
Short Implants versus Longer Implants with Sinus Floor Elevation: A Systemic Review and Meta-Analysis of Randomized Controlled Trials with a Post-Loading Follow-Up Duration of 5 Years


Abstract
:1. Introduction
2. Materials and Methods
2.1. Eligibility Criteria
- RCTs: patients with maxillary atrophy, with 4–7 mm of bone height, were randomized into two groups. One group was rehabilitated with prostheses supported by short implants (<8 mm) without bone grafts. The other was rehabilitated by longer implants combined with sinus floor elevation;
- The study was randomized and included the use of short (<8 mm) and longer implant groups; all patients (male or female) were ≥18 years old;
- The implants were evaluated with an average follow-up duration of at least 5 years after loading;
- Each group included more than 10 patients.
2.2. Search Strategy and Information Sources
2.3. Study Selection
2.4. Risk of Bias
2.5. Data Extraction
2.6. Synthesis and Meta-Analysis of the Data
- Implant failure: implants that were not present in the mouth or that did not match any of the success criteria were judged to have failed;
- Biological complications (intra- or postoperative): sinus membrane perforations, sinusitis (acute sinus infection), soft tissue dehiscence, fistula, swelling, infection, or implant failure;
- Technical complications: abutment screw loosening or screw fracture, crown chipping or loss retention, replacing the crown;
- Peri-implant MBL: the distance between the implant shoulder and most coronal point of bone-to-implant contact at each evaluation time point (implant placement at baseline and the follow-up times).
3. Results
3.1. Literature Search
3.2. Description of the Studies
3.3. Assessment of Study Quality
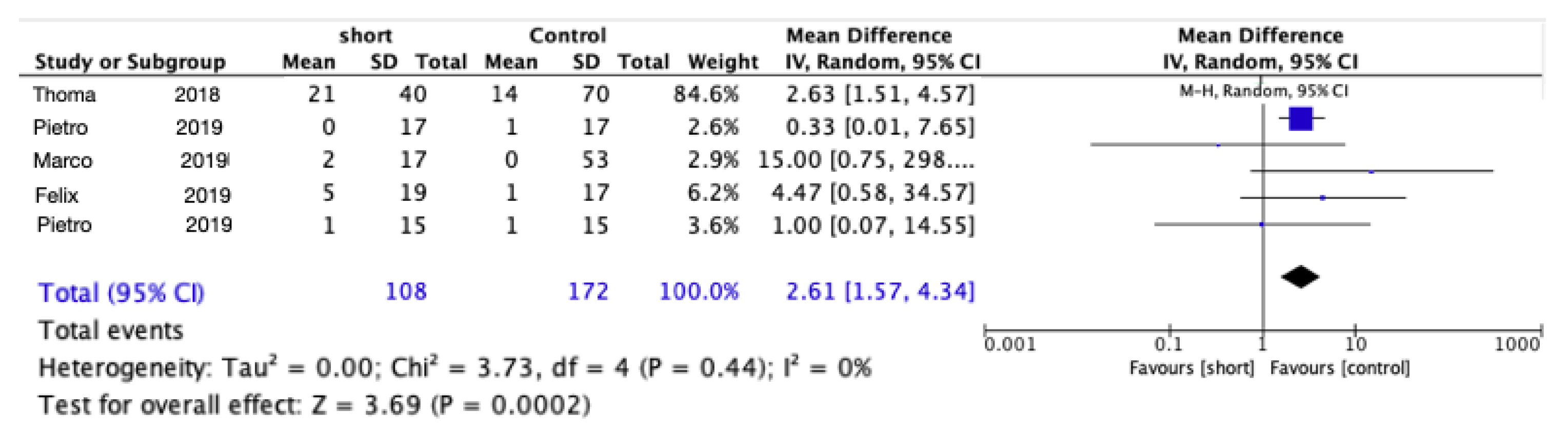
3.4. Implant Failure
3.5. Complications
3.6. Changes in Peri-Implant Marginal Bone Levels

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Reason | References |
|---|---|
| Data from the same group of samples | Pietro et al. [24] |
| Pietro et al. [25] | |
| Roberto et al. [26] | |
| Pohl V et al. [7] | |
| Schincaglia et al. [27] | |
| Marco et al. [28] | |
| Felix et al. [29] | |
| Follow-up time < 5 years | Marco et al. [30] |
| Sahrmann et al. [31] | |
| Pietro et al. [32] | |
| Gastaldi et al. [33] | |
| Bolle et al. [34] | |
| Jun-Yu et al. [35] | |
| Taschieri et al. [36] | |
| Bechara et al. [37] | |
| Hadzik et al. [38] | |
| Shah et al. [39] | |
| Amir et al. [40] | |
| Length of short implant not less than 8 mm | Cannizzaro et al. [41] |
| Study | Unicenter/Multicenter | Total No. of Patients/Implants | No. of Implants in Each Group | Patients’ Age Range (Average) (Years) | Definitive Restoration | Brand and Connection | Dimension of the Implant (Length × Diameter) | |
|---|---|---|---|---|---|---|---|---|
| Felix [18] | Multicenter | 41/41 | Short | 21 | 50 (30–71) | Single crown | Astra, internal | 6 × 4 |
| control | 20 | 48 (29–72) | 11 × 4 | |||||
| Pietro [19] | 1 | 15/72 | Short | 34 | 56 (45–70) | Splint crowns | Megagen, internal | 5 × 6 |
| control | 38 | 10 × 6 or (10,11.5,13) × 4 | ||||||
| Marco [20] | Multicenter | 20/83 41/41 | Short | 36 | 61.1 (45–70) | Splint crowns | Megagen, external | 5 × 5 |
| control | 37 | 58.5 (45–75) | (10,11.5,13,15) × 5 | |||||
| Thoma [21] | Multicenter | 15/72 40/73 | Short | 67 | 50 (23–76) | single | Astra, internal | 6 × 4 |
| control | 70 | 51 (20–77) | (11,13,15) × 4 | |||||
| Pietro [22] | 2 | 101/137 20/83 | Short | 39 | 57.6 (45–80) | Single/ splint crowns | Southern, external | 6 × 4 |
| control | 44 | (10,11.5,13,15) × 4 | ||||||
| Bias | Felix (2019) [18] | Pietro (2019) [19] | Marco (2019) [20] | Thomma (2018) [21] | Pietro (2019) [22] |
|---|---|---|---|---|---|
| Random sequence generation |  | | | | |
| Allocation concealment | | | | | |
| Blinding of patients and surgeons |  | | | | |
| Blinding of outcome assessment | | | | | |
| Incomplete outcome data | | | | | |
| Selective reporting | | | | | |
| Other sources of bias | |||||
| Group imbalance | | | | | |
| Sample size | | |  | | |
| Follow-up time | | | | | |
| Conflict of interest | | | | | |
| Radiographic outcome | | | | | |
| Clinician bias | | | | | |
| Score | 7 | 8 | 7 | 7 | 8 |
| Study | No. Implants in Each Group | Number of Patients with Complications (Number of Complications) | In Total | ||
|---|---|---|---|---|---|
| Biological Complications | Technical Complications | ||||
| Felix [18] | Short | 21 | 1 implant failure | 3 replaced crowns, 1 chips, 1 abutment loosened | 4p (7) (n = 19) |
| Control | 20 | 0 | 1 abutment loosened | 1p (1) (n = 17) | |
| Pietro [19] | short | 34 | 3 perforation, 1 mucositis, 3 implant failures | Prosthesis decementation 1 | 5p (5) (n = 15) |
| control | 38 | 1 sinus perforation, 1 implant failure | prosthesis decementation 1 | 2p (2) (n = 15) | |
| Marco [20] | short | 36 | 1 | 1 replaced crown, 1 failure due to implant | 2p (2) (n = 17) |
| control | 37 | 5p membrane perforated | 0 | 7p (7) (n = 19) | |
| Thoma [21] | short | 67 | Fistula, swelling, infection or implant failure: 5 | Abutment loosened, fracture, chipping, lost crown or loss retention: 21 (47.7%) | 26 (n = 40) |
| control | 70 | Fistula, swell, infection or implant failure: 9 | Abutment loosened, fracture, chipping, lost crown or loss retention: 14(30.4%) | 23 (n = 53) | |
| Pietro [22] | short | 39 | Implant failure | 0 | 1p (n = 17) |
| control | 44 | 4 perforations | 1 chip | 5p (n = 17) | |
4. Discussion
4.1. Definition of a Short Implant
4.2. Implant Failure
4.3. Complications
4.4. Marginal Bone Loss
4.5. Placement of Short Implants in Maxillary Sinus Augmented Sites
4.6. Limitations
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Rossi, F.; Botticelli, D.; Cesaretti, G.; De Santis, E.; Storelli, S.; Lang, N.P. Use of short implants (6 mm) in a single-tooth replacement: A 5-year follow-up prospective randomized controlled multicenter clinical study. Clin. Oral Implant. Res. 2016, 27, 458–464. [Google Scholar] [CrossRef] [PubMed]
- Esfahrood, Z.R.; Ahmadi, L.; Karami, E.; Asghari, S. Short dental implants in the posterior maxilla: A review of the literature. J. Korean Assoc. Oral Maxillofac. Surg. 2017, 43, 70–76. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fan, T.; Li, Y.; Deng, W.W.; Wu, T.; Zhang, W. Short Implants (5 to 8 mm) versus longer implants (>8 mm) with sinus lifting in atrophic posterior maxilla: A meta-analysis of RCTs. Clin. Implant Dent. Relat. Res. 2017, 19, 207–215. [Google Scholar] [CrossRef] [PubMed]
- Lemos, C.A.A.; Ferro-Alves, M.L.; Okamoto, R.; Mendonça, M.R.; Pellizzer, E.P. Short dental implants versus standard dental implants placed in the posterior jaws: A systematic review and meta-analysis. J. Dent. 2016, 47, 8–17. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- French, D.; Larjava, H.; Ofec, R. Retrospective cohort study of 4591 Straumann implants in private practice setting, with up to 10-year follow-up: Part 1: Multivariate survival analysis. Clin. Oral Implant. Res. 2015, 26, 1345–1354. [Google Scholar] [CrossRef]
- Lai, H.C.; Si, M.S.; Zhuang, L.F.; Shen, H.; Liu, Y.L.; Wismeijer, D. Long-term outcomes of short dental implants supporting single crowns in posterior region: A clinical retrospective study of 5–10 years. Clin. Oral Implant. Res. 2013, 24, 230–237. [Google Scholar] [CrossRef]
- Pohl, V.; Thoma, D.S.; Sporniak-Tutak, K.; Garcia-Garcia, A.; Taylor, T.D.; Haas, R.; Hämmerle, C.H.F. Short dental implants (6 mm) versus long dental implants (11–15 mm) in combination with sinus floor elevation procedures: 3-year results from a multicentre, randomized, controlled clinical trial. J. Clin. Periodontol. 2017, 44, 438–445. [Google Scholar] [CrossRef] [Green Version]
- das Neves, F.D.; Fones, D.; Bernardes, S.R.; do Prado, C.J.; Neto, A.J. Short implants—An analysis of longitudinal studies. J. Prosthet. Dent. 2006, 96, 288. [Google Scholar] [CrossRef]
- Renouard, F.; Nisand, D. Impact of implant length and diameter on survival rates. Clin. Oral Implant. Res. 2006, 17, 35–51. [Google Scholar] [CrossRef]
- Thoma, D.S.; Zeltner, M.; Hüsler, J.; Hämmerle, C.H.F.; Jung, R.E. EAO supplement working group 4-EAO CC 2015 short implants versus sinus lifting with longer implants to restore the posterior maxilla: A systematic review. Clin. Oral Implant. Res. 2015, 26, 154–169. [Google Scholar] [CrossRef]
- Plonka, A.; Urban, I.; Wang, H.-L. Decision tree for vertical ridge augmentation. Int. J. Periodontics Restor. Dent. 2018, 38, 269–275. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yan, Q.; Wu, X.; Su, M.; Hua, F.; Shi, B. Short implants (≤6 mm) versus longer implants with sinus floor elevation in atrophic posterior maxilla: A systematic review and meta-analysis. BMJ Open 2019, 9, e029826. [Google Scholar] [CrossRef] [PubMed]
- Lozano-Carrascal, N.; Anglada-Bosqued, A.; Salomó-Coll, O.; Hernández-Alfaro, F.; Wang, H.L.; Gargallo-Albiol, J. Short implants (<8 mm) versus longer implants (≥8 mm) with lateral sinus floor augmentation in posterior atrophic maxilla: A meta-analysis of RCT’s in humans. Med. Oral Patol. Oral y Cir. Bucal 2020, 25, e168–e179. [Google Scholar] [CrossRef]
- Nielsen, H.B.; Schou, S.; Isidor, F.; Christensen, A.E.; Starch-Jensen, T. Short implants (≤8 mm) compared to standard length implants (>8 mm) in conjunction with maxillary sinus floor augmentation: A systematic review and meta-analysis. Int. J. Oral Maxillofac. Surg. 2019, 48, 239–249. [Google Scholar] [CrossRef] [PubMed]
- Chen, S.; Ou, Q.; Wang, Y.; Lin, X. Short implants (5–8 mm) vs long implants (≥10 mm) with augmentation in atrophic posterior jaws: A meta-analysis of randomised controlled trials. J. Oral Rehabil. 2019, 46, 1192–1203. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; Altman, D.; Antes, G.; Atkins, D.; Barbour, V.; Barrowman, N.; Berlin, J.A.; et al. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. Ann. Intern. Med. 2009, 151, 264–269. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Higgins, J.P.T.; Altman, D.G.; Gøtzsche, P.C.; Jüni, P.; Moher, D.; Oxman, A.D.; Savović, J.; Schulz, K.F.; Weeks, L.; Sterne, J.A.C. The cochrane collaboration’s tool for assessing risk of bias in randomised trials. BMJ 2011, 343, d5928. [Google Scholar] [CrossRef] [Green Version]
- Guljé, F.L.; Raghoebar, G.M.; Vissink, A.; Meijer, H.J.A. Single crowns in the resorbed posterior maxilla supported by either 11-mm implants combined with sinus floor elevation or 6-mm implants: A 5-year randomised controlled trial. Int. J. Oral Implant. 2019, 12, 315–326. [Google Scholar]
- Felice, P.; Barausse, C.; Pistilli, R.; Ippolito, D.R.; Esposito, M. Five-year results from a randomised controlled trial comparing prostheses supported by 5-mm long implants or by longer implants in augmented bone in posterior atrophic edentulous jaws. Eur. J. Oral Implantol. 2019, 12, 25–37. [Google Scholar]
- Esposito, M.; Barausse, C.; Pistilli, R.; Piattelli, M.; Di Simone, S.; Ippolito, D.R.; Felice, P. Posterior atrophic jaws rehabilitated with prostheses supported by 5 × 5 mm implants with a nanostructured calcium-incorporated titanium surface or by longer implants in augmented bone. Five-year results from a randomised controlled trial. Eur. J. Oral Implantol. 2019, 12, 39–54. [Google Scholar]
- Thoma, D.S.; Haas, R.; Sporniak-Tutak, K.; Garcia, A.; Taylor, T.D.; Hämmerle, C.H.F. Randomized controlled multicentre study comparing short dental implants (6 mm) versus longer dental implants (11–15 mm) in combination with sinus floor elevation procedures: 5-Year data. J. Clin. Periodontol. 2018, 45, 1465–1474. [Google Scholar] [CrossRef] [PubMed]
- Felice, P.; Pistilli, R.; Barausse, C.; Piattelli, M.; Buti, J.; Esposito, M. Posterior atrophic jaws rehabilitated with prostheses supported by 6-mm-long 4-mm-wide implants or by longer implants in augmented bone. Five-year post-loading results from a within-person randomised controlled trial. Eur. J. Oral Implantol. 2019, 12, 57–72. [Google Scholar]
- Jung, R.E.; Al-Nawas, B.; Araujo, M.; Avila-Ortiz, G.; Barter, S.; Brodala, N.; Chappuis, V.; Chen, B.; De Souza, A.; Almeida, R.F.; et al. Group 1 ITI consensus report: The influence of implant length and design and medications on clinical and patient-reported outcomes. Clin. Oral Implant. Res. 2018, 29, 69–77. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Felice, P.; Cannizzaro, G.; Barausse, C.; Pistilli, R.; Esposito, M. Short implants versus longer implants in vertically augmented posterior mandibles: A randomised controlled trial with 5-year after loading follow-up. Eur. J. Oral Implantol. 2014, 7, 359–369. [Google Scholar]
- Felice, P.; Pistilli, R.; Barausse, C.; Bruno, V.; Trullenque-Eriksson, A.; Esposito, M. Short implants as an alternative to crestal sinus lift: A 1-year multicentre randomised controlled trial. Eur. J. Oral Implantol. 2015, 8, 375–384. [Google Scholar]
- Pistilli, R.; Felice, P.; Cannizzaro, G.; Piattelli, M.; Corvino, V.; Barausse, C.; Buti, J.; Soardi, E.; Esposito, M. Posterior atrophic jaws rehabilitated with prostheses supported by 6 mm long 4 mm wide implants or by longer implants in augmented bone. One-year post-loading results from a pilot randomised controlled trial. Eur. J. Oral Implantol. 2013, 6, 359–372. [Google Scholar]
- Schincaglia, G.P.; Thoma, D.S.; Haas, R.; Tutak, M.; Garcia, A.; Taylor, T.D.; Hämmerle, C.H.F. Randomized controlled multicenter study comparing short dental implants (6 mm) versus longer dental implants (11-15 mm) in combination with sinus floor elevation procedures. Part 2: Clinical and radiographic outcomes at 1 year of loading. J. Clin. Periodontol. 2015, 42, 1042–1051. [Google Scholar] [CrossRef] [Green Version]
- Esposito, M.; Pistilli, R.; Barausse, C.; Felice, P. Three-year results from a randomised controlled trial comparing prostheses supported by 5-mm long implants or by longer implants in augmented bone in posterior atrophic edentulous jaws. Eur. J. Oral Implantol. 2014, 7, 383–395. [Google Scholar]
- Guljé, F.L.; Raghoebar, G.M.; Vissink, A.; Meijer, H.J.A. Single crowns in the resorbed posterior maxilla supported by either 6-mm implants or by 11-mm implants combined with sinus floor elevation surgery: A 1-year randomised controlled trial. Eur. J. Oral Implantol. 2014, 7, 247–255. [Google Scholar]
- Esposito, M.; Barausse, C.; Pistilli, R.; Sammartino, G.; Grandi, G.; Felice, P. Short implants versus bone augmentation for placing longer implants in atrophic maxillae: One-year post-loading results of a pilot randomised controlled trial. Eur. J. Oral Implantol. 2015, 8, 257–268. [Google Scholar]
- Sahrmann, P.; Naenni, N.; Jung, R.E.; Held, U.; Truninger, T.; Hämmerle, C.H.F.; Attin, T.; Schmidlin, P.R. Success of 6-mm implants with single-tooth restorations: A 3-year randomized controlled clinical trial. J. Dent. Res. 2016, 95, 623–628. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Felice, P.; Barausse, C.; Pistilli, R.; Ippolito, D.R.; Esposito, M. Short implants versus longer implants in vertically augmented posterior mandibles: Result at 8 years after loading from a randomised controlled trial. Eur. J. Oral Implantol. 2018, 11, 385–395. [Google Scholar] [PubMed]
- Gastaldi, G.; Felice, P.; Pistilli, R.; Barausse, C.; Trullenque-Eriksson, A.; Esposito, M. Short implants as an alternative to crestal sinus lift: A 3-year multicentre randomised controlled trial. Eur. J. Oral Implantol. 2017, 10, 391–400. [Google Scholar] [PubMed]
- Bolle, C.B.; Felice, P.; Bolle, C.B.; Pistilli, V.; Trullenque-Eriksson, A.; Esposito, M.; Bolle, C.; Felice, P.; Barausse, C.; Pistilli, V.; et al. 4 mm long vs longer implants in augmented bone in posterior atrophic jaws: 1-year post-loading results from a multicentre randomised controlled trial. Eur. J. Oral Implantol. 2018, 11, 31–47. [Google Scholar] [PubMed]
- Shi, J.Y.; Li, Y.; Qiao, S.C.; Gu, Y.X.; Xiong, Y.Y.; Lai, H.C. Short versus longer implants with osteotome sinus floor elevation for moderately atrophic posterior maxillae: A 1-year randomized clinical trial. J. Clin. Periodontol. 2019, 46, 855–862. [Google Scholar] [CrossRef] [PubMed]
- Taschieri, S.; Lolato, A.; Testori, T.; Francetti, L.; Del Fabbro, M. Short dental implants as compared to maxillary sinus augmentation procedure for the rehabilitation of edentulous posterior maxilla: Three-year results of a randomized clinical study. Clin. Implant Dent. Relat. Res. 2018, 20, 9–20. [Google Scholar] [CrossRef]
- Bechara, S.; Kubilius, R.; Veronesi, G.; Pires, J.T.; Shibli, J.A.; Mangano, F.G. Short (6-mm) dental implants versus sinus floor elevation and placement of longer (≥10-mm) dental implants: A randomized controlled trial with a 3-year follow-up. Clin. Oral Implant. Res. 2017, 28, 1097–1107. [Google Scholar] [CrossRef]
- Hadzik, J.; Krawiec, M.; Kubasiewicz-Ross, P.; Prylińska-Czyżewska, A.; Gedrange, T.; Dominiak, M. Short implants and conventional implants in the residual maxillary alveolar ridge: A 36-month follow-up observation. Med. Sci. Monit. 2018, 24, 5645–5652. [Google Scholar] [CrossRef]
- Shah, S.N.; Chung, J.; Kim, D.M.; Machtei, E.E. Can extra-short dental implants serve as alternatives to bone augmentation? A preliminary longitudinal randomized controlled clinical trial. Quintessence Int. 2018, 49, 635–643. [Google Scholar] [CrossRef]
- Rokn, A.R.; Monzavi, A.; Panjnoush, M.; Hashemi, H.M.; Kharazifard, M.J.; Bitaraf, T. Comparing 4-mm dental implants to longer implants placed in augmented bones in the atrophic posterior mandibles: One-year results of a randomized controlled trial. Clin. Implant Dent. Relat. Res. 2018, 20, 997–1002. [Google Scholar] [CrossRef]
- Cannizzaro, G.; Felice, P.; Minciarelli, A.F.; Leone, M.; Viola, P.; Esposito, M. Early implant loading in the atrophic posterior maxilla: 1-stage lateral versus crestal sinus lift and 8 mm hydroxyapatite-coated implants. A 5-year randomised controlled trial. Eur. J. Oral Implantol. 2013, 6, 13–25. [Google Scholar] [CrossRef] [PubMed]
- Vazouras, K.; de Souza, A.B.; Gholami, H.; Papaspyridakos, P.; Pagni, S.; Weber, H.P. Effect of time in function on the predictability of short dental implants (≤6 mm): A meta-analysis. J. Oral Rehabil. 2020, 47, 403–415. [Google Scholar] [CrossRef]
- Papaspyridakos, P.; De Souza, A.; Vazouras, K.; Gholami, H.; Pagni, S.; Weber, H.P. Survival rates of short dental implants (≤6 mm) compared with implants longer than 6 mm in posterior jaw areas: A meta-analysis. Clin. Oral Implant. Res. 2018, 29, 8–20. [Google Scholar] [CrossRef] [PubMed]
- Goiato, M.C.; Dos Santos, D.M.; Santiago, J.F.; Moreno, A.; Pellizzer, E.P. Longevity of dental implants in type IV bone: A systematic review. Int. J. Oral Maxillofac. Surg. 2014, 43, 1108–1116. [Google Scholar] [CrossRef] [PubMed]
- Queiroz, T.P.; Aguiar, S.C.; Margonar, R.; de Souza Faloni, A.P.; Gruber, R.; Luvizuto, E.R. Clinical study on survival rate of short implants placed in the posterior mandibular region: Resonance frequency analysis. Clin. Oral Implant. Res. 2015, 26, 1036–1042. [Google Scholar] [CrossRef] [PubMed]
- Uehara, P.N.; Matsubara, V.H.; Igai, F.; Sesma, N.; Mukai, M.K.; Araujo, M.G. Short dental implants (≤7 mm) versus longer implants in augmented bone area: A meta-analysis of randomized controlled trials. Open Dent. J. 2018, 12, 354–365. [Google Scholar] [CrossRef]
- Annibali, S.; Cristalli, M.P.; Dell’Aquila, D.; Bignozzi, I.; La Monaca, G.; Pilloni, A. Short dental implants: A systematic review. J. Dent. Res. 2012, 91, 25–32. [Google Scholar] [CrossRef]
- Palacios, J.A.V.; Garcia, J.J.; Caramês, J.M.M.; Quirynen, M.; da Silva Marques, D.N. Short implants versus bone grafting and standard-length implants placement: A systematic review. Clin. Oral Investig. 2018, 22, 69–80. [Google Scholar] [CrossRef]
- Lee, S.-A.; Lee, C.-T.; Fu, M.; Elmisalati, W.; Chuang, S.-K. systematic review and meta-analysis of randomized controlled trials for the management of limited vertical height in the posterior region: Short implants (5 to 8 mm) vs longer implants (>8 mm) in vertically augmented sites. Int. J. Oral Maxillofac. Implant. 2014, 29, 1085–1097. [Google Scholar] [CrossRef]
- Villarinho, E.A.; Triches, D.F.; Alonso, F.R.; Mezzomo, L.A.M.; Teixeira, E.R.; Shinkai, R.S.A. Risk factors for single crowns supported by short (6-mm) implants in the posterior region: A prospective clinical and radiographic study. Clin. Implant Dent. Relat. Res. 2017, 19, 671–680. [Google Scholar] [CrossRef]
- Naenni, N.; Sahrmann, P.; Schmidlin, P.R.; Attin, T.; Wiedemeier, D.B.; Sapata, V.; Hämmerle, C.H.F.; Jung, R.E. Five-year survival of short single-tooth implants (6 mm): A randomized controlled clinical trial. J. Dent. Res. 2018, 97, 887–892. [Google Scholar] [CrossRef] [PubMed]
- Bitaraf, T.; Keshtkar, A.; Rokn, A.R.; Monzavi, A.; Geramy, A.; Hashemi, K. Comparing short dental implant and standard dental implant in terms of marginal bone level changes: A systematic review and meta-analysis of randomized controlled trials. Clin. Implant Dent. Relat. Res. 2019, 21, 796–812. [Google Scholar] [CrossRef] [PubMed]
- Ihde, S.; Ihde, A.; Sipic, O.; Pałka, Ł. Peri-Implantitis: A New Definition Proposal Based on Unnatural Spatial Arrangement. and Late Mechanical Coupling between Two Cortical Bone Layers during Osseointegration Phase Part II. Appl. Sci. 2022, 12, 5589. [Google Scholar] [CrossRef]
- Deporter, D.; Ogiso, B.; Sohn, D.-S.; Ruljancich, K.; Pharoah, M. Ultrashort sintered porous-surfaced dental implants used to replace posterior teeth. J. Periodontol. 2008, 79, 1280–1286. [Google Scholar] [CrossRef]
- Sohn, D.-S.; Lee, J.-M.; Park, I.-S.; Jung, H.-S.; Park, D.-Y.; Shin, I.-H. Retrospective study of sintered porous-surfaced dental implants placed in the augmented sinus. Int. J. Periodontics Restor. Dent. 2014, 34, 565–571. [Google Scholar] [CrossRef]
- de Souza Batista, V.E.; Verri, F.R.; Lemos, C.A.A.; Cruz, R.S.; Oliveira, H.F.F.; Gomes, J.M.L.; Pellizzer, E.P. Should the restoration of adjacent implants be splinted or nonsplinted? A systematic review and meta-analysis. J. Prosthet. Dent. 2019, 121, 41–51. [Google Scholar] [CrossRef] [Green Version]
- Mendonça, J.A.; Francischone, C.E.; Senna, P.M.; Matos de Oliveira, A.E.; Sotto-Maior, B.S. A retrospective evaluation of the survival rates of splinted and non-splinted short dental implants in posterior partially edentulous jaws. J. Periodontol. 2014, 85, 787–794. [Google Scholar] [CrossRef]






Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wang, M.; Liu, F.; Ulm, C.; Shen, H.; Rausch-Fan, X. Short Implants versus Longer Implants with Sinus Floor Elevation: A Systemic Review and Meta-Analysis of Randomized Controlled Trials with a Post-Loading Follow-Up Duration of 5 Years. Materials 2022, 15, 4722. https://doi.org/10.3390/ma15134722
Wang M, Liu F, Ulm C, Shen H, Rausch-Fan X. Short Implants versus Longer Implants with Sinus Floor Elevation: A Systemic Review and Meta-Analysis of Randomized Controlled Trials with a Post-Loading Follow-Up Duration of 5 Years. Materials. 2022; 15(13):4722. https://doi.org/10.3390/ma15134722
Chicago/Turabian StyleWang, Miaozhen, Feng Liu, Christian Ulm, Huidan Shen, and Xiaohui Rausch-Fan. 2022. "Short Implants versus Longer Implants with Sinus Floor Elevation: A Systemic Review and Meta-Analysis of Randomized Controlled Trials with a Post-Loading Follow-Up Duration of 5 Years" Materials 15, no. 13: 4722. https://doi.org/10.3390/ma15134722