
Prognostic Factors in Endodontic Surgery Using an Endoscope: A 1 Year Retrospective Cohort Study

 , , , ,
, , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Ethics Statement
2.3. Patients
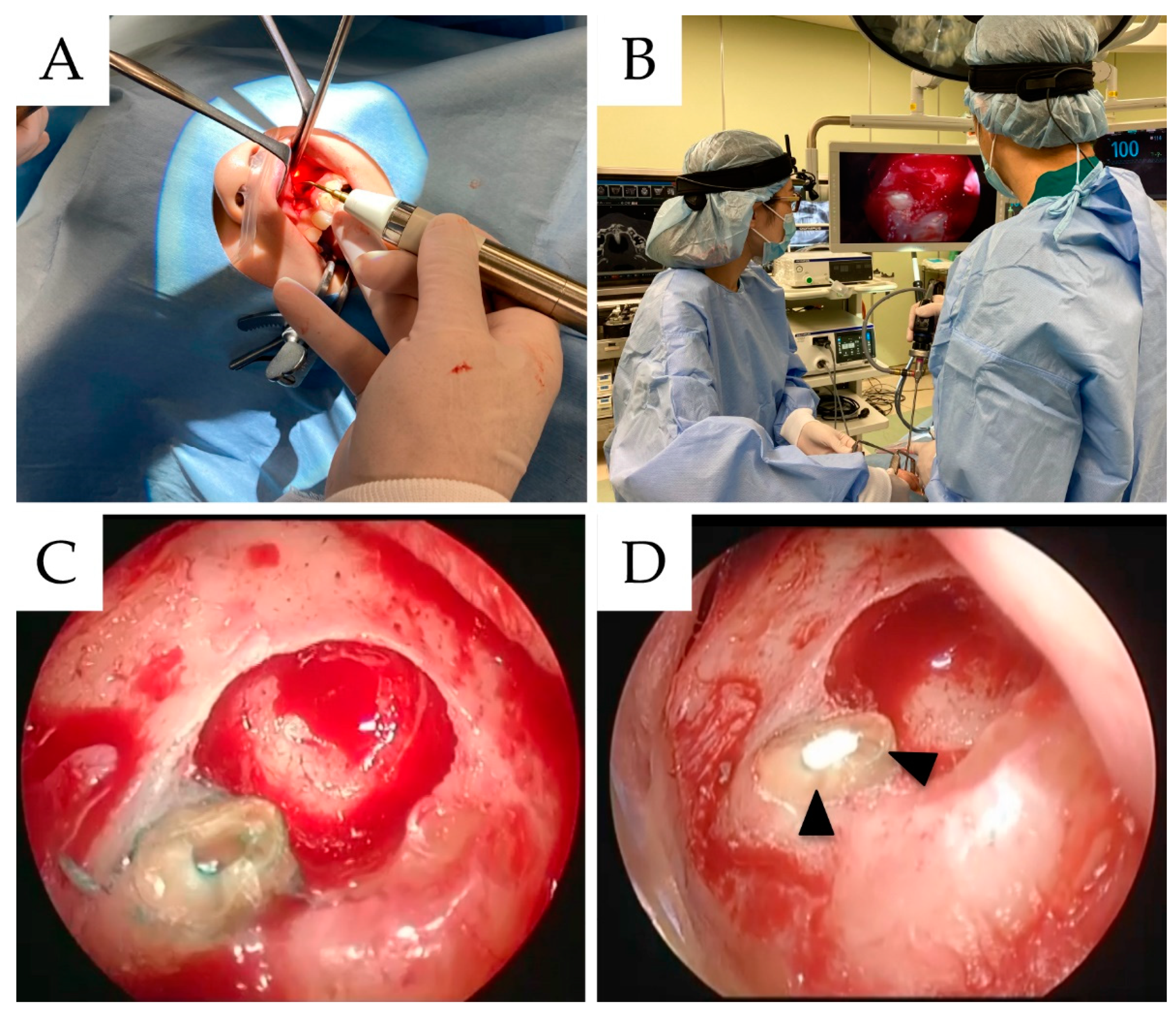
2.4. Surgical Procedure
2.5. Predictor Variables
2.6. Outcome Variables
2.7. Statistical Analysis
3. Results
3.1. Distribution of Predictive Variables Based on the Results Obtained after Endodontic Surgeries
3.2. Correlation Coefficients between Endodontic Surgical Success and Failure Variables
3.3. Multivariate Logistic Regression Model Results of Endodontic Surgery
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Kim, E.; Kim, Y. Endodontic microsurgery: Outcomes and prognostic factors. Curr. Oral Health Rep. 2019, 6, 356–366. [Google Scholar] [CrossRef]
- Tawil, P.Z.; Saraiya, V.M.; Galicia, J.C.; Duggan, D.J. Periapical microsurgery: The effect of root dentinal defects on short- and long-term outcome. J. Endod. 2015, 41, 22–27. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Taschieri, S.; del Fabbro, M.; Testori, T.; Francetti, L.; Weinstein, R. Endodontic surgery using 2 different magnification devices: Preliminary results of a randomized controlled study. J. Oral Maxillofac. Surg. 2006, 64, 235–242. [Google Scholar] [CrossRef] [PubMed]
- Taschieri, S.; del Fabbro, M.; Testori, T.; Weinstein, R. Microscope versus endoscope in root-end management: A randomized controlled study. Int. J. Oral Maxillofac. Surg. 2008, 37, 1022–1026. [Google Scholar] [CrossRef] [PubMed]
- Taschieri, S.; del Fabbro, M. Endoscopic endodontic microsurgery: 2-year evaluation of healing and functionality. Braz. Oral Res. 2009, 23, 23–30. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pallarés-Serrano, A.; Glera-Suarez, P.; Tarazona-Alvarez, B.; Peñarrocha-Diago, M.; Peñarrocha-Diago, M.; Peñarrocha-Oltra, D. Prognostic Factors after Endodontic Microsurgery: A Retrospective Study of 111 Cases with 5 to 9 Years of Follow-up. J. Endod. 2021, 47, 397–403. [Google Scholar] [CrossRef]
- Blahuta, R.; Stanko, P. The use of optical magnifying devices in periradicular microsurgery. Bratislava Med. J. 2012, 113, 311–313. [Google Scholar] [CrossRef] [Green Version]
- Baldassari-Cruz, L.A.; Lilly, J.P.; Rivera, E.M. The influence of dental operating microscope in locating the mesiolingual canal orifice. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 2002, 93, 190–194. [Google Scholar] [CrossRef]
- Filho, T.C.; Sá La Cerda, R.; Filho, E.D.G.; de Deus, G.A.; Magalhães, K.M. The influence of the Surgical Operating Microscope in locating the mesiolingual canal orifice: A laboratory analysis. Braz. Oral Res. 2006, 20, 59–63. [Google Scholar] [CrossRef] [Green Version]
- Sukegawa, S.; Yamamoto, N.; Matsuyama, T.; Takabatake, K.; Kawai, H.; Nagatsuka, H.; Furuki, Y. Factors of Successful Treatment Using the Bone Lid Technique in Maxillofacial Surgery: A Pilot Study. J. Hard Tissue Biol. 2021, 30, 193–198. [Google Scholar] [CrossRef]
- Sukegawa, S.; Kanno, T.; Kawai, H.; Shibata, A.; Matsumoto, K.; Sukegawa-Takahashi, Y.; Sakaida, K.; Nagatsuka, H.; Furuki, Y. Surgical Treatment and Dental Implant Rehabilitation after the Resection of an Osseous Dysplasia. J. Hard Tissue Biol. 2016, 25, 437–441. [Google Scholar] [CrossRef] [Green Version]
- Kang, S.; Ha, S.W.; Kim, U.; Kim, S.; Kim, E. A One-Year Radiographic Healing Assessment after Endodontic Microsurgery Using Cone-Beam Computed Tomographic Scans. J. Clin. Med. 2020, 9, 3714. [Google Scholar] [CrossRef] [PubMed]
- Del Fabbro, M.; Taschieri, S. Endodontic therapy using magnification devices: A systematic review. J. Dent. 2010, 38, 269–275. [Google Scholar] [CrossRef]
- Taschieri, S.; del Fabbro, M.; Testori, T.; Weinstein, R. Endoscopic periradicular surgery: A prospective clinical study. Br. J. Oral Maxillofac. Surg. 2007, 45, 242–244. [Google Scholar] [CrossRef] [PubMed]
- Zuolo, M.L.; Ferreira, M.O.F.; Gutmann, J.L. Prognosis in periradicular surgery: A clinical prospective study. Int. Endod. J. 2000, 33, 91–98. [Google Scholar] [CrossRef]
- Kishimoto, T.; Sukegawa, S.; Ono, S.; Nakamura, S.; Ando, M.; Yoshino, T.; Furuki, Y. Endoscope-assisted enucleation of mandibular dentigerous cysts. J. Oral Maxillofac. Surgery, Med. Pathol. 2021, 33, 126–130. [Google Scholar] [CrossRef]
- Kishimoto, T.; Sukegawa, S.; Katase, N.; Kanno, T.; Sukegawa-Takahashi, Y.; Masui, M.; Sato, A.; Furuki, Y. Endoscope-assisted resection of intramuscular cavernous hemangioma within the temporal muscle. J. Craniofac. Surg. 2019, 30, 193–195. [Google Scholar] [CrossRef]
- Hayashi, H.; Abe, A.; Ota, M.; Momokita, M.; Ishihama, T.; Furuta, H.; Taniguchi, T.; Takeuchi, K. Endoscopic removal of accidental aspirated and ingested dental foreign bodies: A cross-sectional study. Medicine 2021, 100, e27602. [Google Scholar] [CrossRef]
- Von Arx, T.; Peñarrocha, M.; Jensen, S. Prognostic factors in apical surgery with root-end filling: A meta-analysis. J. Endod. 2010, 36, 957–973. [Google Scholar] [CrossRef]
- Bliggenstorfer, S.; Chappuis, V.; von Arx, T. Outcome of Periapical Surgery in Molars: A Retrospective Analysis of 424 Teeth. J. Endod. 2021, 47, 1703–1714. [Google Scholar] [CrossRef]
- Kim, S.; Song, M.; Shin, S.J.; Kim, E. A randomized controlled study of mineral trioxide aggregate and super ethoxybenzoic acid as root-end filling materials in endodontic microsurgery: Long-term outcomes. J. Endod. 2016, 42, 997–1002. [Google Scholar] [CrossRef] [PubMed]
- Bonson, S.; Jeansonne, B.G.; Lallier, T.E. Root-end filling materials alter fibroblast differentiation. J. Dent. Res. 2004, 83, 408–413. [Google Scholar] [CrossRef] [PubMed]
- Song, M.; Jung, I.Y.; Lee, S.J.; Lee, C.Y.; Kim, E. Prognostic factors for clinical outcomes in endodontic microsurgery: A retrospective study. J. Endod. 2011, 37, 927–933. [Google Scholar] [CrossRef] [PubMed]
- Dunfee, B.L.; Sakai, O.; Pistey, R.; Gohel, A. Radiologic and pathologic characteristics of benign and malignant lesions of the mandible. Radiographics 2006, 26, 1751–1768. [Google Scholar] [CrossRef]
- Vinci, R.; Teté, G.; Lucchetti, F.R.; Capparé, P.; Gherlone, E.F. Implant survival rate in calvarial bone grafts: A retrospective clinical study with 10 year follow-up. Clin. Implant Dent. Relat. Res. 2019, 21, 662–668. [Google Scholar] [CrossRef]
- Sukegawa, S.; Matsuzaki, H.; Katase, N.; Kawai, H.; Kanno, T.; Asaumi, J.I.; Furuki, Y. Morphological characteristics of radicular cysts using computed tomography. Odontology 2020, 108, 74–83. [Google Scholar] [CrossRef]
- Maddalone, M.; Gagliani, M. Periapical endodontic surgery: A 3-year follow-up study. Int. Endod. J. 2003, 36, 193–198. [Google Scholar] [CrossRef]
- Taschieri, S.; del Fabbro, M.; Testori, T.; Francetti, L.; Weinstein, R. Endodontic surgery with ultrasonic retrotips: One-year follow-up. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 2005, 100, 380–387. [Google Scholar] [CrossRef]
- Rahbaran, S.; Gilthorpe, M.S.; Harrison, S.D.; Gulabivala, K. Comparison of clinical outcome of periapical surgery in endodontic and oral surgery units of a teaching dental hospital: A retrospective study. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 2001, 91, 700–709. [Google Scholar] [CrossRef]
- Mari, D.D.; Kotz, S. Correlation and Dependence; Imperial College Press: London, UK; World Scientific Publishing Co.: Singapore, 2001. [Google Scholar]
- Tecco, S.; Grusovin, M.G.; Sciara, S.; Bova, F.; Pantaleo, G.; Capparé, P. The association between three attitude-related indexes of oral hygiene and secondary implant failures: A retrospective longitudinal study. Int. J. Dent. Hyg. 2018, 16, 372–379. [Google Scholar] [CrossRef]
- Rosso, M.; Blasi, G.; Gherlone, E.; Rosso, R. Effect of granulocyte-macrophage colony-stimulating factor on prevention of mucositis in head and neck cancer patients treated with chemo-radiotherapy. J. Chemother. 1997, 9, 382–385. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Patients | ||||
|---|---|---|---|---|
| Gender | Male | Female | Total | |
| 90 | 152 | 242 | ||
| % | 37.2 | 62.8 | ||
| Age (years) | Mean | SD | Range | Median |
| 48.3 | 15.0 | 12- 82 | 49.0 | |
| Outcome | n | % | ||
| Success | 345 | 95.3 | ||
| Failure | 17 | 4.7 |
| Failure | Success | p-Value | |
|---|---|---|---|
| Outcome (%) | 17 (4.7) | 345 (95.3) | |
| Demographic variables | |||
| Age | |||
| >60 | 9 | 77 | 0.007 |
| ≤60 | 8 | 268 | |
| Gender | 0.788 | ||
| Male | 6 | 133 | |
| Female | 11 | 212 | |
| Health status variables | |||
| Diabetes | 1 | 12 | 0.603 |
| Chronic hepatitis | 0 | 4 | 0.655 |
| Malignant tumor | 2 | 9 | 0.089 |
| Anatomic variables | |||
| Tooth position | 0.095 | ||
| Anterior | 9 | 259 | |
| Premolar | 5 | 62 | |
| Molar | 3 | 24 | |
| Jaw | 0.774 | ||
| Maxilla | 12 | 260 | |
| Mandible | 5 | 85 | |
| Lt/Rt | 0.325 | ||
| Lt | 7 | 188 | |
| Rt | 10 | 157 | |
| Pathological variables | |||
| Mesio-distal | 0.096 | ||
| Large | 6 | 59 | |
| Small | 11 | 286 | |
| Bucco-lingual | 0.076 | ||
| Large | 6 | 204 | |
| Small | 11 | 141 | |
| Expansion of the jaw | 0.029 | ||
| Presence | 0 | 76 | |
| Absence | 17 | 269 | |
| Cortical bone defect | 0.797 | ||
| Presence | 10 | 221 | |
| Absence | 7 | 124 | |
| Perilesional sclerotic signs | 0.022 | ||
| Presence | 1 | 111 | |
| Absence | 16 | 234 | |
| Through-and-through bone defect | 0.521 | ||
| Presence | 1 | 14 | |
| Absence | 16 | 331 | |
| Operative variables | |||
| Bone lid surgery | 0.583 | ||
| Presence | 0 | 17 | |
| Absence | 6 | 338 | |
| Dental variables | |||
| Restoration | 0.062 | ||
| bridge | 3 | 21 | |
| Single/splinted crown | 14 | 324 | |
| Post | <0.001 | ||
| Presence | 15 | 146 | |
| Absence | 2 | 199 | |
| Standard Error | OR | Lower 95% | Upper 95% | p Value | |
|---|---|---|---|---|---|
| Post | 0.383 | 9.592 | 2.135 | 43.092 | <0.001 |
| Perilesional sclerotic signs | 0.523 | 7.348 | 0.880 | 53.386 | 0.066 |
| Age | 0.263 | 3.107 | 1.118 | 8.635 | 0.030 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sukegawa, S.; Shimizu, R.; Sukegawa, Y.; Hasegawa, K.; Ono, S.; Fujimura, A.; Yamamoto, I.; Nakano, K.; Takabatake, K.; Kawai, H.; et al. Prognostic Factors in Endodontic Surgery Using an Endoscope: A 1 Year Retrospective Cohort Study. Materials 2022, 15, 3353. https://doi.org/10.3390/ma15093353
Sukegawa S, Shimizu R, Sukegawa Y, Hasegawa K, Ono S, Fujimura A, Yamamoto I, Nakano K, Takabatake K, Kawai H, et al. Prognostic Factors in Endodontic Surgery Using an Endoscope: A 1 Year Retrospective Cohort Study. Materials. 2022; 15(9):3353. https://doi.org/10.3390/ma15093353
Chicago/Turabian StyleSukegawa, Shintaro, Rieko Shimizu, Yuka Sukegawa, Kazuaki Hasegawa, Sawako Ono, Ai Fujimura, Izumi Yamamoto, Keisuke Nakano, Kiyofumi Takabatake, Hotaka Kawai, and et al. 2022. "Prognostic Factors in Endodontic Surgery Using an Endoscope: A 1 Year Retrospective Cohort Study" Materials 15, no. 9: 3353. https://doi.org/10.3390/ma15093353