
Finite Element Analysis of Different Osseocartilaginous Reconstruction Techniques in Animal Model Knees

 , , , ,
, , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Animal Model
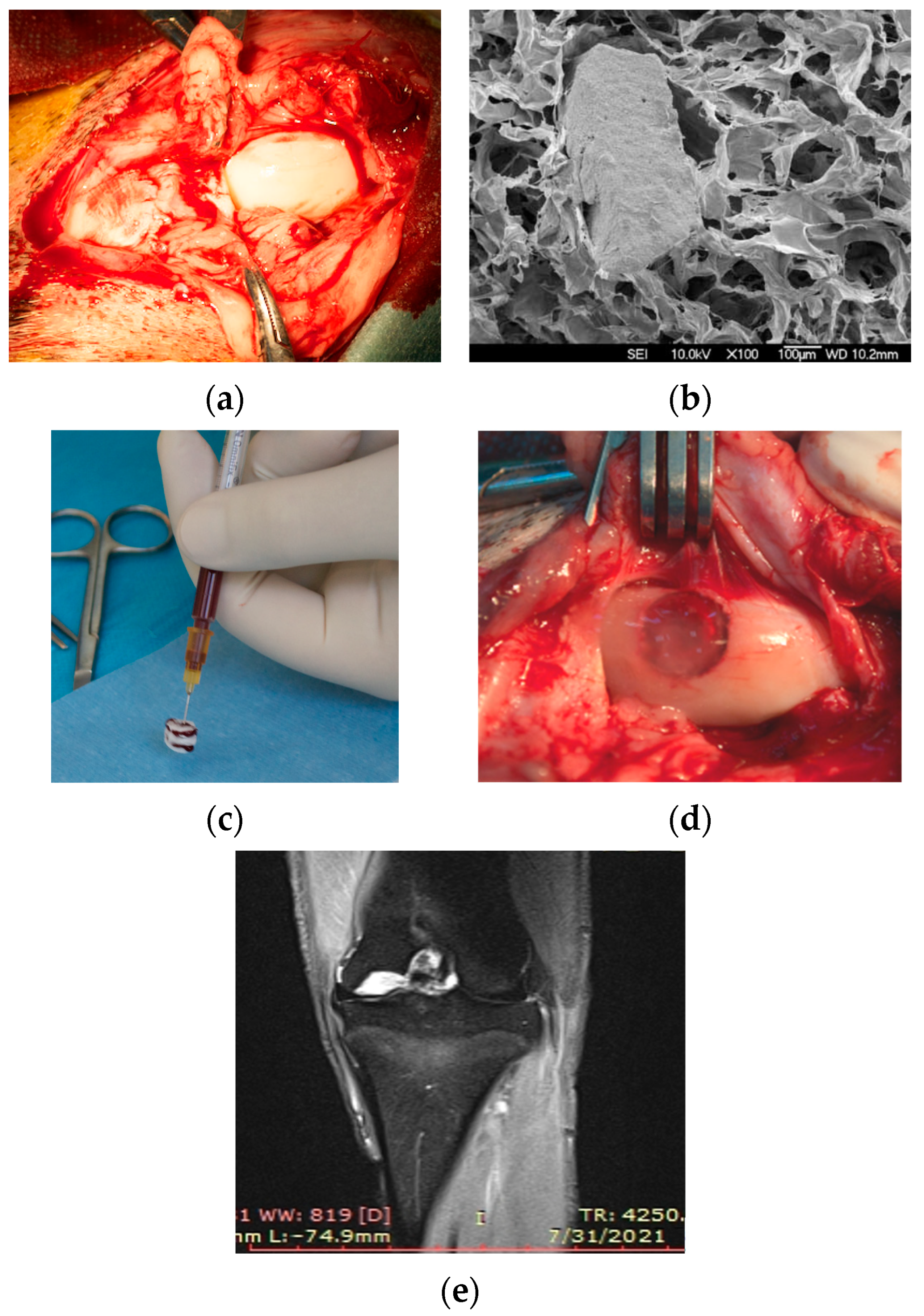
2.2. Surgical Procedure
2.3. CT Scanning and 3D Modelling
2.4. Knee Tissues Properties

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Tissue | Young Modulus [MPa] | Poisson Ratio | Density [g/cm3] | Compressive Strength [MPa] | Specific Heat [103 J/kg °C] | Thermal Expansion Coefficient [10−6/°C] | Thermal Conductivity [J/mm * s * °C] | References |
|---|---|---|---|---|---|---|---|---|
| Trabecular bone | 1500 | 0.30 | 0.61 | 2–16 | 0.44 | 10 | 0.58 | [1,33,34,35,36,37] |
| Cortical bone | 16,160 | 0.33 | 2.45 | 100–147 | [1,34,35,36,37,38,39] | |||
| Subchondral bone | 19,800 | 0.30 | 1.79 | 64 | [10,36,37,40,41] | |||
| Cartilage | 0.8 | 0.40 | 1.1 | 5–20 # | 0.32 | N/A | 0.21 | [1,27,42,43,44,45] |
| UC | 5000 | 0.30 | 1.32 | 5–100 ## | 1.6 | 5 | 0.57 | [5,29,30,31,46,47,48,49] |
| Synovial fluid | 1 | 0.49 | 1 | - | 0.39 | 3.9 * | 0.62 | [1,26,45] |
2.5. Conditions of FEA Simulations
3. Results
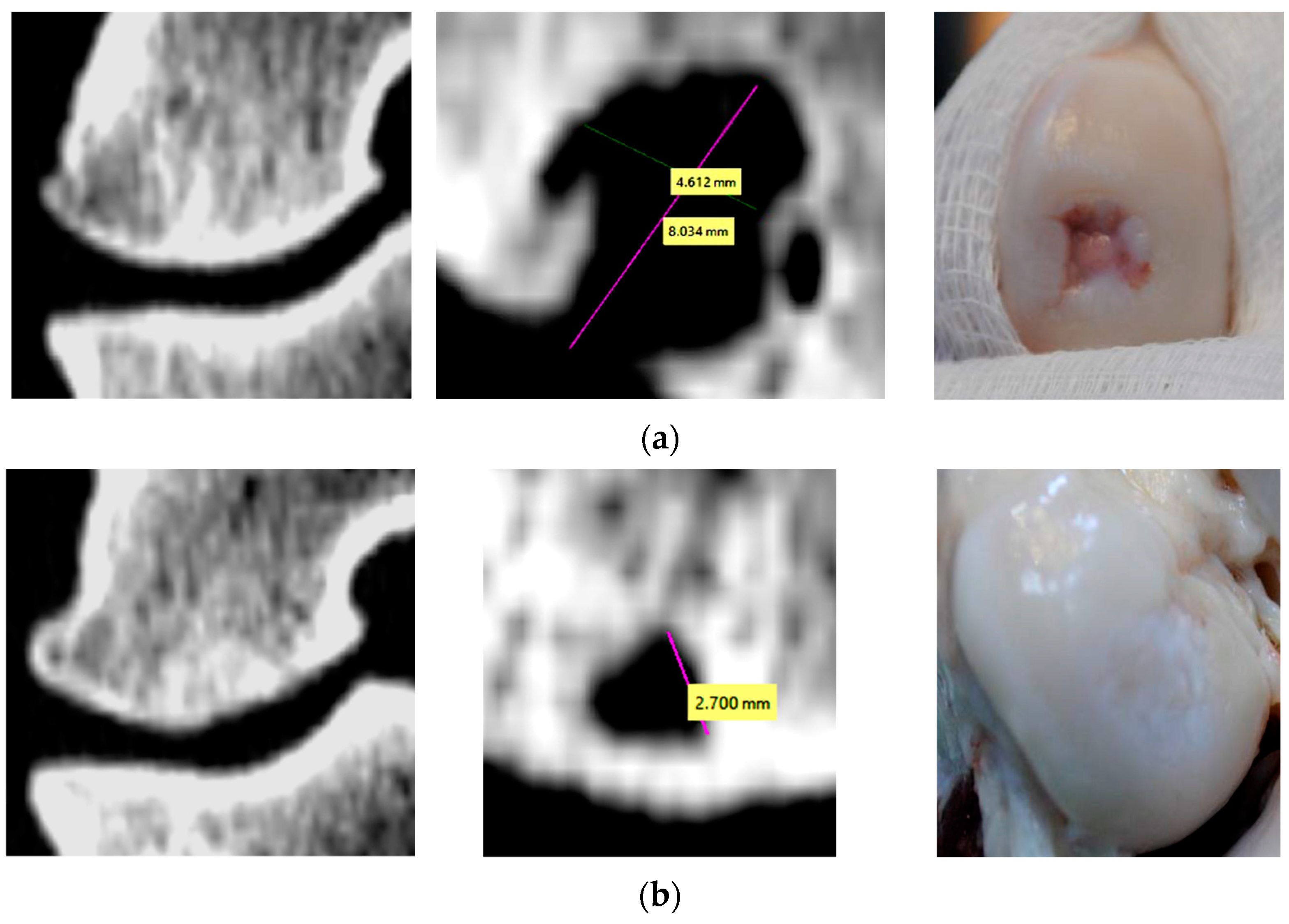
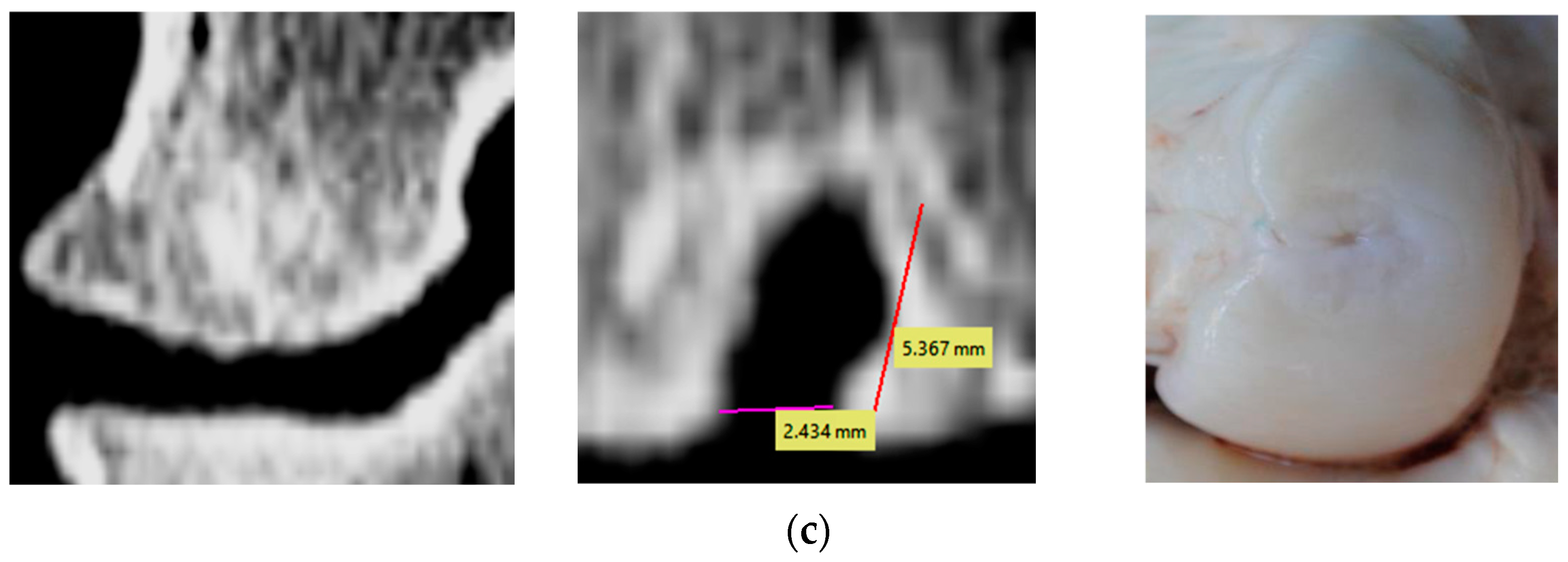
3.1. Evaluation of Bone Changes in Animal Model
3.2. Stress Distribution
3.3. Deformation and Displacement in Reconstruction Region
4. Discussion
4.1. Cartilage Tissue
4.2. Un-resorbed Collagen
4.3. Subchondral and Trabecular Bones
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Manda, K.; Ryd, L.; Eriksson, A. Finite element simulations of a focal knee resurfacing implant applied to localized cartilage defects in a sheep model. J. Biomech. 2011, 44, 794–801. [Google Scholar] [CrossRef]
- Gao, L.; Orth, P.; Goebel, K.H.; Cucchiarini, M.; Madry, H. A novel algorithm for a precise analysis of subchondral bone alterations. Nat. Sci. Rep. 2016, 6, 32982. [Google Scholar] [CrossRef] [PubMed]
- Bonnevie, E.D.; Delco, M.L.; Fortier, L.A.; Alexander, P.G.; Tuan, R.; Bonassar, L.J. Characterization of Tissue Response to Impact Loads Delivered Using a Hand-Held Instrument for Studying Articular Cartilage Injury. Cartilage 2015, 6, 226–232. [Google Scholar] [CrossRef] [Green Version]
- Kaleem, B.; Maier, F.; Drissi, H.; Pierce, D.M. Low-energy impact of human cartilage: Predictors for microcracking the network of collagen. Osteoarthr. Cartil. 2017, 25, 544–553. [Google Scholar] [CrossRef] [Green Version]
- Mononen, M.E.; Tanska, P.; Isaksson, H.; Korhonen, R.K. A Novel Method to Simulate the Progression of Collagen Degeneration of Cartilage in the Knee: Data from the Osteoarthritis Initiative. Nat. Sci. Rep. 2016, 6, 21415. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, S.H.; Park, D.Y.; Min, B.H. A New Era of Cartilage Repair using Cell Therapy and Tissue Engineering: Turning Current Clinical Limitations into New Ideas. Tissue Engineering and Regenerative Medicine 2012, 9, 240–248. [Google Scholar] [CrossRef]
- Gobbi, A.; Karnatzikos, G.; Mahajan, V. Biologic Arthroplasty. In Cartilage Repair: Clinical Guidelines; Brittberg, M., Ed.; DJO Publications: Guilford, Surrey, UK, 2012; pp. 269–279. [Google Scholar]
- Gobbi, A.; Bathan, L. Biological approaches for cartilage repair. J. Knee Surg. 2009, 22, 36–44. [Google Scholar] [CrossRef] [Green Version]
- Nakamura, T.; Sekiya, I.; Muneta, T.; Hatsushika, D.; Horie, M.; Tsuji, K.; Kawarasaki, T.; Watanabe, A.; Hishikawa, S.; Fujimoto, Y.; et al. Arthroscopic, histological and MRI analyses of cartilage repair after a minimally invasive method of transplantation of allogeneic synovial mesenchymal stromal cells into cartilage defects in pigs. Cytotherapy 2012, 14, 327–338. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Malekipour, F.; Oetomo, D.; Lee, P.V. Equine subchondral bone failure threshold under impact compression applied through articular cartilage. J. Biomech. 2016, 49, 2053–2059. [Google Scholar] [CrossRef]
- Martinez-Carranza, N.; Ryd, L.; Hultenby, K.; Hedlund, H.; Nurmi-Sandh, H.; Lagerstedt, A.S.; Schupbach, P.; Berg, H.E. Treatment of full thickness focal cartilage lesions with a metallic resurfacing implant in a sheep animal model, 1 year evaluation. Osteoarthr. Cartil. 2016, 24, 484–493. [Google Scholar] [CrossRef] [Green Version]
- Bobrowitsch, E.; Lorenz, A.; Wülker, N.; Walter, C. Simulation of in vivo dynamics during robot assisted joint movement. BioMedical Eng. OnLine 2014, 13, 167. [Google Scholar] [CrossRef] [Green Version]
- Kon, E.; Filardo, G.; Roffi, A.; Andriolo, L.; Marcacci, M. New trends for knee cartilage regeneration: From cell-free scaffolds to mesenchymal stem cells. Curr. Rev. Musculoskelet. Med. 2012, 5, 236–243. [Google Scholar] [CrossRef] [Green Version]
- Strioga, M.; Viswanathan, S.; Darinskas, A.; Slaby, O.; Michalek, J. Same or not the same? Comparison of adipose tissue-derived versus bone marrow derived mesenchymal stem and stromal cells. Stem. Cells Dev. 2012, 21, 2724–2752. [Google Scholar] [CrossRef] [PubMed]
- Tomoaia, G.; Benea, H.; Miclea, L. Computed study of shoulder dynamics and dynamic analysis of shoulder movement. In Proceedings of the IEEE International Conference on Automation, Quality and Testing, Robotics, Cluj-Napoca, Romania, 22–25 May 2008; Volume 3, pp. 90–93. [Google Scholar] [CrossRef]
- Leordean, D.V.; Dudescu, C.; Marcu, T.; Berce, P.; Balc, N. Customized implants with specific properties, made by selective laser melting. Rapid Prototyp. J. 2015, 21, 98–104. [Google Scholar] [CrossRef]
- Venäläinen, M.S.; Mononen, M.E.; Salo, J.; Räsänen, L.P.; Jurvelin, J.S.; Töyräs, J.; Virén, T.; Korhonen, R.K. Quantitative Evaluation of the Mechanical Risks Caused by Focal Cartilage Defects in the Knee. Nat. Sci. Rep. 2016, 6, 37538. [Google Scholar] [CrossRef] [Green Version]
- Amini, M.; Nazemi, S.M.; Lanovaz, J.L.; Kontulainen, S.; Masri, B.A.; Wilson, D.R.; Szyszkowski, W.; Johnston, J.D. Individual and combined effects of OA-related subchondral bone alterations on proximal tibial surface stiffness: A parametric finite element modeling study. Med. Eng. Phys. 2015, 37, 783–791. [Google Scholar] [CrossRef]
- Bahraminasab, M.; Sahari, B.B.; Hassan, M.R.; Arumugam, M.; Shamsborhan, M. Finite Element Analysis of the Effect of Shape Memory Alloy on the Stress Distribution and Contact Pressure in Total Knee Replacement. Trends Biomater. Artif. Organs 2011, 25, 95–100. [Google Scholar]
- Benea, H.R.C.; Earar, K.; Laittanzi, W.; Quercia, V.; Berce, C.; Sorițău, O.; Saccomanno, M.; Milano, G.; Tomoata, G.; Cherchizan, D.; et al. Collagen Scaffold and Lipoaspirate Fluid-derived Stem Cells for the Treatment of Cartilage Defects in a Rabbit Model. Rev. Chim. 2018, 69, 515–520. [Google Scholar] [CrossRef]
- Lucaciu, O.; Apostu, D.; Mester, A.; Campian, R.S.; Gheban, D.; Miron, R.J. Atelo-collagen type I bovine bone substitute and membrane in guided bone regeneration: A series of clinical cases and histopathological assessments. Histol. Histopathol. 2019, 18108. [Google Scholar] [CrossRef]
- Benea, H.; Tomoaia, G.; Soritau, O.; Pasca, R.D. A review on the reconstruction of articular cartilage using collagen scaffolds. Rom. Biotech. Lett. 2016, 21, 11735–11742. [Google Scholar]
- Armencea, G.; Cosma, C.; Dinu, C.; Onisor, F.; Lazar, M.; Berce, P.; Balc, N.; Baciut, M.; Bran, S. Technical queries of a 3D design custom-made implant made from titanium particles for maxillofacial bone reconstruction. Part. Sci. Technol. 2019, 38, 676–684. [Google Scholar] [CrossRef]
- Horbert, V.; Lange, M.; Reuter, T.; Hoffmann, M.; Bischoff, S.; Borowski, J.; Schubert, H.; Driesch, D.; Mika, J.; Hurschler, C.; et al. Comparison of Near-Infrared Spectroscopy with Needle Indentation and Histology for the Determination of Cartilage Thickness in the Large Animal Model Sheep. Cartilage 2017, 10, 173–185. [Google Scholar] [CrossRef] [PubMed]
- Armstrong, S.J.; Read, R.A.; Price, R. Topographical variation within the articular cartilage and subchondral bone of the normal ovine knee joint: A histological approach. Osteoarthr. Cartil. 1995, 3, 25–33. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Knox, P.; Levick, J.R.; McDonald, J.N. Synovial fluid-its mass, macromolecular content and pressure in major limb joints of the rabbit. Q. J. Exp. Physiol. 1988, 73, 33–45. [Google Scholar] [CrossRef]
- Mansour, J.M. Biomechanics of cartilage. Kinesiol. Mech. Pathomech. Hum. Mov. 2003, 2, 66–79. [Google Scholar]
- Benea, H. Modern Therapeutic Approaches for Repair of Articular Cartilage Lesions. Ph.D. Thesis, Iuliu Hațieganu University of Medicine and Pharmacy, Cluj-Napoca, Romania, 2017. [Google Scholar]
- Shoulders, M.D.; Raines, R.T. Collagen Structure and Stability. Annu. Rev. Biochem. 2009, 78, 929–958. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wenger, M.P.; Bozec, L.; Horton, M.A.; Mesquida, P. Mechanical properties of collagen fibrils. Biophys. J. 2007, 93, 1255–1263. [Google Scholar] [CrossRef] [Green Version]
- Bandyopadhyay-Ghosh, S. Bone as a Collagen-hydroxyapatite Composite and its Repair. Trends Biomater. Artif. Organs 2008, 22, 116–124. [Google Scholar] [CrossRef] [Green Version]
- Campos, D.F.D.; Drescher, W.; Rath, B.; Tingart, M.; Fischer, H. Supporting Biomaterials for Articular Cartilage Repair. Cartilage 2012, 3, 205–221. [Google Scholar] [CrossRef] [Green Version]
- Pearce, A.I.; Richards, R.G.; Milz, S.; Schneider, E.; Pearce, S.G. Animal models for implant biomaterial research in bone: A review. Eur. Cells Mater. 2007, 13, 1–10. [Google Scholar] [CrossRef]
- Zhao, Y.; Wang, W.; Xin, H.; Zang, S.; Zhang, Z.; Wu, Y. The remodeling of alveolar bone supporting the mandibular first molar with different levels of periodontal attachment. Med. Biol. Eng. Comput. 2013, 51, 991–997. [Google Scholar] [CrossRef] [PubMed]
- Tanaka, K.; Tanimoto, Y.; Kita, Y.; Enoki, S.; Katayama, T. The Effects of Trabecular Bone Microstructure on Compression Property of Bovine Cancellous Bone. Key Eng. Mater. 2011, 452–453, 297–300. [Google Scholar] [CrossRef]
- Cakan, U.; Saygılı, G. Comparison of thermal stress on various restorative post and core materials generated by oral temperature changes using three dimensional finite element analysis. Clin. Dent. Res. 2015, 39, 27–35. [Google Scholar]
- Değer, Y.; Adigüzel, Ö.; Özer, S.Y.; Kaya, S.; Polat, Z.; Bozyel, B. Evaluation of Temperature and Stress Distribution on 2 Different Post Systems Using 3-Dimensional Finite Element Analysis. Med. Sci. Monit. 2015, 21, 3716–3721. [Google Scholar] [CrossRef] [Green Version]
- Pal, S. Mechanical Properties of Biological Materials. In Design of Artificial Human Joints & Organs; Spinger: New York, NY, USA, 2014; pp. 23–40. [Google Scholar] [CrossRef]
- Szabelska, A.; Tatara, M.R.; Krupski, W. Morphological, densitometric and mechanical properties of mandible in 5-month-old Polish Merino sheep. BMC Vet. Res. 2017, 13, 12. [Google Scholar] [CrossRef] [Green Version]
- Li, B.; Aspden, R.M. Mechanical and material properties of the subchondral bone plate from the femoral head of patients with osteoarthritis or osteoporosis. Ann. Rheum. Dis. 1997, 56, 247–254. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cheng, C.K.; Lai, Y.S.; Sun, S.S.; Shen, H.W.; Yang, C.T.; Wei, H.W. Mechanical Property of Trabecular Bone of the Femoral Heads from Osteoarthritis and Osteoporosis Patients. In Advanced Bioimaging Technologies in Assessment of the Quality of Bone and Scaffold Materials; Springer: Berlin, Germany, 2007; pp. 673–690. [Google Scholar] [CrossRef]
- Homicz, M.R.; McGowan, K.B.; Lottman, L.M.; Beh, G.; Sah, R.L.; Watson, D. A compositional analysis of human nasal septal cartilage. Arch. Fac. Plast. Surg. 2003, 5, 53–58. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Fan, Y.; Zhang, M. Comparison of stress on knee cartilage during kneeling and standing using finite element models. Med. Eng. Phys. 2014, 36, 439–447. [Google Scholar] [CrossRef] [PubMed]
- Pauken, C.M.; Heyes, R.; Lott, D.G. Mechanical, Cellular, and Proteomic Properties of Laryngotracheal Cartilage. Cartilage 2018, 10, 321–328. [Google Scholar] [CrossRef]
- Moghadam, M.N.; Abdel-Sayed, P.; Camine, V.M.; Pioletti, D.P. Impact of synovial fluid flow on temperature regulation in knee cartilage. J. Biomech. 2015, 48, 370–374. [Google Scholar] [CrossRef] [Green Version]
- Vickers, S.M.; Gotterbarm, T.; Spector, M. Cross-Linking Affects Cellular Condensation and Chondrogenesis in Type II Collagen-GAG Scaffolds Seeded with Bone Marrow-Derived Mesenchymal Stem Cells. J. Orthop. Res. 2010, 28, 1184–1192. [Google Scholar] [CrossRef] [PubMed]
- Barkaoui, A.; Hambli, R. Nanomechanical properties of mineralised collagen microfibrils based on finite elements method: Biomechanical role of cross-links. Comput. Methods Biomech. Biomed. Eng. 2014, 17, 1590–1601. [Google Scholar] [CrossRef] [PubMed]
- Sang, J.; Li, X.; Shao, Y.; Li, Z.; Fu, J. Controlled Tubular Unit Formation from Collagen Film for Modular Tissue Engineering. ACS Biomater. Sci. Eng. 2017, 3, 2860–2868. [Google Scholar] [CrossRef] [PubMed]
- Bhattacharya, A.; Mahajan, L. Temperature dependence of thermal conductivity of biological tissues. Physiol. Meas. 2003, 24, 769–783. [Google Scholar] [CrossRef]
- Brand, R.A. Joint Contact Stress: A Reasonable Surrogate For Biological Processes? Iowa Orthop. J. 2005, 25, 82–94. [Google Scholar] [PubMed]
- Moran, C.J.; Ramesh, A.; Brama, P.A.; O’Byrne, J.M.; O’Brien, F.J.; Levingstone, T.J. The benefits and limitations of animal models for translational research in cartilage repair. J. Exp. Orthop. 2016, 3, 1. [Google Scholar] [CrossRef] [Green Version]
- Taylor, W.R.; Poepplau, B.M.; König, C.; Ehrig, R.M.; Zachow, S.; Duda, G.N.; Heller, M.O. The medial-lateral force distribution in the ovine stifle joint during walking. J. Orthop. Res. 2011, 29, 567–571. [Google Scholar] [CrossRef] [Green Version]
- Becher, C.; Springer, J.; Feil, S.; Cerulli, G.; Paessler, H.H. Intra-articular temperatures of the knee in sports—An in-vivo study of jogging and alpine skiing. BMC Musculoskelet. Disord. 2008, 9, 46. [Google Scholar] [CrossRef] [Green Version]
- Ozturk, H.E.; Stoffel, K.K.; Jones, C.F.; Stachowiak, G.W. The Effect of Surface-Active Phospholipids on the Lubrication of Osteoarthritic Sheep Knee Joints: Friction. Tribol. Lett. 2004, 16, 283–289. [Google Scholar] [CrossRef]
- Waldman, S.D.; Couto, D.C.; Grynpas, M.D.; Pilliar, R.M.; Kandel, R.A. A single application of cyclic loading can accelerate matrix deposition and enhance the properties of tissue-engineered cartilage. OsteoArthritis Cartil. 2006, 14, 323–330. [Google Scholar] [CrossRef] [Green Version]
- Ispas, A.; Cosma, C.; Craciun, A.; Constantiniuc, M.; Lascu, L.; Leordean, D.; Vilau, C. Influence of Ti-Ceramic or Ti-Composite crown on stress distribution: Finite element study and additive manufacturing. J. Optoelectron. Adv. Mater. 2016, 18, 904–912. [Google Scholar]
- Kon, E.; Filardo, G.; Di Matteo, B.; Perdisa, F.; Marcacci, M. Matrix assisted autologous chondrocyte transplantation for cartilage treatment: A systematic review. Bone Jt. Res. 2013, 2, 18–25. [Google Scholar] [CrossRef]
- Gobbi, A.; Karnatzikos, G.; Mahajan, V. Mesenchymal stem cells: Clinical research. ICRS Newslett. Winter 2012, 12, 41–42. [Google Scholar]
- Rai, V.; Dilisio, M.F.; Dietz, N.E.; Agrawal, D.K. Recent Strategies in Cartilage Repair: A Systemic Review of the Scaffold Development and Tissue Engineering. J. Biomed. Mater. Res. A 2017, 105, 2343–2354. [Google Scholar] [CrossRef] [PubMed]
- Hao, T.; Wen, N.; Cao, J.K.; Wang, H.B.; Lü, S.H.; Liu, T.; Lin, Q.X.; Duan, C.M.; Wang, C.Y. The support of matrix accumulation and the promotion of sheep articular cartilage defects repair in vivo by chitosan hydrogels. Osteoarthr. Cartil. 2010, 18, 257–265. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chan, D.D.; Neu, C.P.; Hull, M.L. In situ deformation of cartilage in cyclically loaded tibiofemoral joints by displacement-encoded MRI. Osteoarthr. Cartil. 2009, 17, 1461–1468. [Google Scholar] [CrossRef] [Green Version]
- Haidar, Z.S.; Hamdy, R.C.; Tabrizian, M. Delivery of recombinant bone morphogenetic proteins for bone regeneration and repair. Part A: Current challenges in BMP delivery. Biotechnol. Lett. 2009, 31, 1817–1824. [Google Scholar] [CrossRef] [PubMed]
- Monkova, K.; Vasina, M.; Monka, P.P.; Kozak, D.; Vanca, J. Effect of the Pore Shape and Size of 3D-Printed Open-Porous ABS Materials on Sound Absorption Performance. Materials 2020, 13, 4474. [Google Scholar] [CrossRef]
- Birleanu, C.; Pustan, M.; Müller, R.; Dudescu, C.; Merie, V.; Voicu, R.; Baracu, A. Experimental investigation by atomic force microscopy on mechanical and tribological properties of thin films. Int. J. Mater. Res. 2016, 107, 429–438. [Google Scholar] [CrossRef]
- Zawadzki, P.; Talar, R.; Patalas, A.; Legutko, S. Influence of Machining Parameters on Cutting and Chip-Formation Process during Cortical Bone Orthogonal Machining. Materials 2022, 15, 6414. [Google Scholar] [CrossRef]
- Park, Y.; Huh, K.M.; Kang, S.-W. Applications of Biomaterials in 3D Cell Culture and Contributions of 3D Cell Culture to Drug Development and Basic Biomedical Research. Int. J. Mol. Sci. 2021, 22, 2491. [Google Scholar] [CrossRef]
- Dorozhkin, S.V. Calcium Orthophosphate (CaPO4)-Based Bioceramics: Preparation, Properties, and Applications. Coatings 2022, 12, 1380. [Google Scholar] [CrossRef]
- Caballé-Serrano, J.; Zhang, S.; Sculean, A.; Staehli, A.; Bosshardt, D.D. Tissue Integration and Degradation of a Porous Collagen-Based Scaffold Used for Soft Tissue Augmentation. Materials 2020, 13, 2420. [Google Scholar] [CrossRef] [PubMed]
- Suethao, S.; Phongphanphanee, S.; Wong-ekkabut, J.; Smitthipong, W. The Relationship between the Morphology and Elasticity of Natural Rubber Foam Based on the Concentration of the Chemical Blowing Agent. Polymers 2021, 13, 1091. [Google Scholar] [CrossRef] [PubMed]
- Raj, R.; Dixit, A.R.; Łukaszewski, K.; Wichniarek, R.; Rybarczyk, J.; Kuczko, W.; Górski, F. Numerical and Experimental Mechanical Analysis of Additively Manufactured Ankle–Foot Orthoses. Materials 2022, 15, 6130. [Google Scholar] [CrossRef]









| Knee Tissue | Compression Pressure Applied [MPa] | Case 0 (Healthy) | Case 1 | Case 2 | Case 3 | Compression Strength Limit of Tissue [MPa] |
|---|---|---|---|---|---|---|
| Femoral cartilage | 0.38 | under 1 | 1 | 1 | 1 | 5–20 |
| 0.76 | 4.2 | 2.2 | 3.1 | 3.2 | ||
| Tibial cartilage | 0.38 | under 1 | 2.1 | 2.3 | 2.6 | |
| 0.76 | 2.0 | 4.6 | 3.8 | 3.5 | ||
| UC | 0.38 | N/A | 7.8 | 12.7 | 15.6 | 5–100 |
| 0.76 | N/A | 25.3 | 22.9 | 18.8 | ||
| Femoral subchondral bone | 0.38 | 5.3 | 5.6 | 9.7 | 11.6 | 64 |
| 0.76 | 16.2 | 14.3 | 12.4 | 15.2 | ||
| Tibial subchondral bone | 0.38 | 2.1 | 3.6 | 1.2 | 3.4 | |
| 0.76 | 5.3 | 5.8 | 5.6 | 5.9 | ||
| Femoral trabecular bone | 0.38 | under 1 | 2.8 | 2.5 | 2.6 | 2–16 |
| 0.76 | 3.4 | 5.2 * | 3.6 | 5.8 * |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cosma, C.; Apostu, D.; Vilau, C.; Popan, A.; Oltean-Dan, D.; Balc, N.; Tomoaie, G.; Benea, H. Finite Element Analysis of Different Osseocartilaginous Reconstruction Techniques in Animal Model Knees. Materials 2023, 16, 2546. https://doi.org/10.3390/ma16072546
Cosma C, Apostu D, Vilau C, Popan A, Oltean-Dan D, Balc N, Tomoaie G, Benea H. Finite Element Analysis of Different Osseocartilaginous Reconstruction Techniques in Animal Model Knees. Materials. 2023; 16(7):2546. https://doi.org/10.3390/ma16072546
Chicago/Turabian StyleCosma, Cosmin, Dragos Apostu, Cristian Vilau, Alexandru Popan, Daniel Oltean-Dan, Nicolae Balc, Gheorghe Tomoaie, and Horea Benea. 2023. "Finite Element Analysis of Different Osseocartilaginous Reconstruction Techniques in Animal Model Knees" Materials 16, no. 7: 2546. https://doi.org/10.3390/ma16072546