
Mechanical Properties and Corrosion Behavior of Ti6Al4V Particles Obtained by Implantoplasty: An In Vitro Study. Part II

 , , and
, , and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Sample Preparation
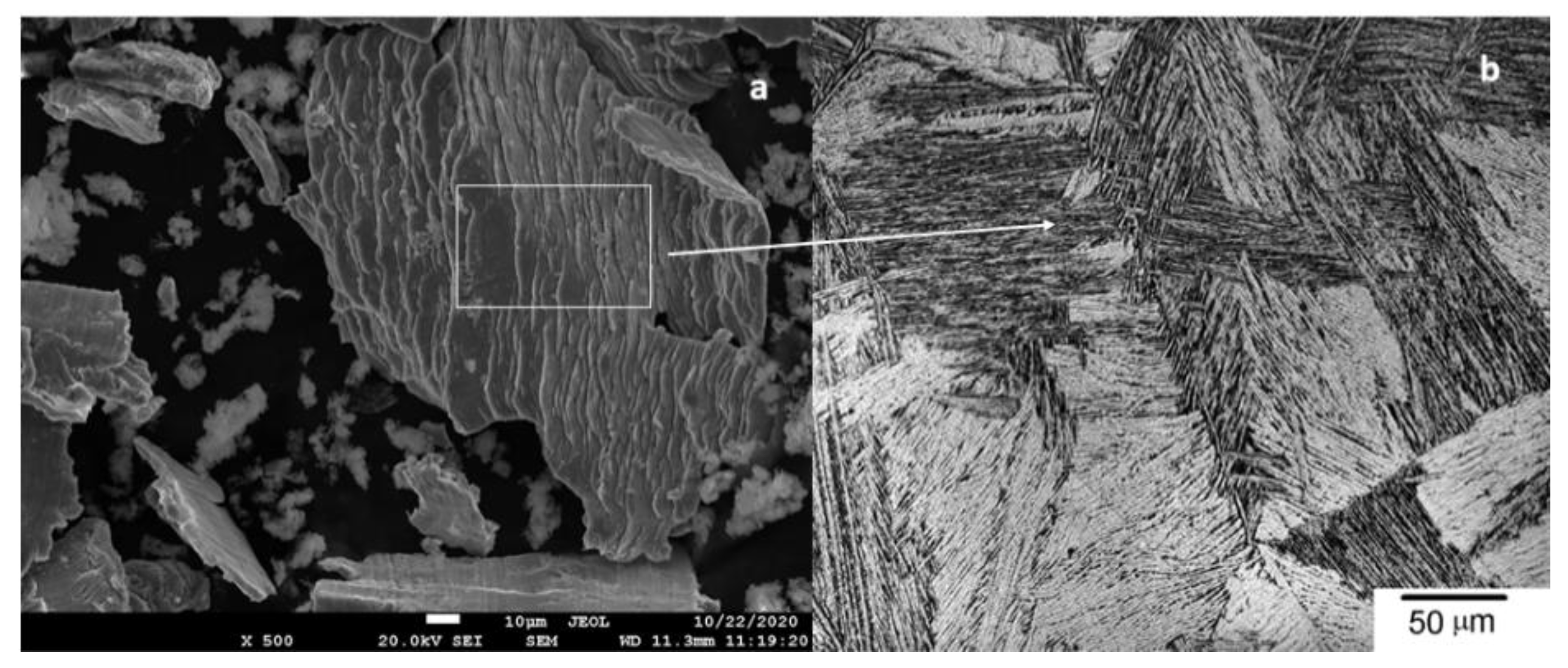
2.2. Scanning Electron Microscopy and Mechanical Properties
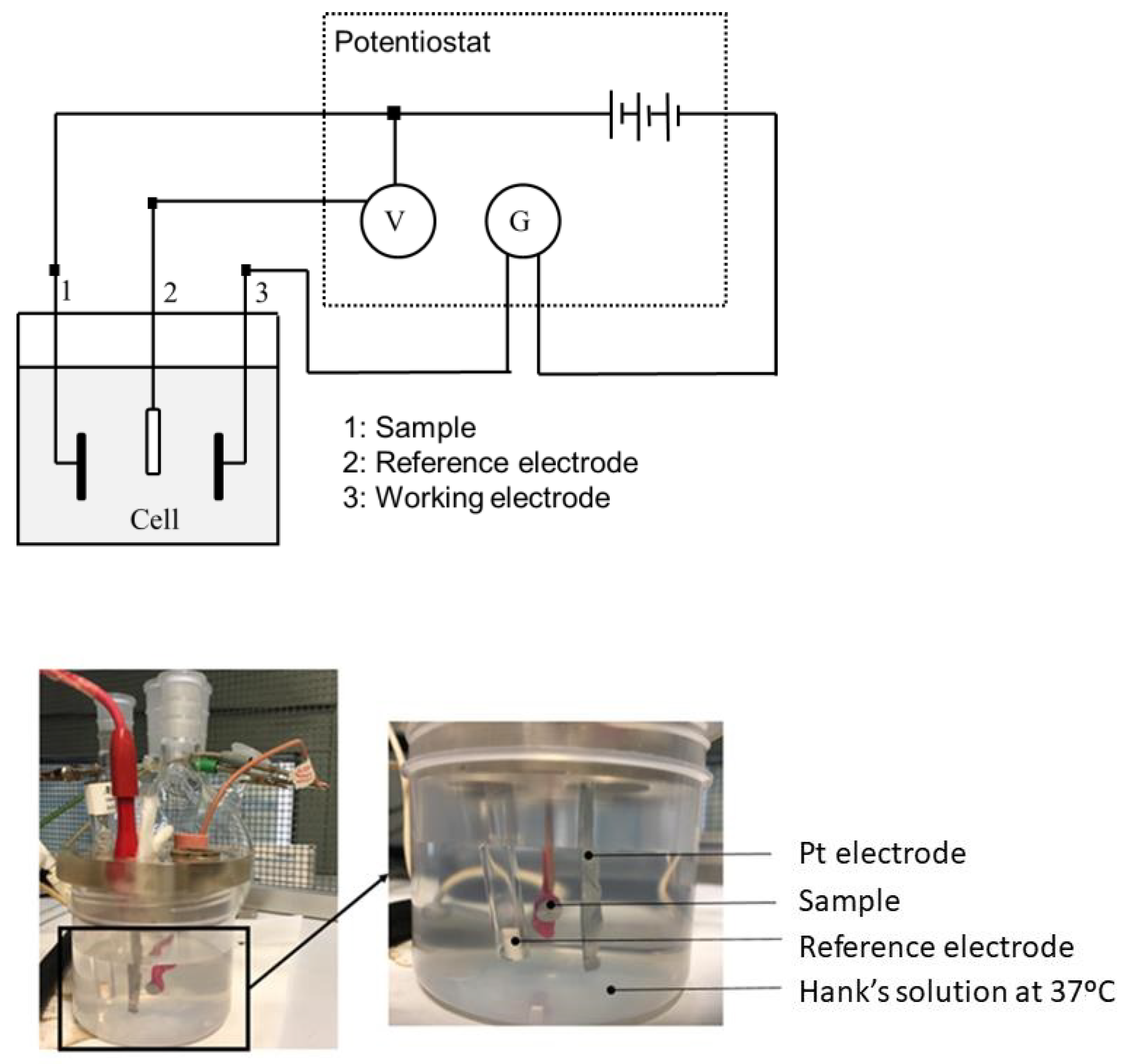
2.3. Corrosion Test
2.3.1. Open Circuit Potential
2.3.2. Potentiodynamic Tests (E-log(I) Curves)
2.4. Statistical Analysis
3. Results
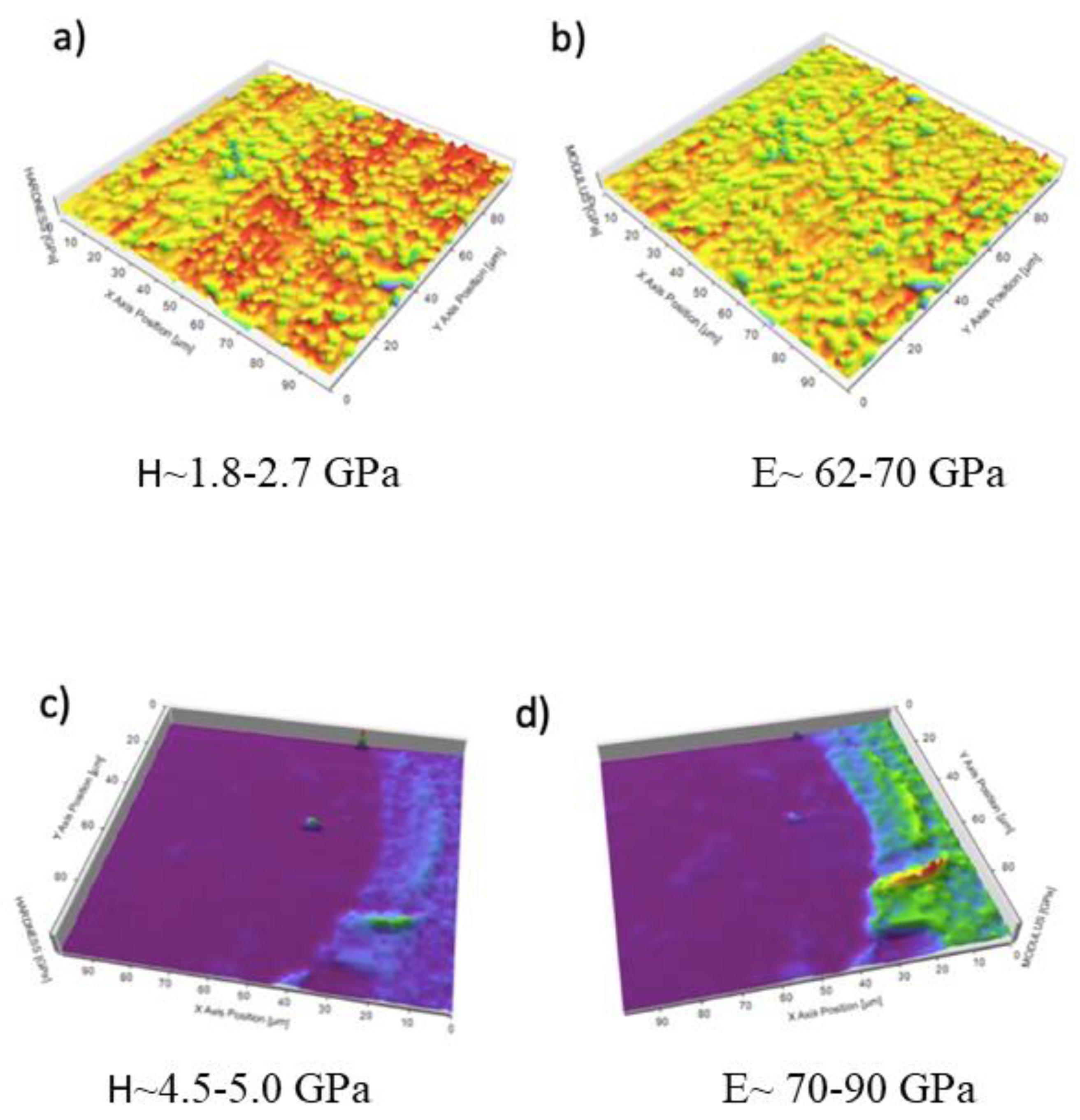
3.1. Scanning Electron Microscopy and Mechanical Properties
3.2. Corrosion Behavior
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Alrabiah, M.; Alrahlah, A.; Al-Hamdan, R.S.; Al-Aali, K.A.; Labban, N.; Abduljabbar, T. Survival of adjacent-dental-implants in prediabetic and systemically healthy subjects at 5-years follow-up. Clin. Implant Dent. Relat. Res. 2019, 21, 232–237. [Google Scholar] [CrossRef]
- Francetti, L.; Cavalli, N.; Taschieri, S.; Corbella, S. Ten years follow-up retrospective study on implant survival rates and prevalence of peri-implantitis in implant-supported full-arch rehabilitations. Clin. Oral Implant. Res. 2019, 30, 252–260. [Google Scholar] [CrossRef]
- Aparicio, C.; Gil, F.J.; Fonseca, C.; Barbosa, M.; Planell, J.A. Corrosion behaviour of commercially pure titanium shot blasted with different materials and sizes of shot blasted with different materials and sizes of shot particles for dental implant applications. Biomaterials 2003, 24, 263–273. [Google Scholar] [CrossRef]
- Ratner, B.D. A Perspective on Titanium Biocompatibility. In Titanium in Medicine: Material Science, Surface Science, Engineering, Biological Responses and Medical Applications; Brunette, D.M., Tengvall, P., Textor, M., Thomsen, P., Eds.; Springer: Berlin, Germany, 2001; pp. 1–12. [Google Scholar]
- Aparicio, C.; Rodríguez, D.; Gil, F.J. Variation of roughness and adhesion strength of deposited apatite layers on titanium dental implants. Mat. Sci. Eng. C 2011, 31, 320–324. [Google Scholar] [CrossRef]
- Zhang, L.C.; Chen, L.Y. A review on biomedical titanium alloys: Recent progress and prospect. Adv. Eng. Mater. 2019, 21, 1801215. [Google Scholar] [CrossRef] [Green Version]
- Dias Corpa Tardelli, J.; Bolfarini, C.; Cândido Dos Reis, A. Comparative analysis of corrosion resistance between beta titanium and Ti6Al4V alloys: A systematic review. J. Trace Elem. Med. Biol. 2020, 62, 126618. [Google Scholar] [CrossRef]
- Berbel, L.O.; Banczek, E.; Karoussis, I.K.; Kotsakis, G.A.; Costa, I. Determinants of corrosion resistance of Ti6Al4V alloy dental implants in an In Vitro model of peri-implant inflammation. PLoS ONE 2019, 14, e0210530. [Google Scholar]
- Gai, X.; Bai, Y.; Li, S.; Hou, W.; Hao, Y.; Zhang, X.; Yang, R.; Misra, R. In-situ monitoring of the electrochemical behavior of cellular structured biomedical Ti6Al4V alloy fabricated by electron beam melting in simulated physiological fluid. Acta Biomater 2020, 106, 387–395. [Google Scholar] [CrossRef]
- Willis, J.; Li, S.; Crean, S.J.; Barrak, F.N. Is titanium alloy Ti-6Al-4 V cytotoxic to gingival fibroblasts—A systematic review. Clin. Exp. Dent. Res. 2021. [Google Scholar] [CrossRef]
- Challa, V.S.; Mali, S.; Misra, R.D. Reduced toxicity and superior cellular response of preosteoblasts to Ti-6Al-7Nb alloy and comparison with Ti6Al4V. J. Biomed. Mater. Res. A 2013, 101, 2083–2089. [Google Scholar] [CrossRef] [PubMed]
- Schwarz, F.; Derks, J.; Monje, A.; Wang, H.L. Peri-implantitis. J. Clin. Periodontol. 2018, 45, 246–266. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Figuero, E.; Graziani, F.; Sanz, I.; Herrera, D.; Sanz, M. Management of peri-implant mucositis and peri-implantitis. Periodontology 2014, 66, 255–273. [Google Scholar] [CrossRef] [PubMed]
- Batalha, V.C.; Bueno, R.A.; Fronchetti Junior, E.; Mariano, J.R.; Santin, G.C.; Freitas, K.M.S.; Ortiz, M.A.L.; Salmeron, S. Dental implants surface in vitro decontamination protocols. Eur. J. Dent. 2021, 15, 407–411. [Google Scholar] [CrossRef] [PubMed]
- Buser, D. Titanium for dental applications (I). In Titanium in Medicine: Material Science, Surface Science, Engineering, Biological Responses and Medical Applications; Brunette, D.M., Tengvall, P., Textor, M., Thomsen, P., Eds.; Springer: Berlin, Germany, 2001; pp. 875–888. [Google Scholar]
- Thomsen, P.; Larsson, C.; Ericsson, L.E.; Sennerby, L.; Lausmaa, J.; Kasemo, B. Bone response to machined cast titanium implants. J. Mater. Sci. Mater. Med. 1997, 8, 653–665. [Google Scholar] [CrossRef]
- Pegueroles, M.; Tonda-Turo, C.; Planell, J.A.; Gil, F.J.; Aparicio, C. Adsorption of fibronectin, fibrinongen, and albumin on TiO2: Time-resolved kinetics, structural changes, and competition study. Biointerphases 2012, 7, 48–61. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Guillem, J.; Delgado, L.; Godoy-Gallardo, M.; Pegueroles, M.; Herrero, M.; Gil, F.J. Fibroblast adhesion and activation onto micro-machined titanium surfaces. Clin. Oral Implant. Res. 2013, 24, 770–780. [Google Scholar] [CrossRef]
- Pegueroles, M.; Aparicio, C.; Bosio, M.; Engel, E.; Gil, F.J.; Planell, J.A.; Altankov, G. Spatial organization of osteoblast fibronectin-matrix on titanium surface—Effects of roughness, chemical heterogeneity, and surface free energy. Acta Biomater. 2010, 6, 291–301. [Google Scholar] [CrossRef]
- Williams, D.F. Titanium for medical applications. In Titanium in Medicine: Material Science, Surface Science, Engineering, Biological Responses and Medical Applications; Brunette, D.M., Tengvall, P., Textor, M., Thomsen, P., Eds.; Springer: Berlin, Germany, 2001; pp. 13–24. [Google Scholar]
- Schliephake, H.; Scharnweber, D. Chemical and biological functionalization of titanium for dental implants. J. Mater. Chem. 2008, 18, 2404–2414. [Google Scholar] [CrossRef]
- Brunski, J.B. Classes of materials used in medicine. Metals. In Biomaterials Science, an Introduction to Materials in Medicine; Rutner, B., Hoffman, A., Schoen, F., Lemons, J., Eds.; Academic Press: San Diego, CA, USA, 1996; pp. 137–152. [Google Scholar]
- Velasco-Ortega, E.; Jiménez-Guerra, A.; Monsalve-Guil, L.; Ortiz-García, I.; Nicolás-Silvente, A.I.; Segura-Egea, J.J.; Lopez-Lopez, J. Long-term clinical outcomes of treatment with dental implants with acid etched surface. Materials 2020, 13, 1553. [Google Scholar] [CrossRef] [Green Version]
- Manero, J.M.; Gil, F.J.; Padrós, A.; Planell, J.A. Applications of environmental scanning electron microscopy (ESEM) in biomaterials field. Microsc. Res. Tech. 2003, 61, 469–480. [Google Scholar] [CrossRef]
- Delgado-Ruiz, R.; Romanos, G. Potential causes of titanium particle and ion release in implant dentistry: A systematic review. Int. J. Mol. Sci. 2018, 19, 3585. [Google Scholar] [CrossRef] [Green Version]
- Costa-Berenguer, X.; García-García, M.; Sánchez-Torres, A.; Sanz-Alonso, M.; Figueiredo, R.; Valmaseda-Castellón, E. Effect of implantoplasty on fracture resistance and surface roughness of standard diameter dental implants. Clin. Oral Implant. Res. 2018, 29, 46–54. [Google Scholar] [CrossRef]
- Camps-Font, O.; González-Barnadas, A.; Mir-Mari, J.; Figueiredo, R.; Gay-Escoda, C.; Valmaseda-Castellón, E. Fracture resistance after implantoplasty in three implant-abutment connection designs. Med. Oral Patol. Oral Cir. Bucal 2020, 25, 691–699. [Google Scholar] [CrossRef]
- Velasco, E.; Monsalve-Guil, L.; Jimenez, A.; Ortiz, I.; Moreno-Muñoz, J.; Nuñez-Marquez, E.; Pegueroles, M.; Pérez, R.A.; Gil, F.J. Importance of the roughness and residual stresses of dental implants on fatigue and osseointegration behavior. In vivo study in rabbits. J. Oral Implantol. 2016, 42, 469–476. [Google Scholar] [CrossRef]
- Pérez, R.A.; Gargallo, J.; Altuna, P.; Herrero-Climent, M.; Gil, F.J. Fatigue of narrow dental implants: Influence of the hardening method. Materials 2020, 13, 1429. [Google Scholar] [CrossRef] [Green Version]
- ASTM-E3-11. Standard Guide for Preparation of Metallographic Specimens; ASTM International: West Conshohocken, PA, USA, 2017. [Google Scholar]
- Standard Reference Test Method for Making Potentiostatic and Potentiodynamic Anodic Polarization Measurements; Technical Report no. ASTM G5-14e1; ASTM International: West Conshohocken, PA, USA, 2014.
- ISO 10993-5:2009. Part 5: Tests for In Vitro Cytotoxicity. In Biological Evaluation of Medical Devices; International Organization for Standardization: Geneve, Switzerland, 2009.
- Mansfeld, F.; Kenkel, J.V. Laboratory studies of galvanic corrosion of aluminium alloys. In Galvanic and Pitting Corrosion-Field and Laboratory Studies; Baboian, R., France, W., Roew, L., Rynewicz, J., Eds.; ASTM: Philadelphia, PA, USA, 1976; pp. 20–47. [Google Scholar]
- Mansfeld, F. The polarization resistance technique for measuring corrosion currents. In Advances in Corrosion Science and Technology; Fontana, M.G., Staehle, R.W., Eds.; Springer: Boston, MA, USA, 1976; pp. 89–92. [Google Scholar]
- Canay, S.; Öktemer, M. In vitro corrosion behaviour of 13 prosthodontic alloys. Quintessence Int. 1992, 23, 279–287. [Google Scholar]
- Senna, P.; Antoninha Del Bel Cury, A.; Kates, S.; Meirelles, L. Surface damage on dental implants with release of loose particles after insertion into bone. Clin. Implant. Dent. Relat. Res. 2015, 17, 681–692. [Google Scholar] [CrossRef] [Green Version]
- Barbieri, M.; Mencio, F.; Papi, P.; Rosella, D.; Di Carlo, S.; Valente, T.; Pompa, G. Corrosion behavior of dental implants immersed into human saliva: Preliminary results of an in vitro study. Eur. Rev. Med. Pharmacol. Sci. 2017, 21, 3543–3548. [Google Scholar]
- Boyer, R.; Welsch, G.; Collings, W. Materials Properties Handbook: Titanium Alloys; ASM International: Novelty, OH, USA, 1994. [Google Scholar]
- Reclaru, L.; Meyer, J.M. Study of corrosion between a titanium implant and dental alloys. J. Dent. 1994, 22, 159–168. [Google Scholar] [CrossRef]
- Ginebra, M.P.; Gil, F.J.; Manero, J.M.; Planell, J.A. Formation of α- Widmanstatten structure: Effects of grain size and cooling rate on the Widmanstatten morphologies and on the mechanical properties in Ti6Al4V alloy. J. Alloys Compd. 2001, 329, 142–152. [Google Scholar]
- Gil, F.J.; Manero, J.M.; Ginebra, M.P.; Planell, J.A. The effect of cooling rate on the cyclic deformation of β-annealed Ti6Al4V. Mat. Sci. Eng. 2003, 349, 150–155. [Google Scholar] [CrossRef]
- Manero, J.M.; Gil, F.J.; Planell, J.A. Deformation mechanisms of Ti6Al4V alloy with a martensitic microstructure subjected to oligocyclic fatigue. Acta Mater. 2000, 48, 3353–3359. [Google Scholar] [CrossRef]
- Gil, F.J.; Planell, J.A.; Padrós, A.; Planell, J.A. Fracture and fatigue behaviour of shot blasted titanium dental implants. Impl. Dent. 2002, 11, 28–32. [Google Scholar] [CrossRef] [PubMed]
- Porter, D.A.; Easterling, K.E.; Sheriff, M. Phase Transformation in Metals and Alloys, 3rd ed.; CRC Press: Boca Raton, FL, USA, 2013. [Google Scholar]
- Geis-Gerstorfer, J. In vitro corrosion measurements of dental alloys. J. Dent. 1994, 22, 247–251. [Google Scholar] [CrossRef]
- Gil, F.J.; Planell, J.A.; Padrós, A.; Aparicio, C. The effect of shot blasting and heat treatment on the fatigue behavior of titanium for dental implant applications. Dent. Mater. 2007, 23, 486–491. [Google Scholar] [CrossRef]
- Gil, F.J.; Espinar, E.; Llamas, J.M.; Sevilla, P. Fatigue life of bioactive titanium dental implants treated by means of grit-blasting and thermo-chemical treatment. Clin. Implant. Dent. Relat. Res. 2014, 16, 273–281. [Google Scholar] [CrossRef]
- Wataha, J.C.; Lockwood, P.E.; Khajotia, S.S. Effect of pH on element release from dental casting alloys. J. Prosthet. Dent. 1998, 80, 691–698. [Google Scholar] [CrossRef]
- Gil, F.J.; Rodríguez, D.; Planell, J.A.; Cortada, M.; Giner, L.; Costa, S. Galvanic corrosion behaviour of Titanium implants coupled to dental alloys. J. Mat. Sci. Mat. Med. 2000, 11, 287–293. [Google Scholar] [CrossRef]
- Brånemark, P.I.; Hansson, I.; Adell, R.; Lindstrom, U.; Hallen, J.; Ohman, O. Osseointegrated implants in the treatment of the edentulous jaw. Experience from a 10-year period. Scand. J. Plast. Reconstr. Surg. Suppl. 1977, 16, 1–132. [Google Scholar] [PubMed]
- Adell, R.; Lekholm, U.; Rocker, U.; Brånemark, P.I. A 15-year study of osseointegrated implants in the treatment of the treatment of the edentulous jaw. Int. J. Oral Surg. 1981, 6, 387–416. [Google Scholar] [CrossRef]
- Sarkar, N.K.; Fuys, R.A.; Stanford, J.W. Applications of electrochemical techniques to characterize the corrosion of dental alloys. In Corrosion and Degradation of Implant Materials; Syrett, B.C., Acharya, A., Eds.; ASTM: Philadelphia, PA, USA, 1979; pp. 277–294. [Google Scholar]
- Hosoki, M.; Bando, E.; Asaoka, K.; Takeuchi, H.; Nishigawa, K. Assessment of allergic hypersensivity to dental materials. Biomed. Mater. Eng. 2009, 19, 53–61. [Google Scholar] [CrossRef] [PubMed]
- Mombelli, A.; Hashim, D.; Cionca, N. What is the impact of titanium particles and bioocorrosion on implant survival and complications? A critical review. Clin. Oral Implant. Res. 2018, 29, 37–53. [Google Scholar] [CrossRef]
- Harloff, T.; Hönle, W.; Holzwarth, U.; Bader, R.; Yhomas, P.; Schuh, A. Titanium allergy or not? “Impurity” of titanium implant materials. Health 2010, 2, 306–310. [Google Scholar] [CrossRef] [Green Version]
- Chaturvedi, T. Allergy related to dental implant and its clinical significance. Clin. Cosmet. Investig. Dent. 2013, 5, 57–61. [Google Scholar] [CrossRef] [PubMed] [Green Version]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Chemical Composition | NaCl | KCl | Na2HPO4 | KH2PO4 | CaCl2 | MgSO4 | NaHCO3 | C6H1206 |
|---|---|---|---|---|---|---|---|---|
| Concentration (mM) | 137 | 5.4 | 0.25 | 0.44 | 1.3 | 1.0 | 4.2 | 5.5 |
| Load, (mN) | Mean Indentation Depth (SD), (mm) | Mean Hardness (SD), (GPa) | Mean Elastic Modulus (SD), (GPa) |
|---|---|---|---|
| 1 | 89 (3) | 2.89 (0.39) | 70 (5) |
| 2 | 135 (5) | 2.28 (0.44) | 66 (4) |
| 3 | 168 (5) | 2.56 (0.33) | 65 (3) |
| 4 | 197 (5) | 2.53 (0.33) | 65 (3) |
| Samples | Mean Hardness (SD), (GPa) | Mean Elastic Modulus (SD), (GPa) | Max Deformation (SD), (%) | Residual Stress (SD), (MPa) |
|---|---|---|---|---|
| Control disks | 2.2 (1.2) | 65 (5) | 12.0 (4.2) | −27.5 (5.2) |
| Implantoplasty | 4.8 (1.0) | 80 (9) | 4.3 (0.7) | −354.5 (35.2) |
| Ti cold-worked disks | 4.7 (0.9) | 78 (8) | 4.0 (0.5) | −345 (3.2) |
| Samples | Ecorr (SD), (mV) | Icorr (SD), (μA/cm2) | Polarization Resistance (SD), (Ω/cm2) | Corrosion Rate (SD), (mm/Year) |
|---|---|---|---|---|
| Control disks | −340 (32) | 0.051 (0.007) | 1.14 × 106 (1.13 × 105) | 4.44 × 10−4 (6.69 × 10−5) |
| Implantoplasty | −368 (47) | 0.055 (0.005) | 1.07 × 106 (1.77 × 105) | 4.77 × 10−4 (4.46 × 10−5) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Toledano-Serrabona, J.; Sánchez-Garcés, M.Á.; Gay-Escoda, C.; Valmaseda-Castellón, E.; Camps-Font, O.; Verdeguer, P.; Molmeneu, M.; Gil, F.J. Mechanical Properties and Corrosion Behavior of Ti6Al4V Particles Obtained by Implantoplasty: An In Vitro Study. Part II. Materials 2021, 14, 6519. https://doi.org/10.3390/ma14216519
Toledano-Serrabona J, Sánchez-Garcés MÁ, Gay-Escoda C, Valmaseda-Castellón E, Camps-Font O, Verdeguer P, Molmeneu M, Gil FJ. Mechanical Properties and Corrosion Behavior of Ti6Al4V Particles Obtained by Implantoplasty: An In Vitro Study. Part II. Materials. 2021; 14(21):6519. https://doi.org/10.3390/ma14216519
Chicago/Turabian StyleToledano-Serrabona, Jorge, Maria Ángeles Sánchez-Garcés, Cosme Gay-Escoda, Eduard Valmaseda-Castellón, Octavi Camps-Font, Pablo Verdeguer, Meritxell Molmeneu, and Francisco Javier Gil. 2021. "Mechanical Properties and Corrosion Behavior of Ti6Al4V Particles Obtained by Implantoplasty: An In Vitro Study. Part II" Materials 14, no. 21: 6519. https://doi.org/10.3390/ma14216519