
Effects of Ultrasonic Activation on Root Canal Filling Quality of Single-Cone Obturation with Calcium Silicate-Based Sealer

 , , ,
, , , 
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Materials and Methods
2.1. Preparation of Tooth Samples
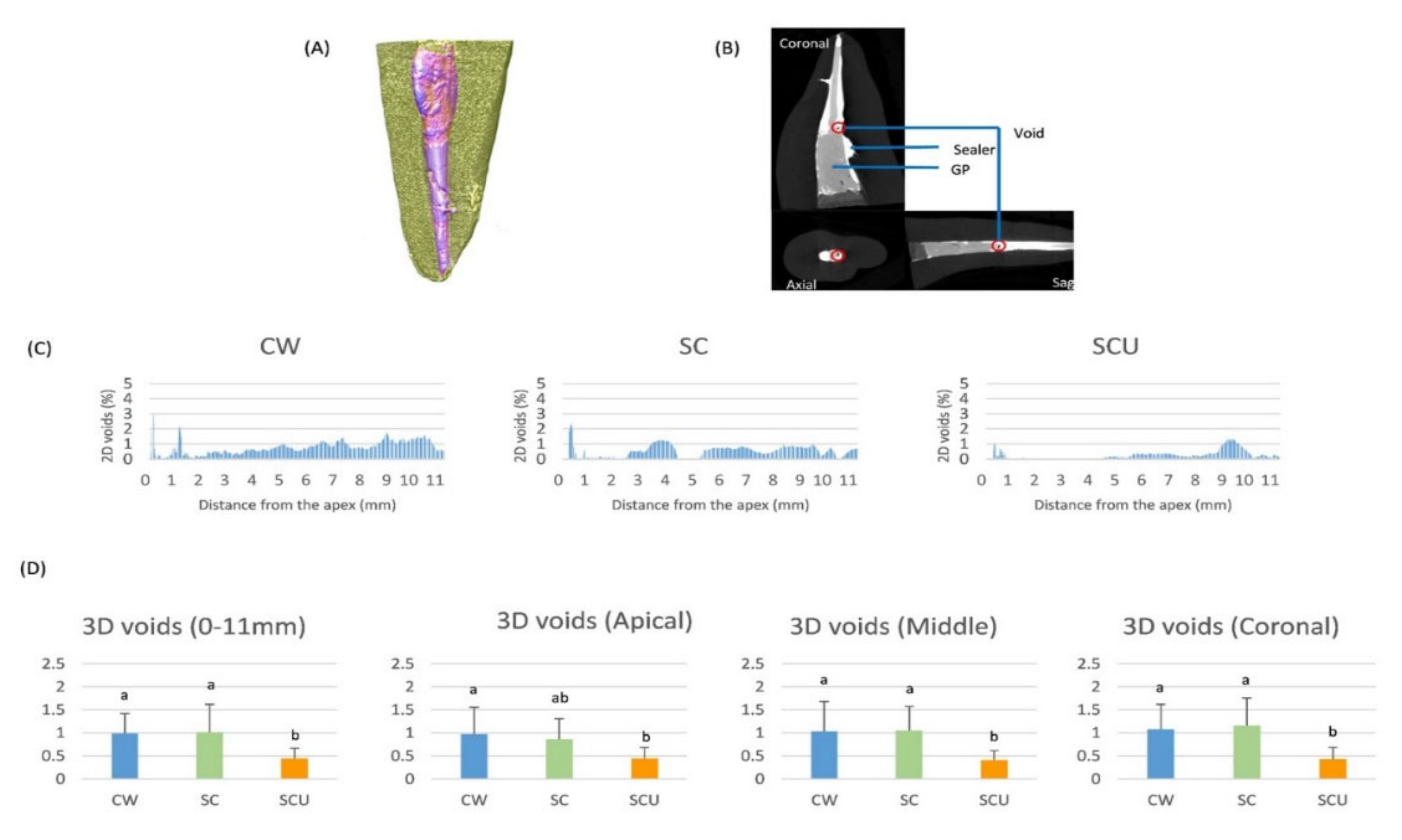
2.2. Micro-CT Evaluation
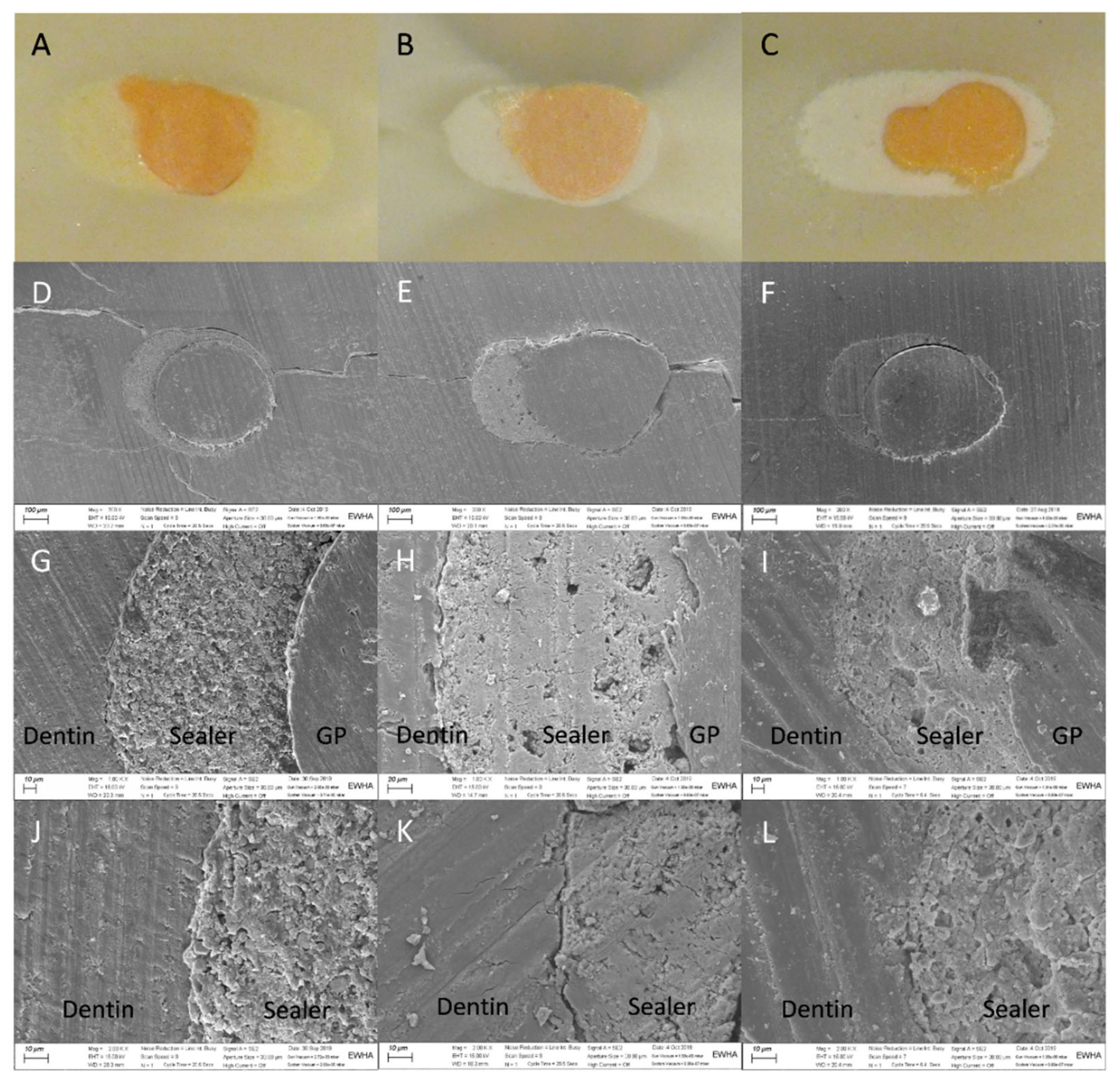
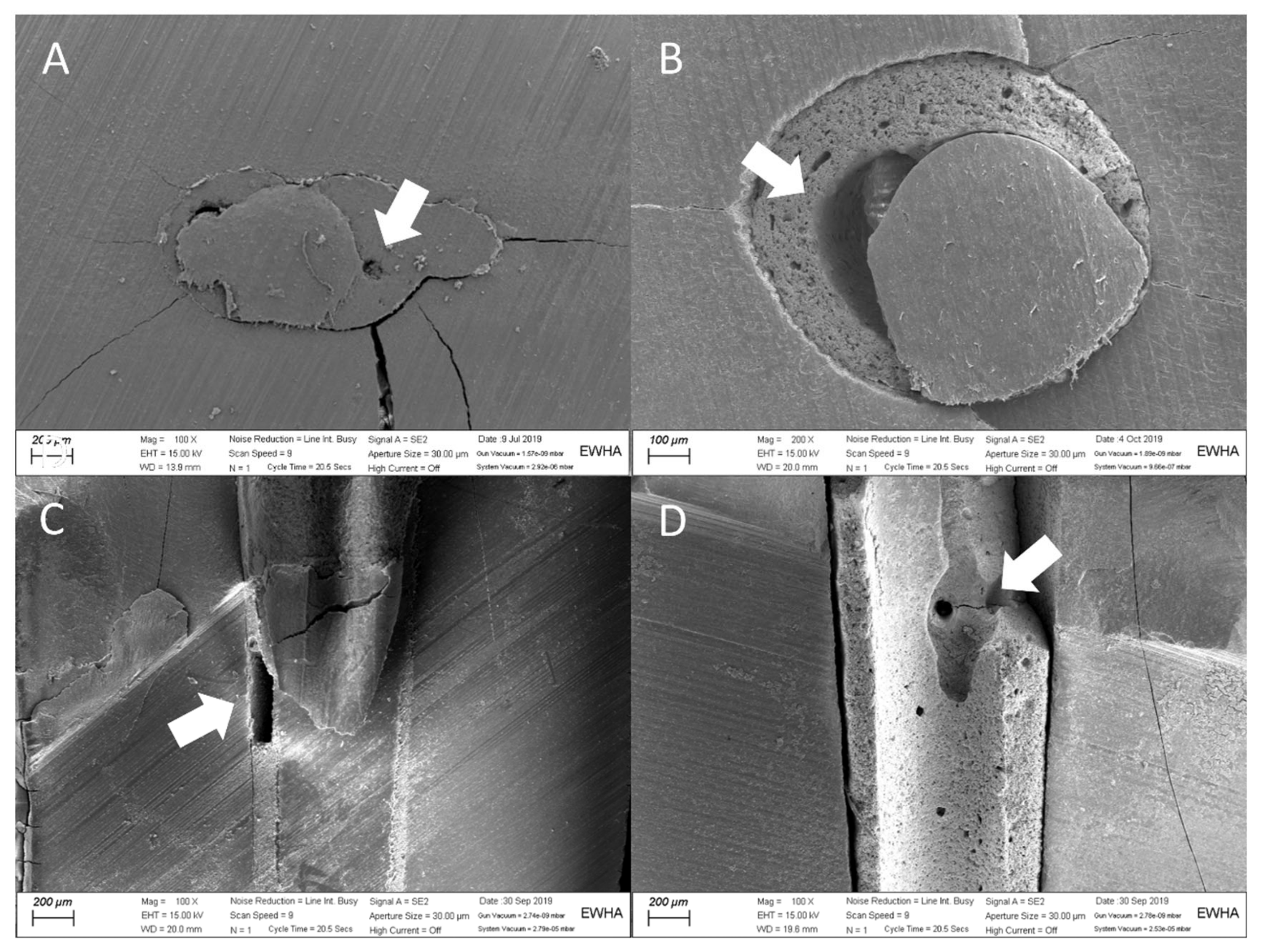
2.3. Light Microscopy and Scanning Electron Microscopy
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Ray, H.A.; Trope, M. Periapical status of endodontically treated teeth in relation to the technical quality of the root filling and the coronal restoration. Int. Endod. J. 1995, 28, 12–18. [Google Scholar] [CrossRef]
- Tay, F.R.; Hosoya, Y.; Loushine, R.J.; Pashley, D.H.; Weller, R.N.; Low, D.C. Ultrastructure of intraradicular dentin after irrigation with BioPure MTAD. II. The consequence of obturation with an epoxy resin-based sealer. J. Endod. 2006, 32, 473–477. [Google Scholar] [CrossRef]
- Zhang, W.; Li, Z.; Peng, B. Assessment of a new root canal sealer’s apical sealing ability. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endodontol. 2009, 107, e79–e82. [Google Scholar] [CrossRef]
- Silva, E.J.; Carvalho, N.K.; Prado, M.C.; Zanon, M.; Senna, P.M.; Souza, E.M.; De-Deus, G. Push-out Bond Strength of Injectable Pozzolan-based Root Canal Sealer. J. Endod. 2016, 42, 1656–1659. [Google Scholar] [CrossRef] [PubMed]
- Giacomino, C.M.; Wealleans, J.A.; Kuhn, N.; Diogenes, A. Comparative Biocompatibility and Osteogenic Potential of Two Bioceramic Sealers. J. Endod. 2019, 45, 51–56. [Google Scholar] [CrossRef]
- Lee, B.N.; Hong, J.U.; Kim, S.M.; Jang, J.H.; Chang, H.S.; Hwang, Y.C.; Hwang, I.N.; Oh, W.M. Anti-inflammatory and Osteogenic Effects of Calcium Silicate-based Root Canal Sealers. J. Endod. 2019, 45, 73–78. [Google Scholar] [CrossRef] [PubMed]
- Jeong, J.W.; DeGraft Johnson, A.; Dorn, S.O.; di Fiore, P.M. Dentinal Tubule Penetration of a Calcium Silicate-based Root Canal Sealer with Different Obturation Methods. J. Endod. 2017, 43, 633–637. [Google Scholar] [CrossRef] [PubMed]
- Nagas, E.; Uyanik, M.O.; Eymirli, A.; Cehreli, Z.C.; Vallittu, P.K.; Lassila, L.V.; Durmaz, V. Dentin moisture conditions affect the adhesion of root canal sealers. J. Endod. 2012, 38, 240–244. [Google Scholar] [CrossRef]
- Celikten, B.; Uzuntas, C.F.; Orhan, A.I.; Orhan, K.; Tufenkci, P.; Kursun, S.; Demiralp, K.O. Evaluation of root canal sealer filling quality using a single-cone technique in oval shaped canals: An In vitro Micro-CT study. Scanning 2016, 38, 133–140. [Google Scholar] [CrossRef] [PubMed]
- Guivarc’h, M.; Jeanneau, C.; Giraud, T.; Pommel, L.; About, I.; Azim, A.A.; Bukiet, F. An international survey on the use of calcium silicate-based sealers in non-surgical endodontic treatment. Clin. Oral Investig. 2020, 24, 417–424. [Google Scholar] [CrossRef] [PubMed]
- Ersahan, S.; Aydin, C. Solubility and apical sealing characteristics of a new calcium silicate-based root canal sealer in comparison to calcium hydroxide-, methacrylate resin- and epoxy resin-based sealers. Acta Odontol. Scand. 2013, 71, 857–862. [Google Scholar] [CrossRef] [PubMed]
- Iglecias, E.F.; Freire, L.G.; de Miranda Candeiro, G.T.; Dos Santos, M.; Antoniazzi, J.H.; Gavini, G. Presence of Voids after Continuous Wave of Condensation and Single-cone Obturation in Mandibular Molars: A Micro-computed Tomography Analysis. J. Endod. 2017, 43, 638–642. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.A.; Hwang, Y.C.; Rosa, V.; Yu, M.K.; Lee, K.W.; Min, K.S. Root Canal Filling Quality of a Premixed Calcium Silicate Endodontic Sealer Applied Using Gutta-percha Cone-mediated Ultrasonic Activation. J. Endod. 2018, 44, 133–138. [Google Scholar] [CrossRef] [Green Version]
- Parashos, P.; Phoon, A.; Sathorn, C. Effect of ultrasonication on physical properties of mineral trioxide aggregate. Biomed Res. Int. 2014, 2014, 191984. [Google Scholar] [CrossRef]
- El-Ma’aita, A.M.; Qualtrough, A.J.; Watts, D.C. A micro-computed tomography evaluation of mineral trioxide aggregate root canal fillings. J. Endod. 2012, 38, 670–672. [Google Scholar] [CrossRef]
- Selem, L.C.; Li, G.H.; Niu, L.N.; Bergeron, B.E.; Bortoluzzi, E.A.; Chen, J.H.; Pashley, D.H.; Tay, F.R. Quality of obturation achieved by a non-gutta-percha-based root filling system in single-rooted canals. J. Endod. 2014, 40, 2003–2008. [Google Scholar] [CrossRef] [PubMed]
- Ng, Y.L.; Mann, V.; Rahbaran, S.; Lewsey, J.; Gulabivala, K. Outcome of primary root canal treatment: Systematic review of the literature—Part 2. Influence of clinical factors. Int. Endod. J. 2008, 41, 6–31. [Google Scholar] [CrossRef] [PubMed]
- Editorial Board of the Journal of Endodontics. Wanted: A base of evidence. J. Endod. 2007, 33, 1401–1402. [Google Scholar] [CrossRef]
- Wolf, M.; Kupper, K.; Reimann, S.; Bourauel, C.; Frentzen, M. 3D analyses of interface voids in root canals filled with different sealer materials in combination with warm gutta-percha technique. Clin. Oral Investig. 2014, 18, 155–161. [Google Scholar] [CrossRef]
- Kim, S.; Park, J.; Jung, I.; Shin, S. Comparison of the Percentage of Voids in the Canal Filling of a Calcium Silicate-Based Sealer and Gutta Percha Cones Using Two Obturation Techniques. Materials 2017, 10, 1170. [Google Scholar] [CrossRef] [Green Version]
- Pawar, S.S.; Pujar, M.A.; Makandar, S.D. Evaluation of the apical sealing ability of bioceramic sealer, AH plus & epiphany: An in vitro study. J. Conserv. Dent. 2014, 17, 579–582. [Google Scholar]
- Horsted-Bindslev, P.; Andersen, M.A.; Jensen, M.F.; Nilsson, J.H.; Wenzel, A. Quality of molar root canal fillings performed with the lateral compaction and the single-cone technique. J. Endod. 2007, 33, 468–471. [Google Scholar] [CrossRef]
- Schafer, E.; Schrenker, C.; Zupanc, J.; Burklein, S. Percentage of Gutta-percha Filled Areas in Canals Obturated with Cross-linked Gutta-percha Core-carrier Systems, Single-Cone and Lateral Compaction Technique. J. Endod. 2016, 42, 294–298. [Google Scholar] [CrossRef] [PubMed]
- Robberecht, L.; Colard, T.; Claisse Crinquette, A. Qualitative evaluation of two endodontic obturation techniques: Tapered single-cone method versus warm vertical condensation and injection system: An in vitro study. J. Oral Sci. 2012, 54, 99–104. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schafer, E.; Nelius, B.; Burklein, S. A comparative evaluation of gutta-percha filled areas in curved root canals obturated with different techniques. Clin. Oral Investig. 2012, 16, 225–230. [Google Scholar] [CrossRef] [PubMed]
- Somma, F.; Cretella, G.; Carotenuto, M.; Pecci, R.; Bedini, R.; de Biasi, M.; Angerame, D. Quality of thermoplasticized and single point root fillings assessed by micro-computed tomography. Int. Endod. J. 2011, 44, 362–369. [Google Scholar] [CrossRef]
- Jung, I.-Y.; Lee, S.-B.; Kim, E.-S.; Lee, C.-Y.; Lee, S.-J. Effect of different temperatures and penetration depths of a System B plugger in the filling of artificially created oval canals. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endodontol. 2003, 96, 453–457. [Google Scholar] [CrossRef]
- Wu, S.D.; van der Sluis, L.W.; Wesselink, P.R. A preliminary study of the percentage of gutta-percha-filled area in the apical canal filled with vertically compacted warm gutta-percha. Int. Endod. J. 2002, 35, 527–535. [Google Scholar] [CrossRef]
- Moinzadeh, A.T.; Zerbst, W.; Boutsioukis, C.; Shemesh, H.; Zaslansky, P. Porosity distribution in root canals filled with gutta percha and calcium silicate cement. Dent. Mater. 2015, 31, 1100–1108. [Google Scholar] [CrossRef]



Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, S.-Y.; Jang, Y.-E.; Kim, B.S.; Pang, E.-K.; Shim, K.; Jin, H.R.; Son, M.K.; Kim, Y. Effects of Ultrasonic Activation on Root Canal Filling Quality of Single-Cone Obturation with Calcium Silicate-Based Sealer. Materials 2021, 14, 1292. https://doi.org/10.3390/ma14051292
Kim S-Y, Jang Y-E, Kim BS, Pang E-K, Shim K, Jin HR, Son MK, Kim Y. Effects of Ultrasonic Activation on Root Canal Filling Quality of Single-Cone Obturation with Calcium Silicate-Based Sealer. Materials. 2021; 14(5):1292. https://doi.org/10.3390/ma14051292
Chicago/Turabian StyleKim, Sin-Young, Young-Eun Jang, Bom Sahn Kim, Eun-Kyoung Pang, Kiche Shim, Hye Ryeon Jin, Min Kyung Son, and Yemi Kim. 2021. "Effects of Ultrasonic Activation on Root Canal Filling Quality of Single-Cone Obturation with Calcium Silicate-Based Sealer" Materials 14, no. 5: 1292. https://doi.org/10.3390/ma14051292