ojo, D.; Armah, G.E.; Akpan, I.; Mafiana, C. Detection and partial characterization of norovirus among children with acute gastroenteritis in Lagos, Nigeria. Int. J. Med. Med. Sci. 2010, 2, 216–221. [Google Scholar]
- Papaventsis, D.C.; Dove, W.; Cunliffe, N.A.; Nakagomi, O.; Combe, P.; Grosjean, P.; Hart, C.A. Norovirus infection in children with acute gastroenteritis, Madagascar, 2004–2005. Emerg. Infect. Dis. 2017, 13, 908–911. [Google Scholar] [CrossRef] [PubMed]
- Hoa Tran, T.N.; Trainor, E.; Nakagomi, T.; Cunliffe, N.A.; Nakagomi, O. Molecular epidemiology of noroviruses associated with acute sporadic gastroenteritis in children: Global distribution of genogroups, genotypes and GII.4 variants. J. Clin. Virol. 2013, 56, 185–193. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ahmed, S.; Lopman, B.; Levy, K. A systematic review and meta-analysis of the global seasonality of norovirus. PLoS ONE 2013, 8, e75922. [Google Scholar] [CrossRef]
- Armah, G.; Steele, A.; Binka, F.; Esona, M.; Asmah, R.; Anto, F.; Brown, D.; Green, J.; Cutts, F.; Hall, A. Changing patterns of rotavirus genotypes in Ghana: Emergence of human rotavirus G9 as a major cause of diarrhea in children. J. Clin. Microbiol. 2003, 41. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nordgren, J.; Nitiema, L.W.; Ouermi, D.; Simpore, J.; Svensson, L. Host genetic factors affect susceptibility to norovirus infections in Burkina Faso. PLoS ONE 2013, 8, e69557. [Google Scholar] [CrossRef]
- Oluwatoyin, J.M.; Adeyemi, A.O.; Famurewa, O.; Svensson, L.; Nordgren, J. Molecular epidemiology of rotavirus and norovirus in Ile-Ife, Nigeria: High prevalence of G12P[8] rotavirus strains and detection of a rare norovirus genotype. J. Med. Virol. 2012, 84, 1489–1496. [Google Scholar] [CrossRef]
- Karst, S.M. Pathogenesis of noroviruses, emerging RNA viruses. Viruses 2010, 2, 748–781. [Google Scholar] [CrossRef]
- Inoue, K.; Motomura, K.; Boonchan, M.; Takeda, N.; Ruchusatsawa, K.; Guntapong, R.; Tacharoenmuang, R.; Sangkitporn, S.; Chantaroj, S. Molecular detection and characterization of noroviruses in river water in Thailand. Lett. Appl. Microbiol. 2016, 62, 243–249. [Google Scholar] [CrossRef]
- Kitajima, M.; Haramoto, E.; Phanuwan, C.; Katayama, H.; Furumai, H. Molecular detection and genotyping of human noroviruses in influent and effluent water at a wastewater treatment plant in Japan. J. Appl. Microbiol. 2012, 112, 605–613. [Google Scholar] [CrossRef]
- Parra, G.I.; Squires, R.B.; Karangwa, C.K.; Johnson, J.A.; Lepore, C.J.; Sosnovtsev, S.V.; Green, K.Y. Static and Evolving Norovirus Genotypes: Implications for Epidemiology and Immunity. PLoS Pathog. 2017, 13, 1006136. [Google Scholar] [CrossRef]
- Immurana, M.; Urmi, A.U. Socio-economic factors and child health status in Ghana. Int. J. Health 2017, 5, 100–106. [Google Scholar] [CrossRef] [Green Version]
- Van Beek, J.; de Graaf, M.; Al-Hello, H.; Allen, D.J.; Ambert-Balay, K.; Botteldoorn, N.; Brytting, M.; Buesa, J.; Cabrerizo, M.; Chan, M.; et al. Molecular surveillance of norovirus, 2005-16: An epidemiological analysis of data collected from the NoroNet network. Lancet Infect. Dis. 2018, 18, 545–553. [Google Scholar] [CrossRef]
- Verhoef, L.; Hewitt, J.; Barclay, L.; Ahmed, S.M.; Lake, R.; Hall, A.J.; Lopman, B.; Kroneman, A.; Vennema, H.; Vinjé, J.; et al. Norovirus genotype profiles associated with foodborne transmission, 1999–2012. Emerg. Infect. Dis 2015, 21, 592–599. [Google Scholar] [CrossRef] [PubMed]
- Nenonen, N.P.; Hannoun, C.; Larsson, C.U.; Bergström, T. Marked Genomic Diversity of Norovirus Genogroup I Strains in a Waterborne Outbreak. Appl. Environ. Microbiol. 2012, 78, 1846–1852. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- De Graaf, M.; van Beek, J.; Vennema, H.; Podkolzin, A.T.; Hewitt, J.; Bucardo, F.; Templeton, K.; Mans, J.; Nordgren, J.; Reuter, G.; et al. Emergence of a novel GII.17 norovirus - End of the GII.4 era? Euro Surveill. 2015, 20, 21178. [Google Scholar] [CrossRef] [Green Version]
- Fu, J.; Ai, J.; Jin, M.; Jiang, C.; Zhang, J.; Shi, C.; Lin, Q.; Yuan, Z.; Qi, X.; Bao, C.; et al. Emergence of a new GII.17 norovirus variant in patients with acute gastroenteritis in Jiangsu, China, September 2014 to March 2015. Euro Surveill. 2015, 20, 21157. [Google Scholar] [CrossRef] [Green Version]
- Desai, R.; Hembree, C.D.; Handel, A.; Matthews, J.E.; Dickey, B.W.; McDonald, S.; Hall, A.J.; Parashar, U.D.; Leon, J.S.; Lopman, B. Severe outcomes are associated with genogroup 2 genotype 4 norovirus outbreaks: A systematic literature review. Clin. Infect. Dis. Off. Publ. Infect. Dis. Soc. Am. 2012, 55, 189–193. [Google Scholar] [CrossRef] [Green Version]
- Huhti, L.; Szakal, E.D.; Puustinen, L.; Salminen, M.; Huhtala, H.; Valve, O.; Blazevic, V.; Vesikari, T. Norovirus GII-4 causes a more severe gastroenteritis than other noroviruses in young children. J. Infect. Dis. 2011, 203, 1442–1444. [Google Scholar] [CrossRef] [Green Version]
- Mathew, S.; Alansari, K.K.; Smatti, M.; Zaraket, H.; Al Thani, A.A.; Yassine, H.M. Epidemiological, Molecular, and Clinical Features of Norovirus Infections among Pediatric Patients in Qatar. Viruses 2019, 11, 400. [Google Scholar] [CrossRef] [Green Version]



{kind=link}
{kind=link}
| Total Tested | NoV Pos (%) | OR (95% CI) | p-Value | |
|---|---|---|---|---|
| * Subject Number | 1142 | 435 | - | - |
| Clinical Profile | ||||
| Diarrhea Duration/day | ||||
| 1–4 | 967 | 381 (39.4) | Ref | |
| 5 | 73 | 23 (31.5) | 0.71 (0.425–1.179) | 0.184 |
| ≥6 | 102 | 31 (30.4) | 0.67 (0.432–1.044) | 0.077 |
| Max No. of diarrheal stools/day | ||||
| ≥6 | 496 | 166 (33.5) | Ref | |
| 4–5 | 378 | 169 (44.7) | 1.61 (1.220–2.117) | 0.287 |
| 1–3 | 268 | 100 (37.3) | 1.18 (0.868–1.613) | 0.001 |
| Vomiting | ||||
| Absent | 325 | 100 (30.8) | Ref | |
| Present | 817 | 335 (41.0) | 1.56 (1.189–2.056) | 0.001 |
| vomit Duration/day | ||||
| 0 | 321 | 99 (30.8) | Ref | |
| 1 | 150 | 69 (46.0) | 1.91 (1.282–2.847) | 0.001 |
| 2 | 234 | 91 (38.9) | 1.43 (1.002–2.033) | 0.049 |
| ≥3 | 437 | 176 (40.3) | 1.51 (1.115–2.050) | 0.008 |
| Max No. of Vomiting episodes/day | ||||
| 0 | 324 | 103 (31.8) | Ref | |
| 1 | 49 | 16 (32.7) | 1.04 (0.548–1.975) | 0.904 |
| 2–4 | 383 | 165 (43.1) | 1.62 (1.192–2.212) | 0.002 |
| ≥5 | 386 | 151 (39.1) | 1.38 (1.010–1.880) | 0.043 |
| Temperature (Fever) | ||||
| 37.1–38.4 | 759 | 254 (33.5) | Ref | |
| 38.5–38.9 | 333 | 154 (46.3) | 1.71 (1.315–2.225) | 0.000 |
| ≥39.0 | 48 | 27 (56.3) | 2.56 (1.417–4.610) | 0.002 |
| Dehydration (as assessed by clinician) | ||||
| None | 480 | 151 (31.5) | Ref | |
| Mild | 238 | 81 (34.0) | 1.11 (0.801–1.549) | 0.523 |
| Moderate | 273 | 150 (55.0) | 2.65 (1.950–3.599) | 0.000 |
| Severe | 148 | 52 (35.1) | 1.18 (0.798–1.735) | 1.176 |
| Treatment | ||||
| Rehydration | 216 | 50 (23.2) | Ref | |
| Hospitalization | 155 | 86 (55.5) | 4.14 (2.645–6.474) | 0.000 |
| Rehydration/Hospitalization | 770 | 299 (38.8) | 2.11 (1.488–2.984) | 0.000 |
| * Vesikari Score | ||||
| Non-Severe (<11) | 273 | 75 (27.5) | Ref | |
| Severe (≥11) | 864 | 359 (41.6) | 1.88 (1.393–2.529) | 0.000 |
| Norovirus Type | Vesikari Score (VS) | Total | ||
|---|---|---|---|---|
| Mild (%) | Moderate (%) | Severe (%) | ||
| NoV Genogroup | 5 (1.2) | 70 (16.1) | 359 (82.7) | 434 (100) |
| GI | 0 | 12 (18.2) | 54 (81.8) | 66 |
| GII | 5 (1.5) | 51 (15.6) | 270 (82.8) | 326 |
| GI/GII | 0 | 7 (16.7) | 35 (83.3) | 42 |
| GII Cap/Pol Genotypes | 1 (0.7) | 17 (11.9) | 125 (87.4) | 143 (100) |
| GII.4[P4] | 0 | 5 (11.4) | 39 (88.6) | 44 |
| GII.4[P16] | 0 | 2 (12.5) | 14 (87.5) | 16 |
| GII.3[P21] | 0 | 0 | 11 (100) | 11 |
| GII.6[P7] | 0 | 2 (28.5) | 5 (71.4) | 7 |
| GII.4[P31] | 0 | 1 (16.7) | 5 (83.3) | 6 |
| GII.21[P21] | 0 | 0 | 4 (100) | 4 |
| GII.17[P17] | 0 | 0 | 3 (100) | 3 |
| GII.9[P7] | 0 | 0 | 2 (100) | 2 |
| GII.8[P8] | 0 | 1 (50.0) | 1 (50.0) | 2 |
| GII.1[P33] | 0 | 1 (100) | 0 | 1 |
| GII.2[P30] | 0 | 0 | 1 (100) | 1 |
| GII.2[P31] | 0 | 0 | 1 (100) | 1 |
| GII.3[P16] | 0 | 0 | 1 (100) | 1 |
| GII.3[P30] | 0 | 0 | 1 (100) | 1 |
| GII.4[P7] | 0 | 1 (100) | 0 | 1 |
| GII.5[P16] | 0 | 1 (100) | 0 | 1 |
| GII.17[P3] | 0 | 0 | 1 (100) | 1 |
| GII.17[P13] | 0 | 0 | 1 (100) | 1 |
| GII.4[P_nd] | 0 | 1 (5.2) | 18 (94.7) | 19 |
| GII.5[P_nd] | 0 | 0 | 6 (100) | 6 |
| GII.2[P_nd] | 0 | 2 (66.7) | 1 (33.3) | 3 |
| GII.12[P_nd] | 0 | 0 | 3 (100) | 3 |
| GII.6[P_nd] | 0 | 0 | 2 (100) | 2 |
| GII.13[P_nd] | 1 (50.0) | 0 | 1 (50.0) | 2 |
| GII.17[P_nd] | 0 | 0 | 2 (100) | 2 |
| GII.7[P_nd] | 0 | 0 | 1 (100) | 1 |
| GII.10[P_nd] | 0 | 0 | 1 (100) | 1 |
| GI Cap/Pol Genotype | 0 | 3 (17.6) | 14 (82.4) | 17 (100) |
| GI.4[P4] | 0 | 2 (40.0) | 3 (60.0) | 5 |
| GI.7[P7] | 0 | 1 (25.0) | 3 (75.0) | 4 |
| GI.3[P3] | 0 | 0 | 2 (100) | 2 |
| GI.1[P1] | 0 | 0 | 1 (100) | 1 |
| GI.3[P13] | 0 | 0 | 1 (100) | 1 |
| GI.3[P14] | 0 | 0 | 1 (100) | 1 |
| GI.7[P_nd] | 0 | 0 | 2 (100) | 2 |
| GI.4[P_nd] | 0 | 0 | 1 (100) | 1 |
| Total | 1 (0.6) | 20 (12.5) | 139 (86.9) | 160 (100) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lartey, B.L.; Quaye, O.; Damanka, S.A.; Agbemabiese, C.A.; Armachie, J.; Dennis, F.E.; Enweronu-Laryea, C.; Armah, G.E. Understanding Pediatric Norovirus Epidemiology: A Decade of Study among Ghanaian Children. Viruses 2020, 12, 1321. https://doi.org/10.3390/v12111321
Lartey BL, Quaye O, Damanka SA, Agbemabiese CA, Armachie J, Dennis FE, Enweronu-Laryea C, Armah GE. Understanding Pediatric Norovirus Epidemiology: A Decade of Study among Ghanaian Children. Viruses. 2020; 12(11):1321. https://doi.org/10.3390/v12111321
Chicago/Turabian StyleLartey, Belinda L., Osbourne Quaye, Susan A. Damanka, Chantal A. Agbemabiese, Joseph Armachie, Francis E. Dennis, Christabel Enweronu-Laryea, and George E. Armah. 2020. "Understanding Pediatric Norovirus Epidemiology: A Decade of Study among Ghanaian Children" Viruses 12, no. 11: 1321. https://doi.org/10.3390/v12111321