
Influence of the Polymerization Modes on the Methacrylic Acid Release from Dental Light-Cured Materials—In Vitro Study
 , ,
, ,
Abstract
:1. Introduction
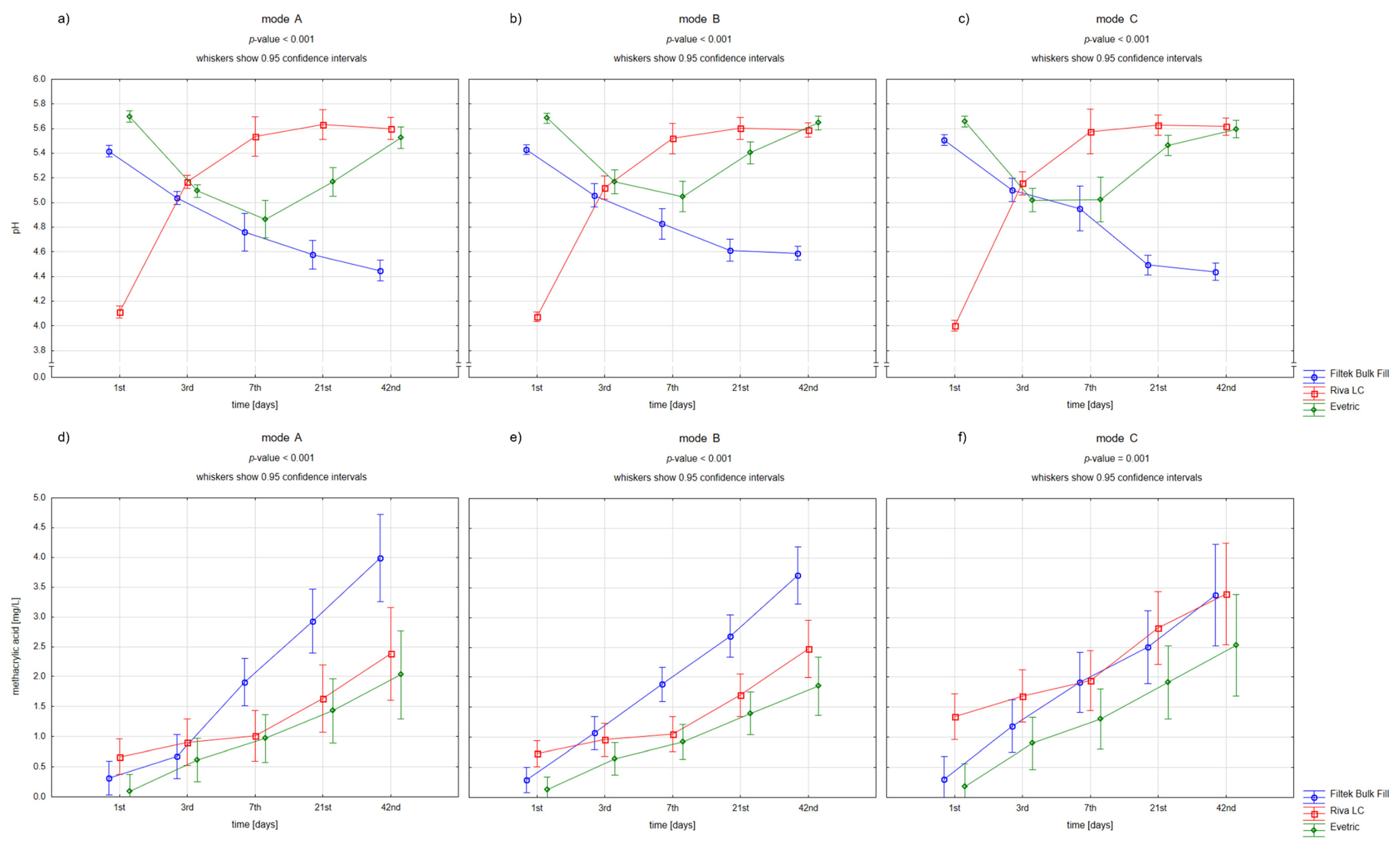
- Acidification around the filling correlates with the amount of methacrylic acid released.
- Polymerization mode affects the amount of methacrylic acid released.
- Selected materials acidify the environment more after the selected polymerization mode.
2. Materials and Methods
2.1. Materials Used in the Study
2.2. Specimen Preparation
- Full power mode (FPM), LED works in full power, 1000 mW/cm2
- Ramping mode (RM), LED turns from weak to stronger and reaches the highest power in 5 s
- Pulse mode (PM), LED pulsating between 850 mW/cm2–1000 mW/m2 in 2 s intervals.
2.3. Specimen Storage and pH Evaluation
2.4. High Performance Liquid Chromatography Analysis
2.5. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Demarco, F.F.; Corrêa, M.B.; Cenci, M.S.; Moraes, R.R.; Opdam, N.J.M. Longevity of Posterior Composite Restorations: Not Only a Matter of Materials. Dent. Mater. 2012, 28, 87–101. [Google Scholar] [CrossRef] [PubMed]
- Moraschini, V.; Fai, C.K.; Alto, R.M.; dos Santos, G.O. Amalgam and Resin Composite Longevity of Posterior Restorations: A Systematic Review and Meta-Analysis. J. Dent. 2015, 43, 1043–1050. [Google Scholar] [CrossRef] [PubMed]
- Ástvaldsdóttir, Á.; Dagerhamn, J.; van Dijken, J.W.V.; Naimi-Akbar, A.; Sandborgh-Englund, G.; Tranæus, S.; Nilsson, M. Longevity of Posterior Resin Composite Restorations in Adults—A Systematic Review. J. Dent. 2015, 43, 934–954. [Google Scholar] [CrossRef] [PubMed]
- Opdam, N.; van de Sande, F.; Bronkhorst, E.; Cenci, M.; Bottenberg, P.; Pallesen, U.; Gaengler, P.; Lindberg, A.; Huysmans, M.; Van Dijken, J. Longevity of Posterior Composite Restorations: A Systematic Review and Meta-Analysis. J. Dent. Res. 2014, 93, 943–949. [Google Scholar] [CrossRef] [Green Version]
- Nedeljkovic, I.; Teughels, W.; De Munck, J.; Van Meerbeek, B.; Van Landuyt, K.L. Is Secondary Caries with Composites a Material-Based Problem? Dent. Mater. Off. Publ. Acad. Dent. Mater. 2015, 31, e247–e277. [Google Scholar] [CrossRef]
- Galvão, M.R.; Caldas, S.G.F.R.; Bagnato, V.S.; de Souza Rastelli, A.N.; de Andrade, M.F. Evaluation of Degree of Conversion and Hardness of Dental Composites Photo-Activated with Different Light Guide Tips. Eur. J. Dent. 2013, 7, 86–93. [Google Scholar]
- Abed, Y.A.; Sabry, H.A.; Alrobeigy, N.A. Degree of Conversion and Surface Hardness of Bulk-Fill Composite versus Incremental-Fill Composite. Tanta Dent. J. 2015, 12, 71–80. [Google Scholar] [CrossRef]
- Lehmann, A.; Nijakowski, K.; Potempa, N.; Sieradzki, P.; Król, M.; Czyż, O.; Radziszewska, A.; Surdacka, A. Press-On Force Effect on the Efficiency of Composite Restorations Final Polishing—Preliminary In Vitro Study. Coatings 2021, 11, 705. [Google Scholar] [CrossRef]
- Lehmann, A.; Nijakowski, K.; Nowakowska, M.; Woś, P.; Misiaszek, M.; Surdacka, A. Influence of Selected Restorative Materials on the Environmental PH: In Vitro Comparative Study. Appl. Sci. 2021, 11, 11975. [Google Scholar] [CrossRef]
- Bansal, K.; Gupta, S.; Nikhil, V.; Jaiswal, S.; Jain, A.; Aggarwal, N. Effect of Different Finishing and Polishing Systems on the Surface Roughness of Resin Composite and Enamel: An In Vitro Profilometric and Scanning Electron Microscopy Study. Int. J. Appl. Basic Med. Res. 2019, 9, 154–158. [Google Scholar] [CrossRef]
- Freund, M.; Munksgaard, E.C. Enzymatic Degradation of BISGMA/TEGDMA-Polymers Causing Decreased Microhardness and Greater Wear in Vitro. Eur. J. Oral Sci. 1990, 98, 351–355. [Google Scholar] [CrossRef] [PubMed]
- Munksgaard, E.C.; Freund, M. Enzymatic Hydrolysis of (Di)Methacrylates and Their Polymers. Eur. J. Oral Sci. 1990, 98, 261–267. [Google Scholar] [CrossRef] [PubMed]
- Ilie, N. Degradation of Dental Methacrylate-Based Composites in Simulated Clinical Immersion Media. J. Funct. Biomater. 2022, 13, 25. [Google Scholar] [CrossRef] [PubMed]
- Yap, A.U.J.; Lee, H.K.; Sabapathy, R. Release of Methacrylic Acid from Dental Composites. Dent. Mater. 2000, 16, 172–179. [Google Scholar] [CrossRef]
- Schneider, T.R.; Hakami-Tafreshi, R.; Tomasino-Perez, A.; Tayebi, L.; Lobner, D. Effects of Dental Composite Resin Monomers on Dental Pulp Cells. Dent. Mater. J. 2019, 38, 579–583. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yoshinaga, K.; Yoshihara, K.; Yoshida, Y. Development of New Diacrylate Monomers as Substitutes for Bis-GMA and UDMA. Dent. Mater. Off. Publ. Acad. Dent. Mater. 2021, 37, e391–e398. [Google Scholar] [CrossRef] [PubMed]
- Wang, X.; Huyang, G.; Palagummi, S.V.; Liu, X.; Skrtic, D.; Beauchamp, C.; Bowen, R.; Sun, J. High Performance Dental Resin Composites with Hydrolytically Stable Monomers. Dent. Mater. Off. Publ. Acad. Dent. Mater. 2018, 34, 228–237. [Google Scholar] [CrossRef]
- Cândea Ciurea, A.; Şurlin, P.; Stratul, Ş.-I.; Soancă, A.; Roman, A.; Moldovan, M.; Barbu-Tudoran, L.; Pall, E. Evaluation of the Biocompatibility of Resin Composite-Based Dental Materials with Gingival Mesenchymal Stromal Cells. Microsc. Res. Tech. 2019, 82, 1768–1778. [Google Scholar] [CrossRef]
- Soancă, A.; Lupse, M.; Moldovan, M.; Pall, E.; Cenariu, M.; Roman, A.; Tudoran, O.; Surlin, P.; Șorițău, O. Applications of Inflammation-Derived Gingival Stem Cells for Testing the Biocompatibility of Dental Restorative Biomaterials. Ann. Anat. Anat. Anz. Off. Organ Anat. Ges. 2018, 218, 28–39. [Google Scholar] [CrossRef]
- Kraus, D.; Wolfgarten, M.; Enkling, N.; Helfgen, E.-H.; Frentzen, M.; Probstmeier, R.; Winter, J.; Stark, H. In-Vitro Cytocompatibility of Dental Resin Monomers on Osteoblast-like Cells. J. Dent. 2017, 65, 76–82. [Google Scholar] [CrossRef]
- Sigusch, B.W.; Völpel, A.; Braun, I.; Uhl, A.; Jandt, K.D. Influence of Different Light Curing Units on the Cytotoxicity of Various Dental Composites. Dent. Mater. Off. Publ. Acad. Dent. Mater. 2007, 23, 1342–1348. [Google Scholar] [CrossRef] [PubMed]
- Tseng, W.-Y.; Huang, C.-H.; Chen, R.-S.; Lee, M.-S.; Chen, Y.-J.; Rueggeberg, F.A.; Chen, M.-H. Monomer Conversion and Cytotoxicity of Dental Composites Irradiated with Different Modes of Photoactivated Curing. J. Biomed. Mater. Res. B Appl. Biomater. 2007, 83, 85–90. [Google Scholar] [CrossRef] [PubMed]
- Reis, A.F.; Vestphal, M.; do Amaral, R.C.; Rodrigues, J.A.; Roulet, J.-F.; Roscoe, M.G. Efficiency of Polymerization of Bulk-Fill Composite Resins: A Systematic Review. Braz. Oral Res. 2017, 31, e59. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ilie, N. Impact of Light Transmittance Mode on Polymerisation Kinetics in Bulk-Fill Resin-Based Composites. J. Dent. 2017, 63, 51–59. [Google Scholar] [CrossRef] [PubMed]
- de Camargo, E.J.; Moreschi, E.; Baseggio, W.; Cury, J.A.; Pascotto, R.C. Composite Depth of Cure Using Four Polymerization Techniques. J. Appl. Oral Sci. 2009, 17, 446–450. [Google Scholar] [CrossRef]
- Yap, A.U.; Ng, S.C.; Siow, K.S. Soft-Start Polymerization: Influence on Effectiveness of Cure and Post-Gel Shrinkage. Oper. Dent. 2001, 26, 260–266. [Google Scholar]
- dos Santos Sousa, G.; Guimarães, G.F.; Marcelino, E.; Rodokas, J.E.P.; de Oliveira Júnior, A.J.; Cesarino, I.; Leão, A.L.; dos Santos Riccardi, C.; Arjmand, M.; Simões, R.P. Shrinkage Stress and Temperature Variation in Resin Composites Cured via Different Photoactivation Methods: Insights for Standardisation of the Photopolymerisation. Polymers 2021, 13, 2065. [Google Scholar] [CrossRef]
- Xie, S.-X.; Song, L.; Yuca, E.; Boone, K.; Sarikaya, R.; VanOosten, S.K.; Misra, A.; Ye, Q.; Spencer, P.; Tamerler, C. Antimicrobial Peptide-Polymer Conjugates for Dentistry. ACS Appl. Polym. Mater. 2020, 2, 1134–1144. [Google Scholar] [CrossRef]
- Aalto-Korte, K.; Alanko, K.; Kuuliala, O.; Jolanki, R. Methacrylate and Acrylate Allergy in Dental Personnel. Contact Dermat. 2007, 57, 324–330. [Google Scholar] [CrossRef]
- Geurtsen, W. Biocompatibility of Resin-Modified Filling Materials. Crit. Rev. Oral Biol. Med. Off. Publ. Am. Assoc. Oral Biol. 2000, 11, 333–355. [Google Scholar] [CrossRef]
- Moharamzadeh, K.; Brook, I.M.; Scutt, A.M.; Thornhill, M.H.; Van Noort, R. Mucotoxicity of Dental Composite Resins on a Tissue-Engineered Human Oral Mucosal Model. J. Dent. 2008, 36, 331–336. [Google Scholar] [CrossRef] [PubMed]
- Song, F.V.; Yang, B.; Tommaso, D.D.; Donnan, R.S.; Chass, G.A.; Yada, R.Y.; Farrar, D.H.; Tian, K.V. Resolving Nanoscopic Structuring and Interfacial THz Dynamics in Setting Cements. Mater. Adv. 2022, 3, 4982–4990. [Google Scholar] [CrossRef]
- Thepveera, W.; Potiprapanpong, W.; Toneluck, A.; Channasanon, S.; Khamsuk, C.; Monmaturapoj, N.; Tanodekaew, S.; Panpisut, P. Rheological Properties, Surface Microhardness, and Dentin Shear Bond Strength of Resin-Modified Glass Ionomer Cements Containing Methacrylate-Functionalized Polyacids and Spherical Pre-Reacted Glass Fillers. J. Funct. Biomater. 2021, 12, 42. [Google Scholar] [CrossRef] [PubMed]
- Yoshikawa, T.; Morigami, M.; Sadr, A.; Tagami, J. Acceleration of Curing of Resin Composite at the Bottom Surface Using Slow-Start Curing Methods. Dent. Mater. J. 2013, 32, 999–1004. [Google Scholar] [CrossRef] [Green Version]
- Furness, A.; Tadros, M.Y.; Looney, S.W.; Rueggeberg, F.A. Effect of Bulk/Incremental Fill on Internal Gap Formation of Bulk-Fill Composites. J. Dent. 2014, 42, 439–449. [Google Scholar] [CrossRef]
- Durner, J.; Schrickel, K.; Watts, D.C.; Ilie, N. Determination of Homologous Distributions of BisEMA Dimethacrylates in Bulk-Fill Resin-Composites by GC–MS. Dent. Mater. 2015, 31, 473–480. [Google Scholar] [CrossRef]
- Lazarchik, D.A.; Hammond, B.D.; Sikes, C.L.; Looney, S.W.; Rueggeberg, F.A. Hardness Comparison of Bulk-Filled/Transtooth and Incremental-Filled/Occlusally Irradiated Composite Resins. J. Prosthet. Dent. 2007, 98, 129–140. [Google Scholar] [CrossRef]
- Jalalian, B.; Golkar, P.; Paktinat, A.; Ahmadi, E.; Panahande, S.A.; Omrani, L.R. Degree of Conversion of Resin-Modified Glass Ionomer Cement Containing Hydroxyapatite Nanoparticles. Front. Dent. 2019, 16, 415–420. [Google Scholar] [CrossRef]
- Potiprapanpong, W.; Thepveera, W.; Khamsuk, C.; Channasanon, S.; Tanodekaew, S.; Patntirapong, S.; Monmaturapoj, N.; Panpisut, P. Monomer Conversion, Dimensional Stability, Biaxial Flexural Strength, Ion Release, and Cytotoxicity of Resin-Modified Glass Ionomer Cements Containing Methacrylate-Functionalized Polyacids and Spherical Pre-Reacted Glass Fillers. Polymers 2021, 13, 2742. [Google Scholar] [CrossRef]
- Lang, O.; Kohidai, L.; Kohidai, Z.; Dobo-Nagy, C.; Csomo, K.B.; Lajko, M.; Mozes, M.; Keki, S.; Deak, G.; Tian, K.V.; et al. Cell Physiological Effects of Glass Ionomer Cements on Fibroblast Cells. Toxicol. In Vitro Int. J. Publ. Assoc. BIBRA 2019, 61, 104627. [Google Scholar] [CrossRef]
- Sideridou, I.D.; Achilias, D.S. Elution Study of Unreacted Bis-GMA, TEGDMA, UDMA, and Bis-EMA from Light-Cured Dental Resins and Resin Composites Using HPLC. J. Biomed. Mater. Res. B Appl. Biomater. 2005, 74B, 617–626. [Google Scholar] [CrossRef] [PubMed]
- Karayannidis, G.P.; Achilias, D.S.; Sideridou, I.D.; Bikiaris, D.N. Alkyd Resins Derived from Glycolized Waste Poly(Ethylene Terephthalate). Eur. Polym. J. 2005, 41, 201–210. [Google Scholar] [CrossRef]
- Sarkar, A.; Xu, F.; Lee, S. Human Saliva and Model Saliva at Bulk to Adsorbed Phases—Similarities and Differences. Adv. Colloid Interface Sci. 2019, 273, 102034. [Google Scholar] [CrossRef] [PubMed]
- Gittings, S.; Turnbull, N.; Henry, B.; Roberts, C.J.; Gershkovich, P. Characterisation of Human Saliva as a Platform for Oral Dissolution Medium Development. Eur. J. Pharm. Biopharm. 2015, 91, 16–24. [Google Scholar] [CrossRef]
- Cai, K.; Delaviz, Y.; Banh, M.; Guo, Y.; Santerre, J.P. Biodegradation of Composite Resin with Ester Linkages: Identifying Human Salivary Enzyme Activity with a Potential Role in the Esterolytic Process. Dent. Mater. Off. Publ. Acad. Dent. Mater. 2014, 30, 848–860. [Google Scholar] [CrossRef]
- Finer, Y.; Santerre, J.P. Influence of Silanated Filler Content on the Biodegradation of BisGMA/TEGDMA Dental Composite Resins. J. Biomed. Mater. Res. A 2007, 81, 75–84. [Google Scholar] [CrossRef]
- Cavalcante, L.M.; Ferraz, L.G.; Antunes, K.B.; Garcia, I.M.; Schneider, L.F.J.; Collares, F.M. Silane Content Influences Physicochemical Properties in Nanostructured Model Composites. Dent. Mater. Off. Publ. Acad. Dent. Mater. 2021, 37, e85–e93. [Google Scholar] [CrossRef]
- Wacławczyk, A.; Postek-Stefańska, L.; Pietraszewska, D.; Birkner, E.; Zalejska-Fiolka, J.; Wysoczańska-Jankowicz, I. TEGDMA and UDMA Monomers Released from Composite Dental Material Polymerized with Diode and Halogen Lamps. Adv. Clin. Exp. Med. 2018, 27, 469–476. [Google Scholar] [CrossRef]
- Granat, M.; Cieloszyk, J.; Kowalska, U.; Buczkowska-Radlińska, J.; Łagocka, R. Surface Geometry of Four Conventional Nanohybrid Resin-Based Composites and Four Regular Viscosity Bulk Fill Resin-Based Composites after Two-Step Polishing Procedure. BioMed Res. Int. 2020, 2020, 6203053. [Google Scholar] [CrossRef]
- Babina, K.; Polyakova, M.; Sokhova, I.; Doroshina, V.; Arakelyan, M.; Novozhilova, N. The Effect of Finishing and Polishing Sequences on The Surface Roughness of Three Different Nanocomposites and Composite/Enamel and Composite/Cementum Interfaces. Nanomaterials 2020, 10, 1339. [Google Scholar] [CrossRef]
- Dewaele, M.; Asmussen, E.; Peutzfeldt, A.; Munksgaard, E.C.; Benetti, A.R.; Finné, G.; Leloup, G.; Devaux, J. Influence of Curing Protocol on Selected Properties of Light-Curing Polymers: Degree of Conversion, Volume Contraction, Elastic Modulus, and Glass Transition Temperature. Dent. Mater. Off. Publ. Acad. Dent. Mater. 2009, 25, 1576–1584. [Google Scholar] [CrossRef] [PubMed]
- Dall’Magro, E.; Correr, A.B.; Costa, A.R.; Correr, G.M.; Consani, R.L.X.; Correr-Sobrinho, L.; Sinhoreti, M.A.C. Effect of Different Photoactivation Techniques on the Bond Strength of a Dental Composite. Braz. Dent. J. 2010, 21, 220–224. [Google Scholar] [CrossRef] [PubMed]
- Asmussen, E.; Peutzfeldt, A. Influence of Pulse-Delay Curing on Softening of Polymer Structures. J. Dent. Res. 2001, 80, 1570–1573. [Google Scholar] [CrossRef] [PubMed]
- Yap, A.U.J.; Wong, N.Y.; Siow, K.S. Composite Cure and Shrinkage Associated with High Intensity Curing Light. Oper. Dent. 2003, 28, 357–364. [Google Scholar] [PubMed]
- Ritter, A.V.; Fahl, N., Jr.; Vargas, M.; Maia, R.R. The Direct-Indirect Technique for Composite Restorations Revisited|Compendium. Available online: https://www.aegisdentalnetwork.com/cced/2017/06/the-direct-indirect-technique-for-composite-restorations-revisited (accessed on 16 November 2022).



{kind=link}
{kind=link}
| Material | Material Group | Manufacturer | Acronym | Composition | Lot Number |
|---|---|---|---|---|---|
| Filtek Bulk Fill, Shade A3 | Composite | 3M/ESPE, Seedfeld, Germany | FBF | Organic matrix: AUDMA, UDMA, 1,12-dodecane-DMA 20 nm silica; Filler fraction (wt%/vol%) 76.5/58.4, Fillers: 4–11 nm zirconia, ytterbium trifluoride filler consisting of agglomerate 100 nm particles | N867070 |
| Evetric, Shade A3 | Composite | Ivoclar Vivadent, Schaan, Liechtenstein | ER | Organic matrix: Bis–GMA, Bis–EMA, UDMA; Filler fraction (wt%/vol%) 80–81/55–57, Fillers: barium glass, ytterbium trifluoride, mixed oxide, copolymers (size 40–3000 nm) | Y20235 |
| Riva LC, Shade A3 | resin-modified glass ionomer cement | SDI Limited, Victoria, Australia | RLC | Liquid: polyacrylic acid 20–30%, tartaric acid 5–10%, HEMA 20–25%, dimethacrylic acid cross linker 10–25%, acid monomer 10–20% Powder: fluoroaminosilicate powder 95–100% | J2011171 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lehmann, A.; Nijakowski, K.; Drożdżyńska, A.; Przybylak, M.; Woś, P.; Surdacka, A. Influence of the Polymerization Modes on the Methacrylic Acid Release from Dental Light-Cured Materials—In Vitro Study. Materials 2022, 15, 8976. https://doi.org/10.3390/ma15248976
Lehmann A, Nijakowski K, Drożdżyńska A, Przybylak M, Woś P, Surdacka A. Influence of the Polymerization Modes on the Methacrylic Acid Release from Dental Light-Cured Materials—In Vitro Study. Materials. 2022; 15(24):8976. https://doi.org/10.3390/ma15248976
Chicago/Turabian StyleLehmann, Anna, Kacper Nijakowski, Agnieszka Drożdżyńska, Martyna Przybylak, Patryk Woś, and Anna Surdacka. 2022. "Influence of the Polymerization Modes on the Methacrylic Acid Release from Dental Light-Cured Materials—In Vitro Study" Materials 15, no. 24: 8976. https://doi.org/10.3390/ma15248976