

The Impact of Forest Therapy Programs on Stress Reduction: A Systematic Review

Abstract
:1. Introduction
2. Materials
2.1. Inclusion and Exclusion Criteria
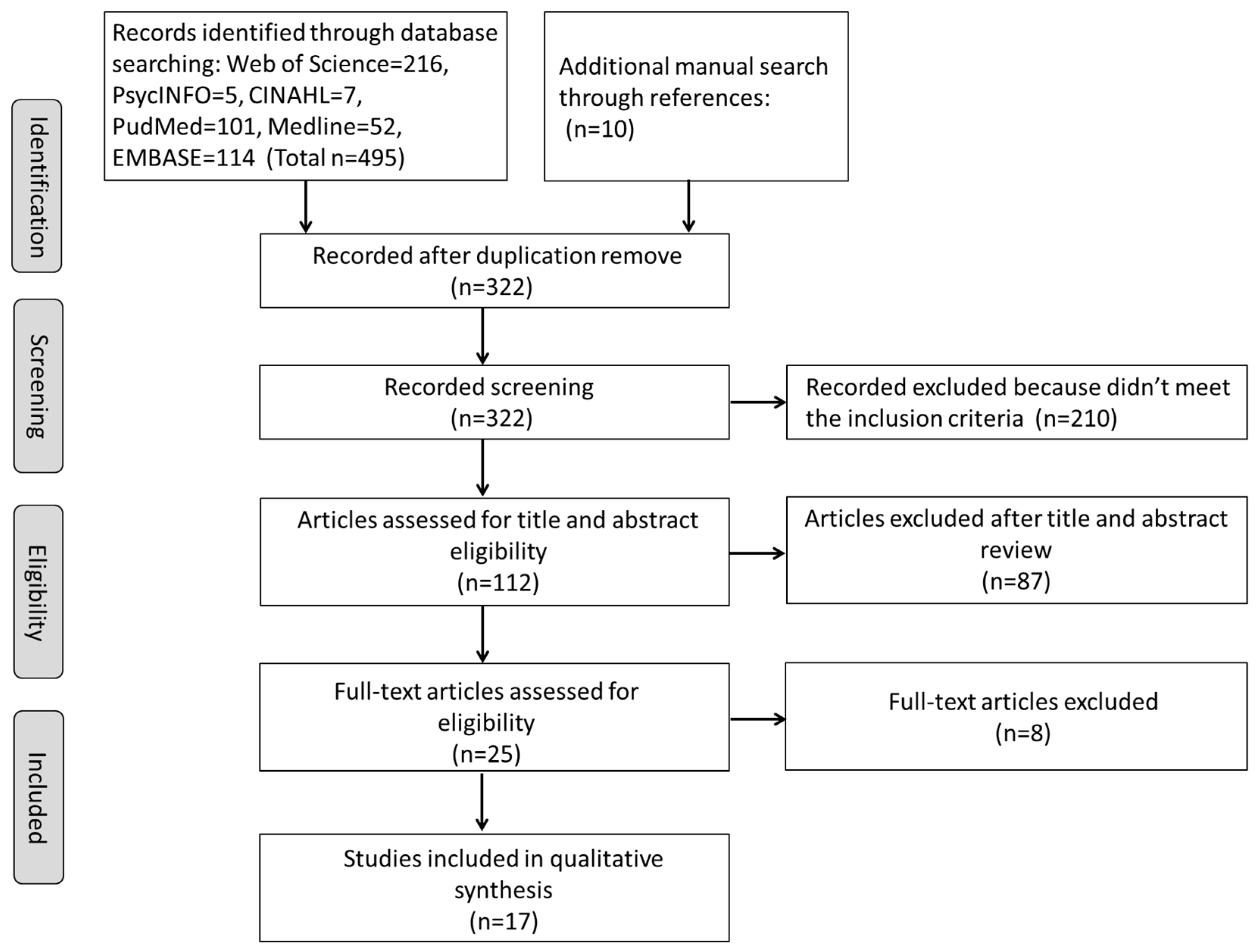
2.2. Study Selection Process
3. Results
3.1. Study Characteristics
3.2. Physiological Impact of Forest Therapy Programs on Stress Reduction
3.2.1. Cardiovascular Outcomes
3.2.2. Cortisol Levels
3.2.3. Other Physiological Impact
3.3. Psychological Impact of Forest Therapy Programs on Stress Reduction
3.3.1. Emotional and Mood Outcomes
3.3.2. Self-Perceived Stress Outcomes
3.3.3. Other Psychological Impact
3.4. Duration of Forest Therapy Programs and Stress Reduction
4. Discussion
4.1. Health Benefits of Forest Therapy Programs
4.2. Future Studies
4.3. Limitations of This Study
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Riva, M.; Curtis, S.; Gauvin, L.; Fagg, J. Unravelling the extent of inequalities in health across urban and rural areas: Evidence from a national sample in England. Soc. Sci. Med. 2009, 68, 654–663. [Google Scholar] [CrossRef] [PubMed]
- Lederbogen, F.; Kirsch, P.; Haddad, L.; Streit, F.; Tost, H.; Schuch, P.; Wüst, S.; Pruessner, J.C.; Rietschel, M.; Deuschle, M. City living and urban upbringing affect neural social stress processing in humans. Nature 2011, 474, 498–501. [Google Scholar] [CrossRef] [PubMed]
- Maja, V.; Jelena, T.D. Urban forest benefits to the younger population: The case study of the city of Belgrade, Serbia. For. Policy Econ. Hum. Biol. 2018, 96, 54–62. [Google Scholar]
- Lee, H.J.; Son, Y.-H.; Kim, S.; Lee, D.K. Healing experiences of middle-aged women through an urban forest therapy program. Urban For. Urban Green. 2019, 38, 383–391. [Google Scholar] [CrossRef]
- Aldwin, C.M. Stress, Coping, and Development: An Integrative Perspective; Guilford Press: New York, NY, USA, 2007. [Google Scholar]
- Ursin, H.; Eriksen, H.R. The cognitive activation theory of stress. Psychoneuroendocrinology 2004, 29, 567–592. [Google Scholar] [CrossRef]
- Selye, H. A syndrome produced by diverse nocuous agents. Nature 1936, 138, 32. [Google Scholar] [CrossRef]
- Mcewen, B.S. Stress, adaptation, and disease. Allostasis and allostatic load. Ann. New York Acad. Sci. 2010, 840, 33–44. [Google Scholar] [CrossRef] [PubMed]
- Mauss, I.B.; Levenson, R.W.; Mccarter, L.; Wilhelm, F.H.; Gross, J.J. The tie that binds? Coherence among emotion experience, behavior, and physiology. Emotion 2005, 5, 175–190. [Google Scholar] [CrossRef]
- Herman, J.P.; Ostrander, M.M.; Mueller, N.K.; Figueiredo, H. Limbic system mechanisms of stress regulation: Hypothalamo-pituitary-adrenocortical axis. Prog. Neuropsychopharmacol. Biol. Psychiatry 2005, 29, 1201–1213. [Google Scholar] [CrossRef]
- American Psychological Association. Stress in America: Coping with Change. Available online: https://www.apa.org/news/press/releases/stress/2016/coping-with-change.pdf (accessed on 10 February 2023).
- Australian Psychological Society. Stress and Wellbeing: How Australians Are Coping with life. Heads Up. 2015. Available online: https://www.headsup.org.au/docs/default-source/default-document-library/stress-and-wellbeing-in-australia-report.pdf (accessed on 13 March 2023).
- McEwen, B.S.; Gianaros, P.J. Central role of the brain in stress and adaptation: Links to socioeconomic status, health, and disease. Ann. New York Acad. Sci. 2010, 1186, 190–222. [Google Scholar] [CrossRef]
- Rajoo, K.S.; Karam, D.S.; Abdullah, M.Z. The physiological and psychosocial effects of forest therapy: A systematic review. Urban For. Urban Green. 2020, 54, 126744. [Google Scholar] [CrossRef]
- World Health Organization. Global Health Diplomacy: Negotiating Health in the 21st Century; WHO: Geneva, Switzerland, 2010. [Google Scholar]
- Bandelow, B.; Reitt, M.; Röver, C.; Michaelis, S.; Görlich, Y.; Wedekind, D. Efficacy of treatments for anxiety disorders: A meta-analysis. Int. Clin. Psychopharmacol. 2015, 30, 183–192. [Google Scholar] [CrossRef]
- Puetz, T.W.; Youngstedt, S.D.; Herring, M.P. Effects of pharmacotherapy on combat-related PTSD, anxiety, and depression: A systematic review and meta-regression analysis. PLoS ONE 2015, 10, e0126529. [Google Scholar] [CrossRef] [PubMed]
- Olfson, M.; King, M.; Schoenbaum, M. Benzodiazepine use in the United States. JAMA Psychiatry 2015, 72, 136–142. [Google Scholar] [CrossRef] [PubMed]
- Glacken, C.J. Traces on the Rhodian Shore: Nature and Culture in Western Thought from ANCIENT times to the End of the Eighteenth Century; University of California Press: Berkeley, CA, USA, 1967; Volume 170. [Google Scholar]
- Song, C.; Ikei, H.; Miyazaki, Y. Sustained effects of a forest therapy program on the blood pressure of office workers. Urban For. Urban Green. 2017, 27, 246–252. [Google Scholar] [CrossRef]
- Cheng, X.; Liu, J.; Liu, H.; Lu, S. A systematic review of evidence of additional health benefits from forest exposure. Landsc. Urban Plan. 2021, 212, 104123. [Google Scholar] [CrossRef]
- Lee, J.; Park, B.-J.; Tsunetsugu, Y.; Kagawa, T.; Miyazaki, Y. Restorative effects of viewing real forest landscapes, based on a comparison with urban landscapes. Scand. J. For. Res. 2009, 24, 227–234. [Google Scholar] [CrossRef]
- Ideno, Y.; Hayashi, K.; Abe, Y.; Ueda, K.; Iso, H.; Noda, M.; Lee, J.S.; Suzuki, S. Blood pressure-lowering effect of Shinrin-yoku (Forest bathing): A systematic review and meta-analysis. BMC Complement Altern. Med. 2017, 17, 409. [Google Scholar] [CrossRef]
- Park, B.J.; Tsunetsugu, Y.; Kasetani, T.; Kagawa, T.; Miyazaki, Y. The physiological effects of Shinrin-yoku (taking in the forest atmosphere or forest bathing): Evidence from field experiments in 24 forests across Japan. Env. Health Prev. Med. 2010, 15, 18–26. [Google Scholar] [CrossRef] [PubMed]
- Tsunetsugu, Y.; Park, B.J.; Ishii, H.; Hirano, H.; Kagawa, T.; Miyazaki, Y. Physiological effects of Shinrin-yoku (taking in the atmosphere of the forest) in an old-growth broadleaf forest in Yamagata Prefecture, Japan. J. Physiol. Anthr. 2007, 26, 135–142. [Google Scholar] [CrossRef] [PubMed]
- Bang, K.-S.; Lee, I.; Kim, S.; Lim, C.S.; Joh, H.-K.; Park, B.-J.; Song, M.K. The Effects of a Campus Forest-Walking Program on Undergraduate and Graduate Students’ Physical and Psychological Health. Int. J. Environ. Res. Public Health 2017, 14, 728. [Google Scholar] [CrossRef] [PubMed]
- Li, Q.; Morimoto, K.; Kobayashi, M.; Inagaki, H.; Katsumata, M.; Hirata, Y.; Hirata, K.; Shimizu, T.; Li, Y.; Wakayama, Y. A forest bathing trip increases human natural killer activity and expression of anti-cancer proteins in female subjects. J. Biol. Regul. Homeost Agents 2008, 22, 45–55. [Google Scholar] [PubMed]
- Kaplan, S. The restorative benefits of nature: Toward an integrative framework. J. Environ. Psychol. 1995, 15, 169–182. [Google Scholar] [CrossRef]
- Kaplan, R.; Kaplan, S. The Experience of Nature: A Psychological Perspective; Cambridge University Press: New York, NY, USA, 1989. [Google Scholar]
- Von Lindern, E. Perceived interdependencies between settings as constraints for self-reported restoration. J. Environ. Psychol. 2017, 49, 8–17. [Google Scholar] [CrossRef]
- Park, B.-J.; Tsunetsugu, Y.; Kasetani, T.; Morikawa, T.; Kagawa, T.; Miyazaki, Y. Physiological Effects of Forest Recreation in a Young Conifer Forest in Hinokage Town, Japan. Silva Fenn. 2009, 43, 291–301. [Google Scholar] [CrossRef]
- Song, C.; Ikei, H.; Kagawa, T.; Miyazaki, Y. Effects of Walking in a Forest on Young Women. Int. J. Environ. Res. Public Health 2019, 16, 229. [Google Scholar] [CrossRef]
- Morita, E.; Imai, M.; Okawa, M.; Miyaura, T.; Miyazaki, S. A before and after comparison of the effects of forest walking on the sleep of a community-based sample of people with sleep complaints. BioPsychoSocial Med. 2011, 5, 13. [Google Scholar] [CrossRef]
- Yu, C.-P.; Lin, C.-M.; Tsai, M.-J.; Tsai, Y.-C.; Chen, C.-Y. Effects of Short Forest Bathing Program on Autonomic Nervous System Activity and Mood States in Middle-Aged and Elderly Individuals. Int. J. Environ. Res. Public Health 2017, 14, 897. [Google Scholar] [CrossRef]
- Lee, J.; Tsunetsugu, Y.; Takayama, N.; Park, B.J.; Li, Q.; Song, C.; Komatsu, M.; Ikei, H.; Tyrväinen, L.; Kagawa, T.; et al. Influence of forest therapy on cardiovascular relaxation in young adults. Evid.-Based Complement. Altern. Med. Ecam 2014, 2014, 834360. [Google Scholar] [CrossRef]
- Hee, K.Y.; Kim, D.J.; Yeoun, P.S.; Choi, B.J. The Analysis of Interests and Needs for the Development of Forest Therapy Program in Adults. J. Korean Inst. For. Recreat. 2014, 18, 45–59. [Google Scholar]
- Jung, W.H.; Woo, J.M.; Ryu, J.S. Effect of a forest therapy program and the forest environment on female workers’ stress. Urban For. Urban Green. 2015, 14, 274–281. [Google Scholar] [CrossRef]
- Kim, J.G.; Khil, T.G.; Lim, Y.; Park, K.; Shin, M.; Shin, W.S. The Psychological Effects of a Campus Forest Therapy Program. Int J Env. Res Public Health 2020, 17, 3409. [Google Scholar] [CrossRef] [PubMed]
- Yu, C.-P.S.; Hsieh, H. Beyond restorative benefits: Evaluating the effect of forest therapy on creativity. Urban For. Urban Green. 2020, 51, 126670. [Google Scholar] [CrossRef]
- Kim, J.-G.; Shin, W.-S. Forest Therapy Alone or with a Guide: Is There a Difference between Self-Guided Forest Therapy and Guided Forest Therapy Programs? Int. J. Environ. Res. Public Health 2021, 18, 6957. [Google Scholar] [CrossRef] [PubMed]
- Rajoo, K.S.; Karam, D.S.; Wook, N.-F.; Abdullah, M.-Z. Forest Therapy: An environmental approach to managing stress in middle-aged working women. Urban For. Urban Green. 2020, 55, 126853. [Google Scholar] [CrossRef]
- Yi, Y.; Seo, E.; An, J. Does Forest Therapy Have Physio-Psychological Benefits? A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Int. J. Environ. Res. Public Health 2022, 19, 10512. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; Group, T.P. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. Int. J. Surg. 2009, 8, 336–341. [Google Scholar] [CrossRef]
- Yao, W.; Zhang, X.; Gong, Q. The effect of exposure to the natural environment on stress reduction: A meta-analysis. Urban For. Urban Green. 2021, 57, 126932. [Google Scholar] [CrossRef]
- Antonelli, M.; Barbieri, G.; Donelli, D. Effects of forest bathing (shinrin-yoku) on levels of cortisol as a stress biomarker: A systematic review and meta-analysis. Int. J. Biometeorol. 2019, 63, 1117–1134. [Google Scholar] [CrossRef]
- Bae, Y.J.; Reinelt, J.; Netto, J.; Uhlig, M.; Willenberg, A.; Ceglarek, U.; Villringer, A.; Thiery, J.; Gaebler, M.; Kratzsch, J. Salivary cortisone, as a biomarker for psychosocial stress, is associated with state anxiety and heart rate. Psychoneuroendocrinology 2019, 101, 35–41. [Google Scholar] [CrossRef]
- Matousek, R.H.; Dobkin, P.L.; Pruessner, J. Cortisol as a marker for improvement in mindfulness-based stress reduction. Complement. Ther. Clin. Pract. 2010, 16, 13–19. [Google Scholar] [CrossRef] [PubMed]
- Van Cauter, E.; Leproult, R.; Kupfer, D.J. Effects of gender and age on the levels and circadian rhythmicity of plasma cortisol. J. Clin. Endocrinol. Metab. 1996, 81, 2468–2473. [Google Scholar] [PubMed]
- Smyth, J.M.; Ockenfels, M.C.; Gorin, A.A.; Catley, D.; Porter, L.S.; Kirschbaum, C.; Hellhammer, D.H.; Stone, A.A. Individual differences in the diurnal cycle of cortisol. Psychoneuroendocrinology 1997, 22, 89–105. [Google Scholar] [CrossRef]
- Ng, M.Y.; Karimzad, Y.; Menezes, R.J.; Wintersperger, B.J.; Li, Q.; Forero, J.; Paul, N.S.; Nguyen, E.T. Randomized controlled trial of relaxation music to reduce heart rate in patients undergoing cardiac CT. Eur. Radiol. 2016, 26, 3635–3642. [Google Scholar] [CrossRef] [PubMed]
- Ossebaard, H.C. Stress reduction by technology? An experimental study into the effects of brainmachines on burnout and state anxiety. Appl. Psychophysiol. Biofeedback 2000, 25, 93–101. [Google Scholar] [CrossRef] [PubMed]
- Lazarus, R.S. Psychological Stress and the Coping Process; McGraw-Hill: New York, NY, USA, 1966. [Google Scholar]
- Pelletier, C.L. The effect of music on decreasing arousal due to stress: A meta-analysis. J. Music Ther. 2004, 41, 192–214. [Google Scholar] [CrossRef]
- Szabo, A.; Nikházy, L.; Tihanyi, B.; Boros, S. An in-situ investigation of the acute effects of Bikram yoga on positive-and negative affect, and state-anxiety in context of perceived stress. J. Ment. Health 2017, 26, 156–160. [Google Scholar] [CrossRef]
- Rosa, C.D.; Larson, L.R.; Collado, S.; Profice, C.C. Forest therapy can prevent and treat depression: Evidence from meta-analyses. Urban For. Urban Green. 2021, 57, 126943. [Google Scholar] [CrossRef]
- Corazon, S.S.; Sidenius, U.; Poulsen, D.V.; Gramkow, M.C.; Stigsdotter, U.K.J.I.J.o.E.R.; Health, P. Psycho-physiological stress recovery in outdoor nature-based interventions: A systematic review of the past eight years of research. Int. J. Environ. Res. Public Health 2019, 16, 1711. [Google Scholar] [CrossRef]
- Sung, J.; Woo, J.M.; Kim, W.; Lim, S.K.; Chung, E.J. The effect of cognitive behavior therapy-based “forest therapy” program on blood pressure, salivary cortisol level, and quality of life in elderly hypertensive patients. Clin. Exp. Hypertens. 2012, 34, 1–7. [Google Scholar] [CrossRef]
- Ochiai, H.; Ikei, H.; Song, C.; Kobayashi, M.; Miura, T.; Kagawa, T.; Li, Q.; Kumeda, S.; Imai, M.; Miyazaki, Y. Physiological and Psychological Effects of a Forest Therapy Program on Middle-Aged Females. Int. J. Environ. Res. Public Health 2015, 12, 15222–15232. [Google Scholar] [CrossRef] [PubMed]
- Ochiai, H.; Ikei, H.; Song, C.; Kobayashi, M.; Takamatsu, A.; Miura, T.; Kagawa, T.; Li, Q.; Kumeda, S.; Imai, M. Physiological and psychological effects of forest therapy on middle-aged males with high-normal blood pressure. Int. J. Environ. Res. Public Health 2015, 12, 2532–2542. [Google Scholar] [CrossRef] [PubMed]
- Chun, M.H.; Chang, M.C.; Lee, S.J. The effects of forest therapy on depression and anxiety in patients with chronic stroke. Int. J. Neurosci. 2017, 127, 199–203. [Google Scholar] [CrossRef]
- Chen, H.-T.; Yu, C.-P.; Lee, H.-Y. The Effects of Forest Bathing on Stress Recovery: Evidence from Middle-Aged Females of Taiwan. Forests 2018, 9, 403. [Google Scholar] [CrossRef]
- Jin, L.H.; Son, S.A. Psychological and Physical Effects of 10 Weeks Urban Forest Therapy Program on Dementia Prevention in Low-Income Elderly Living Alone. J. People Plants Environ. 2018, 21, 557–564. [Google Scholar] [CrossRef]
- Bielinis, E.; Bielinis, L.; Krupinska-Szeluga, S.; Lukowski, A.; Takayama, N. The Effects of a Short Forest Recreation Program on Physiological and Psychological Relaxation in Young Polish Adults. Forests 2019, 10, 34. [Google Scholar] [CrossRef]
- Bielinis, E.; Jaroszewska, A.; Łukowski, A.; Takayama, N. The Effects of a Forest Therapy Programme on Mental Hospital Patients with Affective and Psychotic Disorders. Int. J. Environ. Res. Public Health 2019, 17, 118. [Google Scholar] [CrossRef]
- Rajoo, K.S.; Karam, D.S.; Abdul Aziz, N.A. Developing an effective forest therapy program to manage academic stress in conservative societies: A multi-disciplinary approach. Urban For. Urban Green. 2019, 43, 126353. [Google Scholar] [CrossRef]
- Kang, B.-H.; Won-sop, S. Forest therapy program reduces academic and job-seeking stress among college students. J. People Plants Environ. 2020, 23, 363–375. [Google Scholar] [CrossRef]
- Kim, H.; Kim, J.; Ju, H.J.; Jang, B.J.; Wang, T.K.; Kim, Y.I. Effect of Forest Therapy for Menopausal Women with Insomnia. Int. J. Environ. Res. Public Health 2020, 17, 6548. [Google Scholar] [CrossRef]
- Kim, J.G.; Jeon, J.; Shin, W.S. The Influence of Forest Activities in a University Campus Forest on Student’s Psychological Effects. Int. J. Environ. Res. Public Health 2021, 18, 2457. [Google Scholar] [CrossRef] [PubMed]
- Bum-Jin, P.; Won-Sop, S.; Chang-Seob, S.; Poung-Sik, Y.; Chung-Yeub, C.; Si-Hyung, L.; Dong-Jun, K.; Youn-Hee, K.; Chang-Eun, P.; Park, B.-J.; et al. Effects of Forest Therapy on Psychological Improvement in Middle-aged Women in Korea. J. Prev. Med. Public Health 2022, 55, 492–497. [Google Scholar] [CrossRef]
- Choi, H.; Jeon, Y.H.; Han, J.W.; Moon, J.; Kim, S.Y.; Woo, J.M. The Effects of a Forest Therapy on Work-Related Stress for Employees in the Manufacturing Industry: Randomized Control Study. Glob. Adv. Health Med. 2022, 11, 2164957X221100468. [Google Scholar] [CrossRef]
- Cvikl, D.; Avgustin, C.; Kreft, S. The Physiological and Psychological Effects Benefits of Forest Therapy (FT) on Tourists in the Kranjska Gora Destination. Forests 2022, 13, 1670. [Google Scholar] [CrossRef]
- Roman, M.J.; Devereux, R.B.; Kizer, J.R.; Lee, E.T.; Galloway, J.M.; Ali, T.; Umans, J.G.; Howard, B.V. Central pressure more strongly relates to vascular disease and outcome than does brachial pressure: The Strong Heart Study. Hypertension 2007, 50, 197–203. [Google Scholar] [CrossRef]
- McNair, D.M.; Lorr, M.; Droppleman, L. Profiles of Mood States; Educational Industrial Testing Services: San Diego, CA, USA, 1971. [Google Scholar]
- Chang, Y.C.; Lu, J.H. The revision of profile of mood state questionnaire. Sport Exerc. 2001, 3, 47–55. [Google Scholar]
- Spielberger, C.D. Manual for the State-Trait. Anxiety Inventory; Consulting Psychologists Press: Palo Alto, CA, USA, 1983. [Google Scholar]
- Brzozowski, P.J.P.P.B. Internal structure stability of positive and negative concepts. Pol. Psychol. Bull 1991, 22, 91–106. [Google Scholar]
- Choi, S.-M.; Kang, T.-Y.; Woo, J.-M. Development and validation of a modified form of the stress response inventory for workers. J. Korean Neuropsychiatr. Assoc. 2006, 541–553. [Google Scholar]
- Kang, Y.R. The Influence of Jobs Seeking Stress on Their Career Maturity Dance Majoring Students. Master’s Thesis, Dankook University, Yongin, Korea, 2006. [Google Scholar]
- Obradovic, M.; Lal, A.; Liedgens, H. Validity and responsiveness of EuroQol-5 dimension (EQ-5D) versus Short Form-6 dimension (SF-6D) questionnaire in chronic pain. Health Qual. Life Outcomes 2013, 11, 110–119. [Google Scholar] [CrossRef]
- Bielinis, E.; Takayama, N.; Boiko, S.; Omelan, A.; Bielinis, L. The effect of winter forest bathing on psychological relaxation of young Polish adults. Urban For. Urban Green. 2018, 29, 276–283. [Google Scholar] [CrossRef]
- Haga, A.; Halin, N.; Holmgren, M.; Sörqvist, P. Psychological restoration can depend on stimulus-source attribution: A challenge for the evolutionary account? Front. Psychol. 2016, 7, 1831. [Google Scholar] [CrossRef] [PubMed]
- Christrup, H. The Effect of Dance Therapy on the Concept of Body Image; Costonis, M., Ed.; University of Illinois: Urbana, IL, USA, 2017; pp. 153–161. [Google Scholar]
- Huang, W.; Lin, G. The relationship between urban green space and social health of individuals: A scoping review. Urban For. Urban Green. 2023, 85, 127969. [Google Scholar] [CrossRef]
- Mlinarić, A.; Horvat, M.; Šupak Smolčić, V. Dealing with the positive publication bias: Why you should really publish your negative results. Biochem. Medica 2017, 27, 447–452. [Google Scholar] [CrossRef] [PubMed]
- Neimann Rasmussen, L.; Montgomery, P. The prevalence of and factors associated with inclusion of non-English language studies in Campbell systematic reviews: A survey and meta-epidemiological study. Syst. Rev. 2018, 7, 129. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Author and Year | Country | Study Design | Population and Sample | Tool for Outcome Assessment | Intervention Condition and Duration | Results |
|---|---|---|---|---|---|---|
| Sung, Woo, Kim, Lim, and Chung, 2012 [57] | Republic of Korea | CCT | Elderly hypertensive patients from two local health centers; N = 56 (FT group = 28, Control group = 28); Mean age: FT group = 63 years (SD = ±11), Control group = 66 years (SD = ±7) | Salivary cortisol level | FT group: 3 days (cognitive interventions and behavioral techniques in a forest environment); Control group: Urban daily routine |
|
| Ochiai, Ikei, Song, Kobayashi, Miura, et al., 2015 [58] | Japan | pre/post | Females between the ages of 40 and 73 recruited from a health promotion center; N = 17; Mean age = 62.2 years (SD = ±9.4) | Salivary cortisol level | 4 h and 41 min (stroll, lecture, deep breathing, lie down, abdominal breathing and chat) |
|
| Ochiai, Ikei, Song, Kobayashi, Takamatsu, et al., 2015 [59] | Japan | pre/post | Males with high-normal blood pressure between the ages of 40 and 72; N = 9; Mean age = 56 years (SD = ±13.0) | Serum cortisol level | 4 h and 35 min (stroll, deep breathing, lie down, and sit) |
|
| Chun, Chang, and Lee, 2017 [60] | Republic of Korea | RCT | Patients with chronic stroke recruited from a stroke welfare center; N = 59 (FT group = 30, Control group = 29); FT = 62.1 years (SD = ± 8.3), Control group = 59.5 years (SD = ± 9.7) | STAI-S; d-ROM level; BAP | FT group: 4 days (meditating, experiencing the forest with all five senses, and walking through the forest); Control group: 4 days (meditation and walking activities were conducted similarly in an urban setting) |
|
| Chen, Yu, and Lee, 2018 [61] | China | pre/post | Middle-aged women recruited through the Internet; N = 16; Mean age = 46.88 years (SD = ±7.83) | Chinese revision of POMS; STAI-S; pulse rate; SBP; DBP; SAA | 2 days (2.5-h guided forest walk to stimulate the four senses, night walking on trails, and do-it-yourself handcrafts) |
|
| Jin and Son, 2018 [62] | Republic of Korea | CCT | Low-income elderly living alone recruited from community service centers; N = 61 (FT group= 30, Control group= 31); FT = 76.3 years (SD = ±4.3), Control group = 77 years (SD = ±8) | SRI | FT group: 10 weeks urban forest therapy program (warming up, walking, five senses meditation, and traditional play); Control group: Urban daily routine. |
|
| Ernest Bielinis, Bielinis, Krupinska-Szeluga, Lukowski, and Takayama, 2019 [63] | Poland | pre/post | Young Polish adults recruited from former friends of researchers and their acquaintances; N = 21; Mean age = 23.86 years (SD = ±2.67) | Pulse rate; SBP; DBP; MAP; POMS; PANAS; ROS; SVS | 5 h (program engaged participants’ 4 senses, traveling between sites in forest). |
|
| E. Bielinis, Jaroszewska, Łukowski, and Takayama, 2019 [64] | Poland | pre/post | Patients in mental hospitals suffering from affective and psychotic disorders; N = 50; Mean age = 42.44 years (SD = ±13.23) | POMS; STAI-S | 1 h and 45 min (forest walks with additional exercises in the forest environment) |
|
| Rajoo, Karam, and Abdul Aziz, 2019 [65] | Malaysia | pre/post | University students; N = 29; Mean age = 21.83 (SD = ±0.711) | SBP; DBP; pulse rate; non-standard academic stress self-assessment | 1 day (stroll, river soaking, sensory enjoyment, deep breathing exercises, group sharing) |
|
| B.-H. Kang and Won-sop, 2020 [66] | Republic of Korea | CCT | University students; N = 60 (FT group = 35, Control group = 25); Mean age = 21.5 years SD = ±1.74 | MBI-SS; Job-Seeking Stress Survey | FT group: 8 weeks, 2 h per time (stroll, forest bathing, playing with natural objects, tree climbing, massage, making a bouquet using leaves, rope games, mandala with leaves, dance); Control group: Urban daily routine |
|
| Kim et al., 2020 [67] | Republic of Korea | pre/post | Menopausal women with insomnia; N = 35; Mean age = 58.8 years (SD = ±3.9) | Serum cortisol level | 6 days (meditation, gymnastics, walking, leg massage and stretch, alternately bathing in warm and cold water, a five senses experience program) |
|
| Kim et al., 2020 [38] | Republic of Korea | RCT | University students; N = 38 (FT group = 19, Control group = 19); Mean age = 22 years | SRI-MF | FT group: 8 weeks, 1.5 h per session (forest dance, forest meditation, forest exercise, walk, others under the guidance of therapists); Control group: Urban daily routine |
|
| Rajoo, Karam, Wook, and Abdullah, 2020 [41] | Malaysia | pre/post | Middle-aged working women employed in service industries; N = 19; Mean age = 54.80 (SD = ±0.68) | SBP; DBP; pulse rate; non-standard stress self-assessment | 1 day (leisurely stroll, sensory enjoyment, breathing exercises, group sharing) |
|
| Kim, Jeon, and Shin, 2021 [68] | Republic of Korea | RCT | University students; N = 38 (FT group = 19, Control group = 19); Mean age = 22.1 years, SD = ±1.6 | SRI-MF | FT group: 8 weeks, 1 h per session (stretching, respiration, walking, meditation, and exercise); Control group: Urban daily routine |
|
| Bum-Jin et al., 2022 [69] | Republic of Korea | Crossover study | Middle-aged women; N = 53; Age = 40–65 years | POMS-B | 3 days in forest (meditation, Zen yoga, walking, healing touch exercises), 3 days in an urban site (activities were conducted similarly in an urban setting) |
|
| Choi et al., 2022 [70] | Republic of Korea | RCT | Full-time employees recruited from a public-sector manufacturing company; N = 42 (FT group = 21, Control group = 21); FT group mean age = 43.52 years, SD = ±7.33, Control group mean age = 45.86 years, SD = ±8.20 | NK cell activity; salivary cortisol level; HRV; POMS; WSRI-MF; EQ-VAS | FT group: 2 days in forest environment (walking, mindfulness-based meditation, mandala coloring); Control group: 2 days in urban environment (activities were conducted similarly in an urban setting) |
|
| Cvikl, Avgustin, and Kreft, 2022 [71] | Slovenia | pre/post | Tourists who were willing to spend forty-eight hours at Kranjska Gora; N = 47 | DHEA; salivary cortisol level; SBP; DBP; heart rate; stress index | 1 day (walking, forest based activities that emphasize hearing, sight, and smell) |
|
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zhang, Y.; Feng, L.; Duan, W. The Impact of Forest Therapy Programs on Stress Reduction: A Systematic Review. Forests 2023, 14, 1851. https://doi.org/10.3390/f14091851
Zhang Y, Feng L, Duan W. The Impact of Forest Therapy Programs on Stress Reduction: A Systematic Review. Forests. 2023; 14(9):1851. https://doi.org/10.3390/f14091851
Chicago/Turabian StyleZhang, Yawei, Lu Feng, and Wenjie Duan. 2023. "The Impact of Forest Therapy Programs on Stress Reduction: A Systematic Review" Forests 14, no. 9: 1851. https://doi.org/10.3390/f14091851