
Biocompatibility, Surface Morphology, and Bacterial Load of Dental Implant Abutments following Decontamination Protocols: An In-Vitro Study


Abstract
:1. Introduction
2. Materials and Methods
2.1. Titanium Abutment Preparation
- Surface analysis using scanning electron microscopy (SEM).
- XTT assay for cell viability and proliferation.
- Bacterial direct count of colony-forming units per milliliter (CFU/mL).
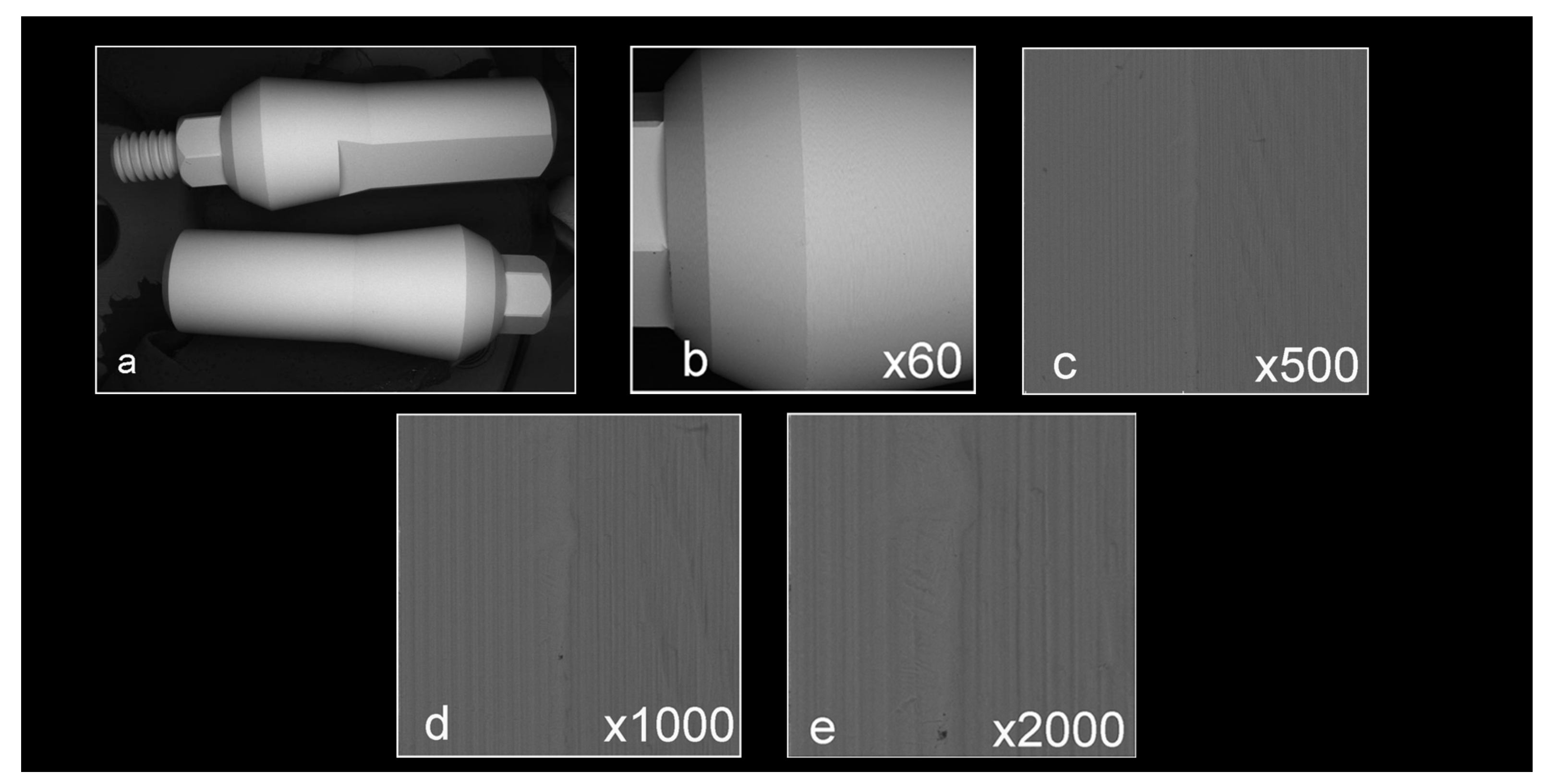
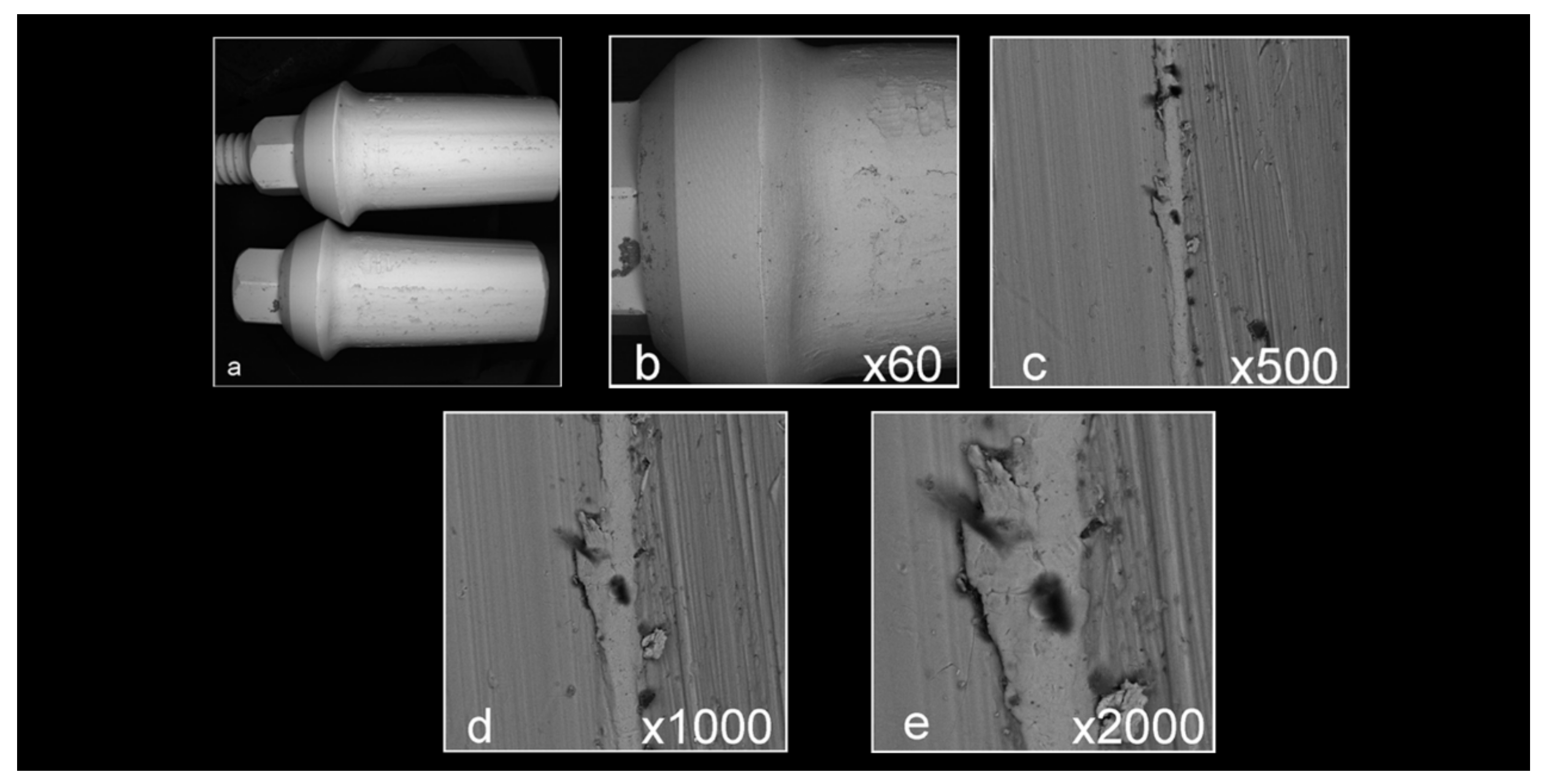
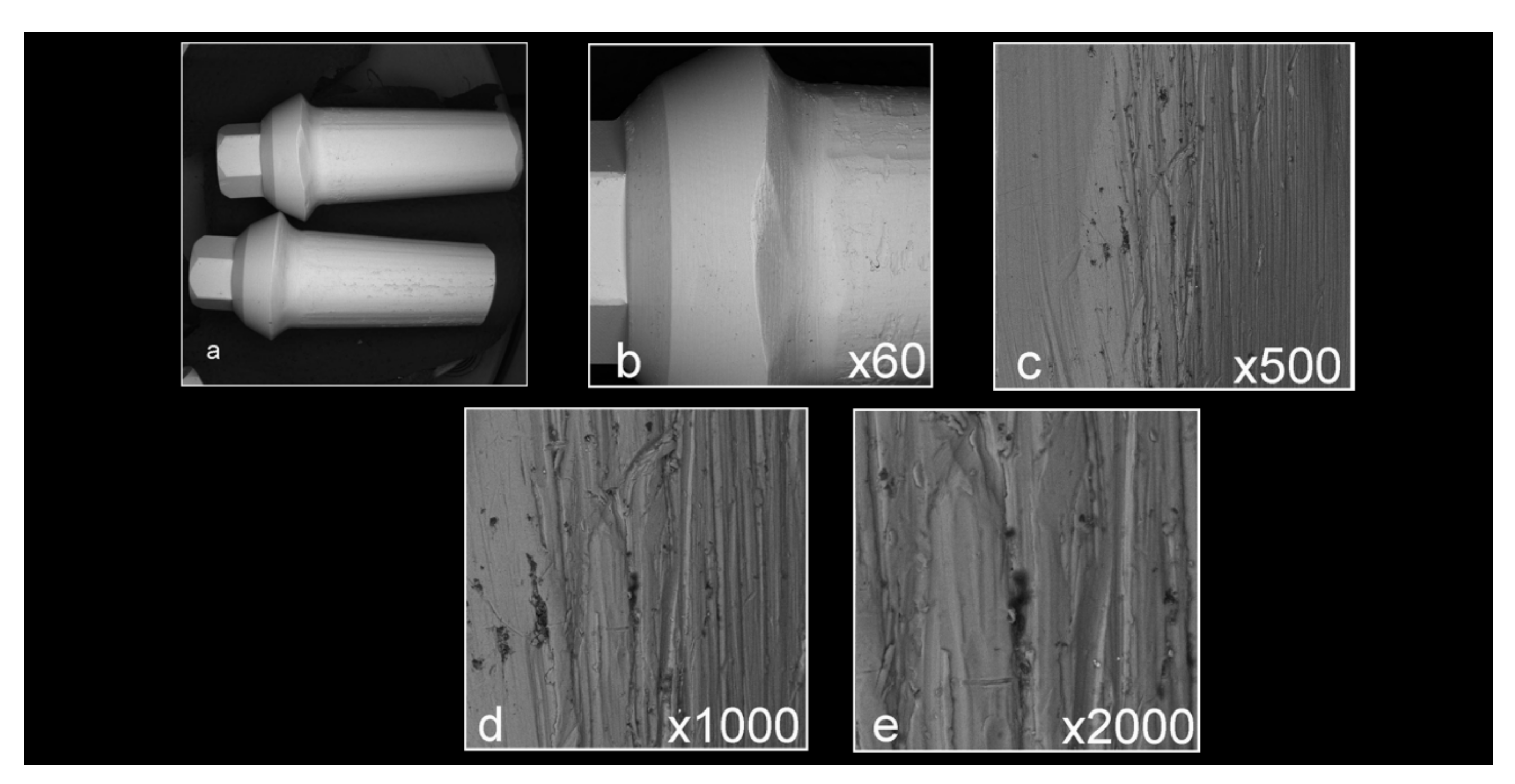
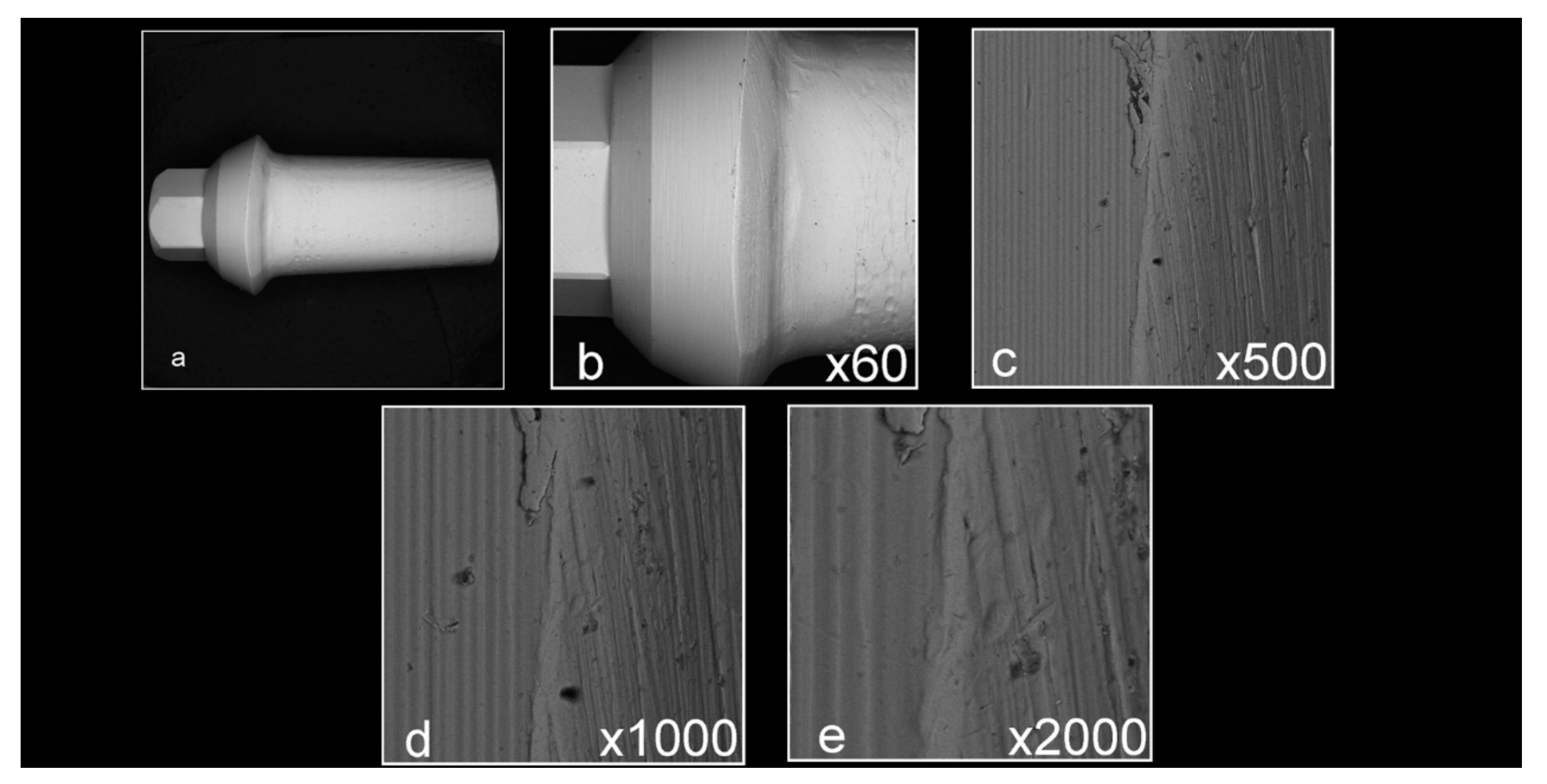
2.2. Surface Analysis by SEM
2.3. XTT Assay for Cell Viability and Proliferation
2.4. Bacterial Evaluation
2.5. Statistical Analysis
3. Results
3.1. Surface Analysis by Scanning Electron Microscopy (SEM)
3.2. XTT Assay for Cell Viability and Proliferation
3.3. Bacterial Evaluation
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Pjetursson, B.E.; Sailer, I.; Latyshev, A.; Rabel, K.; Kohal, R.J.; Karasan, D. A systematic review and meta-analysis evaluating the survival, the failure, and the complication rates of veneered and monolithic all-ceramic implant-supported single crowns. Clin. Oral Implants Res. 2021, 32 (Suppl. S21), 254–288. [Google Scholar] [CrossRef]
- Pjetursson, B.E.; Thoma, D.; Jung, R.; Zwahlen, M.; Zembic, A. A systematic review of the survival and complication rates of implant-supported fixed dental prostheses (FDPs) after a mean observation period of at least 5 years. Clin. Oral Implants Res. 2012, 23 (Suppl. S6), 22–38. [Google Scholar] [CrossRef] [PubMed]
- Jung, R.E.; Pjetursson, B.E.; Glauser, R.; Zembic, A.; Zwahlen, M.; Lang, N.P. A systematic review of the 5-year survival and complication rates of implant-supported single crowns. Clin. Oral Implants Res. 2008, 19, 119–130. [Google Scholar] [CrossRef] [PubMed]
- Jung, R.E.; Zembic, A.; Pjetursson, B.E.; Zwahlen, M.; Thoma, D.S. Systematic review of the survival rate and the incidence of biological, technical, and aesthetic complications of single crowns on implants reported in longitudinal studies with a mean follow-up of 5 years. Clin. Oral Implants Res. 2012, 23 (Suppl. S6), 2–21. [Google Scholar] [CrossRef]
- Welander, M.; Abrahamsson, I.; Berglundh, T. The mucosal barrier at implant abutments of different materials. Clin. Oral Implants Res. 2008, 19, 635–641. [Google Scholar]
- Esposito, M.; Grusovin, M.G.; Worthington, H.V. Interventions for replacing missing teeth: Treatment of peri-implantitis. Cochrane Database Syst. Rev. 2012, 1, Cd004970. [Google Scholar] [CrossRef]
- Schwarz, F.; Ramanauskaite, A. It is all about peri-implant tissue health. Periodontol 2000 2022, 88, 9–12. [Google Scholar] [CrossRef]
- Thoma, D.S.; Gil, A.; Hämmerle, C.H.F.; Jung, R.E. Management and prevention of soft tissue complications in implant dentistry. Periodontol 2000 2022, 88, 116–129. [Google Scholar] [CrossRef] [PubMed]
- Berglundh, T.; Lindhe, J.; Jonsson, K.; Ericsson, I. The topography of the vascular systems in the periodontal and peri-implant tissues in the dog. J. Clin. Periodontol. 1994, 21, 189–193. [Google Scholar] [CrossRef]
- Buser, D.; Weber, H.P.; Donath, K.; Fiorellini, J.P.; Paquette, D.W.; Williams, R.C. Soft tissue reactions to non-submerged unloaded titanium implants in beagle dogs. J. Periodontol. 1992, 63, 225–235. [Google Scholar] [CrossRef] [PubMed]
- Berglundh, T.; Lindhe, J.; Ericsson, I.; Marinello, C.P.; Liljenberg, B.; Thomsen, P. The soft tissue barrier at implants and teeth. Clin. Oral Implants Res. 1991, 2, 81–90. [Google Scholar] [CrossRef]
- Lindhe, J.; Berglundh, T. The interface between the mucosa and the implant. Periodontol 2000 1998, 17, 47–54. [Google Scholar] [CrossRef]
- Schwarz, F.; Derks, J.; Monje, A.; Wang, H.L. Peri-implantitis. J. Periodontol. 2018, 89 (Suppl. S1), S267–S290. [Google Scholar] [CrossRef] [PubMed]
- Park, J.M.; Lee, J.B.; Heo, S.J.; Park, E.J. A comparative study of gold UCLA-type and CAD/CAM titanium implant abutments. J. Adv. Prosthodont. 2014, 6, 46–52. [Google Scholar] [CrossRef]
- Smith, D.C. Dental implants: Materials and design considerations. Int. J. Prosthodont. 1993, 6, 106–117. [Google Scholar] [PubMed]
- Canullo, L.; Tallarico, M.; Chu, S.; Peñarrocha, D.; Özcan, M.; Pesce, P. Cleaning, Disinfection, and Sterilization Protocols Employed for Customized Implant Abutments: An International Survey of 100 Universities Worldwide. Int. J. Oral Maxillofac. Implants 2017, 32, 774–778. [Google Scholar] [CrossRef] [PubMed]
- Tamizifar, A.; Bahador, A.; Moharrami, M.; Rasouli-Ghahroudi, A.A.; Homayooni, A.; Alikhasi, M. Microflora of Laboratory-Customized Dental Implant Abutments. J. Int. Acad. Periodontol. 2018, 20, 86–93. [Google Scholar] [PubMed]
- Mishra, P.K.; Wu, W.; Rozo, C.; Hallab, N.J.; Benevenia, J.; Gause, W.C. Micrometer-sized titanium particles can induce potent Th2-type responses through TLR4-independent pathways. J. Immunol. 2011, 187, 6491–6498. [Google Scholar] [CrossRef]
- Furst, M.M.; Salvi, G.E.; Lang, N.P.; Persson, G.R. Bacterial colonization immediately after installation on oral titanium implants. Clin. Oral Implants Res. 2007, 18, 501–508. [Google Scholar] [CrossRef]
- Quirynen, M.; Bollen, C.M.; Papaioannou, W.; Van Eldere, J.; van Steenberghe, D. The influence of titanium abutment surface roughness on plaque accumulation and gingivitis: Short-term observations. Int. J. Oral Maxillofac. Implants 1996, 11, 169–178. [Google Scholar]
- Canullo, L.; Micarelli, C.; Lembo-Fazio, L.; Iannello, G.; Clementini, M. Microscopical and microbiologic characterization of customized titanium abutments after different cleaning procedures. Clin. Oral Implants Res. 2014, 25, 328–336. [Google Scholar] [CrossRef] [PubMed]
- Rompen, E.; Domken, O.; Degidi, M.; Pontes, A.E.; Piattelli, A. The effect of material characteristics, of surface topography and of implant components and connections on soft tissue integration: A literature review. Clin. Oral Implants Res. 2006, 17 (Suppl. S2), 55–67. [Google Scholar] [CrossRef]
- Asmarz, H.Y.; Magrin, G.L.; Prado, A.M.; Passoni, B.B.; Benfatti, C.A.M. Evaluation of Removal Torque and Internal Surface Alterations in Frictional Morse Taper Connections After Mechanical Loading Associated or Not with Oral Biofilm. Int. J. Oral Maxillofac. Implants 2021, 36, 492–501. [Google Scholar] [CrossRef] [PubMed]
- Canullo, L.; Tallarico, M.; Penarrocha, M.; Corrente, G.; Fiorellini, J.; Penarrocha, D. Plasma of Argon Cleaning Treatment on Implant Abutments in Periodontally Healthy Patients: Six Years Postloading Results of a Randomized Controlled Trial. Int. J. Periodont. Restor. Dent. 2017, 37, 683–690. [Google Scholar] [CrossRef]
- Kyaw, T.T.; Abdou, A.; Nakata, H.; Pimkhaokham, A. Dental implant healing abutment decontamination: A systematic review of in vitro studies. Int. J. Oral Implantol. 2022, 15, 311–324. [Google Scholar]
- Homayouni, A.; Bahador, A.; Moharrami, M.; Pourhajibagher, M.; Rasouli-Ghahroudi, A.A.; Alikhasi, M. Effect of 5 Popular Disinfection Methods on Microflora of Laboratory: Customized Implant Abutments. Implant. Dent. 2019, 28, 437–446. [Google Scholar] [CrossRef] [PubMed]
- Canullo, L.; Micarelli, C.; Iannello, G. Microscopical and chemical surface characterization of the gingival portion and connection of an internal hexagon abutment before and after different technical stages of preparation. Clin. Oral Implants Res. 2013, 24, 606–611. [Google Scholar] [CrossRef]
- Sanchez-Garces, M.A.; Jorba, M.; Ciurana, J.; Vinas, M.; Vinuesa, M.T. Is the re-use of sterilized implant abutments safe enough? (Implant abutment safety). Med. Oral Patol. Oral Cir. Bucal. 2019, 24, e583–e587. [Google Scholar] [CrossRef]
- Chew, M.; Tompkins, G.; Tawse-Smith, A.; Waddell, J.N.; Ma, S. Reusing Titanium Healing Abutments: Comparison of Two Decontamination Methods. Int. J. Prosthodont. 2018, 31, 613–618. [Google Scholar] [CrossRef]
- Gehrke, P.; Tabellion, A.; Fischer, C. Microscopical and chemical surface characterization of CAD/CAM zircona abutments after different cleaning procedures. A qualitative analysis. J. Adv. Prosthodont. 2015, 7, 151–159. [Google Scholar] [CrossRef]
- Mehl, C.; Kern, M.; Zimmermann, A.; Harder, S.; Huth, S.; Selhuber-Unkel, C. Impact of Cleaning Procedures on Adhesion of Living Cells to Three Abutment Materials. Int. J. Oral Maxillofac. Implants 2017, 32, 976–984. [Google Scholar] [CrossRef]
- Smith, K.C.A.; Oatley, C.W. The scanning electron microscope and its fields of application. Br. J. Appl. Phys. 1955, 6, 391–399. [Google Scholar] [CrossRef]
- Kuhn, D.M.; Balkis, M.; Chandra, J.; Mukherjee, P.K.; Ghannoum, M.A. Uses and limitations of the XTT assay in studies of Candida growth and metabolism. J. Clin. Microbiol. 2003, 41, 506–508. [Google Scholar] [CrossRef] [PubMed]
- Roehm, N.W.; Rodgers, G.H.; Hatfield, S.M.; Glasebrook, A.L. An improved colorimetric assay for cell proliferation and viability utilizing the tetrazolium salt XTT. J. Immunol. Methods 1991, 142, 257–265. [Google Scholar] [CrossRef] [PubMed]
- Scudiero, D.A.; Shoemaker, R.H.; Paull, K.D.; Monks, A.; Tierney, S.; Nofziger, T.H.; Currens, M.J.; Seniff, D.; Boyd, M.R. Evaluation of a soluble tetrazolium/formazan assay for cell growth and drug sensitivity in culture using human and other tumor cell lines. Cancer Res. 1988, 48, 4827–4833. [Google Scholar] [PubMed]
- Tuchscheerer, V.; Eickholz, P.; Dannewitz, B.; Ratka, C.; Zuhr, O.; Petsos, H. In vitro surgical and non-surgical air-polishing efficacy for implant surface decontamination in three different defect configurations. Clin. Oral Investig. 2021, 25, 1743–1754. [Google Scholar] [CrossRef]
- Ishiyama, M.; Tominaga, H.; Shiga, M.; Sasamoto, K.; Ohkura, Y.; Ueno, K. A combined assay of cell viability and in vitro cytotoxicity with a highly water-soluble tetrazolium salt, neutral red and crystal violet. Biol. Pharm. Bull. 1996, 19, 1518–1520. [Google Scholar] [CrossRef]
- Jervøe-Storm, P.M.; Hablützel, A.S.; Bartels, P.; Kraus, D.; Jepsen, S.; Enkling, N. Comparison of irrigation protocols for the internal decontamination of dental implants-results of in vitro and in vivo studies. Clin. Oral Implants Res. 2021, 32, 1168–1175. [Google Scholar] [CrossRef]
- Piattelli, A.; Pontes, A.E.; Degidi, M.; Iezzi, G. Histologic studies on osseointegration: Soft tissues response to implant surfaces and components. A review. Dent. Mater. 2011, 27, 53–60. [Google Scholar] [CrossRef]
- Dohan Ehrenfest, D.M.; Coelho, P.G.; Kang, B.S.; Sul, Y.T.; Albrektsson, T. Classification of osseointegrated implant surfaces: Materials, chemistry and topography. Trends Biotechnol. 2010, 28, 198–206. [Google Scholar] [CrossRef]
- Teughels, W.; Van Assche, N.; Sliepen, I.; Quirynen, M. Effect of material characteristics and/or surface topography on biofilm development. Clin. Oral Implants Res. 2006, 17 (Suppl. S2), 68–81. [Google Scholar] [CrossRef] [PubMed]
- Van Assche, N.; Pittayapat, P.; Jacobs, R.; Pauwels, M.; Teughels, W.; Quirynen, M. Microbiological outcome of two screw-shaped titanium implant systems placed following a split-mouth randomised protocol, at the 12th year of follow-up after loading. Eur. J. Oral Implantol. 2011, 4, 103–116. [Google Scholar] [PubMed]
- Canullo, L.; Götz, W. Peri-implant hard tissue response to glow-discharged abutments: Prospective study. Preliminary radiological results. Ann. Anat. 2012, 194, 529–532. [Google Scholar] [CrossRef] [PubMed]











{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Group | Mean OD | Std. Deviation | Std. Error |
|---|---|---|---|
| Autoclave n = 3 | 3.63 | 0.15 | 0.09 |
| Ultrasonic n = 4 | 3.41 | 0.37 | 0.19 |
| Steam n = 3 | 3.29 | 0.22 | 0.12 |
| CHX n = 5 | 0.70 | 0.30 | 0.13 |
| NaOCl n = 2 | 3.54 | 0.09 | 0.06 |
| Prep non-decont. n = 3 | 3.48 | 0.23 | 0.13 |
| Factory n = 3 | 3.62 | 0.04 | 0.02 |
| F df = 6, 16 | 78.896 * |
| Group (I) | Group (J) | Mean Difference (I–J) | Std. Error | Sig. |
|---|---|---|---|---|
| CHX | Autoclave | −2.93 | 0.19 | <0.001 |
| Ultrasonic | −2.71 | 0.17 | ||
| Steam | −2.59 | 0.19 | ||
| NaOCl | −2.84 | 0.21 | ||
| Prep non-decont. | −2.78 | 0.19 | ||
| Factory | −2.92 | 0.19 |
| Group | Mean (CFU/mL) | Std. Deviation |
|---|---|---|
| Steam | 3.18 × 109 | 2.36 × 108 |
| Autoclave | 0 | 0 |
| Ultrasonic | 1.85 × 109 | 1.29 × 108 |
| CHX | 0 | 0 |
| NaOCl | 1 × 108 | 1.15 × 108 |
| CHX + S | 0 | 0 |
| NaOCl + S | 0 | 0 |
| Control Unadjusted untreated abutments | 2.75 × 109 | 1.91 × 108 |
| Control Adjusted untreated abutments | 2.83 × 109 | 2.06 × 108 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sharon, E.; Pietrokovski, Y.; Engel, I.; Assali, R.; Houri-Haddad, Y.; Beyth, N. Biocompatibility, Surface Morphology, and Bacterial Load of Dental Implant Abutments following Decontamination Protocols: An In-Vitro Study. Materials 2023, 16, 4080. https://doi.org/10.3390/ma16114080
Sharon E, Pietrokovski Y, Engel I, Assali R, Houri-Haddad Y, Beyth N. Biocompatibility, Surface Morphology, and Bacterial Load of Dental Implant Abutments following Decontamination Protocols: An In-Vitro Study. Materials. 2023; 16(11):4080. https://doi.org/10.3390/ma16114080
Chicago/Turabian StyleSharon, Esi, Yoav Pietrokovski, Ilana Engel, Rula Assali, Yael Houri-Haddad, and Nurit Beyth. 2023. "Biocompatibility, Surface Morphology, and Bacterial Load of Dental Implant Abutments following Decontamination Protocols: An In-Vitro Study" Materials 16, no. 11: 4080. https://doi.org/10.3390/ma16114080