
Accelerating the Nature Deficit or Enhancing the Nature-Based Human Health during the Pandemic Era: An International Study in Cambodia, Indonesia, Japan, South Korea, and Myanmar, following the Start of the COVID-19 Pandemic



Abstract
:1. Introduction
2. Materials and Methods
2.1. Survey Procedure
2.2. Survey Instrument and Statistical Analysis
3. Results
3.1. A comparison between Recreational Behavior and Changed Perceptions of Nature
3.2. Confirmatory Factor Analysis
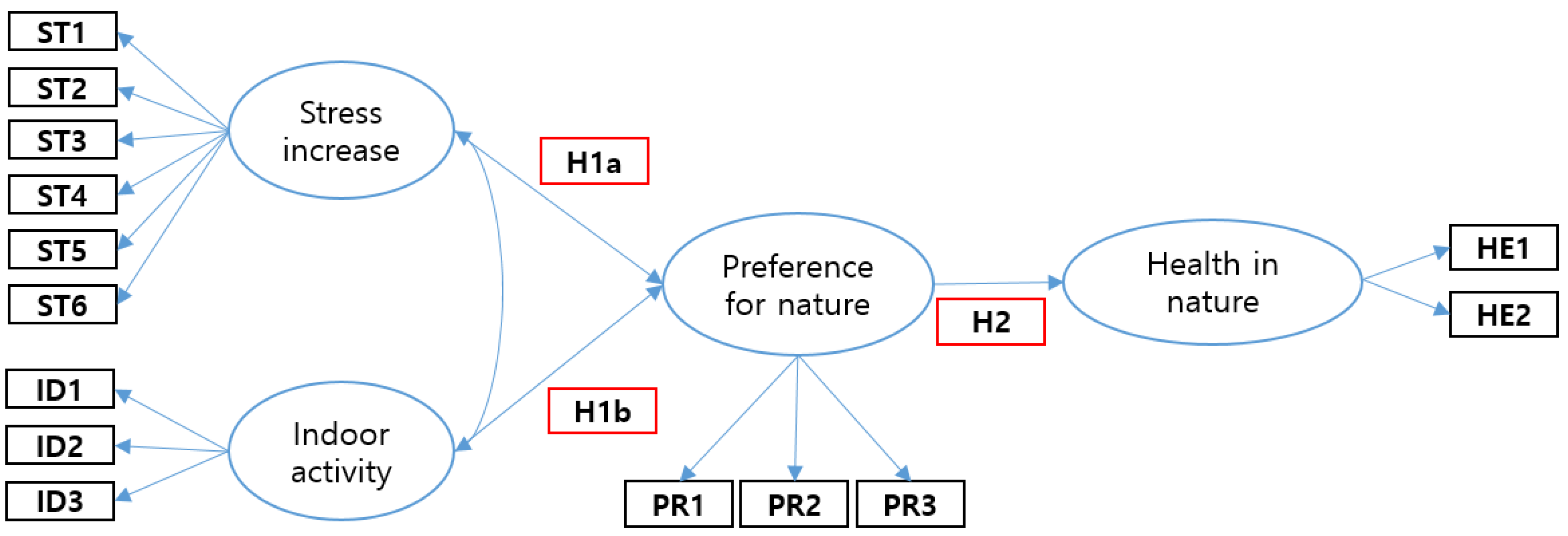
3.3. Structural Equation Model
4. Discussion
4.1. Isolation from Nature during the Pandemic: Increasing the Nature Deficit or Nature Experience
4.2. Enhanced Enthusiasm for Nature-Based Human Health: Overcoming Isolation from Nature
4.3. Study Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Ainsworth, B.E.; Li, F. Physical activity during the coronavirus disease-2019 global pandemic. J. Sport Health Sci. 2020, 9, 291–292. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Rolling Updates on Coronavirus Disease (COVID-19) Pandemic: WHO Characterizes COVID-19. Available online: https://www.who.int/emergencies/diseases/novel-coronavirus-2019/Events-as-they-happen (accessed on 4 December 2021).
- Yamori, K.; Goltz, J. Disasters without Borders: The Coronavirus Pandemic, Global Climate Change and the Ascendancy of Gradual Onset Disasters. Int. J. Environ. Res. Public Health 2021, 18, 3299. [Google Scholar] [CrossRef] [PubMed]
- Panneer, S.; Kantamaneni, K.; Pushparaj, R.; Shekhar, S.; Bhat, L.; Rice, L. Multistakeholder Participation in Disaster Management—The Case of the COVID-19 Pandemic. Healthcare 2021, 9, 203. [Google Scholar] [CrossRef] [PubMed]
- Chan, E.Y.Y.; Huang, Z.; Lo, E.S.K.; Hung, K.K.C.; Wong, E.L.Y.; Wong, S.Y.S. Sociodemographic Predictors of Health Risk Perception, Attitude and Behavior Practices Associated with Health-Emergency Disaster Risk Management for Biological Hazards: The Case of COVID-19 Pandemic in Hong Kong, SAR China. Int. J. Environ. Res. Public Health 2020, 17, 3869. [Google Scholar] [CrossRef] [PubMed]
- Kantor, A.; Kubiczek, J. Polish Culture in the Face of the COVID-19 Pandemic Crisis. J. Risk Financ. Manag. 2021, 14, 181. [Google Scholar] [CrossRef]
- Hakovirta, M.; Denuwara, N. How COVID-19 Redefines the Concept of Sustainability. Sustainability 2020, 12, 3727. [Google Scholar] [CrossRef]
- Landry, C.E.; Bergstrom, J.; Salazar, J.; Turner, D. How Has the COVID-19 Pandemic Affected Outdoor Recreation in the U.S.? A Revealed Preference Approach. Appl. Econ. Perspect. Policy 2021, 43, 443–457. [Google Scholar] [CrossRef]
- Rhodes, R.E.; Liu, S.; Lithopoulos, A.; Zhang, C.; Garcia-Barrera, M.A. Correlates of Perceived Physical Activity Transitions during the COVID-19 Pandemic among Canadian Adults. Appl. Psychol. Health Well-Being 2020, 12, 1157–1182. [Google Scholar] [CrossRef]
- Morse, J.W.; Gladkikh, T.M.; Hackenburg, D.M.; Gould, R.K. COVID-19 and human-nature relationships: Vermonters’ activities in nature and associated nonmaterial values during the pandemic. PLoS ONE 2020, 15, e0243697. [Google Scholar] [CrossRef]
- Küster, H. Geschichte der Landschaft in Mitteleuropa: Von der Eiszeit bis zur Gegenwart; CH Beck: Munich, Germany, 1999; 423p. [Google Scholar]
- Küster, H. Geschichte des Waldes: Von der Urzeit bis zur Gegenwart; CH Beck: Munich, Germany, 2003; 266p. [Google Scholar]
- Lees, L.; Phillips, M. Handbook of Gentrification Studies; Edward Elgar Publishing: Northampton, MA, USA, 2018; 520p. [Google Scholar]
- Stein, S. Capital City: Gentrification and the Real Estate State; Verso Books: Brooklyn, NY, USA, 2019; 208p. [Google Scholar]
- Atkinson, R. Alpha City: How London Was Captured by the Super-Rich; Verso Books: Brooklyn, NY, USA, 2021; 241p. [Google Scholar]
- Grebler, L. Urban Renewal in European Countries. J. Am. Inst. Plan. 1962, 28, 229–238. [Google Scholar] [CrossRef]
- Sklair, L. The Icon Project: Architecture, Cities, and Capitalist Globalization; Oxford University Press: New York, NY, USA, 2017; 329p. [Google Scholar]
- Lee, J.-H.; Lee, D.-J. Nature experience, recreation activity and health benefits of visitors in mountain and urban forests in Vienna, Zurich and Freiburg. J. Mt. Sci. 2015, 12, 1551–1561. [Google Scholar] [CrossRef]
- Lee, J.-H.; Lee, S.-J. Nature experience influences nature aversion: Comparison of South Korea and Germany. Soc. Behav. Pers. Int. J. 2018, 46, 161–176. [Google Scholar] [CrossRef]
- Sobel, D. Beyond Ecophobia; Orion Society: Great Barrington, MA, USA, 1996; 61p. [Google Scholar]
- Louv, R. Last Child in the Woods: Saving Our Children from Nature-Deficit Disorder; Algonquin Books: Chapel Hill, NC, USA, 2008; 390p. [Google Scholar]
- Strife, S.J. Children’s Environmental Concerns: Expressing Ecophobia. J. Environ. Educ. 2012, 43, 37–54. [Google Scholar] [CrossRef]
- Fabris, L.M.F.; Camerin, F.; Semprebon, G.; Balzarotti, R.M. New Healthy Settlements Responding to Pandemic Outbreaks: Approaches from (and for) the Global City. Plan J. 2020, 5, 385–406. [Google Scholar] [CrossRef]
- Mueller, N.; Rojas-Rueda, D.; Khreis, H.; Cirach, M.; Andrés, D.; Ballester, J.; Bartoll, X.; Daher, C.; Deluca, A.; Echave, C.; et al. Changing the urban design of cities for health: The superblock model. Environ. Int. 2020, 134, 105132. [Google Scholar] [CrossRef]
- Capolongo, S.; Rebecchi, A.; Buffoli, M.; Appolloni, L.; Signorelli, C.; Fara, G.M.; D’Alessandro, D. COVID-19 and Cities: From Urban Health strategies to the pandemic challenge. A Decalogue of Public Health opportunities. Acta Biomed. 2020, 91, 13–22. [Google Scholar] [CrossRef]
- Honey-Rosés, J.; Anguelovski, I.; Chireh, V.K.; Daher, C.; van den Bosch, C.K.; Litt, J.S.; Mawani, V.; McCall, M.K.; Orellana, A.; Oscilowicz, E.; et al. The impact of COVID-19 on public space: An early review of the emerging questions—Design, perceptions and inequities. Cities Health 2020, 1–17. [Google Scholar] [CrossRef]
- Slater, S.J.; Christiana, R.W.; Gustat, J. Recommendations for Keeping Parks and Green Space Accessible for Mental and Physical Health During COVID-19 and Other Pandemics. Prev. Chronic Dis. 2020, 17, E59. [Google Scholar] [CrossRef]
- Gecas, V.; Seff, M.A. Social Class and Self-Esteem: Psychological Centrality, Compensation, and the Relative Effects of Work and Home. Soc. Psychol. Q. 1990, 53, 165–173. [Google Scholar] [CrossRef]
- Moradi, H.; Vaezi, A. Lessons learned from Korea: COVID-19 pandemic. Infect. Control Hosp. Epidemiol. 2020, 41, 873–874. [Google Scholar] [CrossRef] [Green Version]
- Winter, P.L.; Selin, S.; Cerveny, L.; Bricker, K. Outdoor Recreation, Nature-Based Tourism, and Sustainability. Sustainability 2020, 12, 81. [Google Scholar] [CrossRef] [Green Version]
- Reis, A.C.; Thompson-Carr, A.; Lovelock, B. Parks and families: Addressing management facilitators and constraints to outdoor recreation participation. Ann. Leis. Res. 2012, 15, 315–334. [Google Scholar] [CrossRef]
- Heberlein, T.A. Navigating Environmental Attitudes; Oxford University Press: New York, NY, USA, 2012; 240p. [Google Scholar]
- Ekuo, M. How might contact with nature promote human health? Promising mechanisms and a possible central pathway. Front. Psychol. 2015, 6, 1093. [Google Scholar] [CrossRef]
- Hammitt, W.E.; Backlund, E.A.; Bixler, R.D. Experience Use History, Place Bonding and Resource Substitution of Trout Anglers During Recreation Engagements. J. Leis. Res. 2004, 36, 356–378. [Google Scholar] [CrossRef]
- Vaske, J.J. Survey Research and Analysis: Applications in Parks, Recreation and Human Dimensions; Venture Publishing: State College, PA, USA, 2008; 635p. [Google Scholar]
- Marsh, H.W.; Dowson, M.; Pietsch, J.; Walker, R. Why Multicollinearity Matters: A Reexamination of Relations between Self-Efficacy, Self-Concept, and Achievement. J. Educ. Psychol. 2004, 96, 518–522. [Google Scholar] [CrossRef]
- Rindam, N.; Islamul, H. Pembatasan Sosial Berskala Besar (PSBB) dan Masyarakat Berpenghasilan Rendah. J. Sos. Dan Budaya Syar-I 2020, 7, 639–648. [Google Scholar]
- Tun, U.T. The Measure of a Nation: Myanmar’s “Whole-of-Nation Approach” to Combatting COVID-19. Global New Light of Myanmar. Available online: https://www.memoscow.org/index.php/en/update-news/722-the-measure-of-a-nation-myanmar-s-whole-of-nation-approach-to-combatting-covid-19 (accessed on 4 December 2021).
- Nit, B.; Kobashi, Y.; Vory, S.; Lim, S.; Chea, S.; Ito, S.; Tsubokura, M. The introduction of telemedicine is required immediately in Cambodia: Barriers and lessons from COVID-19. J. Glob. Health 2021, 11, 03047. [Google Scholar] [CrossRef]
- Henseler, J.; Ringle, C.M.; Sarstedt, M. A new criterion for assessing discriminant validity in variance-based structural equation modeling. J. Acad. Mark. Sci. 2015, 43, 115–135. [Google Scholar] [CrossRef] [Green Version]
- Chen, F.F. Sensitivity of Goodness of Fit Indexes to Lack of Measurement Invariance. Struct. Equ. Model. Multidiscip. J. 2007, 14, 464–504. [Google Scholar] [CrossRef]
- Cangur, S.; Ercan, I. Comparison of model fit indices used in structural equation modeling under multivariate normality. J. Mod. Appl. Stat. Methods 2015, 14, 14. [Google Scholar] [CrossRef]
- Hu, L.-t.; Bentler, P.M. Cutoff criteria for fit indexes in covariance structure analysis: Conventional criteria versus new alternatives. Struct. Equ. Model. Multidiscip. J. 1999, 6, 1–55. [Google Scholar] [CrossRef]
- Steiger, J.H. Understanding the limitations of global fit assessment in structural equation modeling. Pers. Individ. Differ. 2007, 42, 893–898. [Google Scholar] [CrossRef]
- Kotera, Y.; Richardson, M.; Sheffield, D. Effects of Shinrin-Yoku (Forest Bathing) and Nature Therapy on Mental Health: A Systematic Review and Meta-analysis. Int. J. Ment. Health Addict. 2020, 1–25. [Google Scholar] [CrossRef]
- Shin, W.S.; Yeoun, P.S.; Yoo, R.W.; Shin, C.S. Forest experience and psychological health benefits: The state of the art and future prospect in Korea. Environ. Health Prev. Med. 2010, 15, 38–47. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Oh, K.H.; Shin, W.S.; Khil, T.G.; Kim, D.J. Six-Step Model of Nature-Based Therapy Process. Int. J. Environ. Res. Public Health 2020, 17, 685. [Google Scholar] [CrossRef] [Green Version]
- Ebenberger, M.; Arnberger, A. Exploring visual preferences for structural attributes of urban forest stands for restoration and heat relief. Urban For. Urban Green. 2019, 41, 272–282. [Google Scholar] [CrossRef]
- Nilsson, K.; Sangster, M.; Gallis, C.; Hartig, T.; De Vries, S.; Seeland, K.; Schipperijn, J. (Eds.) Forests, Trees and Human Health; Springer Science & Business Media: New York, NY, USA; Dordrecht, The Netherlands; Berlin/Heidelberg, Germany; London, UK, 2010; 427p. [Google Scholar]
- Park, B.-J.; Shin, C.-S.; Shin, W.-S.; Chung, C.-Y.; Lee, S.-H.; Kim, D.-J.; Kim, Y.-H.; Park, C.-E. Effects of Forest Therapy on Health Promotion among Middle-Aged Women: Focusing on Physiological Indicators. Int. J. Environ. Res. Public Health 2020, 17, 4348. [Google Scholar] [CrossRef]
- Arnberger, A.; Eder, R.; Allex, B.; Ebenberger, M.; Hutter, H.-P.; Wallner, P.; Bauer, N.; Zaller, J.G.; Frank, T. Health-Related Effects of Short Stays at Mountain Meadows, a River and an Urban Site—Results from a Field Experiment. Int. J. Environ. Res. Public Health 2018, 15, 2647. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, J.; Park, D.-B.; Seo, J.I. Exploring the Relationship between Forest Structure and Health. Forests 2020, 11, 1264. [Google Scholar] [CrossRef]
- Sacchelli, S.; Grilli, G.; Capecchi, I.; Bambi, L.; Barbierato, E.; Borghini, T. Neuroscience Application for the Analysis of Cultural Ecosystem Services Related to Stress Relief in Forest. Forests 2020, 11, 190. [Google Scholar] [CrossRef] [Green Version]
- Zeng, C.; Lin, W.; Li, N.; Wen, Y.; Wang, Y.; Jiang, W.; Zhang, J.; Zhong, H.; Chen, X.; Luo, W.; et al. Electroencephalography (EEG)-Based Neural Emotional Response to the Vegetation Density and Integrated Sound Environment in a Green Space. Forests 2021, 12, 1380. [Google Scholar] [CrossRef]
- Wang, Y.; Xu, M. Electroencephalogram Application for the Analysis of Stress Relief in the Seasonal Landscape. Int. J. Environ. Res. Public Health 2021, 18, 8522. [Google Scholar] [CrossRef]
- Olszewska-Guizzo, A.; Escoffier, N.; Chan, J.; Yok, T.P. Window View and the Brain: Effects of Floor Level and Green Cover on the Alpha and Beta Rhythms in a Passive Exposure EEG Experiment. Int. J. Environ. Res. Public Health 2018, 15, 2358. [Google Scholar] [CrossRef] [Green Version]
- Bae, Y.M.; Lee, Y.; Kim, S.-M.; Piao, Y.H. A Comparative Study on the Forest Therapy Policies of Japan and Korea. J. Korean For. Soc. 2014, 103, 299–306. [Google Scholar] [CrossRef] [Green Version]
- Ohe, Y.; Ikei, H.; Song, C.; Miyazaki, Y. Evaluating the relaxation effects of emerging forest-therapy tourism: A multidisciplinary approach. Tour. Manag. 2017, 62, 322–334. [Google Scholar] [CrossRef]
- Yonemura, M. Shared Visions and Common Roots: Montessori, Pratt and Steiner. Educ. Forum 1990, 54, 49–64. [Google Scholar] [CrossRef]
- Sellars, M.; Imig, D. Pestalozzi and pedagogies of love: Pathways to educational reform. Early Child Dev. Care 2021, 191, 1152–1163. [Google Scholar] [CrossRef]
- Locher, C.; Pforr, C. The Legacy of Sebastian Kneipp: Linking Wellness, Naturopathic, and Allopathic Medicine. J. Altern. Complement. Med. 2014, 20, 521–526. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rice, W.L.; Mateer, T.; Taff, B.D.; Lawhon, B.; Reigner, N.; Newman, P. Longitudinal Changes in the Outdoor Recreation Community’s Reaction to the COVID-19 Pandemic: Final Report on a Three-Phase National Survey of Outdoor Enthusiasts. SocArXiv 2020. [Google Scholar] [CrossRef]
- Ettman, C.K.; Abdalla, S.M.; Cohen, G.H.; Sampson, L.; Vivier, P.M.; Galea, S. Prevalence of Depression Symptoms in US Adults Before and During the COVID-19 Pandemic. JAMA Netw. Open 2020, 3, e2019686. [Google Scholar] [CrossRef]
- Bartoszek, A.; Walkowiak, D.; Bartoszek, A.; Kardas, G. Mental Well-Being (Depression, Loneliness, Insomnia, Daily Life Fatigue) during COVID-19 Related Home-Confinement—A Study from Poland. Int. J. Environ. Res. Public Health 2020, 17, 7417. [Google Scholar] [CrossRef]
- Nwachukwu, I.; Nkire, N.; Shalaby, R.; Hrabok, M.; Vuong, W.; Gusnowski, A.; Surood, S.; Urichuk, L.; Greenshaw, A.J.; Agyapong, V.I.O. COVID-19 Pandemic: Age-Related Differences in Measures of Stress, Anxiety and Depression in Canada. Int. J. Environ. Res. Public Health 2020, 17, 6366. [Google Scholar] [CrossRef]
- Stanton, R.; To, Q.G.; Khalesi, S.; Williams, S.L.; Alley, S.J.; Thwaite, T.L.; Fenning, A.S.; Vandelanotte, C. Depression, Anxiety and stress during COVID-19: Associations with changes in physical activity, sleep, tobacco and alcohol use in Australian adults. Int. J. Environ. Res. Public Health 2020, 17, 4065. [Google Scholar] [CrossRef]
- Chopdar, P.K.; Paul, J.; Prodanova, J. Mobile shoppers’ response to Covid-19 phobia, pessimism and smartphone addiction: Does social influence matter? Technol. Forecast. Soc. Chang. 2022, 174, 121249. [Google Scholar] [CrossRef]
- Elhai, J.D.; Yang, H.; McKay, D.; Asmundson, G.J. COVID-19 anxiety symptoms associated with problematic smartphone use severity in Chinese adults. J. Affect. Disord. 2020, 274, 576–582. [Google Scholar] [CrossRef]
- Limone, P.; Toto, G.A. Psychological and Emotional Effects of Digital Technology on Children in COVID-19 Pandemic. Brain Sci. 2021, 11, 1126. [Google Scholar] [CrossRef] [PubMed]
- Daglis, T. The Increase in Addiction during COVID-19. Encyclopedia 2021, 1, 1257–1266. [Google Scholar] [CrossRef]
- David, M.; Roberts, J. Smartphone Use during the COVID-19 Pandemic: Social Versus Physical Distancing. Int. J. Environ. Res. Public Health 2021, 18, 1034. [Google Scholar] [CrossRef] [PubMed]
- Nathan, A.; George, P.; Ng, M.; Wenden, E.; Bai, P.; Phiri, Z.; Christian, H. Impact of COVID-19 Restrictions on Western Australian Children’s Physical Activity and Screen Time. Int. J. Environ. Res. Public Health 2021, 18, 2583. [Google Scholar] [CrossRef] [PubMed]
- García-Tascón, M.; Sahelices-Pinto, C.; Mendaña-Cuervo, C.; Magaz-González, A.M. The Impact of the COVID-19 Confinement on the Habits of PA Practice According to Gender (Male/Female): Spanish Case. Int. J. Environ. Res. Public Health 2020, 17, 6961. [Google Scholar] [CrossRef]
- Kahn, P.H., Jr. Developmental Psychology and the Biophilia Hypothesis: Children’s Affiliation with Nature. Dev. Rev. 1997, 17, 1–61. [Google Scholar] [CrossRef]
- Gullone, E. The Biophilia Hypothesis and Life in the 21st Century: Increasing Mental Health or Increasing Pathology? J. Happiness Stud. 2000, 1, 293–322. [Google Scholar] [CrossRef]
- Lovelock, J. Gaia: The living Earth. Nature 2003, 426, 769–770. [Google Scholar] [CrossRef] [PubMed]
- Herzog, T.R. A cognitive analysis of preference for urban nature. J. Environ. Psychol. 1989, 9, 27–43. [Google Scholar] [CrossRef]
- Kaplan, R.; Kaplan, S. The Experience of Nature: A Psychological Perspective; Cambridge University Press: New York, NY, USA, 1989; 340p. [Google Scholar]
- Kaplan, S. The restorative benefits of nature: Toward an integrative framework. J. Environ. Psychol. 1995, 15, 169–182. [Google Scholar] [CrossRef]
- Kaplan, R. The Nature of the View from Home: Psychological benefits. Environ. Behav. 2001, 33, 507–542. [Google Scholar] [CrossRef]
- Cruz, M.P.; Santos, E.; Cervantes, M.V.; Juárez, M.L. COVID-19, a worldwide public health emergency. Rev. Clín. Española 2021, 221, 55–61. [Google Scholar] [CrossRef]
- Heymann, D.L.; Shindo, N. COVID-19: What is next for public health? Lancet 2020, 395, 542–545. [Google Scholar] [CrossRef] [Green Version]
- Hartley, D.M.; Perencevich, E.N. Public Health Interventions for COVID-19: Emerging evidence and implications for an evolving public health crisis. JAMA 2020, 323, 1908. [Google Scholar] [CrossRef] [Green Version]
- Hong, J.-Y.; Lee, J.-H. Analysis of Electroencephalogram and Electrocardiogram Changes in Adults in National Healing Forests Environment. J. People Plants Environ. 2018, 21, 575–589. [Google Scholar] [CrossRef] [Green Version]
- Lim, Y.-S.; Kim, J.; Khil, T.; Yi, J.; Kim, D.-J. Effects of the Forest Healing Program on Depression, Cognition, and the Autonomic Nervous System in the Elderly with Cognitive Decline. J. People Plants Environ. 2021, 24, 107–117. [Google Scholar] [CrossRef]
- Yu, Y.-M.; Lee, Y.-J.; Kim, J.-Y.; Yoon, S.-B.; Shin, C.-S. Effects of forest therapy camp on quality of life and stress in postmenopausal women. For. Sci. Technol. 2016, 12, 125–129. [Google Scholar] [CrossRef]
- Jung, W.H.; Woo, J.-M.; Ryu, J.S. Effect of a forest therapy program and the forest environment on female workers’ stress. Urban For. Urban Green. 2015, 14, 274–281. [Google Scholar] [CrossRef]
- Lee, M.-M.; Park, B.-J. Effects of Forest Healing Program on Depression, Stress and Cortisol Changes of Cancer Patients. J. People Plants Environ. 2020, 23, 245–254. [Google Scholar] [CrossRef]
- Li, Q.; Kobayashi, M.; Kumeda, S.; Ochiai, T.; Miura, T.; Kagawa, T.; Imai, M.; Wang, Z.; Otsuka, T.; Kawada, T. Effects of Forest Bathing on Cardiovascular and Metabolic Parameters in Middle-Aged Males. Evid.-Based Complement. Altern. Med. 2016, 2016, 2587381. [Google Scholar] [CrossRef]
- Ideno, Y.; Hayashi, K.; Abe, Y.; Ueda, K.; Iso, H.; Noda, M.; Lee, J.-S.; Suzuki, S. Blood pressure-lowering effect of Shinrin-yoku (Forest bathing): A systematic review and meta-analysis. BMC Complement. Altern. Med. 2017, 17, 409. [Google Scholar] [CrossRef] [PubMed]
- Baek, J.-E.; Shin, H.-J.; Kim, S.-H.; Kim, J.Y.; Park, S.; Sung, S.-Y.; Cho, H.-Y.; Hahm, S.-C.; Lee, M.-G. The Effects of Forest Healing Anti-aging Program on Physical Health of the Elderly: A Pilot Study. J. Korean Soc. Phys. Med. 2021, 16, 81–90. [Google Scholar] [CrossRef]
- Kim, T.; Song, B.; Cho, K.S.; Lee, I.-S. Therapeutic Potential of Volatile Terpenes and Terpenoids from Forests for Inflammatory Diseases. Int. J. Mol. Sci. 2020, 21, 2187. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Park, S.; Kim, S.; Kim, G.; Choi, Y.; Kim, E.; Paek, D. Evidence-Based Status of Forest Healing Program in South Korea. Int. J. Environ. Res. Public Health 2021, 18, 10368. [Google Scholar] [CrossRef] [PubMed]
- Dolling, A.; Nilsson, H.; Lundell, Y. Stress recovery in forest or handicraft environments—An intervention study. Urban For. Urban Green. 2017, 27, 162–172. [Google Scholar] [CrossRef]
- Kim, J.G.; Khil, T.G.; Lim, Y.; Park, K.; Shin, M.; Shin, W.S. The Psychological Effects of a Campus Forest Therapy Program. Int. J. Environ. Res. Public Health 2020, 17, 3409. [Google Scholar] [CrossRef]
- Bielinis, E.; Jaroszewska, A.; Łukowski, A.; Takayama, N. The Effects of a Forest Therapy Programme on Mental Hospital Patients with Affective and Psychotic Disorders. Int. J. Environ. Res. Public Health 2019, 17, 118. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Doimo, I.; Masiero, M.; Gatto, P. Forest and Wellbeing: Bridging Medical and Forest Research for Effective Forest-Based Initiatives. Forests 2020, 11, 791. [Google Scholar] [CrossRef]
- Kim, Y.-H. The preference analysis of adults on the forest therapy program with regard to demographic characteristics. J. Korean For. Soc. 2015, 104, 150–161. [Google Scholar] [CrossRef]
- Naomi, A.S. Access to Nature Has Always Been Important; with COVID-19, It Is Essential. HERD Health Environ. Res. Des. J. 2020, 13, 242–244. [Google Scholar] [CrossRef] [PubMed]
- Birkmeyer, J.D.; Barnato, A.; Birkmeyer, N.; Bessler, R.; Skinner, J. The Impact of the COVID-19 Pandemic on Hospital Admissions in the United States. Health Aff. 2020, 39, 2010–2017. [Google Scholar] [CrossRef]
- Treston, C. COVID-19 in the Year of the Nurse. J. Assoc. Nurses AIDS Care 2020, 31, 359–360. [Google Scholar] [CrossRef]
- Prestia, A.S. The Moral Obligation of Nurse Leaders. Nurse Lead. 2020, 18, 326–328. [Google Scholar] [CrossRef]
- Brode, N. 15% of Americans Plan to Hike More than Usual Due to COVID-19. Civic Science. 2020. Available online: https://civicscience.com/how-americans-are-fighting-cabin-fever/ (accessed on 4 December 2021).
- Venter, Z.S.; Barton, D.N.; Gundersen, V.; Figari, H.; Nowell, M. Urban nature in a time of crisis: Recreational use of green space increases during the COVID-19 outbreak in Oslo, Norway. Environ. Res. Lett. 2020, 15, 104075. [Google Scholar] [CrossRef]
- Gamil, Y.; Alhagar, A. The Impact of Pandemic Crisis on the Survival of Construction Industry: A Case of COVID-19. Mediterr. J. Soc. Sci. 2020, 11, 122. [Google Scholar] [CrossRef]
- Gursoy, D.; Chi, C.G. Effects of COVID-19 pandemic on hospitality industry: Review of the current situations and a research agenda. J. Hosp. Mark. Manag. 2020, 29, 527–529. [Google Scholar] [CrossRef]
- Laing, T. The economic impact of the Coronavirus 2019 (COVID-2019): Implications for the mining industry. Extr. Ind. Soc. 2020, 7, 580–582. [Google Scholar] [CrossRef] [PubMed]
- Gupta, M.; Abdelmaksoud, A.; Jafferany, M.; Lotti, T.; Sadoughifar, R.; Goldust, M. COVID-19 and economy. Dermatol. Ther. 2020, 33, e13329. [Google Scholar] [CrossRef]
- Shankar, K. The Impact of COVID-19 on IT Services Industry—Expected Transformations. Br. J. Manag. 2020, 31, 450–452. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Country/Surveyed Area | Forested Area /% of Land Surface | Population (Thousands) | GDP/People ($) | Survey Respondents | ||||
|---|---|---|---|---|---|---|---|---|
| Female/Total Respondents (%) | Age (%) | |||||||
| –29 | –39 | –49 | 50– | |||||
| Cambodia/Phnom Penh | 80,683 sq.km (45.7%) | 16,718 | 1512 | 41/97 (42.3%) | 64.9 | 20.6 | 10.3 | 4.1 |
| Indonesia/Jakarta | 921,332 sq.km (49.1%) | 273,523 | 3869 | 61/103 (59.2%) | 48.5 | 45.6 | 3.9 | 1.9 |
| Japan/Tokyo | 249,350 sq.km (68.4%) | 125,836 | 40,113 | 59/96 (61.5%) | 40.6 | 27.1 | 22.9 | 9.4 |
| Korea/Seoul | 62,870 sq.km (64.5%) | 51,780 | 31,489 | 95/146 (65.1%) | 31.9 | 30.4 | 28.8 | 8.9 |
| Myanmar/Yangon | 285,438 sq.km (43.7%) | 54,409 | 1400 | 59/100 (59.0%) | 55.0 | 15.0 | 25.0 | 5.0 |
| Category | Items | Var. | Cronbach α | ||||
|---|---|---|---|---|---|---|---|
| CA | IN | JA | KO | MY | |||
| Increased stress | I have decreased my economic activity since the start of the COVID-19 pandemic. | ST1 | 0.779 | 0.799 | 0.882 | 0.783 | 0.791 |
| I am uncomfortable with limited freedom of movement and activity. | ST2 | ||||||
| I am uncomfortable having little contact with other people. | ST3 | ||||||
| Since the start of the COVID-19 pandemic, communication with other people (apart from family) has decreased. | ST4 | ||||||
| Since the start of the COVID-19 pandemic, communication with my family has increased. * | ST5 | ||||||
| I have not had enough leisure activities since the start of the COVID-19 pandemic. | ST6 | ||||||
| Indoor activity | Since the start of the COVID-19 pandemic, my screen viewing time on smartphones, the Internet, and TVs has increased. | ID1 | 0.826 | 0.813 | 0.872 | 0.830 | 0.843 |
| Since the start of the COVID-19 pandemic, I have preferred online activities to offline activities (shopping, chatting, video meetings, etc.) | ID2 | ||||||
| In general, I don’t think it is a good idea to increase screen viewing time. | ID3 | ||||||
| Preference for nature | Since the start of the COVID-19 pandemic, I feel better when I go outdoors into a natural environment. * | PR1 | 0.894 | 0.850 | 0.944 | 0.853 | 0.829 |
| Since the start of the COVID-19 pandemic, it has become more difficult to go outdoors into a natural environment. | PR2 | ||||||
| Since the start of the COVID-19 pandemic, I have been more inclined to go outdoors into a natural environment as part of my usual routine. | PR3 | ||||||
| Perception of health in nature | Since the start of the COVID-19 pandemic, I have started to think that the natural environment really improves mental health. * | HE1 | 0.858 | 0.729 | 0.867 | 0.895 | 0.829 |
| Since the start of the COVID-19 pandemic, I have started to think that the natural environment really improves physical health. * | HE2 | ||||||
| Visit Frequency | Time Spent | |||||
|---|---|---|---|---|---|---|
| Pre-Pandemic | Post- Pandemic | t-Value | Pre-Pandemic | Post- Pandemic | t-Value | |
| Cambodia | 2.59 | 1.87 | 7.752 *** | 3.42 | 2.07 | 11.340 *** |
| Indonesia | 3.34 | 1.64 | 21.170 *** | 2.58 | 1.88 | 8.237 *** |
| Japan | 3.32 | 3.29 | 2.258 | 2.02 | 1.96 | 1.548 |
| Korea | 3.01 | 3.31 | −4.509 *** | 2.80 | 2.38 | 3.961 *** |
| Myanmar | 3.58 | 2.48 | 9.950 *** | 2.66 | 1.70 | 8.952 *** |
| Increased Stress | Indoor Activity | Preference for Nature | Visit Frequency | Time Spent | Psychological Benefit | Physical Benefit | |
|---|---|---|---|---|---|---|---|
| Cambodia | 3.47 | 4.13 | 3.77 | 1.87 | 2.07 | 4.08 | 4.01 |
| Indonesia | 3.37 | 4.23 | 3.62 | 1.64 | 1.88 | 4.06 | 4.04 |
| Japan | 3.52 | 3.58 | 3.42 | 3.29 | 1.96 | 3.46 | 3.35 |
| Korea | 3.77 | 3.82 | 4.03 | 3.31 | 2.38 | 4.24 | 4.08 |
| Myanmar | 3.26 | 4.23 | 3.54 | 2.48 | 1.70 | 4.26 | 4.11 |
| F-value | 23.385 *** | 33.424 *** | 26.198 *** | 110.081 *** | 12.836 *** | 22.156 *** | 22.948 *** |
| Category | Test Objects | Cambodia | Indonesia | Japan | Korea | Myanmar | |
|---|---|---|---|---|---|---|---|
| Increased stress | ß-coeff. | ST 1 | 0.409 | 0.625 | 0.887 | 0.556 | 0.737 |
| ST 2 | 0.822 | 0.571 | 0.84 | 0.806 | 0.935 | ||
| ST 3 | 0.797 | 0.659 | 0.894 | 0.833 | 0.862 | ||
| ST 4 | 0.604 | 0.740 | 0.707 | 0.723 | 0.632 | ||
| ST 5 | 0.484 | 0.484 | 0.582 | 0.316 | 0.301 | ||
| ST 6 | 0.580 | 0.707 | 0.565 | 0.460 | 0.343 | ||
| CR | 0.917 | 0.929 | 0.941 | 0.893 | 0.926 | ||
| AVE | 0.632 | 0.689 | 0.732 | 0.602 | 0.705 | ||
| Indoor activity | ß-coeff. | ID 1 | 0.859 | 0.853 | 0.973 | 0.901 | 0.760 |
| ID 2 | 0.870 | 0.846 | 0.978 | 0.898 | 0.841 | ||
| ID 3 | 0.633 | 0.625 | 0.572 | 0.599 | 0.804 | ||
| C.R | 0.922 | 0.947 | 0.960 | 0.906 | 0.948 | ||
| AVE | 0.801 | 0.857 | 0.895 | 0.769 | 0.860 | ||
| Preference for nature | ß-coeff. | PR 1 | 0.862 | 0.776 | 0.928 | 0.863 | 0.866 |
| PR 2 | 0.862 | 0.958 | 0.880 | 0.722 | 0.882 | ||
| PR 3 | 0.852 | 0.709 | 0.963 | 0.850 | 0.714 | ||
| C.R | 0.947 | 0.947 | 0.973 | 0.922 | 0.948 | ||
| AVE | 0.856 | 0.858 | 0.924 | 0.799 | 0.859 | ||
| Health in nature | ß-coeff. | HE 1 | 0.940 | 0.921 | 0.894 | 0.928 | 0.429 |
| HE 2 | 0.843 | 0.624 | 0.857 | 0.873 | 0.859 | ||
| C.R | 0.947 | 0.943 | 0.912 | 0.947 | 0.720 | ||
| AVE | 0.900 | 0.895 | 0.838 | 0.900 | 0.588 | ||
| Model fit summary | Chi2 | 85.538 | 121.600 | 155.414 | 102.944 | 109.353 | |
| p-value | 0.115 | 0.010 | 0.001 | 0.008 | 0.039 | ||
| GFI | 0.910 | 0.913 | 0.932 | 0.923 | 0.907 | ||
| AGFI | 0.878 | 0.877 | 0.916 | 0.896 | 0.897 | ||
| NFI | 0.936 | 0.942 | 0.955 | 0.948 | 0.929 | ||
| IFI | 0.974 | 0.939 | 0.957 | 0.964 | 0.959 | ||
| TLI | 0.966 | 0.919 | 0.943 | 0.953 | 0.946 | ||
| CFI | 0.974 | 0.937 | 0.956 | 0.963 | 0.958 | ||
| RMSEA | 0.046 | 0.065 | 0.061 | 0.056 | 0.056 |
| Hypothesis: Direction | Cambodia | Indonesia | Japan | Korea | Myanmar | |
|---|---|---|---|---|---|---|
| H1a: Stress → Nature | Estimate | 0.562 | 0.672 | 0.242 | 0.338 | 0.018 |
| S.E. | 0.173 | 0.171 | 0.110 | 0.152 | 0.149 | |
| C.R. | 1.857 | 1.254 | 1.290 | 0.927 | 0.162 | |
| P | 0.013 | 0.043 | 0.017 | 0.026 | 0.871 | |
| Result | Accept | Accept | Accept | Accept | Reject | |
| H1b: Indoor → Nature | Estimate | 0.288 | 0.247 | 0.093 | 0.247 | 0.290 |
| S.E. | 0.132 | 0.135 | 0.114 | 0.076 | 0.149 | |
| C.R. | 10.886 | 0.992 | 0.815 | 0.933 | 10.940 | |
| P | 0.044 | 0.318 | 0.415 | 0.040 | 0.042 | |
| Result | Accept | Reject | Reject | Accept | Accept | |
| H2: Nature → Health | Estimate | 0.304 | 0.873 | 0.528 | 0.565 | 0.198 |
| S.E. | 0.131 | 0.192 | 0.126 | 0.116 | 0.155 | |
| C.R. | 2.323 | 2.039 | 4.195 | .974 | .816 | |
| P | 0.002 | 0.041 | 0.000 | 0.000 | 0.045 | |
| Result | Accept | Accept | Accept | Accept | Accept | |
| Model fit test | Chi2 | 87.320 | 132.094 | 182.907 | 114.406 | 126.149 |
| p-value | 0.121 | 0.001 | 0.001 | 0.009 | 0.051 | |
| GFI | 0.908 | 0.909 | 0.928 | 0.921 | 0.901 | |
| AGFI | 0.870 | 0.874 | 0.915 | 0.890 | 0.893 | |
| NFI | 0.931 | 0.917 | 0.952 | 0.946 | 0.924 | |
| IFI | 0.972 | 0.924 | 0.954 | 0.954 | 0.944 | |
| TLI | 0.965 | 0.913 | 0.937 | 0.943 | 0.930 | |
| CFI | 0.973 | 0.925 | 0.951 | 0.952 | 0.941 | |
| RMSEA | 0.047 | 0.068 | 0.062 | 0.061 | 0.058 |
| Indirect Effect | Cambodia | Indonesia | Japan | Korea | Myanmar | |
|---|---|---|---|---|---|---|
| Stress → Nature → Health | Z-value | 1.888 | 2.973 | 1.947 | 2.022 | 0.120 |
| P | 0.058 | 0.002 | 0.051 | 0.043 | 0.904 | |
| Indoor → Nature → Health | Z-value | 1.589 | 1.697 | 0.800 | 2.703 | 1.067 |
| P | 0.111 | 0.089 | 0.423 | 0.006 | 0.285 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lee, J.-h.; Cheng, M.; Syamsi, M.N.; Lee, K.H.; Aung, T.R.; Burns, R.C. Accelerating the Nature Deficit or Enhancing the Nature-Based Human Health during the Pandemic Era: An International Study in Cambodia, Indonesia, Japan, South Korea, and Myanmar, following the Start of the COVID-19 Pandemic. Forests 2022, 13, 57. https://doi.org/10.3390/f13010057
Lee J-h, Cheng M, Syamsi MN, Lee KH, Aung TR, Burns RC. Accelerating the Nature Deficit or Enhancing the Nature-Based Human Health during the Pandemic Era: An International Study in Cambodia, Indonesia, Japan, South Korea, and Myanmar, following the Start of the COVID-19 Pandemic. Forests. 2022; 13(1):57. https://doi.org/10.3390/f13010057
Chicago/Turabian StyleLee, Ju-hyoung, Marady Cheng, Muhammad Nur Syamsi, Ki Hwan Lee, Thu Rain Aung, and Robert C. Burns. 2022. "Accelerating the Nature Deficit or Enhancing the Nature-Based Human Health during the Pandemic Era: An International Study in Cambodia, Indonesia, Japan, South Korea, and Myanmar, following the Start of the COVID-19 Pandemic" Forests 13, no. 1: 57. https://doi.org/10.3390/f13010057