
Biocompatibility of a New Calcium Silicate-Based Root Canal Sealer Mediated via the Modulation of Macrophage Polarization in a Rat Model

 ,
,  , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Preparation of Specimens
2.2. Tube Implantation
2.3. Analysis of Dentine Tube Sealer Composition and Structure
2.4. Analysis of Systemic Toxicity
2.5. Analysis of Inflammatory Responses and Foreign Body Reactions
2.6. Analysis of Macrophage Polarization In Vivo
2.7. In Vitro Macrophage Polarization Analysis
2.7.1. Isolation of Bone-Marrow-Derived Macrophages (BMDMs)
2.7.2. RT–qPCR Assessment of the Effects of iRoot SP and HiFlow Extracts on the Expression of Inflammatory Mediators
2.7.3. Analysis of BMDM Surface Marker Expression by Flow Cytometry
2.8. Statistical Analysis
3. Results
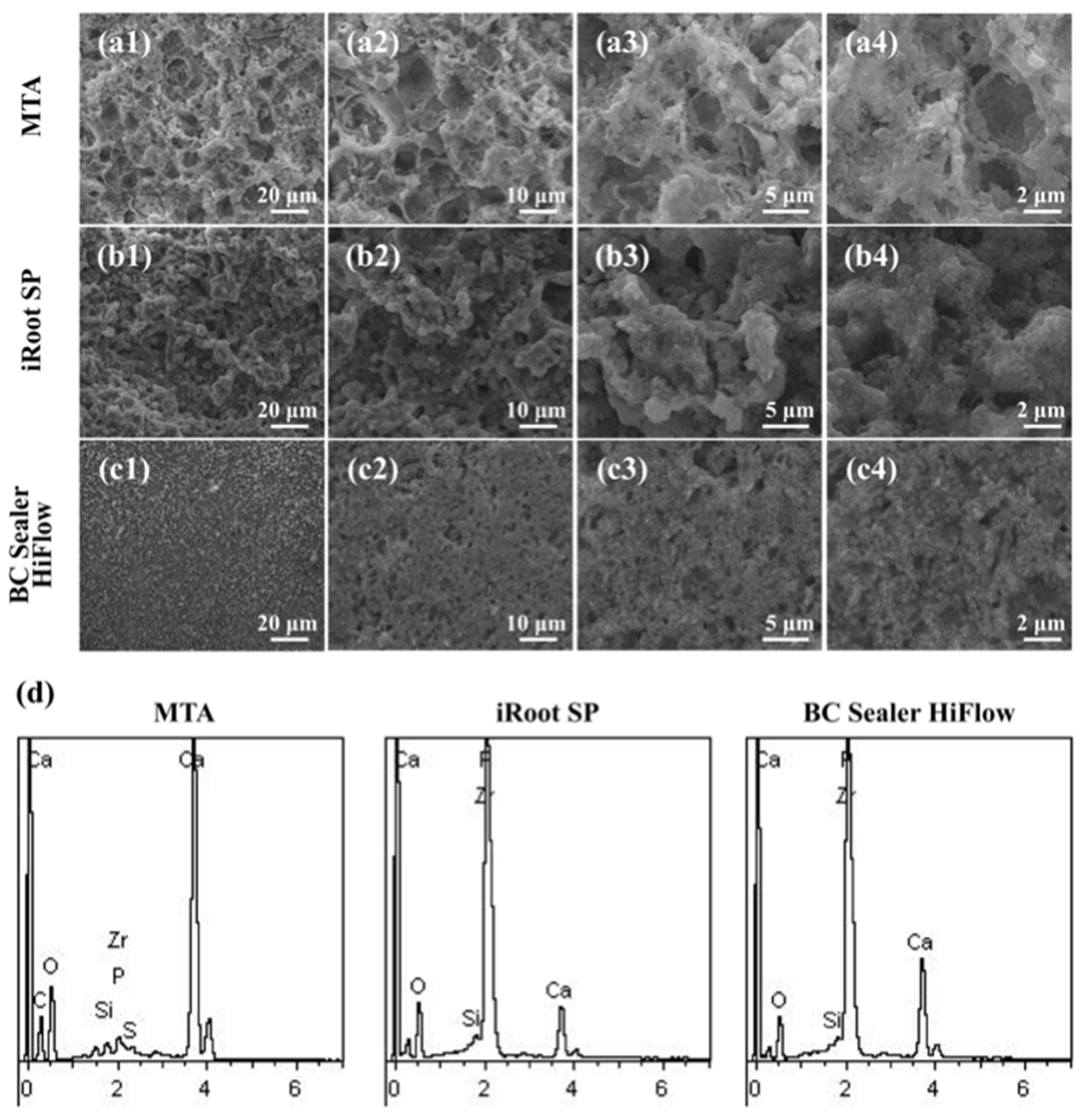
3.1. Apatite Layers Formed on the Surfaces of MTA, iRoot SP and HiFlow In Vivo
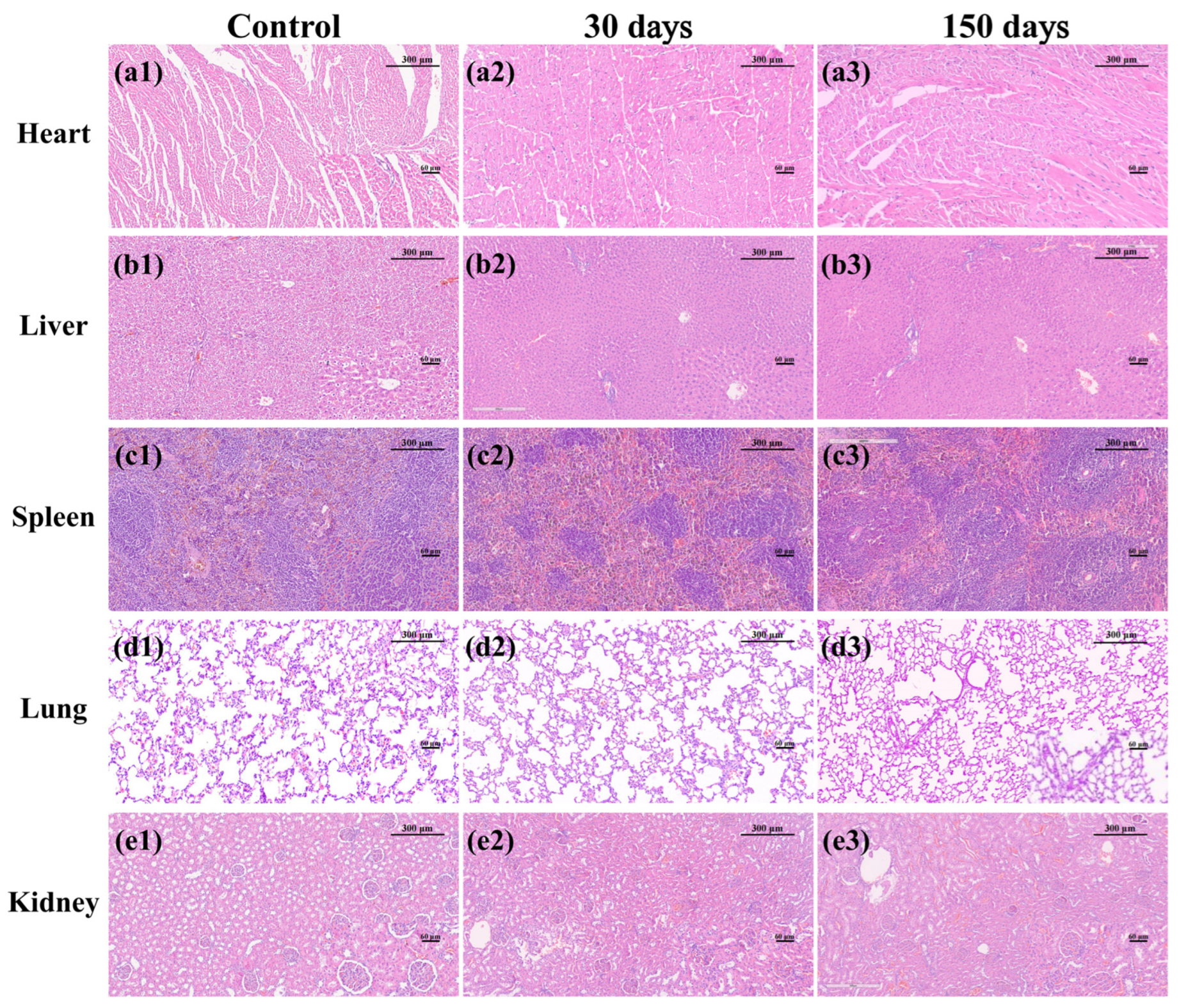
3.2. MTA, iRoot SP and HiFlow Exhibited No Systemic Toxicity
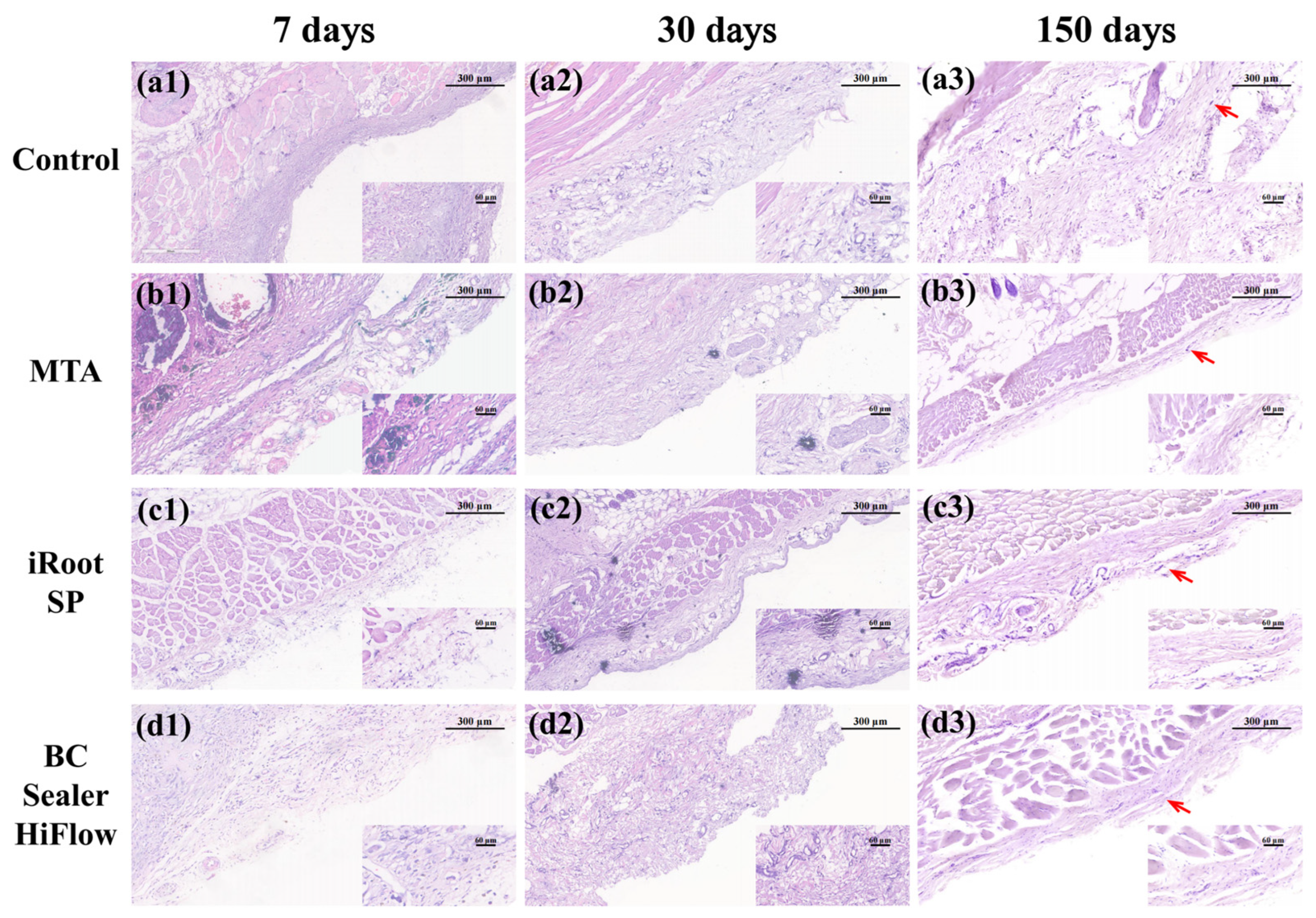
3.3. Long-Term Biocompatibility of MTA, iRoot SP and HiFlow
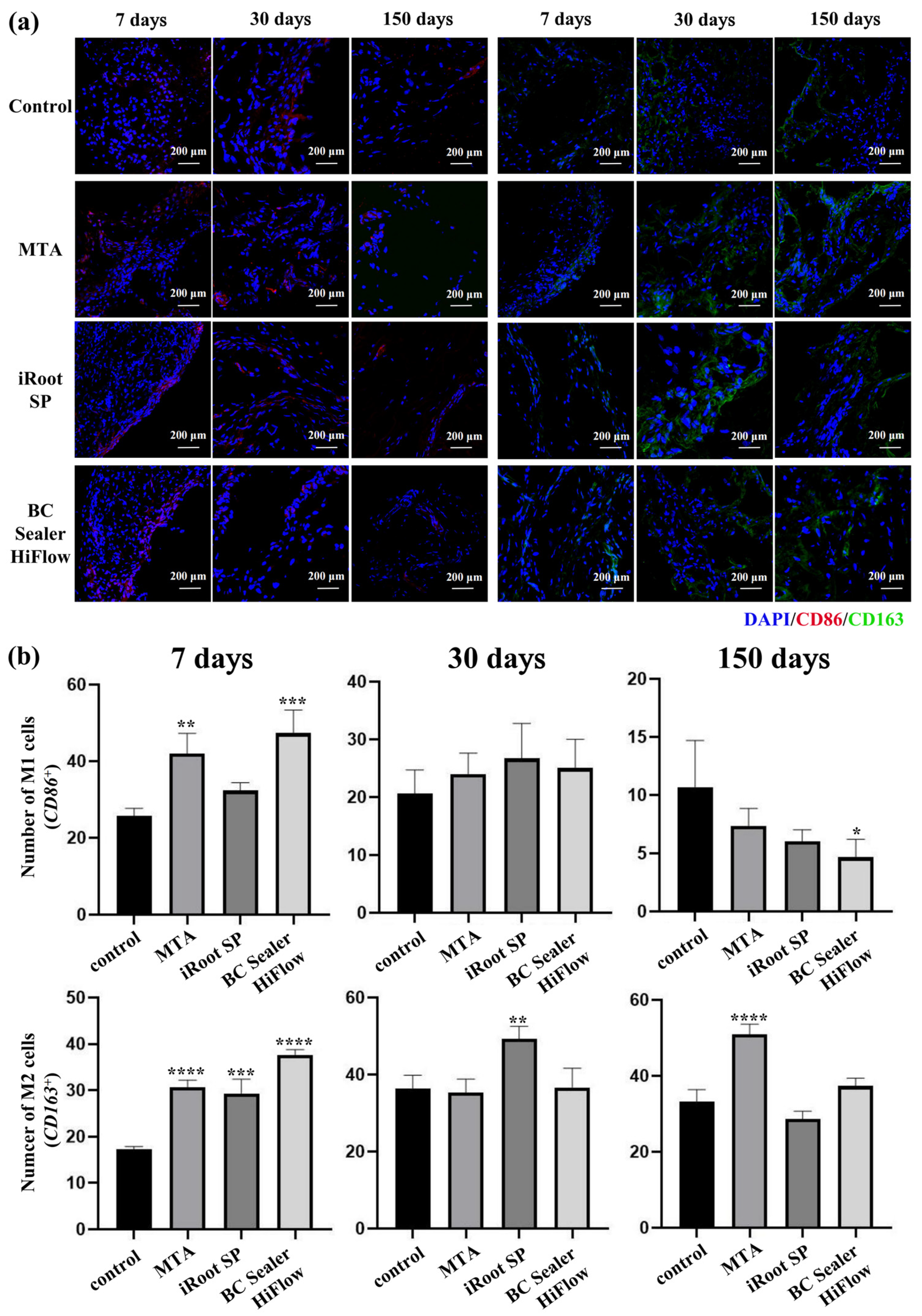
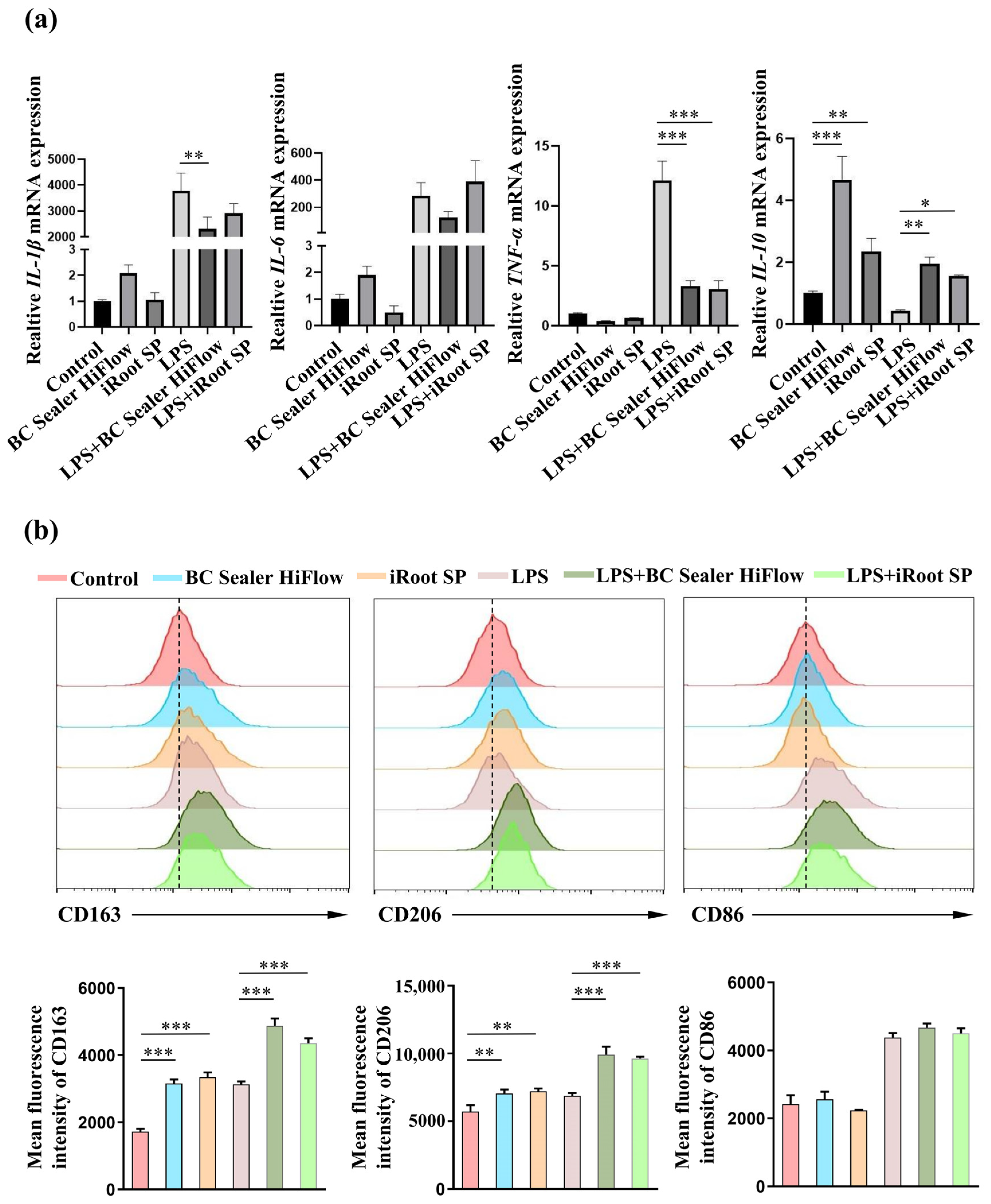
3.4. iRoot SP and HiFlow Promoted M2-like Macrophage Polarization
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Donnermeyer, D.; Burklein, S.; Dammaschke, T.; Schafer, E. Endodontic sealers based on calcium silicates: A systematic review. Odontology 2019, 107, 421–436. [Google Scholar] [CrossRef] [PubMed]
- Candeiro, G.T.; Correia, F.C.; Duarte, M.A.; Ribeiro-Siqueira, D.C.; Gavini, G. Evaluation of radiopacity, pH, release of calciumions, and flow of a bioceramic root canal sealer. J. Endod. 2012, 38, 842–845. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhou, H.M.; Shen, Y.; Zheng, W.; Li, L.; Zheng, Y.F.; Haapasalo, M. Physical properties of 5 root canal sealers. J. Endod. 2013, 39, 1281–1286. [Google Scholar] [CrossRef] [PubMed]
- Bosio, C.C.; Felippe, G.S.; Bortoluzzi, E.A.; Felippe, M.C.; Felippe, W.T.; Rivero, E.R. Subcutaneous connective tissue reactions to iRoot SP, mineral trioxide aggregate (MTA) Fillapex, DiaRoot BioAggregate and MTA. Int. Endod. J. 2014, 47, 667–674. [Google Scholar] [CrossRef]
- Chang, S.W.; Lee, S.Y.; Kang, S.K.; Kum, K.Y.; Kim, E.C. In vitro biocompatibility, inflammatory response, and osteogenic potential of 4 root canal sealers: Sealapex, Sankin apatite root sealer, MTA Fillapex, and iRoot SP root canal sealer. J. Endod. 2014, 40, 1642–1648. [Google Scholar] [CrossRef]
- Marashdeh, M.Q.; Friedman, S.; Lévesque, C.; Finer, Y. Esterases affect the physical properties of materials used to seal the endodontic space. Dent. Mater. 2019, 35, 1065–1072. [Google Scholar] [CrossRef]
- Fernández, R.; Restrepo, J.S.; Aristizábal, D.C.; Álvarez, L.G. Evaluation of the filling ability of artificial lateral canals using calcium silicate-based and epoxy resin-based endodontic sealers and two gutta-percha filling techniques. Int. Endod. J. 2016, 49, 365–373. [Google Scholar] [CrossRef]
- Oliveira, D.S.; Cardoso, M.L.; Queiroz, T.F.; Silva, E.J.; Souza, E.M.; De-Deus, G. Suboptimal push-out bond strengths of calcium silicate-based sealers. Int. Endod. J. 2016, 49, 796–801. [Google Scholar] [CrossRef]
- Qu, W.; Bai, W.; Liang, Y.H.; Gao, X.J. Influence of Warm Vertical Compaction Technique on Physical Properties of Root Canal Sealers. J. Endod. 2016, 42, 1829–1833. [Google Scholar] [CrossRef]
- Yang, R.; Tian, J.; Huang, X.; Lei, S.; Cai, Y.; Xu, Z.; Wei, X. A comparative study of dentinal tubule penetration and the retreatability of EndoSequence BC Sealer HiFlow, iRoot SP, and AH Plus with different obturation techniques. Clin. Oral. Investig. 2021, 25, 4163–4173. [Google Scholar] [CrossRef]
- Zhang, W.J.; Liu, H.; Wang, Z.J.; Haapasalo, M.; Jiang, Q.Z.; Shen, Y. Long-term porosity and retreatability of oval-shaped canals obturated using two different methods with a novel tricalcium silicate sealer. Clin. Oral. Investig. 2022, 26, 1045–1052. [Google Scholar] [CrossRef] [PubMed]
- Rodriguez-Lozano, F.J.; Lopez-Garcia, S.; Garcia-Bernal, D.; Tomas-Catala, C.J.; Santos, J.M.; Llena, C.; Lozano, A.; Murcia, L.; Forner, L. Chemical composition and bioactivity potential of the new Endosequence BC Sealer formulation HiFlow. Int. Endod. J. 2020, 53, 1216–1228. [Google Scholar] [CrossRef] [PubMed]
- Sanz, J.L.; Lopez-Garcia, S.; Lozano, A.; Pecci-Lloret, M.P.; Llena, C.; Guerrero-Girones, J.; Rodriguez-Lozano, F.J.; Forner, L. Microstructural composition, ion release, and bioactive potential of new premixed calcium silicate-based endodontic sealers indicated for warm vertical compaction technique. Clin. Oral. Investig. 2021, 25, 1451–1462. [Google Scholar] [CrossRef] [PubMed]
- Silva, E.C.A.; Tanomaru-Filho, M.; Silva, G.F.; Lopes, C.S.; Cerri, P.S.; Guerreiro Tanomaru, J.M. Evaluation of the biological properties of two experimental calcium silicate sealers: An in vivo study in rats. Int. Endod. J. 2021, 54, 100–111. [Google Scholar] [CrossRef] [PubMed]
- Bossu, M.; Mancini, P.; Bruni, E.; Uccelletti, D.; Preziosi, A.; Rulli, M.; Relucenti, M.; Donfrancesco, O.; Iaculli, F.; Di Giorgio, G.; et al. Biocompatibility and antibiofilm properties of calcium silicate-based cements: An in vitro evaluation and report of two clinical cases. Biology 2021, 10, 470. [Google Scholar] [CrossRef] [PubMed]
- Kang, C.M.; Seong, S.; Song, J.S.; Shin, Y. The role of hydraulic silicate cements on long-term properties and biocompatibility of partial pulpotomy in permanent teeth. Materials 2021, 14, 305. [Google Scholar] [CrossRef]
- Yeh, H.W.; Chiang, C.F.; Chen, P.H.; Su, C.C.; Wu, Y.C.; Chou, L.; Huang, R.Y.; Liu, S.Y.; Shieh, Y.S. Axl involved in mineral trioxide aggregate induces macrophage polarization. J. Endod. 2018, 44, 1542–1548. [Google Scholar] [CrossRef]
- Santos, J.M.; Coelho, C.M.; Sequeira, D.B.; Marques, J.A.; Pereira, J.F.; Sousa, V.; Palma, P.J.; Santos, A.C. Subcutaneous implantation assessment of new calcium-silicate based Sealer for warm obturation. Biomedicines 2021, 9, 24. [Google Scholar] [CrossRef]
- Davaie, S.; Hooshmand, T.; Ansarifard, S. Different types of bioceramics as dental pulp capping materials: A systematic review. Ceram. Int. 2021, 47, 20781–20792. [Google Scholar] [CrossRef]
- Oh, H.; Kim, E.; Lee, S.; Park, S.; Chen, D.; Shin, S.J.; Kim, E.; Kim, S. Comparison of biocompatibility of calcium silicate-based sealers and epoxy resin-based sealer on human periodontal ligament stem cells. Materials 2020, 13, 5242. [Google Scholar] [CrossRef]
- Abou ElReash, A.; Hamama, H.; Abdo, W.; Wu, Q.; Zaen El-Din, A.; Xiaoli, X. Biocompatibility of new bioactive resin composite versus calcium silicate cements: An animal study. BMC Oral Health 2019, 19, 194. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Olsson, B.; Sliwkowski, A.; Langeland, K. Subcutaneous implantation for the biological evaluation of endodontic materials. J. Endod. 1981, 7, 355–367. [Google Scholar] [CrossRef]
- Hoshino, R.A.; Silva, G.F.D.; Delfino, M.M.; Guerreiro-Tanomaru, J.M.; Tanomaru-Filho, M.; Sasso-Cerri, E.; Filho, I.B.; Cerri, P.S. Physical Properties, Antimicrobial Activity and In Vivo Tissue Response to Apexit Plus. Materials 2020, 13, 1171. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Prati, C.; Gandolfi, M.G. Calcium silicate bioactive cements: Biological perspectives and clinical applications. Dent. Mater. 2015, 31, 351–370. [Google Scholar] [CrossRef]
- Kim, M.; Yang, W.; Kim, H.; Ko, H. Comparison of the biological properties of ProRoot MTA, OrthoMTA, and Endocem MTA cements. J. Endod. 2014, 40, 1649–1653. [Google Scholar] [CrossRef] [PubMed]
- Reyes-Carmona, J.F.; Felippe, M.S.; Felippe, W.T. Biomineralization ability and interaction of mineral trioxide aggregate and white portland cement with dentin in a phosphate-containing fluid. J. Endod. 2009, 35, 731–736. [Google Scholar] [CrossRef]
- Swarup, S.J.; Rao, A.; Boaz, K.; Srikant, N.; Shenoy, R. Pulpal response to nano hydroxyapatite, mineral trioxide aggregate and calcium hydroxide when used as a direct pulp capping agent: An in vivo study. J. Clin. Pediatr. Dent. 2014, 38, 201–206. [Google Scholar] [CrossRef]
- Delfino, M.M.; de Abreu Jampani, J.L.; Lopes, C.S.; Guerreiro-Tanomaru, J.M.; Tanomaru-Filho, M.; Sasso-Cerri, E.; Cerri, P.S. Comparison of Bio-C Pulpo and MTA Repair HP with White MTA: Effect on liver parameters and evaluation of biocompatibility and bioactivity in rats. Int. Endod. J. 2021, 54, 1597–1613. [Google Scholar] [CrossRef]
- Talabani, R.M.; Garib, B.T.; Masaeli, R. Bioactivity and physicochemical properties of three calcium silicate-based cements: An in vitro study. Biomed. Res. Int. 2020, 2020, 9576930. [Google Scholar] [CrossRef]
- Hinata, G.; Yoshiba, K.; Han, L.; Edanami, N.; Yoshiba, N.; Okiji, T. Bioactivity and biomineralization ability of calcium silicate-based pulp-capping materials after subcutaneous implantation. Int. Endod. J. 2017, 50, e40–e51. [Google Scholar] [CrossRef] [Green Version]
- Antunes, T.B.M.; Janini, A.C.P.; Pelepenko, L.E.; Abuna, G.F.; Paiva, E.M.; Sinhoreti, M.A.C.; Raimundo, I.M., Jr.; Gomes, B.; de-Jesus-Soares, A.; Marciano, M.A. Heating stability, physical and chemical analysis of calcium silicate-based endodontic sealers. Int. Endod. J. 2021, 54, 1175–1188. [Google Scholar] [CrossRef] [PubMed]
- Sumer, M.; Muglali, M.; Bodrumlu, E.; Guvenc, T. Reactions of connective tissue to amalgam, intermediate restorative material, mineral trioxide aggregate, and mineral trioxide aggregate mixed with chlorhexidine. J. Endod. 2006, 32, 1094–1096. [Google Scholar] [CrossRef] [PubMed]
- Yaltirik, M.; Ozbas, H.; Bilgic, B.; Issever, H. Reactions of connective tissue to mineral trioxide aggregate and amalgam. J. Endod. 2004, 30, 95–99. [Google Scholar] [CrossRef] [PubMed]
- Ferreira, C.M.A.; Sassone, L.M.; Goncalves, A.S.; de Carvalho, J.J.; Tomas-Catala, C.J.; Garcia-Bernal, D.; Onate-Sanchez, R.E.; Rodriguez-Lozano, F.J.; Silva, E. Physicochemical, cytotoxicity and in vivo biocompatibility of a high-plasticity calcium-silicate based material. Sci. Rep. 2019, 9, 3933. [Google Scholar] [CrossRef]
- Wismayer, P.S.; Lung, C.Y.K.; Rappa, F.; Cappello, F.; Camilleri, J. Assessment of the interaction of Portland cement-based materials with blood and tissue fluids using an animal model. Sci. Rep. 2016, 6, 34547. [Google Scholar] [CrossRef] [Green Version]
- Bae, W.J.; Chang, S.W.; Lee, S.I.; Kum, K.Y.; Bae, K.S.; Kim, E.C. Human periodontal ligament cell response to a newly developed calcium phosphate-based root canal sealer. J. Endod. 2010, 36, 1658–1663. [Google Scholar] [CrossRef]
- Corral Nunez, C.; Altamirano Gaete, D.; Maureira, M.; Martin, J.; Covarrubias, C. Nanoparticles of bioactive glass enhance biodentine bioactivity on dental pulp stem cells. Materials 2021, 14, 2684. [Google Scholar] [CrossRef]
- Patlolla, A.; Arinzeh, T.L. Evaluating apatite formation and osteogenic activity of electrospun composites for bone tissue engineering. Biotechnol. Bioeng. 2014, 111, 1000–1017. [Google Scholar] [CrossRef]
- Chen, B.; Haapasalo, M.; Mobuchon, C.; Li, X.; Ma, J.; Shen, Y. Cytotoxicity and the effect of temperature on physical properties and chemical composition of a new calcium silicate-based root canal sealer. J. Endod. 2020, 46, 531–538. [Google Scholar] [CrossRef]
- Mosser, D.M.; Edwards, J.P. Exploring the full spectrum of macrophage activation. Nat. Rev. Immunol. 2008, 8, 958–969. [Google Scholar] [CrossRef]
- Italiani, P.; Boraschi, D. From monocytes to M1/M2 macrophages: Phenotypical vs. functional differentiation. Front. Immunol. 2014, 5, 514. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pajarinen, J.; Lin, T.; Gibon, E.; Kohno, Y.; Maruyama, M.; Nathan, K.; Lu, L.; Yao, Z.; Goodman, S.B. Mesenchymal stem cell-macrophage crosstalk and bone healing. Biomaterials 2019, 196, 80–89. [Google Scholar] [CrossRef] [PubMed]
- Murray, P.J.; Wynn, T.A. Protective and pathogenic functions of macrophage subsets. Nat. Rev. Immunol. 2011, 11, 723–737. [Google Scholar] [CrossRef] [PubMed]
- Zhou, P.; Xia, D.; Ni, Z.; Ou, T.; Wang, Y.; Zhang, H.; Mao, L.; Lin, K.; Xu, S.; Liu, J. Calcium silicate bioactive ceramics induce osteogenesis through oncostatin M. Bioact. Mater. 2021, 6, 810–822. [Google Scholar] [CrossRef] [PubMed]
- van Putten, S.M.; Ploeger, D.T.; Popa, E.R.; Bank, R.A. Macrophage phenotypes in the collagen-induced foreign body reaction in rats. Acta Biomater. 2013, 9, 6502–6510. [Google Scholar] [CrossRef]
- Lucke, S.; Hoene, A.; Walschus, U.; Kob, A.; Pissarek, J.W.; Schlosser, M. Acute and chronic local inflammatory reaction after implantation of different extracellular porcine dermis collagen matrices in rats. Biomed. Res. Int. 2015, 2015, 938059. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Target Gene | Sequence | Product Size (bp) | GeneBank Number |
|---|---|---|---|
| β-actin | Forward: GTGACGTTGACATCCGTAAAGA Reverse: GCCGGACTCATCGTACTCC | 245 | NM_007393 |
| IL-1β | Forward: GAAATGCCACCTTTTGACAGTG Reverse: TGGATGCTCTCATCAGGACAG | 116 | NM_008361 |
| IL-6 | Forward: CTGCAAGAGACTTCCATCCAG Reverse: AGTGGTATAGACAGGTCTGTTGG | 131 | NM_031168 |
| TNF-ɑ | Forward: CTGAACTTCGGGGTGATCGG Reverse: GGCTTGTCACTCGAATTTTGAGA | 122 | NM_013693 |
| IL-10 | Forward: AGCCTTATCGAAATGATCCAGT Reverse: GGCCTTGTAGACACCTTGGT | 229 | NM_010548 |
| MTA | iRoot SP | BC Sealer HiFlow | |||
|---|---|---|---|---|---|
| Element | Atomic% | Element | Atomic% | Element | Atomic% |
| C-K | 22.41 | O-K | 70.68 | O-K | 62.29 |
| O-K | 58.06 | - | - | - | - |
| Si-K | 0.66 | Si-K | 0.10 | Si-K | 0.10 |
| P-K | 0.64 | P-K | 2.85 | P-K | 7.25 |
| S-K | 0.23 | - | - | - | - |
| Ca-K | 18.00 | Ca-K | 6.24 | Ca-K | 12.24 |
| Zr-L | 0.00 | Zr-L | 20.13 | Zr-L | 18.12 |
| Totals | 100.00 | Totals | 100.00 | Totals | 100.00 |
| Material | Inflammatory Score * | Macrophage † | Necrosis # | ||||||
|---|---|---|---|---|---|---|---|---|---|
| 0 | 1 | 2 | 3 | 0 | 1 | 2 | 0 | 1 | |
| 7 days | |||||||||
| Control | 20.6 | 20.6 | 23.5 | 35.3 | 41.2 a | 47.1 a | 11.8 a | 61.8 | 38.2 |
| MTA | 8.8 | 8.8 | 35.3 | 47.1 | 17.6 b | 82.4 b | 0 b | 41.2 | 58.8 |
| iRoot SP | 5.9 | 11.8 | 41.2 | 41.2 | 17.6 a | 70.6 a | 11.8 a | 47.1 | 52.9 |
| BC Sealer HiFlow | 8.8 | 17.6 | 41.2 | 32.4 | 14.7 b | 85.3 b | 0 b | 50.0 | 50.0 |
| 30 days | |||||||||
| Control | 29.4 a | 38.2 a | 32.4 a | 0 a | 67.6 a | 32.4 a | 0 a | 88.2 a | 11.8 a |
| MTA | 34.8 a | 52.2 a | 13.0 a | 0 a | 80.4 a | 19.6 a | 0 a | 60.9 b | 39.1 b |
| iRoot SP | 14.7 à | 38.2 à | 47.1 à | 0 à | 91.1 a | 8.8 a | 0 a | 55.9 b | 44.1 b |
| BC Sealer HiFlow | 8.8 à | 44.1 à | 47.1 à | 0 à | 58.8 ã | 41.2 ã | 0 ã | 61.8 b | 38.2 b |
| 150 days | |||||||||
| Control | 68.9 a | 23.0 a | 8.2 a | 0 a | 68.9 a | 31.1 a | 0 a | 95.1 | 4.9 |
| MTA | 41.9 a | 48.8 a | 9.3 a | 0 a | 87.5 b | 12.5 b | 0 b | 95.8 | 4.2 |
| iRoot SP | 58.5 a | 37.7 a | 3.8 a | 0 a | 96.2 b | 3.8 b | 0 b | 83.0 | 17.0 |
| BC Sealer HiFlow | 73.7 à | 26.3 à | 0 à | 0 à | 97.4 b | 2.6 b | 0 b | 92.1 | 7.9 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yang, X.; Tian, J.; Li, M.; Chen, W.; Liu, H.; Wang, Z.; Haapasalo, M.; Shen, Y.; Wei, X. Biocompatibility of a New Calcium Silicate-Based Root Canal Sealer Mediated via the Modulation of Macrophage Polarization in a Rat Model. Materials 2022, 15, 1962. https://doi.org/10.3390/ma15051962
Yang X, Tian J, Li M, Chen W, Liu H, Wang Z, Haapasalo M, Shen Y, Wei X. Biocompatibility of a New Calcium Silicate-Based Root Canal Sealer Mediated via the Modulation of Macrophage Polarization in a Rat Model. Materials. 2022; 15(5):1962. https://doi.org/10.3390/ma15051962
Chicago/Turabian StyleYang, Xiaoqian, Jun Tian, Mengjie Li, Weiyang Chen, He Liu, Zhejun Wang, Markus Haapasalo, Ya Shen, and Xi Wei. 2022. "Biocompatibility of a New Calcium Silicate-Based Root Canal Sealer Mediated via the Modulation of Macrophage Polarization in a Rat Model" Materials 15, no. 5: 1962. https://doi.org/10.3390/ma15051962