
Understanding the Stress Distribution on Anatomic Customized Root-Analog Dental Implant at Bone-Implant Interface for Different Bone Densities

 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
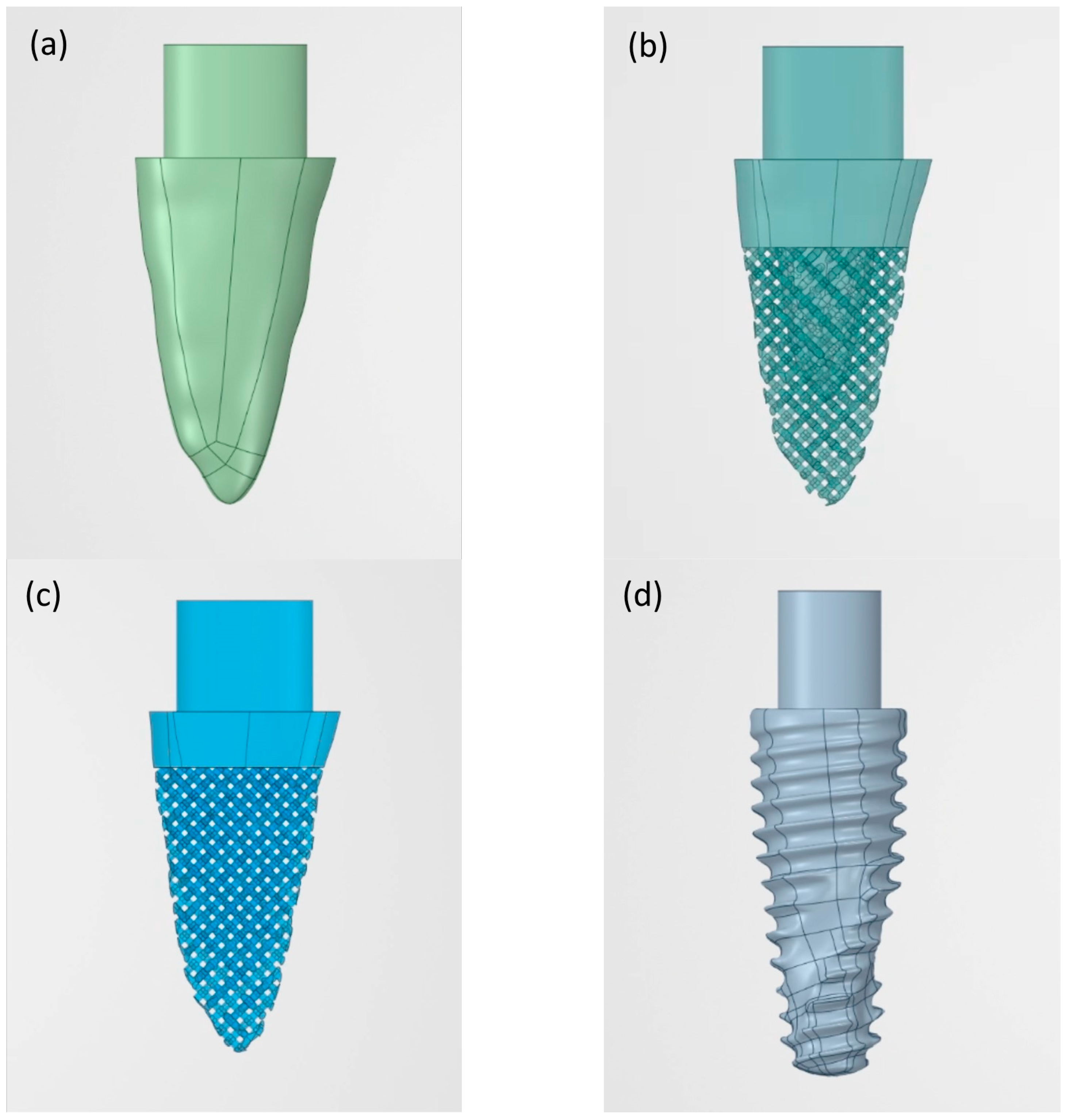
2.1. Design of Custom Digital 3D Models
2.2. Digital Stock Implant Model
2.3. Bone Boundary Model
2.4. Finite Element Analysis
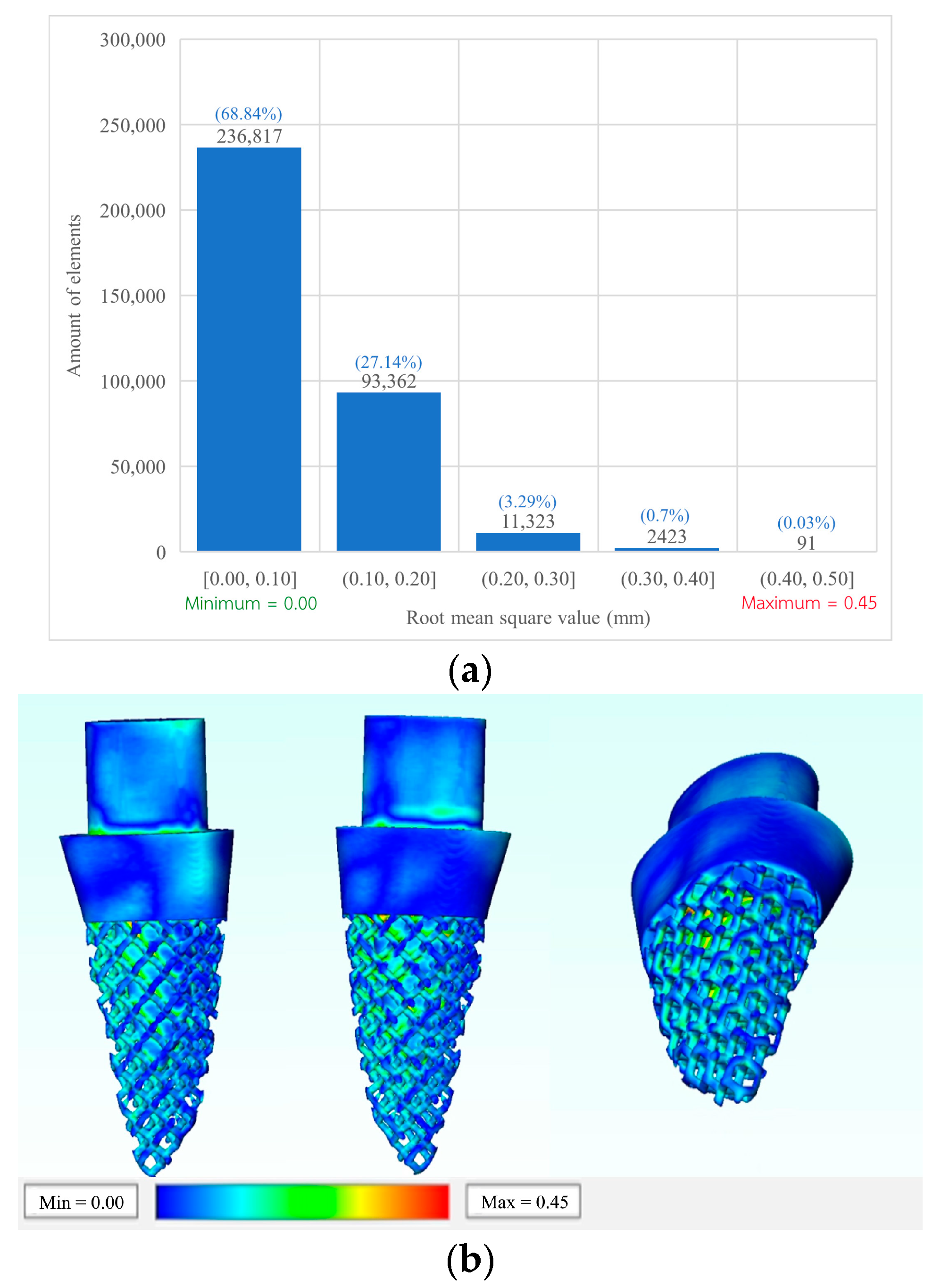
2.5. Validation of Novel 3D Printed RAI
3. Results
3.1. Von Mises Stress on Cortical Bone
3.2. Von Mises Stress on Cancellous Bone
3.3. Von Mises Stress on Implant Models
3.4. Implant Validation
4. Discussion
5. Conclusions
- The RAI was found to have a more favorable stress distribution pattern at the bone tissues and the bone-implant interface than the conventional screw-type implant in all types of bone density.
- The presence of a porous structure reduced the stress in cancellous bone of type IV.
- All designs demonstrated lower stress than what could cause plastic deformation or fracture based on the ultimate stress tolerance of both the bone and implant.
- Type I bone presents the lowest stress values at both bone tissue and the bone-implant interface than the other bone types.
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Goiato, M.C.; dos Santos, D.M.; Santiago, J.F.; Moreno, A.; Pellizzer, E.P. Longevity of dental implants in type IV bone: A systematic review. Int. J. Oral Maxillofac. Surg. 2014, 43, 1108–1116. [Google Scholar] [CrossRef] [PubMed]
- Steigenga, J.T.; Al-Shammari, K.F.; Nociti, F.; Misch, C.E.; Wang, H.-L. Dental implant design and its relationship to long-term implant success. Implant Dent. 2003, 12, 306–317. [Google Scholar] [CrossRef]
- Chen, J.; Zhang, Z.; Chen, X.; Zhang, C.; Zhang, G.; Xu, Z. Design and manufacture of customized dental implants by using reverse engineering and selective laser melting technology. J. Prosthet. Dent. 2014, 112, 1088–1095.e1. [Google Scholar] [CrossRef] [PubMed]
- Chen, X.; Xie, L.; Chen, J.; Du, R.; Deng, F. Design and fabrication of custom-made dental implants. J. Mech. Sci. Technol. 2012, 26, 1993–1998. [Google Scholar] [CrossRef]
- Thomrungpiyathan, T.; Luenam, S.; Lohwongwatana, B.; Sirichativapee, W.; Nabudda, K.; Puncreobutr, C. A custom-made distal humerus plate fabricated by selective laser melting. Comput. Methods Biomech. Biomed. Eng. 2021, 24, 585–596. [Google Scholar] [CrossRef]
- Figliuzzi, M.; Mangano, F.; Mangano, C. A novel root analogue dental implant using CT scan and CAD/CAM: Selective laser melting technology. Int. J. Oral Maxillofac. Surg. 2012, 41, 858–862. [Google Scholar] [CrossRef]
- Chunate, H.-T.; Khamwannah, J.; Aliyu, A.A.A.; Tantavisut, S.; Puncreobutr, C.; Khamkongkaeo, A.; Tongyam, C.; Tumkhanon, K.; Phetrattanarangsi, T.; Chanamuangkon, T.; et al. Titania Nanotube Architectures Synthesized on 3D-Printed Ti-6Al-4V Implant and Assessing Vancomycin Release Protocols. Materials 2021, 14, 6576. [Google Scholar] [CrossRef]
- Decha-Umphai, D.; Chunate, H.-T.; Phetrattanarangsi, T.; Boonchuduang, T.; Choosri, M.; Puncreobutr, C.; Lohwongwatana, B.; Khamwannah, J. Effects of post-processing on microstructure and adhesion strength of TiO2 nanotubes on 3D-printed Ti-6Al-4V alloy. Surf. Coat. Technol. 2021, 421, 127431. [Google Scholar] [CrossRef]
- Cai, H.; Chen, J.; Li, C.; Wang, J.; Wan, Q.; Liang, X. Quantitative discoloration assessment of peri-implant soft tissue around zirconia and other abutments with different colours: A systematic review and meta-analysis. J. Dent. 2018, 70, 110–117. [Google Scholar] [CrossRef]
- Albrektsson, T.; Brånemark, P.I.; Hansson, H.A.; Lindström, J. Osseointegrated titanium implants: Requirements for ensuring a long-lasting, direct bone-to-implant anchorage in man. Acta Orthop. Scand. 1981, 52, 155–170. [Google Scholar] [CrossRef] [Green Version]
- Linkow, L.I.; Rinaldi, A.W.; Weiss, W.W.; Smith, G.H. Factors influencing long-term implant success. J. Prosthet. Dent. 1990, 63, 64–73. [Google Scholar] [CrossRef]
- Almeida, D.A.D.F.; Pellizzer, E.P.; Verri, F.; Santiago, J.F., Jr.; De Carvalho, P.S.P. Influence of tapered and external hexagon connections on bone stresses around tilted dental implants: Three-dimensional finite element method with statistical analysis. J. Periodontol. 2014, 85, 261–269. [Google Scholar] [CrossRef] [PubMed]
- Pellizzer, E.P.; Carli, R.I.; Falcón-Antenucci, R.M.; Verri, F.; Goiato, M.; Villa, L.M.R. Photoelastic analysis of stress distribution with different implant systems. J. Oral Implantol. 2014, 40, 117–122. [Google Scholar] [CrossRef] [PubMed]
- Verri, F.R.; Batista, V.E.D.S.; Santiago, J.F.; Almeida, D.A.D.F.; Pellizzer, E.P. Effect of crown-to-implant ratio on peri-implant stress: A finite element analysis. Mater. Sci. Eng. C 2014, 45, 234–240. [Google Scholar] [CrossRef]
- Faverani, L.P.; Barão, V.A.R.; Ramalho-Ferreira, G.; Delben, J.; Ferreira, M.B.; Júnior, I.R.G.; Assunção, W.G. The influence of bone quality on the biomechanical behavior of full-arch implant-supported fixed prostheses. Mater. Sci. Eng. C 2014, 37, 164–170. [Google Scholar] [CrossRef]
- Pellizzer, E.P.; Verri, F.R.; de Moraes, S.L.D.; Falcón-Antenucci, R.M.; de Carvalho, P.S.P.; Noritomi, P.Y. Influence of the implant diameter with different sizes of hexagon: Analysis by 3-dimensional finite element method. J. Oral Implantol. 2013, 39, 425–431. [Google Scholar] [CrossRef]
- Antonelli, A.; Bennardo, F.; Brancaccio, Y.; Barone, S.; Femiano, F.; Nucci, L.; Minervini, G.; Fortunato, L.; Attanasio, F.; Giudice, A. Can bone compaction improve primary implant stability? An in vitro comparative study with osseodensification technique. Appl. Sci. 2020, 10, 8623. [Google Scholar] [CrossRef]
- De Almeida, E.O.; Rocha, E.; Freitas, A.C.; Freitas, M., Jr.; Martin, M., Jr. Finite element stress analysis of edentulous mandibles with different bone types supporting multiple-implant superstructures. Int. J. Oral Maxillofac. Implant 2010, 25, 1108–1114. [Google Scholar]
- Geng, J.-P.; Tan, K.B.C.; Liu, G.-R. Application of finite element analysis in implant dentistry: A review of the literature. J. Prosthet. Dent. 2001, 85, 585–598. [Google Scholar] [CrossRef]
- Linetskiy, I.; Demenko, V.; Linetska, L.; Yefremov, O. Impact of annual bone loss and different bone quality on dental implant success–A finite element study. Comput. Biol. Med. 2017, 91, 318–325. [Google Scholar] [CrossRef]
- Chang, H.-S.; Chen, Y.-C.; Hsieh, Y.-D.; Hsu, M.-L. Stress distribution of two commercial dental implant systems: A three-dimensional finite element analysis. J. Dent. Sci. 2013, 8, 261–271. [Google Scholar] [CrossRef] [Green Version]
- Hsu, J.-T.; Shen, Y.-W.; Kuo, C.-W.; Wang, R.-T.; Fuh, L.-J.; Huang, H.-L. Impacts of 3D bone-to-implant contact and implant diameter on primary stability of dental implant. J. Formos. Med. Assoc. 2017, 116, 582–590. [Google Scholar] [CrossRef] [PubMed]
- Skalak, R. Biomechanical considerations in osseointegrated prostheses. J. Prosthet. Dent. 1983, 49, 843–848. [Google Scholar] [CrossRef]
- Pengrung, N.; Lakdee, N.; Puncreobutr, C.; Lohwongwatana, B.; Sa-Ngasoongsong, P. Finite element analysis comparison between superior clavicle locking plate with and without screw holes above fracture zone in midshaft clavicular fracture. BMC Musculoskelet. Disord. 2019, 20, 465. [Google Scholar] [CrossRef] [PubMed]
- Valera-Jiménez, J.; Burgueño-Barris, G.; Gómez-González, S.; López-López, J.; Valmaseda-Castellón, E.; Fernández-Aguado, E. Finite element analysis of narrow dental implants. Dent. Mater. 2020, 36, 927–935. [Google Scholar] [CrossRef]
- Dhatrak, P.; Shirsat, U.; Sumanth, S.; Deshmukh, V. Finite element analysis and experimental investigations on stress distribution of dental implants around implant-bone interface. Mater. Today Proc. 2018, 5, 5641–5648. [Google Scholar] [CrossRef]
- Woelfel, J.B.; Scheid, R.C. Basic terminology for understanding tooth morphology. In Dental Anatomy: Its Relevance to Dentistry, 5th ed.; Lippincott Williams & Wilkins: Baltimore, MD, USA, 1997; pp. 87–118. [Google Scholar]
- Lee, J.W.; Wen, H.B.; Gubbi, P.; Romanos, G.E. New bone formation and trabecular bone microarchitecture of highly porous tantalum compared to titanium implant threads: A pilot canine study. Clin. Oral Implant Res. 2018, 29, 164–174. [Google Scholar] [CrossRef]
- Barba, D.; Alabort, E.; Reed, R. Synthetic bone: Design by additive manufacturing. Acta Biomater. 2019, 97, 637–656. [Google Scholar] [CrossRef]
- SInglam, S.; Chantarapanich, N.; Suebnukarn, S.; Vatanapatimakul, N.; Sucharitpwatskul, S.; Sitthiseripratip, K. Biomechanical evaluation of a novel porous-structure implant: Finite element study. Int. J. Oral Maxillofac. Implant 2013, 28, e48–e56. [Google Scholar] [CrossRef]
- Teixeira, E.R.; Sato, Y.; Akagawa, Y.; Shindoi, N. A comparative evaluation of mandibular finite element models with different lengths and elements for implant biomechanics. J. Oral Rehabil. 1998, 25, 299–303. [Google Scholar] [CrossRef]
- Sevimay, M.; Turhan, F.; Kiliçarslan, M.A.; Eskitascioglu, G. Three-dimensional finite element analysis of the effect of different bone quality on stress distribution in an implant-supported crown. J. Prosthet. Dent. 2005, 93, 227–234. [Google Scholar] [CrossRef] [PubMed]
- Tada, S.; Stegaroiu, R.; Kitamura, E.; Miyakawa, O.; Kusakari, H. Influence of implant design and bone quality on stress/strain distribution in bone around implants: A 3-dimensional finite element analysis. Int. J. Oral Maxillofac. Implant 2003, 18, 292–300. [Google Scholar]
- Junior, J.F.S.; Verri, F.R.; de Faria Almeida, D.A.; de Souza Batista, V.E.; Lemos, C.A.A.; Pellizzer, E.P. Finite element analysis on influence of implant surface treatments, connection and bone types. Mater. Sci. Eng. C 2016, 63, 292–300. [Google Scholar]
- Pellizzer, E.P.; Lemos, C.A.A.; Almeida, D.A.F.; Batista, V.E.D.S.; Júnior, J.F.S.; Verri, F.R. Biomechanical analysis of different implant-abutments interfaces in different bone types: An in silico analysis. Mater. Sci. Eng. C 2018, 90, 645–650. [Google Scholar] [CrossRef]
- Petrie, C.S.; Williams, J.L. Comparative evaluation of implant designs: Influence of diameter, length, and taper on strains in the alveolar crest: A three-dimensional finite-element analysis. Clin. Oral Implant Res. 2005, 16, 486–494. [Google Scholar] [CrossRef]
- Nordin, M.; Frankel, V.H. Basic Biomechanics of the Musculoskeletal System; Lippincott Williams & Wilkins: Baltimore, MD, USA, 2001. [Google Scholar]
- Chen, J.; Zhang, Z.; Chen, X.; Zhang, X. Influence of custom-made implant designs on the biomechanical performance for the case of immediate post-extraction placement in the maxillary esthetic zone: A finite element analysis. Comput. Methods Biomechanics Biomedical Eng. 2017, 20, 636–644. [Google Scholar] [CrossRef]
- Chen, L.-J.; He, H.; Li, Y.-M.; Li, T.; Guo, X.-P.; Wang, R.-F. Finite element analysis of stress at implant–bone interface of dental implants with different structures. Trans. Nonferrous Met. Soc. China 2011, 21, 1602–1610. [Google Scholar] [CrossRef]
- Tsai, M.-H.; Yang, C.-M.; Hung, Y.-X.; Jheng, C.-Y.; Chen, Y.-J.; Fu, H.-C.; Chen, I.-G. Finite Element Analysis on Initial Crack Site of Porous Structure Fabricated by Electron Beam Additive Manufacturing. Materials 2021, 14, 7467. [Google Scholar] [CrossRef]
- Hansson, S. The implant neck: Smooth or provided with retention elements. A biomechanical approach. Clin. Oral Implant Res. 1999, 10, 394–405. [Google Scholar] [CrossRef]
- Schrotenboer, J.; Tsao, Y.-P.; Kinariwala, V.; Wang, H.-L. Effect of microthreads and platform switching on crestal bone stress levels: A finite element analysis. J. Periodontol. 2008, 79, 2166–2172. [Google Scholar] [CrossRef]
- Pałka, K.; Pokrowiecki, R. Porous titanium implants: A review. Adv. Eng. Mater. 2018, 20, 1700648. [Google Scholar] [CrossRef]
- Shaoki, A.; Xu, J.-Y.; Sun, H.; Chen, X.-S.; Ouyang, J.; Zhuang, X.-M.; Deng, F.-L. Osseointegration of three-dimensional designed titanium implants manufactured by selective laser melting. Biofabrication 2016, 8, 045014. [Google Scholar] [CrossRef] [PubMed]
- Albrektsson, T.; Wennerberg, A. Oral implant surfaces: Part 1—Review focusing on topographic and chemical properties of different surfaces and in vivo responses to them. Int. J. Prosthodont. 2004, 17, 536–543. [Google Scholar] [PubMed]
- Brentel, A.S.; De Vasconcellos, L.M.R.; Oliveira, M.V.; Graça, M.L.D.A.; De Vasconcellos, L.G.O.; Cairo, C.A.A.; Carvalho, Y.R. Histomorphometric analysis of pure titanium implants with porous surface versus rough surface. J. Appl. Oral Sci. 2006, 14, 213–218. [Google Scholar] [CrossRef] [PubMed]
- Albertini, M.; Fernandez-Yague, M.; Lázaro, P.; Herrero-Climent, M.; Rios-Santos, J.V.; Bullon, P.; Gil, F.J. Advances in surfaces and osseointegration in implantology. Biomimetic surfaces. Med. Oral Patol. Oral Cir. Bucal 2015, 20, e316. [Google Scholar] [CrossRef]
- Depboylu, F.N.; Yasa, E.; Poyraz, Ö.; Minguella-Canela, J.; Korkusuz, F.; López, M.A.D.L.S. Titanium based bone implants production using laser powder bed fusion technology. J. Mater. Res. Technol. 2022, 17, 1408–1426. [Google Scholar] [CrossRef]
- Tawhid, A.; Teotia, T.; Elmiligi, H. Machine learning for optimizing healthcare resources. In Machine Learning, Big Data, and IoT for Medical Informatics; Elsevier: Amsterdam, The Netherlands, 2021; pp. 215–239. [Google Scholar]
- García-Alonso, J.; Fonseca, C. Gerontechnology: Second International Workshop, Proceedings of the IWoG 2019, Cáceres, Spain, 4–5 September 2019, Revised Selected Papers; Springer Nature: Berlin, Germany, 2020. [Google Scholar]
- Unsal, G. Three-Dimensional Finite Element Analysis of Different Implant Configurations in Enlarged First Molar Areas. Int. J. Oral Maxillofac. Implant 2020, 35, 675–683. [Google Scholar] [CrossRef]
- Kayumi, S.; Takayama, Y.; Yokoyama, A.; Ueda, N. Effect of bite force in occlusal adjustment of dental implants on the distribution of occlusal pressure: Comparison among three bite forces in occlusal adjustment. Int. J. Implant Dent. 2015, 1, 14. [Google Scholar] [CrossRef]
- Lian, Z.; Guan, H.; Ivanovski, S.; Loo, Y.-C.; Johnson, N.; Zhang, H. Effect of bone to implant contact percentage on bone remodelling surrounding a dental implant. Int. J. Oral Maxillofac. Surg. 2010, 39, 690–698. [Google Scholar] [CrossRef]
- Yemineni, B.C.; Mahendra, J.; Nasina, J.; Mahendra, L.; Shivasubramanian, L.; Perika, S.B. Evaluation of maximum principal stress, von mises stress, and deformation on surrounding mandibular bone during insertion of an implant: A three-dimensional finite element study. Cureus 2020, 12, e9430. [Google Scholar] [CrossRef]
- Nelson, S.; Ash, M. Wheeler’s Dental Anatomy, Physiology and Occlusion; Elsevier: Amsterdam, The Netherlands, 2009. [Google Scholar]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Materials | Modulus of Elasticity (GPa) | Poisson’s Ratio (V) |
|---|---|---|
| Cortical bone | 13.7 | 0.3 |
| Cancellous bone (bone type II, II) | 1.37 | 0.3 |
| Cancellous bone (bone type IV) | 0.69 | 0.3 |
| Titanium | 110.0 | 0.35 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nimmawitt, P.; Aliyu, A.A.A.; Lohwongwatana, B.; Arunjaroensuk, S.; Puncreobutr, C.; Mattheos, N.; Pimkhaokham, A. Understanding the Stress Distribution on Anatomic Customized Root-Analog Dental Implant at Bone-Implant Interface for Different Bone Densities. Materials 2022, 15, 6379. https://doi.org/10.3390/ma15186379
Nimmawitt P, Aliyu AAA, Lohwongwatana B, Arunjaroensuk S, Puncreobutr C, Mattheos N, Pimkhaokham A. Understanding the Stress Distribution on Anatomic Customized Root-Analog Dental Implant at Bone-Implant Interface for Different Bone Densities. Materials. 2022; 15(18):6379. https://doi.org/10.3390/ma15186379
Chicago/Turabian StyleNimmawitt, Pawhat, Abdul Azeez Abdu Aliyu, Boonrat Lohwongwatana, Sirida Arunjaroensuk, Chedtha Puncreobutr, Nikos Mattheos, and Atiphan Pimkhaokham. 2022. "Understanding the Stress Distribution on Anatomic Customized Root-Analog Dental Implant at Bone-Implant Interface for Different Bone Densities" Materials 15, no. 18: 6379. https://doi.org/10.3390/ma15186379