
In Vitro Comparison of Internal and Marginal Adaptation between Printed and Milled Onlays
 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
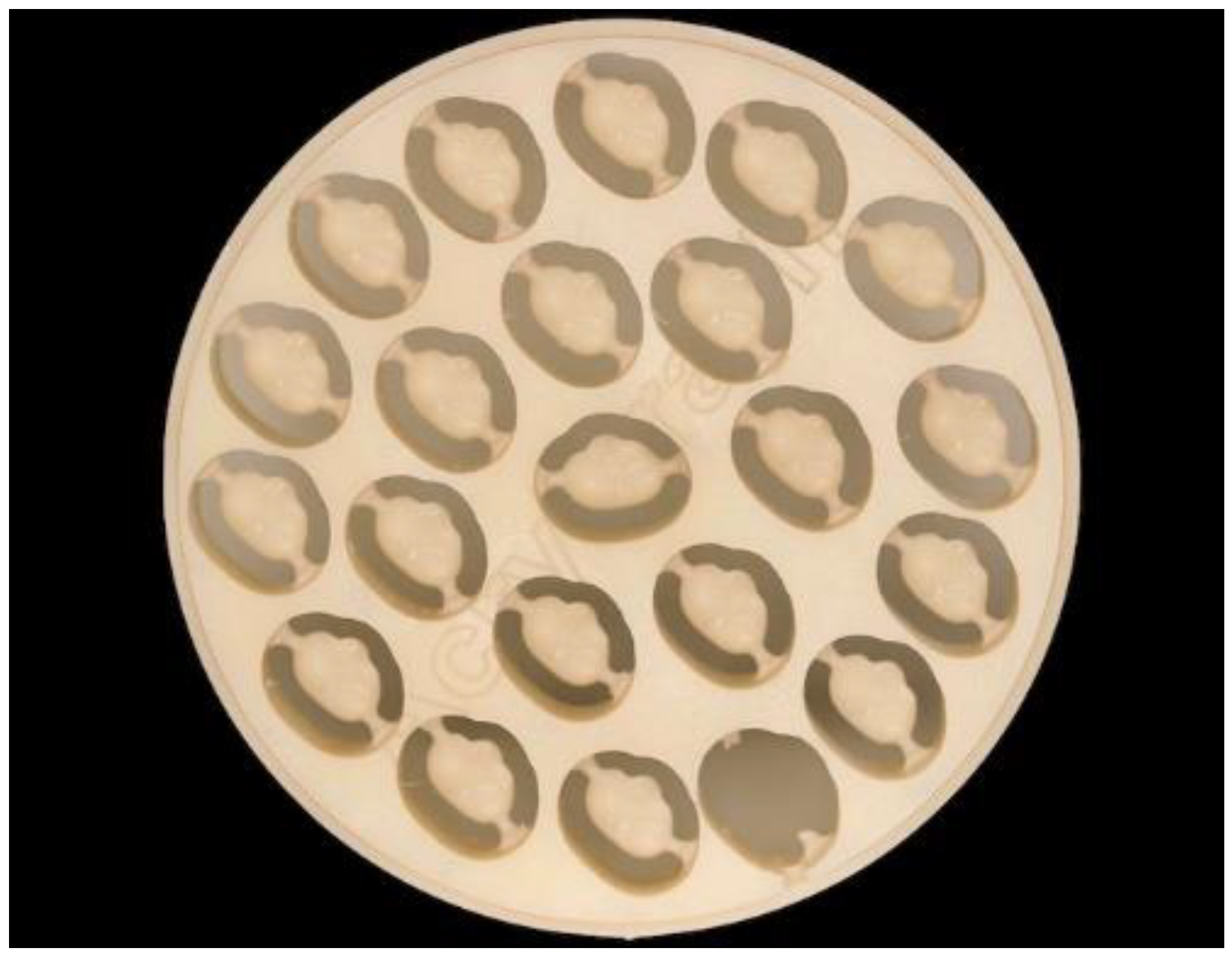
2.1. Sample Preparation
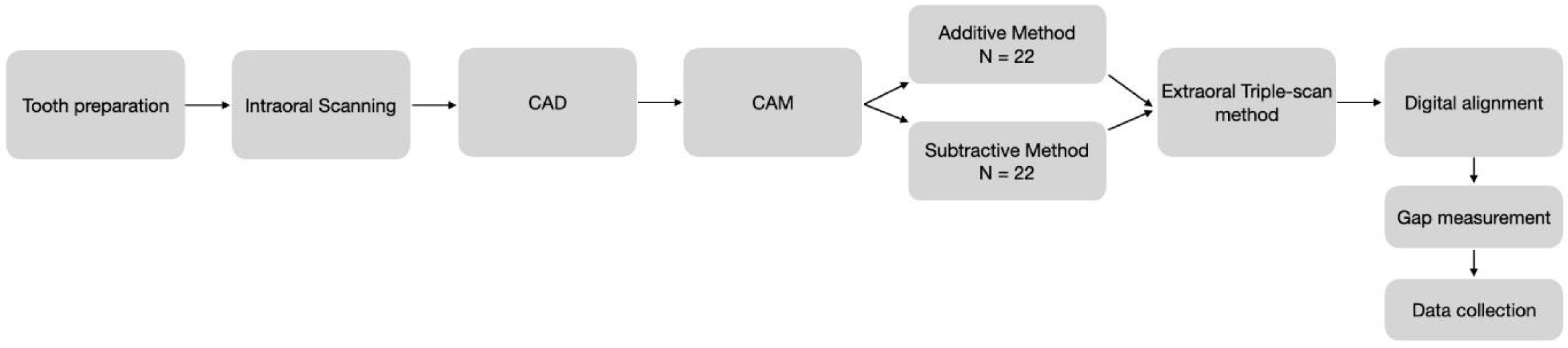
2.2. Sample Manufacturing
2.3. Digitalization of Samples
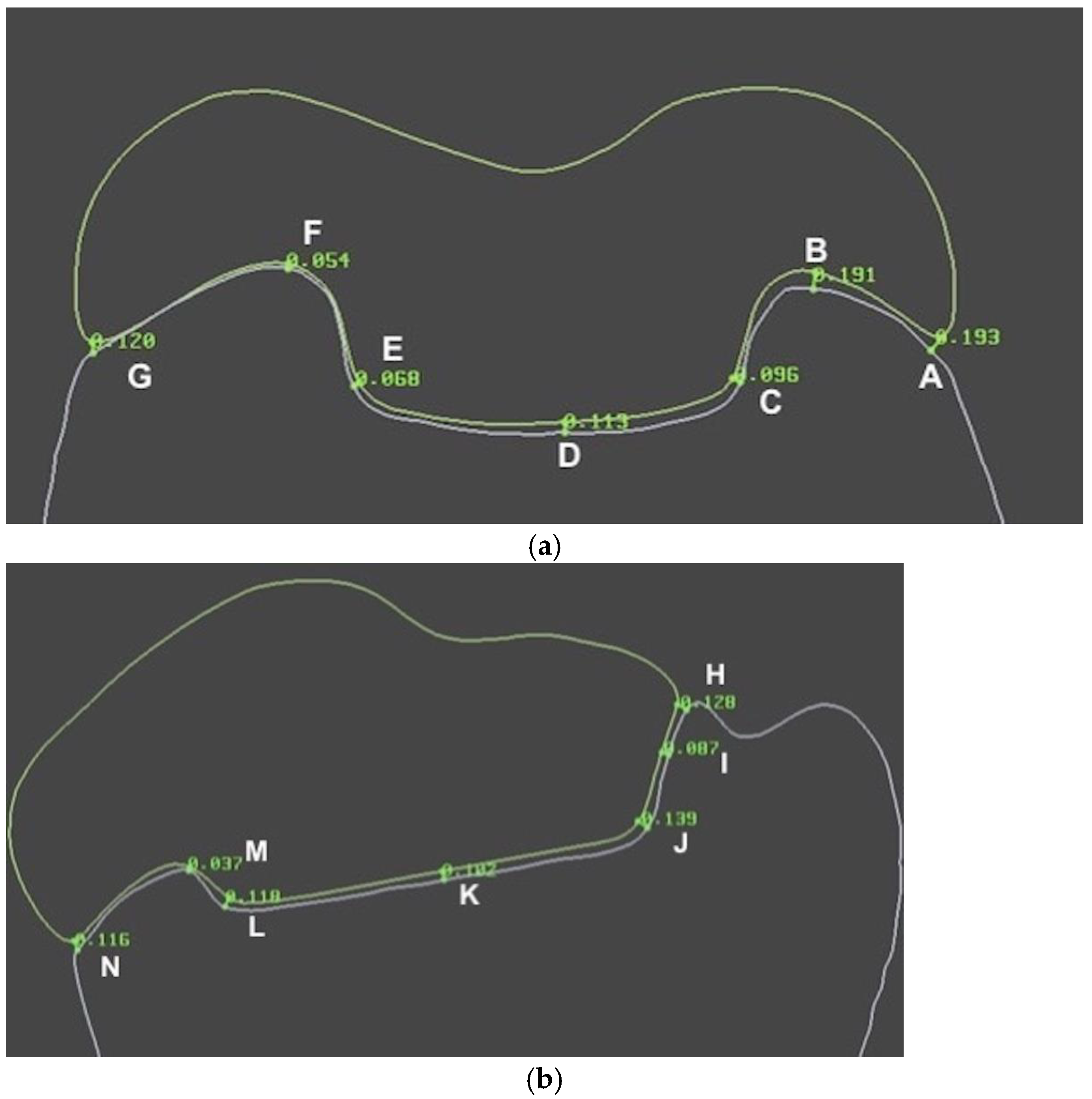
2.4. Evaluation of Adaptation
2.5. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
- The printed onlays adapt significantly better to the prepared tooth than milled onlays.
- A significantly higher gap reproducibility within the group of the printed onlays was demonstrated.
- Further research is needed to determine intraorally printed restorations’ longevity and long-term behavior.
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Bustamante-Hernández, N.; Montiel-Company, J.M.; Bellot-Arcís, C.; Mañes-Ferrer, J.F.; Solá-Ruíz, M.F.; Agustín-Panadero, R.; Fernández-Estevan, L. Clinical Behavior of Ceramic, Hybrid and Composite Onlays. A Systematic Review and Meta-Analysis. Int. J. Environ. Res. Public Health 2020, 17, 7582. [Google Scholar] [CrossRef] [PubMed]
- da Veiga, A.M.; Cunha, A.C.; Ferreira, D.M.; da Silva Fidalgo, T.K.; Chianca, T.K.; Reis, K.R.; Maia, L.C. Longevity of Direct and Indirect Resin Composite Restorations in Permanent Posterior Teeth: A systematic review and meta-analysis. J. Dent. 2016, 54, 1. [Google Scholar] [CrossRef]
- Opdam, N.J.; van de Sande, F.H.; Bronkhorst, E.; Cenci, M.S.; Bottenberg, P.; Pallesen, U.; Gaengler, P.; Lindberg, A.; Huysmans, M.C.; van Dijken, J.W. Longevity of Posterior Composite Restorations. J. Dent. Res. 2014, 93, 943. [Google Scholar] [CrossRef] [PubMed]
- Joda, T.; Zarone, F.; Ferrari, M. The Complete Digital Workflow in Fixed Prosthodontics: A Systematic Review. BMC Oral Health 2017, 17, 124. [Google Scholar] [CrossRef]
- Kalberer, N.; Mehl, A.; Schimmel, M.; Müller, F.; Srinivasan, M. CAD-CAM Milled Versus Rapidly Prototyped (3D-printed) Complete Dentures: An in vitro evaluation of trueness. J. Prosthet. Dent. 2019, 121, 637. [Google Scholar] [CrossRef] [PubMed]
- Mangano, F.; Gandolfi, A.; Luongo, G.; Logozzo, S. Intraoral Scanners in Dentistry: A Review of the Current Literature. BMC Oral Health 2017, 17, 149. [Google Scholar] [CrossRef]
- Stanley, M.; Paz, A.G.; Miguel, I.; Coachman, C. Fully Digital Workflow, Integrating Dental Scan, Smile Design and CAD-CAM: Case Report. BMC Oral Health 2018, 18, 134. [Google Scholar] [CrossRef]
- Bae, E.; Jeong, I.; Kim, W.; Kim, J. A Comparative Study of Additive and Subtractive Manufacturing for Dental Restorations. J. Prosthet. Dent. 2017, 118, 187. [Google Scholar] [CrossRef] [PubMed]
- Haddadi, Y.; Ranjkesh, B.; Isidor, F.; Bahrami, G. Marginal and Internal Fit of Crowns Based on Additive or Subtractive Manufacturing. Biomater. Investig. Dent. 2021, 8, 87. [Google Scholar] [CrossRef] [PubMed]
- Karasan, D.; Legaz, J.; Boitelle, P.; Mojon, P.; Fehmer, V.; Sailer, I. Accuracy of Additively Manufactured and Milled Interim 3-Unit Fixed Dental Prostheses. J. Prosthodont. 2022, 31, 58. [Google Scholar] [CrossRef]
- Kakinuma, H.; Izumita, K.; Yoda, N.; Egusa, H.; Sasaki, K. Comparison of the Accuracy of Resin-composite Crowns Fabricated by Three-dimensional Printing and Milling Methods. Dent. Mater. J. 2022, 41, 808. [Google Scholar] [CrossRef]
- Ruse, N.D.; Sadoun, M.J. Resin-composite Blocks for Dental CAD/CAM Applications. J. Dent. Res. 2014, 93, 1232. [Google Scholar] [CrossRef]
- Ge, Z.; Yang, L.; Xiao, F.; Wu, Y.; Yu, T.; Chen, J.; Lin, J.; Zhang, Y. Graphene Family Nanomaterials: Properties and Potential Applications in Dentistry. Int. J. Biomater. 2018, 2018, 1539678. [Google Scholar] [CrossRef]
- Li, X.; Liang, X.; Wang, Y.; Wang, D.; Teng, M.; Xu, H.; Zhao, B.; Han, L. Graphene-Based Nanomaterials for Dental Applications: Principles, Current Advances, and Future Outlook. Front. Bioeng. Biotechnol. 2022, 10, 804201. [Google Scholar] [CrossRef] [PubMed]
- Selva-Otaolaurruchi, E.J.; Fernández-Estevan, L.; Solá-Ruiz, M.F.; García-Sala-Bonmati, F.; Selva-Ribera, I.; Agustín-Panadero, R. Graphene-Doped Polymethyl Methacrylate (PMMA) as a New Restorative Material in Implant-Prosthetics: In Vitro Analysis of Resistance to Mechanical Fatigue. J. Clin. Med. 2023, 12, 1269. [Google Scholar] [CrossRef] [PubMed]
- Di Carlo, S.; De Angelis, F.; Brauner, E.; Pranno, N.; Tassi, G.; Senatore, M.; Bossù, M. Flexural Strength and Elastic Modulus Evaluation of Structures Made by Conventional PMMA and PMMA Reinforced with Graphene. Eur. Rev. Med. Pharmacol. Sci. 2020, 24, 5201. [Google Scholar] [PubMed]
- Tahriri, M.; Del Monico, M.; Moghanian, A.; Tavakkoli Yaraki, M.; Torres, R.; Yadegari, A.; Tayebi, L. Graphene and Its Derivatives: Opportunities and Challenges in Dentistry. Mater. Sci. Eng. C 2019, 102, 171. [Google Scholar] [CrossRef] [PubMed]
- Azevedo, L.; Antonaya-Martin, J.L.; Molinero-Mourelle, P.; Del Río-Highsmith, J. Improving PMMA Resin Using Graphene Oxide for a Definitive Prosthodontic Rehabilitation—A Clinical Report. J. Clin. Exp. Dent. 2019, 11, e670–e674. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.; Jo, J.; Kim, D.; Patel, K.D.; Kim, H.; Lee, H. Nano-graphene Oxide Incorporated into PMMA Resin to Prevent Microbial Adhesion. Dent. Mater. 2018, 34, e63–e72. [Google Scholar] [CrossRef] [PubMed]
- Bacali, C.; Badea, M.; Moldovan, M.; Sarosi, C.; Nastase, V.; Baldea, I.; Chiorean, R.S.; Constantiniuc, M. The Influence of Graphene in Improvement of Physico-Mechanical Properties in PMMA Denture Base Resins. Materials 2019, 12, 2335. [Google Scholar] [CrossRef] [PubMed]
- Lerner, H.; Nagy, K.; Pranno, N.; Zarone, F.; Admakin, O.; Mangano, F. Trueness and Precision of 3D-printed Versus Milled Monolithic Zirconia Crowns: An in vitro study. J. Dent. 2021, 113, 103792. [Google Scholar] [CrossRef]
- Tian, Y.; Chen, C.; Xu, X.; Wang, J.; Hou, X.; Li, K.; Lu, X.; Shi, H.; Lee, E.S.; Jiang, H.B. A Review of 3D Printing in Dentistry: Technologies, Affecting Factors, and Applications. Scanning 2021, 2021, 1. [Google Scholar] [CrossRef]
- Katreva, I.; Dikova, T.; Abadzhiev, M.; Tonchev, T.; Dzhendov, D.; Simov, M.; Angelova, S.; Pavlova, D.; Doychinova, M. 3D-printing in Contemporary Prosthodontic Treatment. Scr. Sci. Med. Dent. 2016, 2, 7. [Google Scholar] [CrossRef]
- Della Bona, A.; Cantelli, V.; Britto, V.T.; Collares, K.F.; Stansbury, J.W. 3D Printing Restorative Materials Using a Stereolithographic Technique: A Systematic Review. Dent. Mater. 2021, 37, 336. [Google Scholar] [CrossRef]
- Schweiger, J.; Edelhoff, D.; Güth, J. 3D Printing in Digital Prosthetic Dentistry: An Overview of Recent Developments in Additive Manufacturing. J. Clin. Med. 2021, 10, 2010. [Google Scholar] [CrossRef] [PubMed]
- Vichi, A.; Balestra, D.; Scotti, N.; Louca, C.; Paolone, G. Translucency of CAD/CAM and 3D Printable Composite Materials for Permanent Dental Restorations. Polymers 2023, 15, 1443. [Google Scholar] [CrossRef] [PubMed]
- García-Cuesta, C.; Faus-Llácer, V.; Zubizarreta-Macho, Á.; Botello-Torres, R.; Faus-Matoses, V. A Comparison of the Marginal Adaptation of Composite Overlays Fabricated with Silicone and an Intraoral Scanner. J. Clin. Exp. Dent. 2021, 13, e473–e478. [Google Scholar] [CrossRef]
- Kim, K.; Kim, J.; Kim, W.; Kim, J. Three-dimensional Evaluation of Gaps Associated with Fixed Dental Prostheses Fabricated with New Technologies. J. Prosthet. Dent. 2014, 112, 1432. [Google Scholar] [CrossRef]
- Patel, T.; Nathwani, N.; Fine, P.; Leung, A. A Scoping Review of Marginal and Internal Fit Accuracy of Lithium Disilicate Restorations. Dent. J. 2022, 10, 236. [Google Scholar] [CrossRef]
- Hasanzade, M.; Koulivand, S.; Moslemian, N.; Alikhasi, M. Comparison of Three-dimensional Digital Technique with Two-dimensional Replica Method for Measuring Marginal and Internal Fit of Full Coverage Restorations. J. Adv. Prosthodont. 2020, 12, 173. [Google Scholar] [CrossRef] [PubMed]












{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Product Name | Manufacturer | City/State/Country | Shade | Composition | Lot Number |
|---|---|---|---|---|---|
| Permanent Crown Resin | Bego | Bremen, Germany | A2 | Esterification products of 4,4’-isopropylidene diphenol (ethoxylated), 2-methylprop-2-enoic acid, silanized dental glass, methyl benzoyl formate, and diphenyl (2,4,6-trimethylbenzoyl) phosphine oxide. Total proportion of inorganic fillers (particle size 0.7 μm) is 30–50% by mass | 600,926 |
| Acrylgraph | Nuprodent | Soneja, Spain | A3 | Poly(methyl methacrylate)+ Graphene | 3 February 2020 |
| Source | Sum of Squares | Df | Mean Square | F-Ratio | p-Value |
|---|---|---|---|---|---|
| MAIN EFFECTS | |||||
| A: Type | 227,327 | 1 | 227,327 | 82.01 | 0.0000 |
| B: Location | 54,414.4 | 2 | 27,207.2 | 9.82 | 0.0001 |
| INTERACTIONS | |||||
| AB | 15,310.6 | 2 | 7655.28 | 2.76 | 0.0670 |
| RESIDUAL | 349,251 | 126 | 2771.83 | ||
| TOTAL (CORRECTED) | 646,303 | 131 |
| 1. Marginal GAP | 2. Inner GAP | 3. Central GAP | p* | |
|---|---|---|---|---|
| Milled (G1) | 216.90 ± 107.45 | 160.57 ± 67.72 | 225.73 ± 11.31 | <0.05 (1–2, 2–3) |
| Printed (G2) | 137.86 ± 41.33 | 101.74 ± 58.98 | 114.60 ± 6.62 | >0.05 |
| p* | <0.05 | <0.05 | <0.05 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cantó-Navés, O.; Michels, K.; Figueras-Alvarez, O.; Fernández-Villar, S.; Cabratosa-Termes, J.; Roig, M. In Vitro Comparison of Internal and Marginal Adaptation between Printed and Milled Onlays. Materials 2023, 16, 6962. https://doi.org/10.3390/ma16216962
Cantó-Navés O, Michels K, Figueras-Alvarez O, Fernández-Villar S, Cabratosa-Termes J, Roig M. In Vitro Comparison of Internal and Marginal Adaptation between Printed and Milled Onlays. Materials. 2023; 16(21):6962. https://doi.org/10.3390/ma16216962
Chicago/Turabian StyleCantó-Navés, Oriol, Kyra Michels, Oscar Figueras-Alvarez, Sandra Fernández-Villar, Josep Cabratosa-Termes, and Miguel Roig. 2023. "In Vitro Comparison of Internal and Marginal Adaptation between Printed and Milled Onlays" Materials 16, no. 21: 6962. https://doi.org/10.3390/ma16216962