
3D Printing of Customizable Phantoms to Replace Cadaveric Models in Upper Extremity Surgical Residency Training


Abstract
:1. Introduction
2. Materials and Methods
2.1. Periosteum
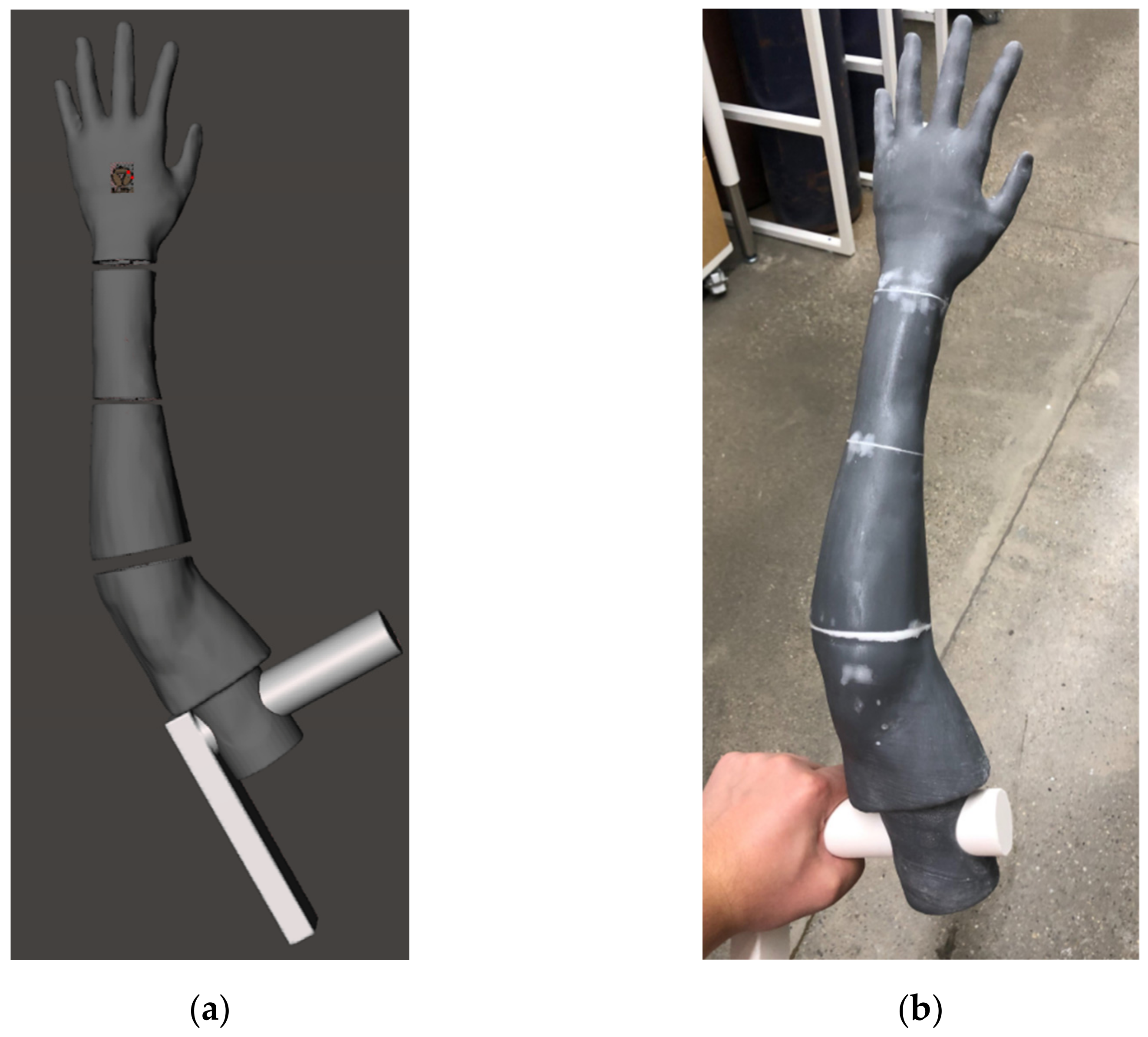
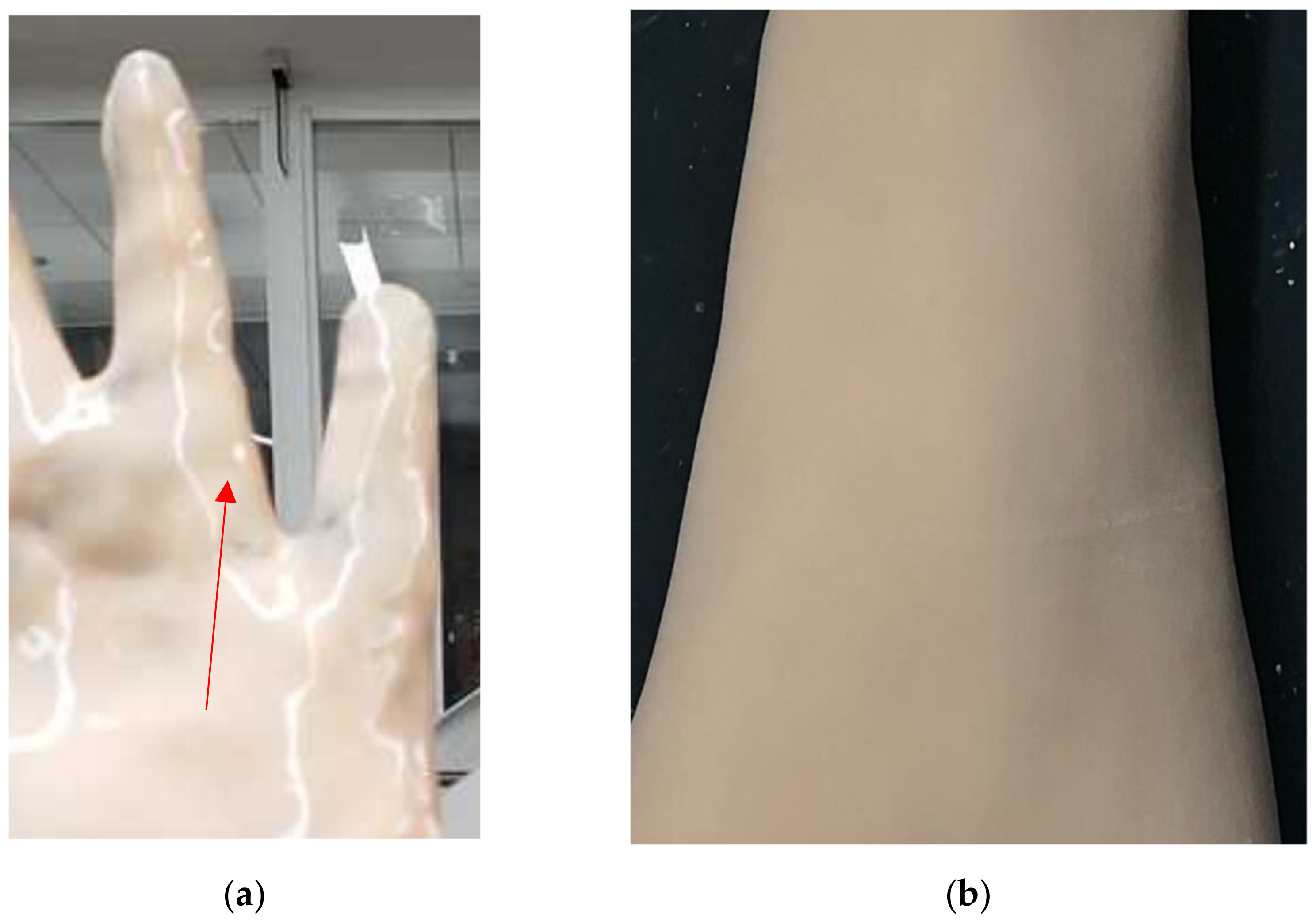
2.2. Opaque Skin Covering
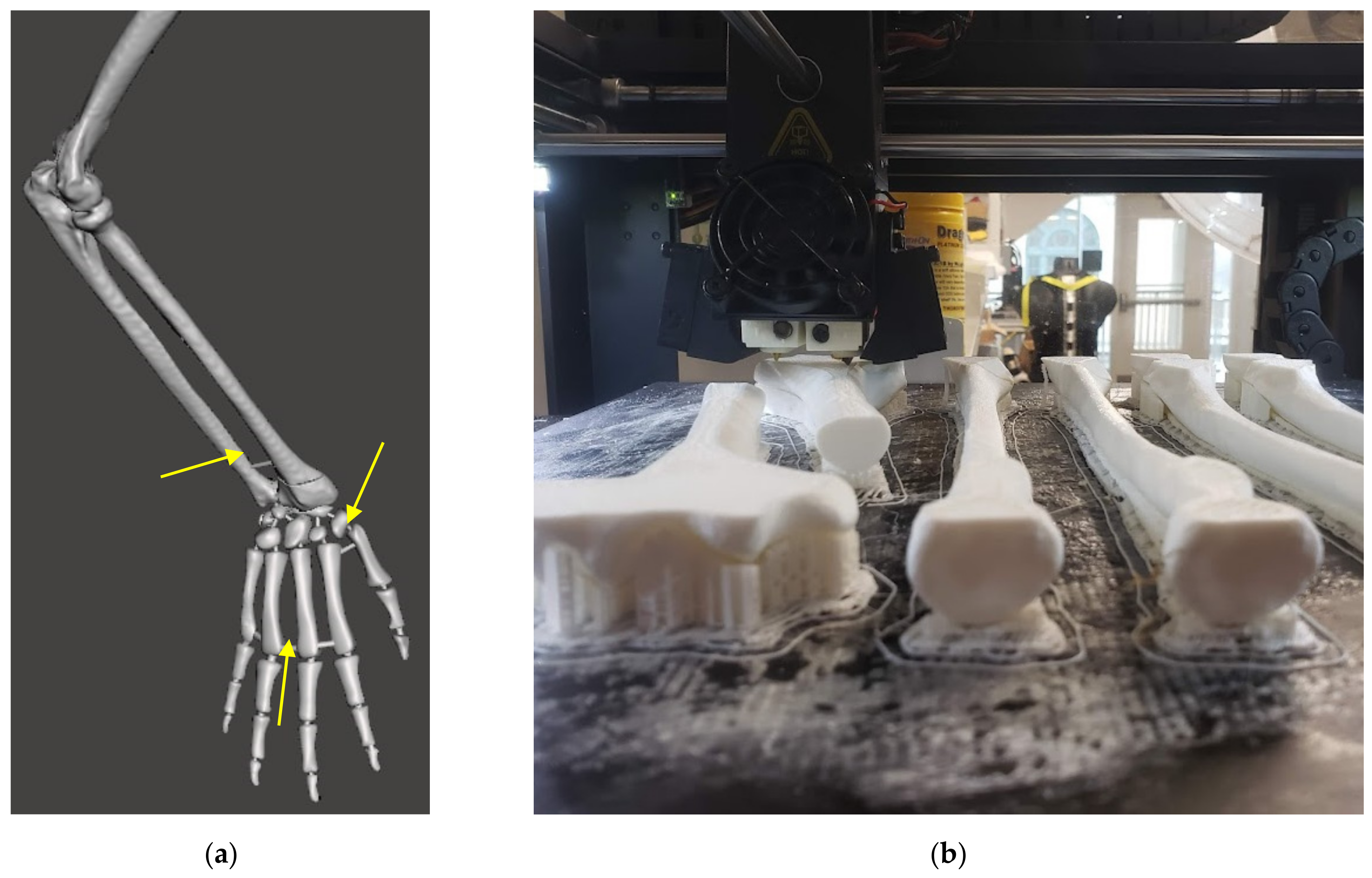
2.3. Extended Phantom Skeleton
2.4. Medical Imaging
3. Results
4. Discussion
4.1. Current Limitations
4.2. Future Work
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
1. Identify the tendon(s) most likely to rupture as a result of closed reduction and casting of a distal radius fracture. | 2. On the figure below, draw how you would measure radial height and inclination (use an x to indicate the radial height and an α to indicate radial inclination). |
3. What is the acceptable maximum amount of radial shortening for non-operative management of a distal radius fracture (DRF) according to the AAOS clinical practice guidelines?
| 4. What is the maximum accepted dorsal angulation, from neutral, for non-operative management of a DRF according to the AAOS clinical practice guidelines?
|
5. What is the maximum acceptable amount of articular displacement for non-operative management of a DRF according to the AAOS clinical practice guidelines?
| 6. Which of the following has been associated with loss of reduction and re-displacement following closed reduction of a DRF?
|
7. Which of the following is a contraindication to isolated closed reduction and percutaneous pinning of a DRF?
| 8. What is considered normal radial inclination?
|
9. A polytrauma patient presents to the ED following a motorcycle collision with a distal radius fracture. What is the risk of acute carpal tunnel syndrome in this patient after reduction and splinting?
| 10. A patient has symptoms suggestive of acute carpal tunnel syndrome following a DRF and you are going to the operating room to release their carpal tunnel. Your planned approach to allow for carpal tunnel release may include:
|
11. A patient presented to the ED with a DRF from a ground-level fall. The DRF was closed reduced by an on-call resident. After discharge from the ED the patient calls your office with a complaint of worsening pain and progressive loss of sensation in the thumb and index finger. What splinting position could have put this patient at increased risk to develop this complication and what is the incidence of this complication occurring in this setting?
| 12. A 75-year-old woman has a DRF that is closed reduced and casted in the ED. She is in acceptable alignment and is managed non-operatively. At her 6-week follow up she cannot actively extend her thumb. What is the etiology of this new finding and how should it be managed?
|
13. Which of the following factors has been found to significantly impact the DASH score in patients who undergo non-operative management of DRFs?
| 14. While reducing a grossly unstable DRF, you find that supinating the arm lessens re-displacement of your reduction. In the below figure, identify and name the muscle that was contributing to re-displacement of your reduction and which was neutralized by supination. |
15. You are considering multi-planar external fixation versus non-operative management of a DRF in a 68-year-old male. When counseling this patient, which of the following is true regarding external fixation?
| |
References
- Raeker-Jordan, E.A.; Martinez, M.; Aziz, K.T.; Miles, M.R.; Means, K.R.; LaPorte, D.M.; Giladi, A.M.; Shimada, K. High-Fidelity Wrist Fracture Phantom as a Training Tool to Develop Competency in Orthopaedic Surgical Trainees. JAAOS Glob. Res. Rev. 2021, 5, e20.00224-8. [Google Scholar] [CrossRef] [PubMed]
- Henry, B.; Clark, P.; Sudan, R. Cost and Logistics of Implementing a Tissue-Based American College of Surgeons/Association of Program Directors in Surgery Surgical Skills Curriculum for General Surgery Residents of All Clinical Years. Am. J. Surg. 2014, 207, 201–208. [Google Scholar] [CrossRef] [PubMed]
- Jackson, T.J.; Shah, A.S.; Buczek, M.J.; Lawrence, J.T.R. Simulation Training of Orthopaedic Residents for Distal Radius Fracture Reductions Improves Radiographic Outcomes. J. Pediatr. Orthop. 2020, 40, e6–e13. [Google Scholar] [CrossRef] [PubMed]
- Nigicser, I.; Szabo, B.; Jaksa, L.; Nagy, D.A.; Garamvolgyi, T.; Barcza, S.; Galambos, P.; Haidegger, T. Anatomically Relevant Pelvic Phantom for Surgical Simulation. In Proceedings of the 2016 7th IEEE International Conference on Cognitive Infocommunications (CogInfoCom), Wroclaw, Poland, 16–18 October 2016. [Google Scholar] [CrossRef]
- Brenner, E. Human body preservation—Old and new techniques. J. Anat. 2014, 224, 316–344. [Google Scholar] [CrossRef] [PubMed]
- Klingensmith, M.E.; Lewis, F.R. General Surgery Residency Training Issues. Adv. Surg. 2013, 47, 251–270. [Google Scholar] [CrossRef] [PubMed]
- Matson, A.M. Orthopedic Review: Distal Radius Fracture Reduction. In Brown Emergency Medicine; 26 October 2015. Available online: Blogs.brown.edu/emergency-medicine-residency/orthopedic-review-distal-radius-fracture-reduction/ (accessed on 20 November 2021).
- Akhtar, K.S.N.; Chen, A.; Standfield, N.J.; Gupte, C.M. The Role of Simulation in Developing Surgical Skills. Curr. Rev. Musculoskelet. Med. 2014, 7, 155–160. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Aldridge, M. Defining and Exploring Clinical Skills and Simulation-Based Education. In Developing Healthcare Skills through Simulation; SAGE Publications, Inc.: Los Angeles, CA, USA, 2013; pp. 3–17. [Google Scholar] [CrossRef]
- Seeley, M.A.; Fabricant, P.; Lawrence, J.T.R. Teaching the Basics: Development and Validation of a Distal Radius Reduction and Casting Model. Clin. Orthop. Relat. Res. 2017, 475, 2298–2305. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Arm with Clamping Post for Casting, Pediatric Sawbones. Available online: www.sawbones.com/arm-pediatric-for-casting-includes-proximal-clamping-post-1530-13-2.html (accessed on 20 November 2021).
- Peripheral Doppler Ultrasound Training Model. Blue Phantom. Available online: www.bluephantom.com/product/Peripheral-Doppler-Ultrasound-Training-Model.aspx?cid=496 (accessed on 20 November 2021).
- Michaud, M. Creating the ‘Model Human’ to Practice Surgery. URMC Newsroom, URMC Newsroom, 6 August 2020. Available online: https://www.urmc.rochester.edu/news/story/creating-the-model-human-to-practice-surgery (accessed on 20 November 2021).
- Meshmixer Is State-of-the-Art Software for Working with Triangle Meshes. Autodesk Meshmixer. Available online: https://www.meshmixer.com/ (accessed on 20 November 2021).
- Wu, Y.Y.; Rajaraman, M.; Guth, J.; Salopek, T.; Altman, D.; Sangimino, M.; Shimada, K. A High-Fidelity Tactile Hand Simulator as a Training Tool to Develop Competency in Percutaneous Pinning in Residents. JAAOS Glob. Res. Rev. 2018, 2, e028. [Google Scholar] [CrossRef] [PubMed]
- Arm, Solid Foam, Right. Sawbones. Available online: www.sawbones.com/arm-large-right-foam-cortical-shell-w-cancellous-humerus-hand-1024-49.html (accessed on 20 November 2021).
- Raise3D Pro2 Plus. Raise3D. Available online: https://www.raise3d.com/pro2-series/ (accessed on 20 November 2021).
- Researchers Optimize Robust, Lightweight, Bone-Inspired 3D Printing Infill—3dprint.Com: The Voice of 3D Printing/Additive Manufacturing. 3DPrint, 19 October 2021. Available online: https://3dprint.com/165006/3d-printed-bone-infill/ (accessed on 20 November 2021).
- FormLabs Form2. FormLabs. Available online: https://formlabs.com/3d-printers/form-3/ (accessed on 20 November 2021).
- Fluoroscopy Better than X-rays in Diagnosing Certain Wrist Conditions. Maimonides Bone and Joint Center, 7 Jane 2019. Available online: https://www.orthobrooklyn.com/blog/fluoroscopy-better-than-x-rays-in-diagnosing-certain-wrist-conditions-14562.html (accessed on 20 November 2021).
- Tahmasebi, A.M.; Hashtrudi-Zaad, K.; Thompson, D.; Abolmaesumi, P. A Framework for the Design of a Novel Haptic-Based Medical Training Simulator. IEEE Trans. Inf. Technol. Biomed. 2008, 12, 658–666. [Google Scholar] [CrossRef] [PubMed]
- OSATS. C-SATS. Available online: https://www.csats.com/osats (accessed on 20 November 2021).
- Psychology: Motivation and Learning. GSI Teaching Resource Center. Available online: https://gsi.berkeley.edu/gsi-guide-contents/learning-theory-research/motivation/ (accessed on 20 November 2021).
- Pontius, J.L.; Harper, S.R. Principles for good practice in graduate and professional student engagement. New Dir. Stud. Serv. 2006, 2006, 47–58. [Google Scholar] [CrossRef]
- Simple Measures—Arm Anthropometry. DAPA Measurement Toolkit; National Institute for Health Research: London, UK. Available online: https://dapa-toolkit.mrc.ac.uk/anthropometry/objective-methods/simple-measures-muac (accessed on 20 November 2021).












| Subject 1 | Subject 2 | Subject 3 | Subject 4 | |
|---|---|---|---|---|
| Check List Grader #1 (0–12) | 7 | 5 | 5 | 7 |
| Check List Grader #2 (0–12) | 6 | 6 | 4 | 8 |
| Radial Inclination (deg) | 4 | 12 | 3 | 18 |
| Volar Tilt (deg) | 8 | 0 | −2 | 7 |
| Procedure Time (min) | 21.18 | 36.24 | 26.34 | 18.28 |
| Procedure Rating #1 (1–5) | 3.14 | 2.14 | 2.29 | 3.57 |
| Procedure Rating #2 (1–5) | 3.71 | 2.00 | 2.43 | 3.86 |
| Written Assessment (0–15) | 10 | 5 | 7 | 12 |
| Pass/Fail | Pass | Fail | Fail | Pass |
| Impression of the phantom (Likert 1–5) | 5 | 5 | 5 | 5 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Raeker-Jordan, E.; Martinez, M.; Shimada, K. 3D Printing of Customizable Phantoms to Replace Cadaveric Models in Upper Extremity Surgical Residency Training. Materials 2022, 15, 694. https://doi.org/10.3390/ma15020694
Raeker-Jordan E, Martinez M, Shimada K. 3D Printing of Customizable Phantoms to Replace Cadaveric Models in Upper Extremity Surgical Residency Training. Materials. 2022; 15(2):694. https://doi.org/10.3390/ma15020694
Chicago/Turabian StyleRaeker-Jordan, Elisha, Miguel Martinez, and Kenji Shimada. 2022. "3D Printing of Customizable Phantoms to Replace Cadaveric Models in Upper Extremity Surgical Residency Training" Materials 15, no. 2: 694. https://doi.org/10.3390/ma15020694