
Advantages of Porcine Xenograft over Autograft in Sinus Lift: A Randomised Clinical Trial

 , , , and
, , , and
Abstract
:
1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Surgical Procedures
2.3. Radiological Analysis
2.4. Histology Processing and Histomorphometric Analysis
2.5. Statistical Analysis
3. Results
3.1. Patient and Intervention Characteristics
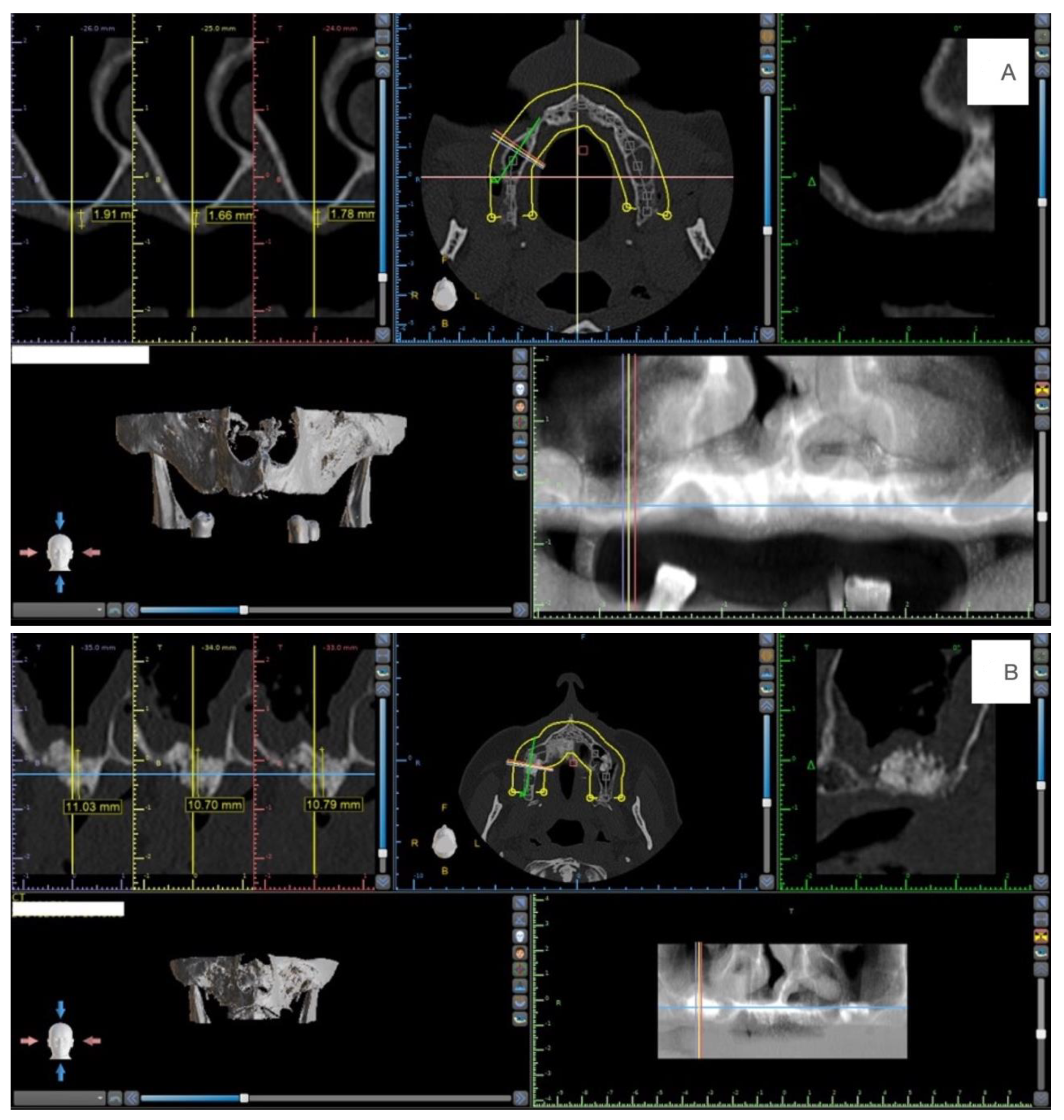
3.2. Radiological Findings
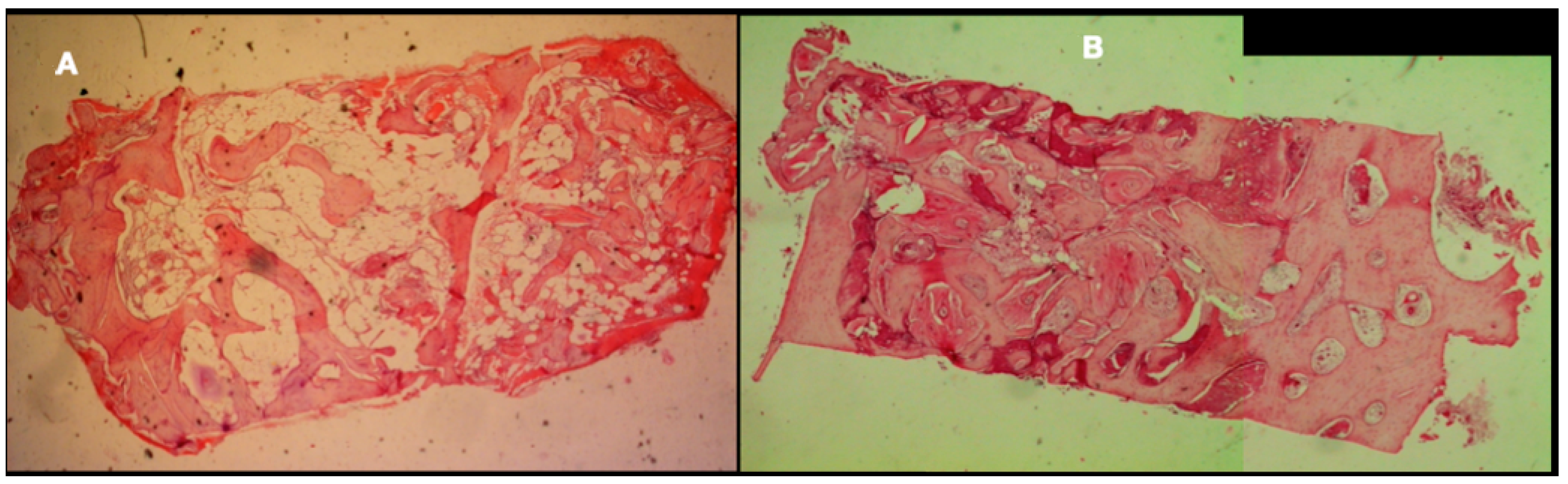
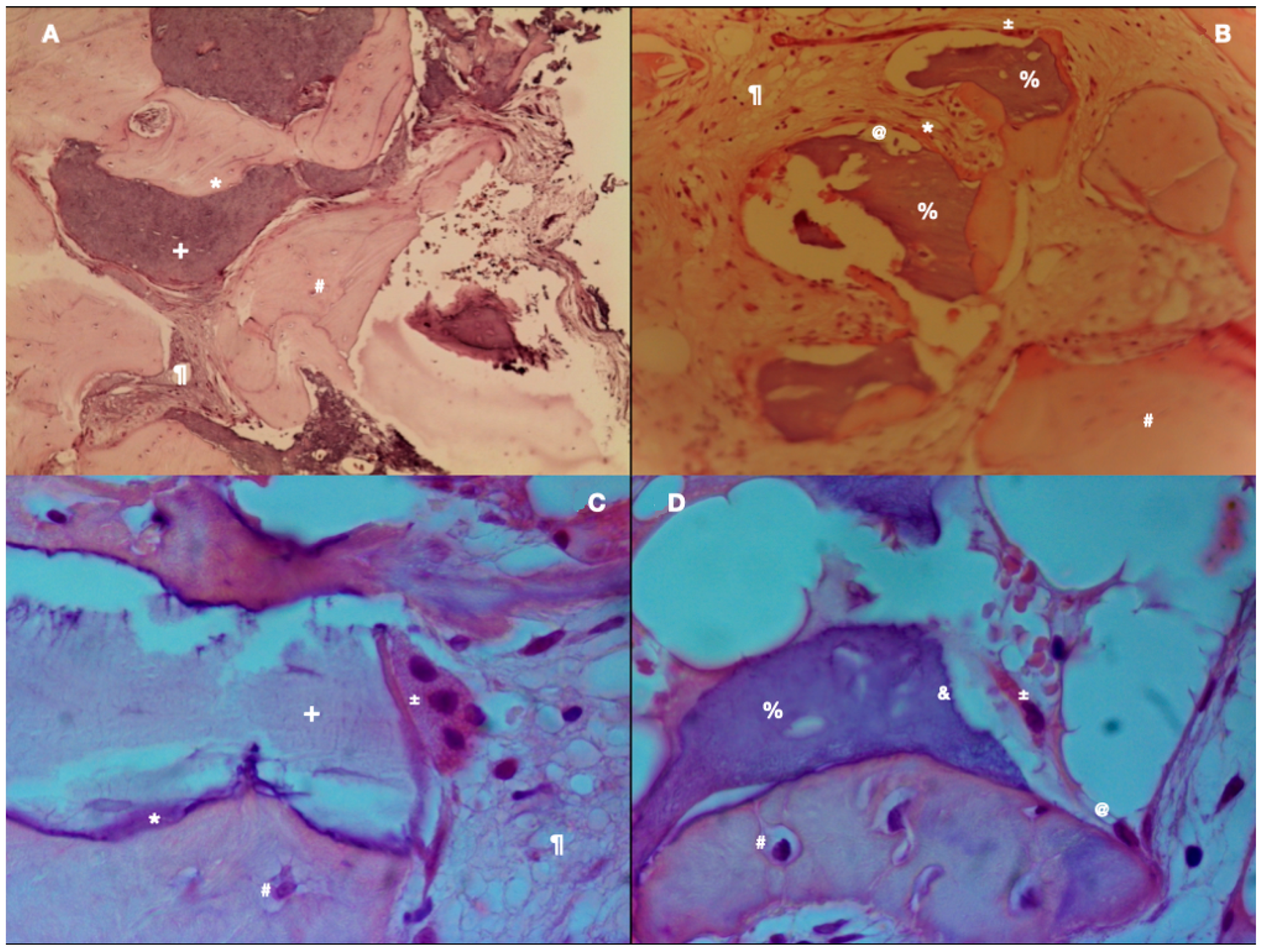
3.3. Histological Findings
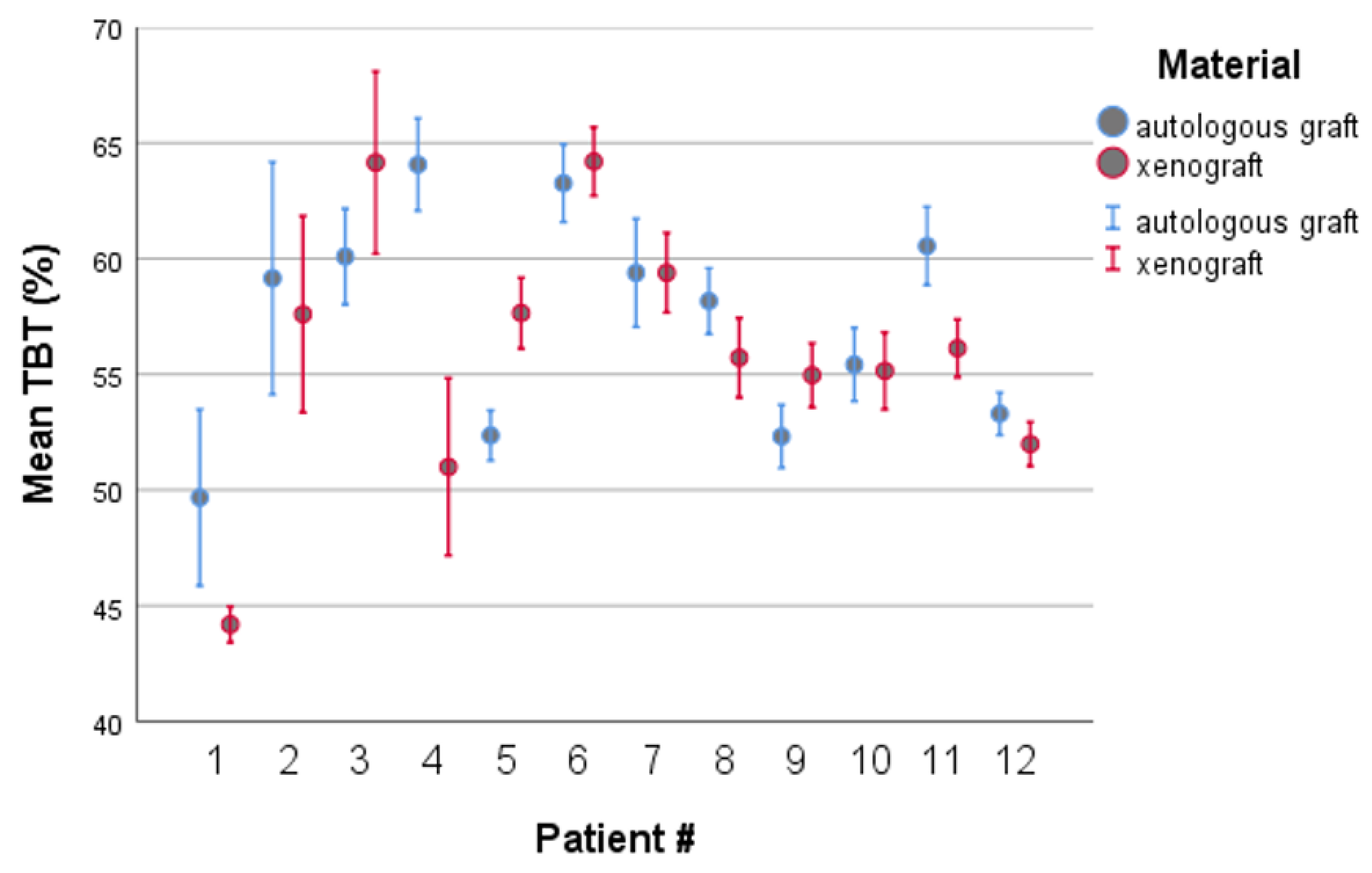
3.4. Histomorphometric Findings
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Jaffin, R.A.; Berman, C.L. The excessive loss of Branemark fixtures in type IV bone: A 5-year analysis. J. Periodontol. 1991, 62, 2–4. [Google Scholar] [CrossRef]
- Lekholm, U.; Zarb, G.A. Patient Selecion. In Tissue Integrated Prsotheses; Branemark, P.-I., Zarb, G.A., Albrektsson, T., Eds.; Quibtessence: Chicago, IL, USA, 1985. [Google Scholar]
- Sharan, A.; Madjar, D. Maxillary sinus pneumatization following extractions: A radiographic study. Int. J. Oral Maxillofac. Implants 2008, 23, 48–56. [Google Scholar]
- Small, S.A.; Zinner, I.D.; Panno, F.V.; Shapiro, H.J.; Stein, J.I. Augmenting the maxillary sinus for implants: Report of 27 patients. Int. J. Oral Maxillofac. Implants 1993, 8, 523–528. [Google Scholar]
- Sanz, M.; Donos, N.; Alcoforado, G.; Balmer, M.; Gurzawska, K.; Mardas, N.; Milinkovic, I.; Nisand, D.; Rocchietta, I.; Stavropoulos, A.; et al. Therapeutic concepts and methods for improving dental implant outcomes. Summary and consensus statements. The 4th EAO Consensus Conference 2015. Clin. Oral Implants Res. 2015, 26 (Suppl. 11), 202–206. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rapani, M.; Rapani, C.; Ricci, L. Schneider membrane thickness classification evaluated by cone-beam computed tomography and its importance in the predictability of perforation. Retrospective analysis of 200 patients. Br. J. Oral Maxillofac. Surg. 2016, 54, 1106–1110. [Google Scholar] [CrossRef] [PubMed]
- Seong, W.J.; Barczak, M.; Jung, J.; Basu, S.; Olin, P.S.; Conrad, H.J. Prevalence of sinus augmentation associated with maxillary posterior implants. J. Oral Implantol. 2013, 39, 680–688. [Google Scholar] [CrossRef]
- Stacchi, C.; Spinato, S.; Lombardi, T.; Bernardello, F.; Bertoldi, C.; Zaffe, D.; Nevins, M. Minimally Invasive Management of Implant-Supported Rehabilitation in the Posterior Maxilla, Part I. Sinus Floor Elevation: Biologic Principles and Materials. Int. J. Periodontics Restor. Dent. 2020, 40, e85–e93. [Google Scholar] [CrossRef] [PubMed]
- Raghoebar, G.M.; Onclin, P.; Boven, G.C.; Vissink, A.; Meijer, H.J.A. Long-term effectiveness of maxillary sinus floor augmentation: A systematic review and meta-analysis. J. Clin. Periodontol. 2019, 46 (Suppl. 21), 307–318. [Google Scholar] [CrossRef] [Green Version]
- Esposito, M.; Grusovin, M.G.; Felice, P.; Karatzopoulos, G.; Worthington, H.V.; Coulthard, P. Interventions for replacing missing teeth: Horizontal and vertical bone augmentation techniques for dental implant treatment. Cochrane Database Syst. Rev. 2009, CD003607. [Google Scholar] [CrossRef]
- Yin, L.; Yu, Z.; Chen, Z.; Huang, B.; Zhang, K.; Zhou, A.; Li, X. Analysis of Bone Height Changes after Maxillary Sinus Augmentation with Simultaneous and Delayed Placement of Dental Implants: A Clinical and Radiographic Study. J. Prosthodont. Off. J. Am. Coll. Prosthodont. 2016, 25, 440–445. [Google Scholar] [CrossRef]
- van Den Bergh, J.P.; Ten Bruggenkate, C.M.; Disch, F.J.; Tuinzing, D.B. Anatomical aspects of sinus floor elevations. Clin. Oral Implants Res. 2000, 11, 256–265. [Google Scholar] [CrossRef] [PubMed]
- McAllister, B.S.; Haghighat, K. Bone augmentation techniques. J. Periodontol. 2007, 78, 377–396. [Google Scholar] [CrossRef] [Green Version]
- Delilbasi, C.; Gurler, G. Comparison of piezosurgery and conventional rotative instruments in direct sinus lifting. Implant Dent. 2013, 22, 662–665. [Google Scholar] [CrossRef]
- Testori, T.; Weinstein, T.; Taschieri, S.; Wallace, S.S. Risk factors in lateral window sinus elevation surgery. Periodontol. 2000 2019, 81, 91–123. [Google Scholar] [CrossRef] [PubMed]
- Correia, F.; Faria Almeida, R.; Lemos Costa, A.; Carvalho, J.; Felino, A. Levantamento do seio maxilar pela técnica da janela lateral: Tipos enxertos. Rev. Port. de Estomatol. Med. Dentária e Cir. Maxilofac. 2012, 53, 190–196. [Google Scholar] [CrossRef] [Green Version]
- Benic, G.I.; Hammerle, C.H. Horizontal bone augmentation by means of guided bone regeneration. Periodontol. 2000 2014, 66, 13–40. [Google Scholar] [CrossRef]
- Yip, I.; Ma, L.; Mattheos, N.; Dard, M.; Lang, N.P. Defect healing with various bone substitutes. Clin. Oral Implants Res. 2015, 26, 606–614. [Google Scholar] [CrossRef]
- Zizzari, V.L.; Zara, S.; Tete, G.; Vinci, R.; Gherlone, E.; Cataldi, A. Biologic and clinical aspects of integration of different bone substitutes in oral surgery: A literature review. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2016, 122, 392–402. [Google Scholar] [CrossRef]
- Al-Dajani, M. Recent Trends in Sinus Lift Surgery and Their Clinical Implications. Clin. Implant Dent. Relat. Res. 2016, 18, 204–212. [Google Scholar] [CrossRef] [PubMed]
- Danesh-Sani, S.A.; Loomer, P.M.; Wallace, S.S. A comprehensive clinical review of maxillary sinus floor elevation: Anatomy, techniques, biomaterials and complications. Br. J. Oral Maxillofac. Surg. 2016, 54, 724–730. [Google Scholar] [CrossRef] [PubMed]
- Nasr, S.; Slot, D.E.; Bahaa, S.; Dorfer, C.E.; Fawzy El-Sayed, K.M. Dental implants combined with sinus augmentation: What is the merit of bone grafting? A systematic review. J. Cranio Maxillofac. Surg. 2016, 44, 1607–1617. [Google Scholar] [CrossRef]
- Starch-Jensen, T.; Aludden, H.; Hallman, M.; Dahlin, C.; Christensen, A.E.; Mordenfeld, A. A systematic review and meta-analysis of long-term studies (five or more years) assessing maxillary sinus floor augmentation. Int. J. Oral Maxillofac. Surg 2018, 47, 103–116. [Google Scholar] [CrossRef] [PubMed]
- Soardi, C.M.; Suarez-Lopez del Amo, F.; Galindo-Moreno, P.; Catena, A.; Zaffe, D.; Wang, H.L. Reliability of Cone Beam Computed Tomography in Determining Mineralized Tissue in Augmented Sinuses. Int. J. Oral Maxillofac. Implants 2016, 31, 352–358. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Suarez-Lopez Del Amo, F.; Ortega-Oller, I.; Catena, A.; Monje, A.; Khoshkam, V.; Torrecillas-Martinez, L.; Wang, H.L.; Galindo-Moreno, P. Effect of barrier membranes on the outcomes of maxillary sinus floor augmentation: A meta-analysis of histomorphometric outcomes. Int. J. Oral Maxillofac. Implants 2015, 30, 607–618. [Google Scholar] [CrossRef] [Green Version]
- Xavier, S.P.; Santos Tde, S.; Sehn, F.P.; Silva, E.R.; Garcez-Filho Jde, A.; Martins-Filho, P.R. Maxillary sinus grafting with fresh frozen allograft versus bovine bone mineral: A tomographic and histological study. J. Cranio Maxillofac. Surg. 2016, 44, 708–714. [Google Scholar] [CrossRef]
- Iezzi, G.; Piattelli, A.; Giuliani, A.; Mangano, C.; Barone, A.; Manzon, L.; Degidi, M.; Scarano, A.; Filippone, A.; Perrotti, V. Molecular, Cellular and Pharmaceutical Aspects of Bone Grafting Materials and Membranes During Maxillary Sinus-lift Procedures. Part 2: Detailed Characteristics of the Materials. Curr. Pharm. Biotechnol. 2017, 18, 33–44. [Google Scholar] [CrossRef]
- Barone, A.; Ricci, M.; Covani, U.; Nannmark, U.; Azarmehr, I.; Calvo-Guirado, J.L. Maxillary sinus augmentation using prehydrated corticocancellous porcine bone: Hystomorphometric evaluation after 6 months. Clin. Implant Dent. Relat. Res. 2012, 14, 373–379. [Google Scholar] [CrossRef]
- Silvestri, M.; Martegani, P.; D’Avenia, F.; Farneti, M.; Capri, D.; Paolantoni, G.; Landi, L. Simultaneous sinus augmentation with implant placement: Histomorphometric comparison of two different grafting materials. A multicenter double-blind prospective randomized controlled clinical trial. Int. J. Oral Maxillofac. Implants 2013, 28, 543–549. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pagliani, L.; Andersson, P.; Lanza, M.; Nappo, A.; Verrocchi, D.; Volpe, S.; Sennerby, L. A collagenated porcine bone substitute for augmentation at Neoss implant sites: A prospective 1-year multicenter case series study with histology. Clin. Implant Dent. Relat. Res. 2012, 14, 746–758. [Google Scholar] [CrossRef]
- Nannmark, U.; Sennerby, L. The bone tissue responses to prehydrated and collagenated cortico-cancellous porcine bone grafts: A study in rabbit maxillary defects. Clin. Implant Dent. Relat. Res. 2008, 10, 264–270. [Google Scholar] [CrossRef] [PubMed]
- Barone, A.; Ricci, M.; Grassi, R.F.; Nannmark, U.; Quaranta, A.; Covani, U. A 6-month histological analysis on maxillary sinus augmentation with and without use of collagen membranes over the osteotomy window: Randomized clinical trial. Clin. Oral Implants Res. 2013, 24, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Orsini, G.; Scarano, A.; Piattelli, M.; Piccirilli, M.; Caputi, S.; Piattelli, A. Histologic and ultrastructural analysis of regenerated bone in maxillary sinus augmentation using a porcine bone-derived biomaterial. J. Periodontol. 2006, 77, 1984–1990. [Google Scholar] [CrossRef]
- Tete, S.; Zizzari, V.L.; Vinci, R.; Zara, S.; Di Tore, U.; Manica, M.; Cataldi, A.; Mortellaro, C.; Piattelli, A.; Gherlone, E. Equine and porcine bone substitutes in maxillary sinus augmentation: A histological and immunohistochemical analysis of VEGF expression. J. Craniofacial Surg. 2014, 25, 835–839. [Google Scholar] [CrossRef]
- Wolf, M.; Wurm, A.; Heinemann, F.; Gerber, T.; Reichert, C.; Jager, A.; Gotz, W. The Effect of Patient Age on Bone Formation Using a Fully Synthetic Nanocrystalline Bone Augmentation Material in Maxillary Sinus Grafting. Int. J. Oral Maxillofac. Implant. 2014, 29, 976–983. [Google Scholar] [CrossRef] [Green Version]
- Antczak-Bouckoms, A.A.; Tulloch, J.F.; Berkey, C.S. Split-mouth and cross-over designs in dental research. J. Clin. Periodontol. 1990, 17, 446–453. [Google Scholar] [CrossRef]
- Lesaffre, E.; Philstrom, B.; Needleman, I.; Worthington, H. The design and analysis of split-mouth studies: What statisticians and clinicians should know. Stat. Med. 2009, 28, 3470–3482. [Google Scholar] [CrossRef]
- Ramirez-Fernandez, M.P.; Calvo-Guirado, J.L.; Mate-Sanchez Del Val, J.E.; Delgado-Ruiz, R.A.; Negri, B.; Barona-Dorado, C. Ultrastructural study by backscattered electron imaging and elemental microanalysis of bone-to-biomaterial interface and mineral degradation of porcine xenografts used in maxillary sinus floor elevation. Clin. Oral Implants Res. 2013, 24, 523–530. [Google Scholar] [CrossRef] [PubMed]
- Scarano, A.; Piattelli, A.; Assenza, B.; Quaranta, A.; Perrotti, V.; Piattelli, M.; Iezzi, G. Porcine bone used in sinus augmentation procedures: A 5-year retrospective clinical evaluation. J. Oral Maxillofac. Surg. 2010, 68, 1869–1873. [Google Scholar] [CrossRef]
- Younes, F.; Cosyn, J.; De Bruyckere, T.; Cleymaet, R.; Eghbali, A. A 2-year prospective case series on volumetric changes, PROMs, and clinical outcomes following sinus floor elevation using deproteinized bovine bone mineral as filling material. Clin. Implant Dent. Relat. Res. 2019, 21, 301–309. [Google Scholar] [CrossRef]
- Corbella, S.; Taschieri, S.; Weinstein, R.; Del Fabbro, M. Histomorphometric outcomes after lateral sinus floor elevation procedure: A systematic review of the literature and meta-analysis. Clin. Oral Implants Res. 2016, 27, 1106–1122. [Google Scholar] [CrossRef] [PubMed]
- Trimmel, B.; Gede, N.; Hegyi, P.; Szakacs, Z.; Mezey, G.A.; Varga, E.; Kivovics, M.; Hanak, L.; Rumbus, Z.; Szabo, G. Relative performance of various biomaterials used for maxillary sinus augmentation: A Bayesian network meta-analysis. Clin. Oral Implants Res. 2021, 32, 135–153. [Google Scholar] [CrossRef]
- Barone, A.; Crespi, R.; Aldini, N.N.; Fini, M.; Giardino, R.; Covani, U. Maxillary sinus augmentation: Histologic and histomorphometric analysis. Int. J. Oral Maxillofac. Implants 2005, 20, 519–525. [Google Scholar]
- Merli, M.; Moscatelli, M.; Mariotti, G.; Pagliaro, U.; Bernardelli, F.; Nieri, M. A minimally invasive technique for lateral maxillary sinus floor elevation: A Bayesian network study. Clin. Oral Implants Res. 2016, 27, 273–281. [Google Scholar] [CrossRef]
- Danesh-Sani, S.A.; Engebretson, S.P.; Janal, M.N. Histomorphometric results of different grafting materials and effect of healing time on bone maturation after sinus floor augmentation: A systematic review and meta-analysis. J. Periodontal. Res. 2017, 52, 301–312. [Google Scholar] [CrossRef]
- Soardi, C.M.; Clozza, E.; Turco, G.; Biasotto, M.; Engebretson, S.P.; Wang, H.L.; Zaffe, D. Microradiography and microcomputed tomography comparative analysis in human bone cores harvested after maxillary sinus augmentation: A pilot study. Clin. Oral Implants Res. 2014, 25, 1161–1168. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Reich, K.M.; Huber, C.D.; Heimel, P.; Ulm, C.; Redl, H.; Tangl, S. A quantification of regenerated bone tissue in human sinus biopsies: Influences of anatomical region, age and sex. Clin. Oral Implants Res. 2016, 27, 583–590. [Google Scholar] [CrossRef] [PubMed]
- Froum, S.J.; Khouly, I.; Favero, G.; Cho, S.C. Effect of maxillary sinus membrane perforation on vital bone formation and implant survival: A retrospective study. J. Periodontol. 2013, 84, 1094–1099. [Google Scholar] [CrossRef] [PubMed]
- Kolerman, R.; Nissan, J.; Rahmanov, M.; Vered, H.; Cohen, O.; Tal, H. Comparison between mineralized cancellous bone allograft and an alloplast material for sinus augmentation: A split mouth histomorphometric study. Clin. Implant Dent. Relat. Res. 2017, 19, 812–820. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Hard Tissue Levels (mm) | ||||||||
|---|---|---|---|---|---|---|---|---|
| ID | Gender | Age | ABG | Xenograft | ||||
| Baseline Bone Height (Mean) | Mean 6 Months | Diferences mm (6 Months—Baseline) | Baseline Bone Height (Mean) | Mean 6 Months | Diferences mm (6 Months—Baseline) | |||
| 1 | F | 63.74 | 2.10 | 11.30 | 9.2 | 4.80 | 10.15 | 5.4 |
| 2 | F | 42.23 | 2.60 | 11.05 | 8.5 | 2.85 | 12.00 | 9.2 |
| 3 | M | 58.66 | 3.15 | 6.80 | 3.7 | 2.55 | 9.65 | 7.1 |
| 4 | M | 63.70 | 4.70 | 10.15 | 5.5 | 2.85 | 11.55 | 8.7 |
| 5 | F | 67.83 | 3.30 | 9.90 | 6.6 | 3.60 | 10.40 | 6.8 |
| 6 | M | 75.04 | 1.30 | 8.83 | 7.5 | 1.20 | 9.83 | 8.6 |
| 7 | M | 59.56 | 4.10 | 16.56 | 12.5 | 3.91 | 15.11 | 11.2 |
| 8 | M | 54.14 | 2.59 | 11.98 | 9.4 | 1.54 | 12.40 | 10.9 |
| 9 | M | 65.54 | 3.43 | 9.86 | 6.4 | 2.50 | 15.00 | 12.5 |
| 10 | F | 61.05 | 3.67 | 13.13 | 9.5 | 4.90 | 12.44 | 7.5 |
| 11 | F | 55.48 | 3.88 | 9.87 | 6.0 | 2.67 | 9.21 | 6.5 |
| 12 | F | 49.49 | 3.50 | 12.63 | 9.1 | 3.30 | 13.40 | 10.1 |
| Total | M-6 F-6 | 59.70 | 3.20 ± 0.93 | 11.02 ± 2.45 | 7.81 ± 2.34 | 3.06 ± 1.13 | 11.76 ± 2.01 | 8.71 ± 2.15 |
| ID | Total Hard Tissue Volume (THT%) | Total Soft Tissue (TST%) | ||||||
|---|---|---|---|---|---|---|---|---|
| Autologous | Xenograft | Autologous | Xenograft | |||||
| Mean | SD | Mean | SD | Mean | SD | Mean | SD | |
| 1 | 49.67 | 5.33 | 44.19 | 1.08 | 50.33 | 5.33 | 55.81 | 1.08 |
| 2 | 59.15 | 7.03 | 57.60 | 5.94 | 40.85 | 7.03 | 42.40 | 5.94 |
| 3 | 60.09 | 2.90 | 64.15 | 5.51 | 39.91 | 2.90 | 35.85 | 5.51 |
| 4 | 64.07 | 2.79 | 51.00 | 5.36 | 35.93 | 2.79 | 49.00 | 5.36 |
| 5 | 52.35 | 1.52 | 57.65 | 2.14 | 47.65 | 1.52 | 42.35 | 2.14 |
| 6 | 63.26 | 2.35 | 64.19 | 2.07 | 36.74 | 2.35 | 35.81 | 2.07 |
| 7 | 59.39 | 3.27 | 59.39 | 2.41 | 40.61 | 3.27 | 40.61 | 2.41 |
| 8 | 58.16 | 1.99 | 55.72 | 2.40 | 41.84 | 1.99 | 44.28 | 2.40 |
| 9 | 52.31 | 1.91 | 54.96 | 1.94 | 47.69 | 1.91 | 45.04 | 1.94 |
| 10 | 55.42 | 2.22 | 55.15 | 2.33 | 44.58 | 2.22 | 44.85 | 2.33 |
| 11 | 60.55 | 2.37 | 56.12 | 1.75 | 39.45 | 2.37 | 43.88 | 1.75 |
| 12 | 53.29 | 1.29 | 51.98 | 1.33 | 46.71 | 1.29 | 48.02 | 1.33 |
| mean | 57.31 | 2.91 | 56.01 | 2.86 | 42.69 | 2.91 | 43.99 | 2.86 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Correia, F.; Pozza, D.H.; Gouveia, S.; Felino, A.C.; Faria-Almeida, R. Advantages of Porcine Xenograft over Autograft in Sinus Lift: A Randomised Clinical Trial. Materials 2021, 14, 3439. https://doi.org/10.3390/ma14123439
Correia F, Pozza DH, Gouveia S, Felino AC, Faria-Almeida R. Advantages of Porcine Xenograft over Autograft in Sinus Lift: A Randomised Clinical Trial. Materials. 2021; 14(12):3439. https://doi.org/10.3390/ma14123439
Chicago/Turabian StyleCorreia, Francisco, Daniel Humberto Pozza, Sónia Gouveia, António Campos Felino, and Ricardo Faria-Almeida. 2021. "Advantages of Porcine Xenograft over Autograft in Sinus Lift: A Randomised Clinical Trial" Materials 14, no. 12: 3439. https://doi.org/10.3390/ma14123439