

Impact of Dentistry Materials on Chemical Remineralisation/Infiltration versus Salivary Remineralisation of Enamel—In Vitro Study

 , , , , , ,
, , , , , ,  , and
, and
Abstract
:1. Introduction
- For incipient enamel lesions, the only recommendation is to modify the diet to increase the salivary pH, for remineralisation to occur as a natural process with the help of saliva;
- For a medium demineralisation lesion, the dentist can choose a treatment based on fluoride solutions; the studies show that fluoride therapy has very good results;
- For enamel demineralisation lesions (without loss of substance), remineralising fluoride therapy is no longer sufficient; in this case, it is necessary to infiltrate the enamel with low viscosity resin to stop the demineralisation process by obliteration of the pores. The diagnosis of demineralisation can be accurately performed in clinical practice with the help of a DiagnoDent laser diode.
2. Materials and Methods
2.1. Biological Material
2.2. Confocal Laser System Microscopy Analysis (CLSM)
2.3. Protocol Study 1
2.3.1. In Vitro Chemical Demineralisation
2.3.2. Infiltration of Demineralised Lesions with Fluor Protector (Fluor Protector, Ivoclar Vivadent)
2.3.3. Infiltration of Demineralisation Lesions with Icon, Low Viscosity Resin (Icon, DMG, Hamburg)
2.3.4. Infiltration of Demineralisation Lesion with Artificial Saliva of Basic pH 8
Preparation of the Artificial Saliva
2.4. Protocol Study 2: Salivary Demineralisation and Infiltration with Artificial Saliva
2.5. Macro Elemental Composition
2.6. Statistical Analysis
3. Results
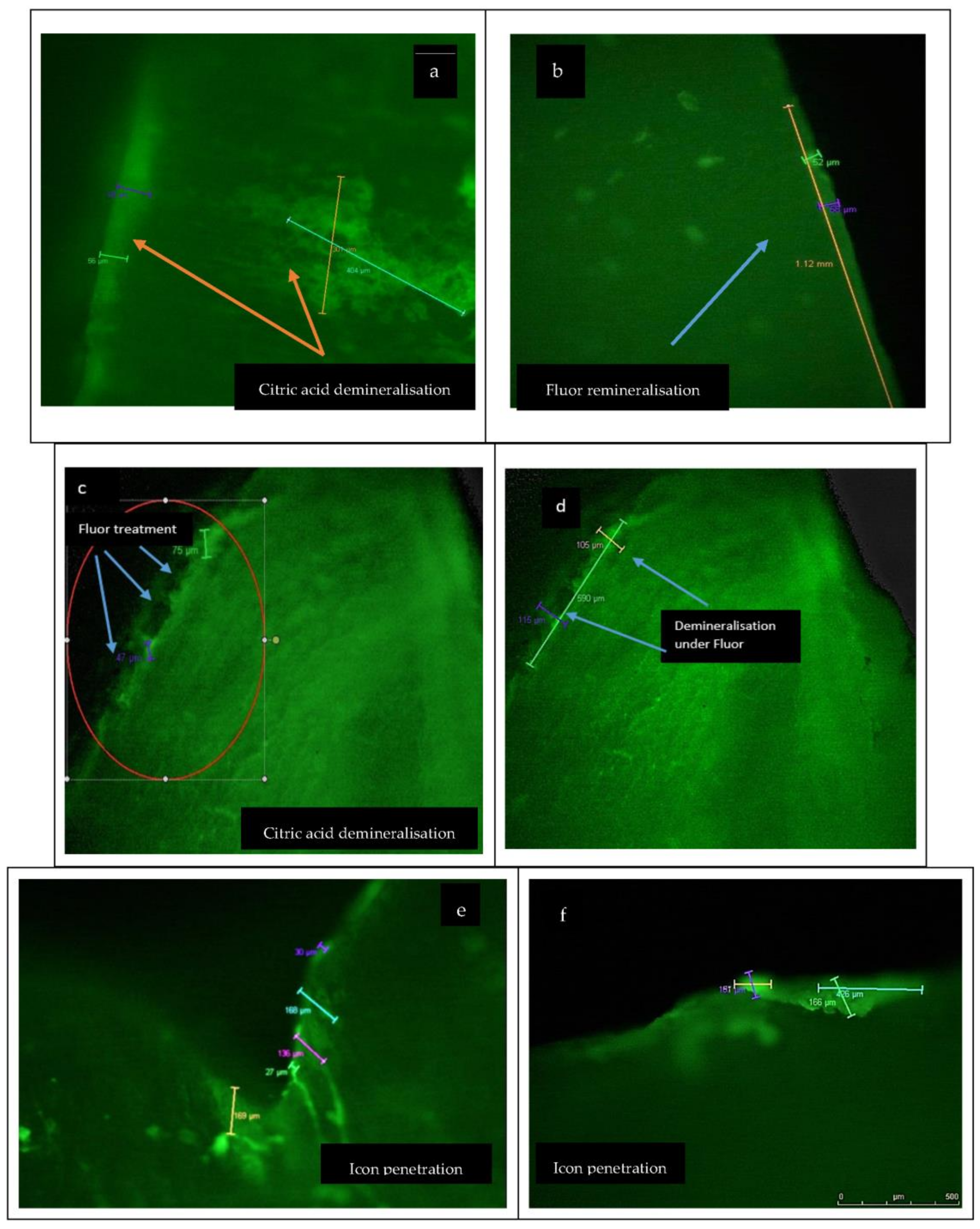
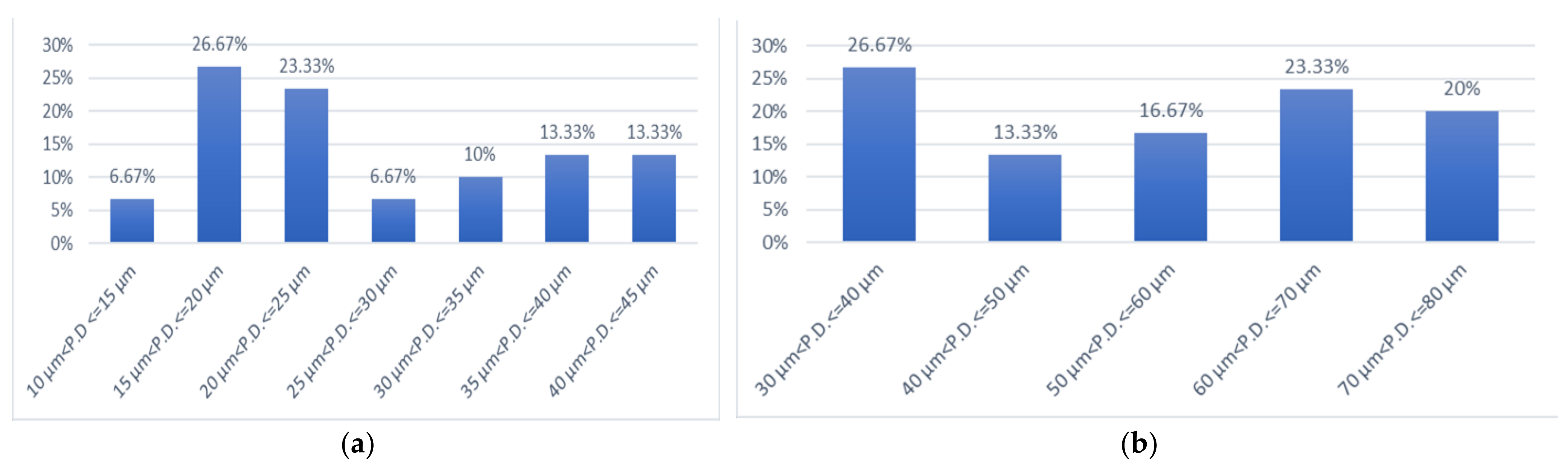
3.1. Chemical Demineralisation and Infiltration with Fluor Protect (Ivoclar Vivadent)
3.2. Salivary Demineralisation and Infiltration
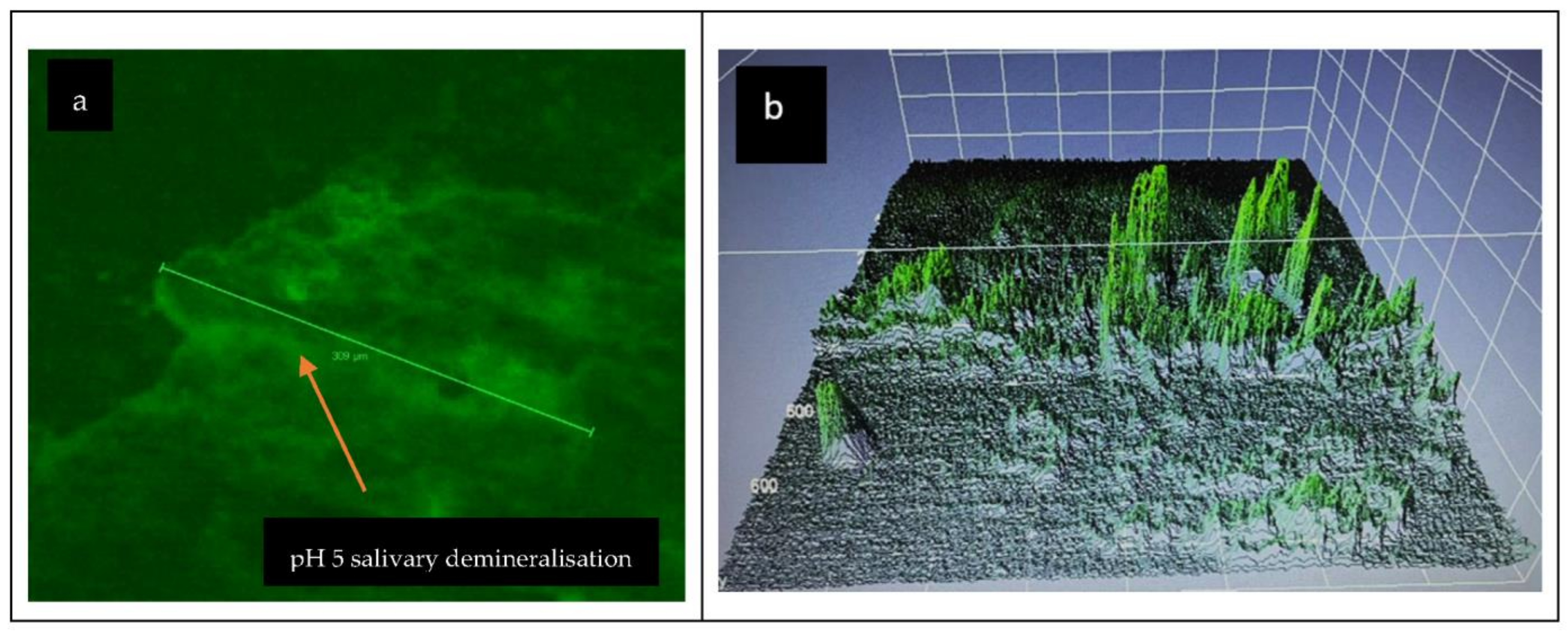
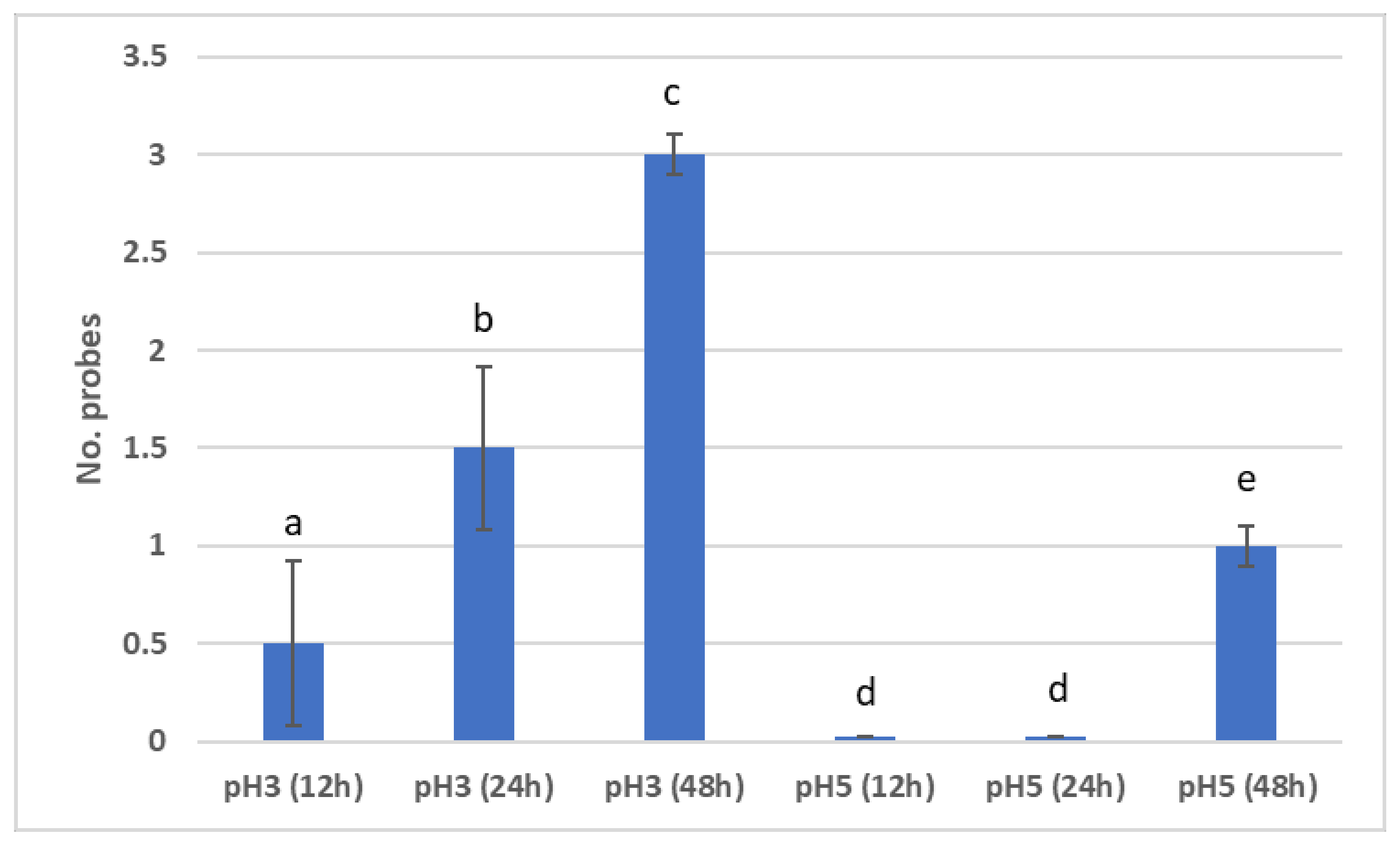
3.2.1. Demineralisation in Salivary Acid Medium
3.2.2. Remineralisation in Basic Salivary Medium
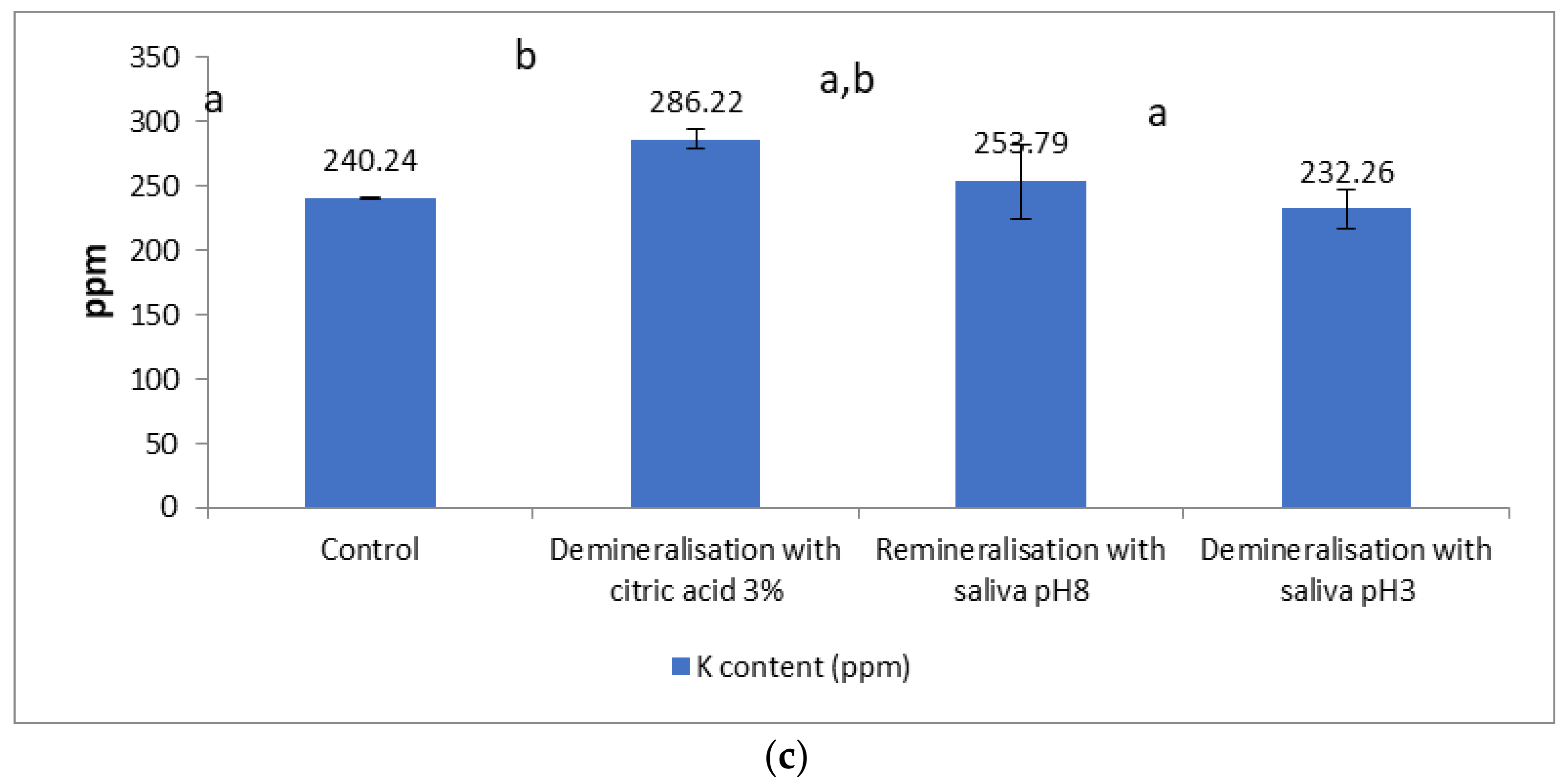
3.3. Macro Elemental Composition
4. Discussion
4.1. Chemical Demineralisation/Remineralisation
4.2. Salivary Demineralisation/Remineralisation
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Walsh, L.J. Preventive Dentistry for the General Dental Practitioner. Aust. Dent. J. 2000, 45, 76–82. [Google Scholar] [CrossRef] [PubMed]
- Moynihan, P. The Interrelationship between Diet and Oral Health. Proc. Nutr. Soc. 2005, 64, 571–580. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pathak, S.; Roopa, K.; Poornima, P.; Neena, I. White Spot Lesions: A Literature Review. J. Paediatr. Dent. 2015, 3, 1–7. [Google Scholar] [CrossRef]
- Lussi, A. Erosive Tooth Wear—A Multifactorial Condition of Growing Concern and Increasing Knowledge. In Monographs in Oral Science; Lussi, A., Ed.; Karger: Basel, Switzerland, 2006; Volume 20, pp. 1–8. ISBN 978-3-8055-8097-7. [Google Scholar]
- O’Toole, S.; Bernabé, E.; Moazzez, R.; Bartlett, D. Timing of Dietary Acid Intake and Erosive Tooth Wear: A Case-Control Study. J. Dent. 2017, 56, 99–104. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Buzalaf, M.A.; Hannas, A.R.; Kato, M.T. Saliva and dental erosion. J. Appl. Oral Sci. 2012, 20, 493–502. [Google Scholar] [CrossRef] [Green Version]
- Hicks, J.; Garcia-Godoy, F.; Flaitz, C. Biological Factors in Dental Caries: Role of Saliva and Dental Plaque in the Dynamic Process of Demineralization and Remineralization (Part 1). J. Clin. Pediatr. Dent. 2004, 28, 47–52. [Google Scholar] [CrossRef]
- Cao, C.; Mei, M.; Li, Q.; Lo, E.; Chu, C. Methods for Biomimetic Mineralisation of Human Enamel: A Systematic Review. Materials 2015, 8, 2873–2886. [Google Scholar] [CrossRef] [Green Version]
- Simmer, J.P.; Hardy, N.C.; Chinoy, A.F.; Bartlett, J.D.; Hu, J.C. How Fluoride Protects Dental Enamel from Demineralization. J. Int. Soc. Prev. Community Dent. 2020, 10, 134–141. [Google Scholar] [CrossRef]
- Prodan, D.; Moldovan, M.; Chisnoiu, A.M.; Saroși, C.; Cuc, S.; Filip, M.; Gheorghe, G.F.; Chisnoiu, R.M.; Furtos, G.; Cojocaru, I.; et al. Development of New Experimental Dental Enamel Resin Infiltrants—Synthesis and Characterization. Materials 2022, 15, 803. [Google Scholar] [CrossRef]
- Manoharan, V.; Arun Kumar, S.; Arumugam, S.B.; Anand, V.; Krishnamoorthy, S.; Methippara, J.J. Is Resin Infiltration a Microinvasive Approach to White Lesions of Calcified Tooth Structures? A Systemic Review. Int. J. Clin. Pediatr. Dent. 2019, 12, 53–58. [Google Scholar] [CrossRef]
- Arnold, W.H.; Meyer, A.-K.; Naumova, E.A. Surface Roughness of Initial Enamel Caries Lesions in Human Teeth After Resin Infiltration. Open Dent. J. 2016, 10, 505–515. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Paolone, G.; Moratti, E.; Goracci, C.; Gherlone, E.; Vichi, A. Effect of Finishing Systems on Surface Roughness and Gloss of Full-Body Bulk-Fill Resin Composites. Materials 2020, 13, 5657. [Google Scholar] [CrossRef] [PubMed]
- Rashid, H. Application of Confocal Laser Scanning Microscopy in Dentistry. J. Adv. Microsc. Res. 2014, 9, 245–252. [Google Scholar] [CrossRef]
- Alexa, V.T.; Szuhanek, C.; Cozma, A.; Galuscan, A.; Borcan, F.; Obistioiu, D.; Dehelean, C.A.; Jumanca, D. Natural Preparations Based on Orange, Bergamot and Clove Essential Oils and Their Chemical Compounds as Antimicrobial Agents. Molecules 2020, 25, 5502. [Google Scholar] [CrossRef] [PubMed]
- Alexa, V.T.; Galuscan, A.; Popescu, I.; Tirziu, E.; Obistioiu, D.; Floare, A.D.; Perdiou, A.; Jumanca, D. Synergistic/Antagonistic Potential of Natural Preparations Based on Essential Oils Against Streptococcus Mutans from the Oral Cavity. Molecules 2019, 24, 4043. [Google Scholar] [CrossRef] [Green Version]
- Arnold, W.H.; Haddad, B.; Schaper, K.; Hagemann, K.; Lippold, C.; Danesh, G. Enamel Surface Alterations after Repeated Conditioning with HCl. Head Face Med. 2015, 11, 32. [Google Scholar] [CrossRef] [Green Version]
- Péreza, R. Confocal Laser Microscopy Analysis of Resin Infiltration in Fluorotic Teeth. Revista Clínica de Periodoncia Implantología y Rehabilitación Oral 2014, 7, 53–58. [Google Scholar] [CrossRef]
- Eslami, S.; Faber, J.; Fateh, A.; Sheikholaemmeh, F.; Grassia, V.; Jamilian, A. Treatment Decision in Adult Patients with Class III Malocclusion: Surgery versus Orthodontics. Prog. Orthod. 2018, 19, 28. [Google Scholar] [CrossRef] [Green Version]
- Meyer-Lueckel, H.; Chatzidakis, A.; Naumann, M.; Dörfer, C.E.; Paris, S. Influence of Application Time on Penetration of an Infiltrant into Natural Enamel Caries. J. Dent. 2011, 39, 465–469. [Google Scholar] [CrossRef]
- Enan, E.T.; Aref, N.S.; Hammad, S.M. Resistance of Resin-infiltrated Enamel to Surface Changes in Response to Acidic Challenge. J. Esthet. Restor. Dent. 2019, 31, 353–358. [Google Scholar] [CrossRef]
- Chokshi, K. An in Vitro Comparative Evaluation of Three Remineralizing Agents Using Confocal Microscopy. JCDR 2016, 10, ZC39. [Google Scholar] [CrossRef] [PubMed]
- Zhang, J.; Lynch, R.J.M.; Watson, T.F.; Banerjee, A. Remineralisation of Enamel White Spot Lesions Pre-Treated with Chitosan in the Presence of Salivary Pellicle. J. Dent. 2018, 72, 21–28. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Meyer-Lueckel, H.; Paris, S. Infiltration of Natural Caries Lesions with Experimental Resins Differing in Penetration Coefficients and Ethanol Addition. Caries Res. 2010, 44, 408–414. [Google Scholar] [CrossRef] [PubMed]
- Dinu, M.; Tarcolea, M.; Cojocaru, M.; Gherghilescu, A.I.; Cotrut, C.M. Influence of ph value and NaF addition on the corrosion behavior of Ni + Cr and Co + Cr dental alloys. UPB Sci. Bull. Ser. B 2015, 77, 10. [Google Scholar]
- Farhadian, N.; Miresmaeili, A.; Eslami, B.; Mehrabi, S. Effect of Fluoride Varnish on Enamel Demineralization around Brackets: An in-Vivo Study. Am. J. Orthod. Dentofac. Orthop. 2008, 133, S95–S98. [Google Scholar] [CrossRef] [PubMed]
- Evrenol, B.I.; Kucukkeles, N.; Arun, T.; Yarat, A. Fluoride Release Capacities of Four Different Orthodontic Adhesives. J. Clin. Pediatr. Dent. 1999, 23, 315–319. [Google Scholar]
- García-Godoy, F.; Hicks, M.J. Maintaining the Integrity of the Enamel Surface. J. Am. Dent. Assoc. 2008, 139, 25S–34S. [Google Scholar] [CrossRef]
- De Leeuw, N.H. Resisting the Onset of Hydroxyapatite Dissolution through the Incorporation of Fluoride. J. Phys. Chem. B 2004, 108, 1809–1811. [Google Scholar] [CrossRef]
- Epple, M.; Enax, J.; Meyer, F. Prevention of Caries and Dental Erosion by Fluorides—A Critical Discussion Based on Physico-Chemical Data and Principles. Dent. J. 2022, 10, 6. [Google Scholar] [CrossRef]
- Ludovichetti, F.S.; Zambon, G.; Cimolai, M.; Gallo, M.; Signoriello, A.G.; Pezzato, L.; Bertolini, R.; Mazzoleni, S. Efficacy of Two Toothpaste in Preventing Tooth Erosive Lesions Associated with Gastroesophageal Reflux Disease. Appl. Sci. 2022, 12, 1023. [Google Scholar] [CrossRef]
- Cazzolla, A.P.; De Franco, A.R.; Lacaita, M.; Lacarbonara, V. Efficacy of 4-year treatment of icon infiltration resin on postorthodontic white spot lesions. Case Rep. 2018, 2018, bcr-2018-225639. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Abdel-Hakim, S.M.; Metwalli, N.; El-Askary, F.; Wasse, M.O. Microhardness, sem and color change analysis of artificial enamel lesions in primary teeth treated with resin infiltration, cpp-acp or fluoride gel: An in vitro study. Dent. J. 2016, 62, 3744. [Google Scholar]
- Subramaniam, P.; Girish Babu, K.; Lakhotia, D. Evaluation of Penetration Depth of a Commercially Available Resin Infiltrate into Artificially Created Enamel Lesions: An in Vitro Study. J. Conserv. Dent. 2014, 17, 146. [Google Scholar] [CrossRef] [PubMed]
- Klaisiri, A.; Janchum, S.; Wongsomtakoon, K.; Sirimanathon, P.; Krajangta, N. Microleakage of Resin Infiltration in Artificial White-Spot Lesions. J. Oral Sci. 2020, 62, 427–429. [Google Scholar] [CrossRef] [PubMed]
- Gherlone, E.; Polizzi, E.; Tetè, G.; Capparè, P. Dentistry and Covid-19 Pandemic: Operative Indications Post-Lockdown. New Microbiol. 2021, 44, 1–11. [Google Scholar]
- Voronets, J.; Jaeggi, T.; Buergin, W.; Lussi, A. Controlled Toothbrush Abrasion of Softened Human Enamel. Caries Res. 2008, 42, 286–290. [Google Scholar] [CrossRef]
- Lopes, R.M.; da Silva, J.S.A.; João-Souza, S.H.; Maximiano, V.; Machado, A.C.; Scaramucci, T.; Aranha, A.C.C. Enamel Surface Loss after Erosive and Abrasive Cycling with Different Periods of Immersion in Human Saliva. Arch. Oral Biol. 2020, 109, 104549. [Google Scholar] [CrossRef]
- Milosevic, A.; Lennon, M.A.; Fear, S.C. Risk Factors Associated with Tooth Wear in Teenagers: A Case Control Study. Community Dent. Health 1997, 14, 143–147. [Google Scholar]
- Moazzez, R.; Smith, B.G.N.; Bartlett, D.W. Oral PH and Drinking Habit during Ingestion of a Carbonated Drink in a Group of Adolescents with Dental Erosion. J. Dent. 2000, 28, 395–397. [Google Scholar] [CrossRef]
- Hans, R.; Thomas, S.; Garla, B.; Dagli, R.J.; Hans, M.K. Effect of Various Sugary Beverages on Salivary PH, Flow Rate, and Oral Clearance Rate amongst Adults. Scientifica 2016, 2016, 5027283. [Google Scholar] [CrossRef] [Green Version]
- Mutahar, M.; Carpenter, G.; Bartlett, D.; German, M.; Moazzez, R. The Presence of Acquired Enamel Pellicle Changes Acid-Induced Erosion from Dissolution to a Softening Process. Sci. Rep. 2017, 7, 10920. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wetton, S.; Hughes, J.; West, N.; Addy, M. Exposure Time of Enamel and Dentine to Saliva for Protection against Erosion: A Study in Vitro. Caries Res. 2006, 40, 213–217. [Google Scholar] [CrossRef] [PubMed]
- Bartlett, D.W.; Lussi, A.; West, N.X.; Bouchard, P.; Sanz, M.; Bourgeois, D. Prevalence of Tooth Wear on Buccal and Lingual Surfaces and Possible Risk Factors in Young European Adults. J. Dent. 2013, 41, 1007–1013. [Google Scholar] [CrossRef] [PubMed]
- Hannig, C.; Hannig, M.; Attin, T. Enzymes in the Acquired Enamel Pellicle. Eur. J. Oral Sci. 2005, 113, 2–13. [Google Scholar] [CrossRef] [PubMed]
- Aljulayfi, I.; O’Toole, S.; Healy, M.; Sumaidaa, S.; Ali, Z.; Bartlett, D.; Austin, R. The Interplay of Saliva, Erosion and Attrition on Enamel and Dentine. Saudi Dent. J. 2022, 34, 232–236. [Google Scholar] [CrossRef]
- McCarl, C.-A.; Picard, C.; Khalil, S.; Kawasaki, T.; Röther, J.; Papolos, A.; Kutok, J.; Hivroz, C.; LeDeist, F.; Plogmann, K.; et al. ORAI1 Deficiency and Lack of Store-Operated Ca2+ Entry Cause Immunodeficiency, Myopathy, and Ectodermal Dysplasia. J. Allergy Clin. Immunol. 2009, 124, 1311–1318.e7. [Google Scholar] [CrossRef] [Green Version]
- Smith, C.E. Cellular and Chemical Events During Enamel Maturation. Crit. Rev. Oral Biol. Med. 1998, 9, 128–161. [Google Scholar] [CrossRef]
- Takano, Y. Enamel Mineralization and the Role of Ameloblasts in Calcium Transport. Connect. Tissue Res. 1995, 33, 127–137. [Google Scholar] [CrossRef]
- Eckstein, M.; Lacruz, R.S. CRAC Channels in Dental Enamel Cells. Cell Calcium 2018, 75, 14–20. [Google Scholar] [CrossRef]
- West, N.X.; Hughes, J.A.; Addy, M. The Effect of PH on the Erosion of Dentine and Enamel by Dietary Acids in Vitro: Dentine and enamel erosion by dietary acids. J. Oral Rehabil. 2008, 28, 860–864. [Google Scholar] [CrossRef]
- Lussi, A.; Schlueter, N.; Rakhmatullina, E.; Ganss, C. Dental Erosion—An Overview with Emphasis on Chemical and Histopathological Aspects. Caries Res. 2011, 45, 2–12. [Google Scholar] [CrossRef] [PubMed]
- Gilbert, J.; Schoolfield, J. The Outcome Index and System Outcome Score: A Method of Quality Assurance through Outcome Analysis in the Special Care Area. J. Clin. Monit. Comput. 1991, 8, 85–94. [Google Scholar] [CrossRef] [PubMed]
- Manazza, F. A Simplified Digital Workflow for the Prosthetic Finishing of Implant Rehabilitations: A Case Report. J. Biol. Regul. Homeost. Agents 2021, 35 (Suppl. S1), 87–97. [Google Scholar] [CrossRef]
- Ferrari Cagidiaco, E.; Carboncini, F.; Parrini, S.; Doldo, T.; Nagni, M.; Uti, N.; Ferrari, M. Functional Implant Prosthodontic Score of a One-Year Prospective Study on Three Different Connections for Single-Implant Restorations. J. Osseointegr. 2018, 10, 130–135. [Google Scholar] [CrossRef]















{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Citric Acid 3% at Room Temperature | 3 min Immersion | 5 min Immersion | 7 min Immersion |
|---|---|---|---|
| Washing distilled water | 30 s | 30 s | 30 s |
| Demineralisation lesion (CLSM) | Absence | Initiated | Present |
| Procedure | Penetration Depth (μm) Before Procedure | Penetration Depth (μm) After Procedure | ||
|---|---|---|---|---|
| Mean ± Std. Dev | Min.–Max Values | Mean ± Std. Dev | Min.–Max Values | |
| Infiltration with Fluor Protector (Ivoclar Vivadent) | 115 ± 21.72 | 87–143 | 77 ± 5.08 | 64–81 |
| Infiltration with Icon resin infiltration (DMG) | 115 ± 20.41 | 90–141 | 115 ± 20.41 | 90–141 |
| Infiltration with artificial saliva with pH 8 | 118 ± 19.23 | 94–145 | 39 ± 5.99 | 30–45 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Damian, L.-R.; Dumitrescu, R.; Alexa, V.T.; Focht, D.; Schwartz, C.; Balean, O.; Jumanca, D.; Obistioiu, D.; Lalescu, D.; Stefaniga, S.-A.; et al. Impact of Dentistry Materials on Chemical Remineralisation/Infiltration versus Salivary Remineralisation of Enamel—In Vitro Study. Materials 2022, 15, 7258. https://doi.org/10.3390/ma15207258
Damian L-R, Dumitrescu R, Alexa VT, Focht D, Schwartz C, Balean O, Jumanca D, Obistioiu D, Lalescu D, Stefaniga S-A, et al. Impact of Dentistry Materials on Chemical Remineralisation/Infiltration versus Salivary Remineralisation of Enamel—In Vitro Study. Materials. 2022; 15(20):7258. https://doi.org/10.3390/ma15207258
Chicago/Turabian StyleDamian, Lia-Raluca, Ramona Dumitrescu, Vlad Tiberiu Alexa, David Focht, Cristoph Schwartz, Octavia Balean, Daniela Jumanca, Diana Obistioiu, Dacian Lalescu, Sebastian-Aurelian Stefaniga, and et al. 2022. "Impact of Dentistry Materials on Chemical Remineralisation/Infiltration versus Salivary Remineralisation of Enamel—In Vitro Study" Materials 15, no. 20: 7258. https://doi.org/10.3390/ma15207258