
Medical Waste Treatment Technologies for Energy, Fuels, and Materials Production: A Review



Abstract
:1. Introduction
2. Medical Waste Generation and Classification
2.1. Medical Waste Generation
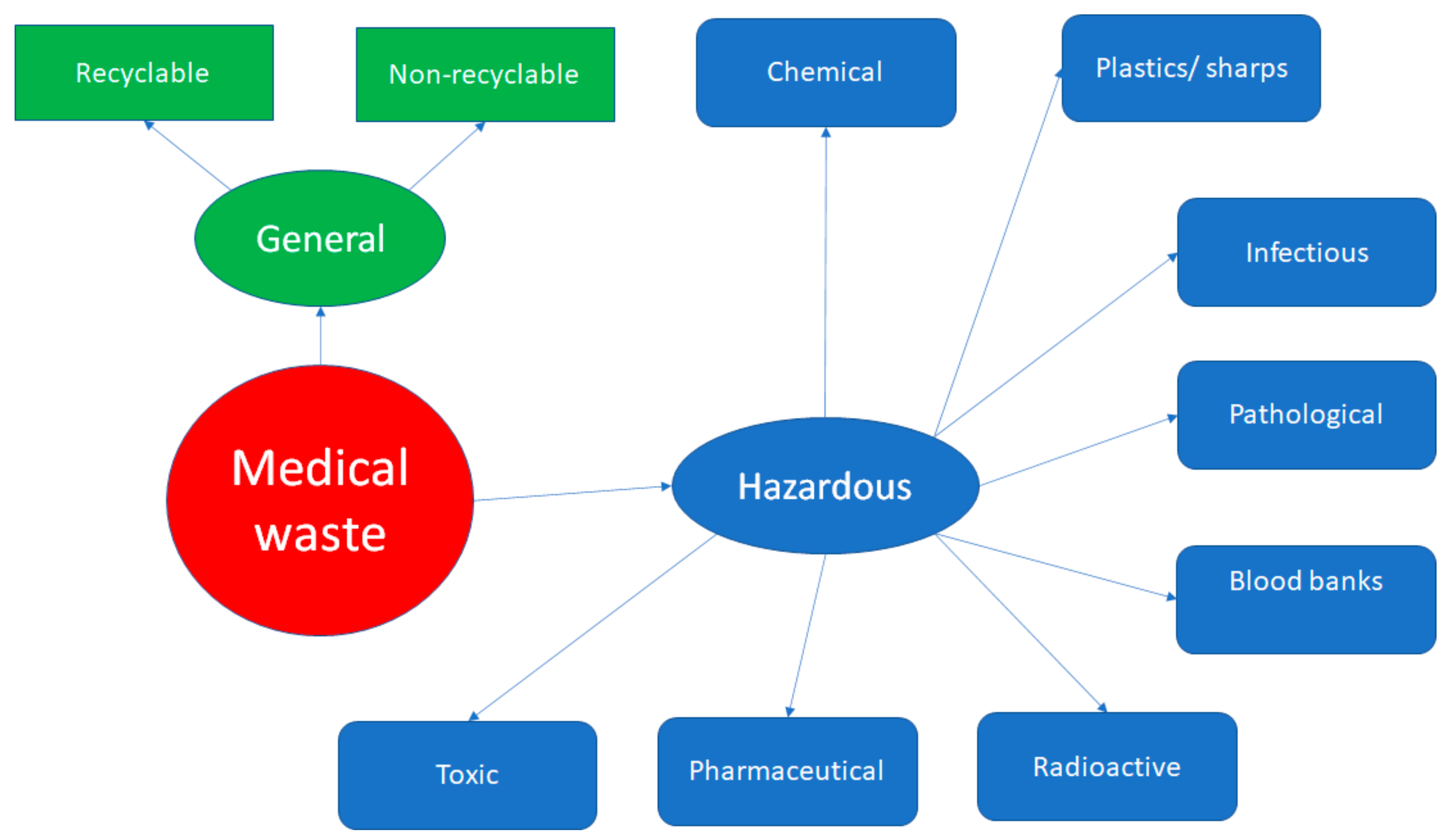
2.2. Medical Waste Classification
3. Medical Waste Treatment Technologies
3.1. Medical Waste Handling
3.2. Medical Waste Collection, Separation and Transportation
3.3. Treatment and Disposal Technologies for Medical Waste
3.4. Sanitary Landfill Technology
3.5. High Temperature Incineration Technology
3.6. High Temperature Pyrolysis Technology
3.7. Medium Temperature Microwave Technology
3.8. Pressure Steam Sterilization Technology
3.9. Chemical Disinfection Technology
3.10. Plasma Technology
3.11. Torrefaction Technology
3.12. Acid and Enzymatic Hydrolysis Technology
4. Energy, Fuels and Materials Produced by Medical Waste Treatment
5. Optimization Process Limitations, Economic Feasibility, and Recommendations for Future Research
5.1. Optimization Process Limitations and Economic Feasibility
5.2. Recommendations for Future Research
- More work can be conducted as regards the optimization of the MW collection and transportation processes, in combination with the location/allocation of MWT facilities installation problem.
- The categorization and separation of MW can be significantly improved, while the segregation of MW at the location where it is generated (hospitals, healthcare facilities, etc.) can substantially enhance the economic feasibility of the following steps as regards the MWTTs applied for energy, fuels, and materials production.
- The thermal energy produced during MWT via incineration and similar technologies can be utilized more efficiently by innovative recycling and recovering techniques while the environmental impact via thermal pollution will be eliminated.
- The determination of the HHV values and the physical/chemical properties of the specific MW fractions will facilitate the processes optimization and the costs minimization.
- MWTTs data from pilot and full-scale MWT facilities can be collected to improve the accuracy and universality of the processes optimization results and the economic feasibility of the proposed applications.
- Further research is needed on the application of the MW plastic or lignocellulosic fraction (cotton, paper/cardboard, textiles) conversion technologies, focusing on the fuels/materials production.
- Finally, more work can be conducted on the co-processing of the MW plastic or lignocellulosic fraction (cotton/paper/cardboard/textiles) with similar fractions coming from municipal/industrial solid waste (plastics or cotton/paper/cardboard/textiles/wood) or agricultural (straw/wood/husks/chaff/cobs/bagasse can) and forest (wood/bark/leaves/stems/roots) lignocellulosic biomass, aiming at value added fuels/materials production technologies with low-cost (see Figure 4).
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Das, A.K.; Islam, M.; Billah, M.; Sarker, A. COVID-19 pandemic and healthcare solid waste management strategy–A mini-review. Sci. Total Environ. 2021, 778, 146220. [Google Scholar] [CrossRef] [PubMed]
- Barua, U.; Hossain, D. A review of the medical waste management system at Covid-19 situation in Bangladesh. J. Mater. Cycles Waste Manag. 2021, 23, 2087–2100. [Google Scholar] [CrossRef]
- Alrawi, A.S.; Amin, S.A.; Al-Ani, R.R. Medical waste management during COVID-19 pandemic, a review study. IOP Conf. Ser. Earth Environ. Sci. 2021, 779, 012130. [Google Scholar] [CrossRef]
- Fadaei, A. Study of solid waste (municipal and medical) management during the COVID-19 pandemic: A review study. Rev. Environ. Health 2021. [Google Scholar] [CrossRef]
- Kenny, C.; Priyadarshini, A. Review of Current Healthcare Waste Management Methods and Their Effect on Global Health. Healthcare 2021, 9, 284. [Google Scholar] [CrossRef]
- Khan, B.A.; Cheng, L.; Khan, A.A.; Ahmed, H. Healthcare waste management in Asian developing countries: A mini review. Waste Manag. Res. 2019, 37, 863–875. [Google Scholar] [CrossRef] [Green Version]
- Antoniadou, M.; Varzakas, T.; Tzoutzas, I. Circular Economy in Conjunction with Treatment Methodologies in the Biomedical and Dental Waste Sectors. Circ. Econ. Sustain. 2021, 1, 563–592. [Google Scholar] [CrossRef]
- Singh, N.; Ogunseitan, O.A.; Tang, Y. Medical waste: Current challenges and future opportunities for sustainable management. Crit. Rev. Environ. Sci. Technol. 2021, 1–23. [Google Scholar] [CrossRef]
- Capoor, M.R.; Parida, A. Biomedical Waste and Solid Waste Management in the Time of COVID-19: A Comprehensive Review of the National and International Scenario and Guidelines. J. Lab. Phys. 2021, 13, 175–182. [Google Scholar] [CrossRef]
- Chisholm, J.M.; Zamani, R.; Negm, A.M.; Said, N.; Abdel Daiem, M.M.; Dibaj, M.; Akrami, M. Sustainable waste management of medical waste in African developing countries: A narrative review. Waste Manag. Res. 2021, 39, 1149–1163. [Google Scholar] [CrossRef]
- El-Ramady, H.; Brevik, E.C.; Elbasiouny, H.; Elbehiry, F.; Amer, M.; Elsakhawy, T.; Omara, A.E.-D.; Mosa, A.A.; El-Ghamry, A.M.; Abdalla, N.; et al. Planning for disposal of COVID-19 pandemic wastes in developing countries: A review of current challenges. Environ. Monit. Assess. 2021, 193, 592. [Google Scholar] [CrossRef]
- Tirkolaee, E.B.; Aydın, N.S. A sustainable medical waste collection and transportation model for pandemics. Waste Manag. Res. 2021, 39, 34–44. [Google Scholar] [CrossRef]
- Lotfi, R.; Kargar, B.; Gharehbaghi, A.; Weber, G.-W. Viable medical waste chain network design by considering risk and robustness. Environ. Sci. Pollut. Res. 2021, 1–16. [Google Scholar] [CrossRef]
- He, X.; Quan, H.; Lin, W.; Deng, W.; Tan, Z. AGV Scheduling Optimization for Medical Waste Sorting System. Sci. Program. 2021, 2021, 4313749. [Google Scholar] [CrossRef]
- Song, Y.; Ye, J.; Liu, Y.; Zhong, Y. Estimation of Solid Medical Waste Production and Environmental Impact Analysis in the Context of COVID-19: A Case Study of Hubei Province in China. Preprints 2021, 2021040327. [Google Scholar] [CrossRef]
- Kalantary, R.R.; Jamshidi, A.; Mofrad, M.M.G.; Jafari, A.J.; Heidari, N.; Fallahizadeh, S.; Arani, M.H.; Torkashvand, J. Effect of COVID-19 pandemic on medical waste management: A case study. J. Environ. Health Sci. Eng. 2021, 19, 831–836. [Google Scholar] [CrossRef]
- Maalouf, A.; Maalouf, H. Impact of COVID-19 pandemic on medical waste management in Lebanon. Waste Manag. Res. 2021, 39, 45–55. [Google Scholar] [CrossRef]
- Mekonnen, B.; Solomon, N.; Wndimu, W. Healthcare Waste Status and Handling Practices during COVID-19 Pandemic in Tepi General Hospital, Ethiopia. J. Environ. Public Health 2021, 2021, 6614565. [Google Scholar] [CrossRef]
- Khalid, S.; Haq, N.; Sabiha, Z.-U.; Latif, A.; Khan, M.A.; Iqbal, J.; Yousaf, N. Current practices of waste management in teaching hospitals and presence of incinerators in densely populated areas. BMC Public Health 2021, 21, 1340. [Google Scholar] [CrossRef]
- Nguyen, T.D.; Kawai, K.; Nakakubo, T. Estimation of COVID-19 waste generation and composition in Vietnam for pandemic management. Waste Manag. Res. 2021, 39, 1356–1364. [Google Scholar] [CrossRef]
- Tsai, W.T. Analysis of medical waste management and impact analysis of COVID-19 on its generation in Taiwan. Waste Manag. Res. 2021, 39, 27–33. [Google Scholar] [CrossRef] [PubMed]
- Anicetus, H.; Saria, J.; Mohamed, H. Estimation of Different Categories of Healthcare Waste Generated at Two Different Hospital Categories in Four Hospitals in Dar es Salaam City. J. Environ. Prot. 2020, 11, 872–888. [Google Scholar] [CrossRef]
- Borowy, I. Medical waste: The dark side of healthcare. Hist. Cienc. Saude-Manguinhos 2020, 27, 231–251. [Google Scholar] [CrossRef] [PubMed]
- Meleko, A.; Tesfaye, T.; Henok, A. Assessment of Healthcare Waste Generation Rate and Its Management System in Health Centers of Bench Maji Zone. Ethiop. J. Health Sci. 2018, 28, 125–134. [Google Scholar] [CrossRef] [PubMed]
- Minoglou, M.; Gerassimidou, S.; Komilis, D. Healthcare Waste Generation Worldwide and Its Dependence on Socio-Economic and Environmental Factors. Sustainability 2017, 9, 220. [Google Scholar] [CrossRef] [Green Version]
- Maamari, O.; Brandam, C.; Lteif, R.; Salameh, D. Health Care Waste generation rates and patterns: The case of Lebanon. Waste Manag. 2015, 43, 550–554. [Google Scholar] [CrossRef] [Green Version]
- Debere, M.K.; Gelaye, K.A.; Alamdo, A.G.; Trifa, Z.M. Assessment of the health care waste generation rates and its management system in hospitals of Addis Ababa, Ethiopia, 2011. BMC Public Health 2013, 13, 28. [Google Scholar] [CrossRef] [Green Version]
- Komilis, D.P.; Voudrias, E.A.; Anthoulakis, S.; Iosifidis, N. Composition and production rate of solid waste from dental laboratories in Xanthi, Greece. Waste Manag. 2009, 29, 1208–1212. [Google Scholar] [CrossRef]
- Komilis, D.; Katsafaros, N.; Vassilopoulos, P. Hazardous medical waste generation in Greece: Case studies from medical facilities in Attica and from a small insular hospital. Waste Manag. Res. 2011, 29, 807–814. [Google Scholar] [CrossRef]
- Komilis, D.; Fouki, A.; Papadopoulos, D. Hazardous medical waste generation rates of different categories of health-care facilities. Waste Manag. 2012, 32, 1434–1441. [Google Scholar] [CrossRef]
- Hamoda, H.M.; El-Tomi, H.N.; Bahman, Q.Y. Variations in Hospital Waste Quantities and Generation Rates. J. Environ. Sci. Health Part A 2005, 40, 467–476. [Google Scholar] [CrossRef]
- Altin, S.; Altin, A.; Elevli, B.; Cerit, O. Determination of Hospital Waste Composition and Disposal Methods: A Case Study. Pol. J. Environ. Stud. 2003, 12, 251–255. [Google Scholar]
- Tudor, T.L.; Marsh, C.L.; Butler, S.; Van Horn, J.A.; Jenkin, L.E.T. Realising resource efficiency in the management of healthcare waste from the Cornwall National Health Service (NHS) in the UK. Waste Manag. 2008, 28, 1209–1218. [Google Scholar] [CrossRef]
- De Delmonico, D.V.G.; dos Santos, H.H.; Pinheiro, M.A.; de Castro, R.; de Souza, R.M. Waste management barriers in developing country hospitals: Case study and AHP analysis. Waste Manag. Res. 2017, 36, 48–58. [Google Scholar] [CrossRef] [Green Version]
- Hossain, S.; Santhanam, A.; Nik Norulaini, N.A.; Mohd Omar, M.K. Clinical solid waste management practices and its impact on human health and environment—A review. Waste Manag. 2011, 31, 754–766. [Google Scholar] [CrossRef]
- Tesfahun, E.; Kumie, A.; Beyene, A. Developing models for the prediction of hospital healthcare waste generation rate. Waste Manag. Res. 2015, 34, 219–220. [Google Scholar] [CrossRef]
- Ansari, M.; Ehrampoush, M.H.; Farzadkia, M.; Ahmadi, E. Dynamic assessment of economic and environmental performance index and generation composition, environmental and human health risks of hospital solid waste in developing countries; A state of the art of review. Environ. Int. 2019, 132, 105073. [Google Scholar] [CrossRef]
- Farzadkia, M.; Emamjomeh, M.M.; Golbaz, S.; Sajadi, H.S. An investigation in hospital solid waste management in Iran. Glob. NEST J. 2015, 17, 771–783. [Google Scholar]
- Sanida, G.; Karagiannidis, A.; Mavidou, F.; Vartzopoulos, D.; Moussiopoulos, N.; Chatzopoulos, S. Assessing generated quantities of infectious medical wastes: A case study for a health region administration in Central Macedonia, Greece. Waste Manag. 2010, 30, 532–538. [Google Scholar] [CrossRef]
- Zamparas, M.; Kalavrouziotis, I.K. Healthcare waste management in Greece. The example of Health Region of Western Greece, Peloponnese, Epirus and Ionian Islands. Glob. NEST J. 2017, 20, 96–102. [Google Scholar] [CrossRef] [Green Version]
- Zamparas, M.; Kapsalis, V.C.; Kyriakopoulos, G.L.; Aravossis, K.G.; Kanteraki, A.E.; Vantarakis, A.; Kalavrouziotis, I.K. Medical waste management and environmental assessment in the Rio University Hospital, Western Greece. Sustain. Chem. Pharm. 2019, 13, 100163. [Google Scholar] [CrossRef]
- Munir, S.; Batool, S.A.; Chaudhry, M.N. Characterization of hospital waste in Lahore, Pakistan. Chin. Med. J. 2014, 127, 1732–1736. [Google Scholar]
- Taghipour, H.; Mosaferi, M. Characterization of medical waste from hospitals in Tabriz, Iran. Sci. Total Environ. 2009, 407, 1527–1595. [Google Scholar] [CrossRef] [PubMed]
- Gusca, J.; Kalnins, S.N.; Blumberga, D.; Bozhko, L.; Khabdullina, Z.; Khabdullin, A. Assessment Method of Health Care Waste Generation in Latvia and Kazakhstan. Energy Procedia 2015, 72, 175–179. [Google Scholar] [CrossRef] [Green Version]
- United States Environmental Protection Agency (EPA). Medical Waste. Available online: https://www.epa.gov/rcra/medical-waste (accessed on 28 October 2021).
- Sawalem, M.; Selic, E.; Herbell, J.-D. Hospital waste management in Libya: A case study. Waste Manag. 2009, 29, 1370–1375. [Google Scholar] [CrossRef]
- Imdad, S.; Anwar, S.; Shoukat, M.S. Healthcare waste: Evaluation of its generation rate and management practices in tertiary care hospitals of Lahore. Ann. King Edw. Med. Univ. 2013, 19, 274–281. [Google Scholar] [CrossRef]
- Ali, S.; Mahmood, U.; Malik, A.U.; Aziz, F.; Naghman, R.B.; Ahmed, I. Current hospital waste management practices in Pakistan: Case study and curative measures. J. Prev. Med. 2015, 1, 125–129. [Google Scholar]
- Al-Khatib, I.A.; Khalaf, A.-S.; Al-Sari, M.I.; Anayah, F. Medical waste management at three hospitals in Jenin district, Palestine. Environ. Monit. Assess. 2019, 192, 10. [Google Scholar] [CrossRef]
- Windfeld, E.A.; Brooks, S.L.M. Medical waste management—A review. J. Environ. Manag. 2015, 163, 98–108. [Google Scholar] [CrossRef]
- Nguyen, D.L.; Bui, X.T.; Nguyen, T.H. Estimation of Current and Future Generation of Medical Solid Wastes in Hanoi City, Vietnam. Int. J. Waste Resour. 2014, 4, 1–5. [Google Scholar] [CrossRef] [Green Version]
- Alwabr, G.M.A.; Al-Mikhlafi, A.S.; Al-Hakimi, S.A.; Dughish, M.A. Determination of medical waste composition in hospitals of Sana’a city, Yemen. J. Appl. Sci. Environ. 2016, 20, 343–347. [Google Scholar] [CrossRef]
- World Health Organization (WHO). Health-Care Waste. Available online: https://www.who.int/news-room/fact-sheets/detail/health-care-waste (accessed on 28 October 2021).
- Korkut, E.N. Estimations and analysis of medical waste amounts in the city of Istanbul and proposing a new approach for the estimation of future medical waste amounts. Waste Manag. 2018, 81, 168–176. [Google Scholar] [CrossRef]
- Eker, H.H.; Bilgili, M.S. Statistical analysis of waste generation in healthcare services: A case study. Waste Manag. Res. 2011, 29, 791–796. [Google Scholar] [CrossRef]
- Johannessen, L.M. Management of health care waste. In Proceedings of the Environment ’97 Conference, Cairo, Egypt, 16–18 February 1997. [Google Scholar]
- Kagonji, I.S.; Manyele, S.V. Analysis of the Measured Medical Waste Generation at Amana and Ligula Hospitals Using Statistical Methods. Afr. J. Environ. Sci. Technol. 2011, 5, 815–833. [Google Scholar]
- Reinhardt, P.A.; Gordon, J.G. Infectious and Medical Waste Management, 1st ed.; CRC Press: Boca Raton, FL, USA, 1991. [Google Scholar] [CrossRef]
- Thakur, V.; Anbanandam, R. Healthcare waste management: An interpretive structural modeling approach. Int. J. Health Care Qual. Assur. 2016, 29, 559–581. [Google Scholar] [CrossRef]
- Liberti, L.; Tursi, A.; Costantino, N.; Ferrara, L.; Nuzzo, G. Optimization of Infectious Hospital Waste Management in Italy: Part II. Waste Characterization by Origin. Waste Manag. Res. 1996, 14, 417–431. [Google Scholar] [CrossRef]
- Alagöz, B.A.Z.; Kocasoy, G. Treatment and disposal alternatives for health-care waste in developing countries—A case study in Istanbul, Turkey. Waste Manag. Res. 2007, 25, 83–89. [Google Scholar] [CrossRef]
- Capoor, M.R.; Bhowmik, K.T. Current perspectives on biomedical waste management: Rules, conventions and treatment technologies. Indian J. Med. Microbiol. 2017, 35, 157–164. [Google Scholar] [CrossRef]
- Chen, F.; Lou, J.; Hu, J.; Chen, H.; Long, R.; Li, W. Study on the relationship between crisis awareness and medical waste separation behavior shown by residents during the COVID-19 epidemic. Sci. Total Environ. 2021, 787, 147522. [Google Scholar] [CrossRef]
- Chen, Y.; Ding, Q.; Yang, X.; Peng, Z.; Xu, D.; Feng, Q. Application countermeasures of non-incineration technologies for medical waste treatment in China. Waste Manag. Res. 2013, 31, 1237–1244. [Google Scholar] [CrossRef]
- Nwachukwu, N.C.; Anayo, F.; Ugbogu, O.C. Health Care Waste Management–Public Health Benefits, and the Need for Effective Environmental Regulatory Surveillance in Federal Republic of Nigeria. Open access peer-reviewed chapter. Curr. Top. Public Health 2013, 2, 149–178. [Google Scholar] [CrossRef] [Green Version]
- Graikos, A.; Voudrias, E.; Papazachariou, A.; Iosifidis, N.; Kalpakidou, M. Composition and production rate of medical waste from a small producer in Greece. Waste Manag. 2010, 30, 1683–1689. [Google Scholar] [CrossRef] [PubMed]
- Hama, A.R.; Tahir, T.A.; Ali, B.J. A study on solid waste generation, composition and management in Sulaimania city, Kurdistan region, Iraq. IOP Conf. Ser. Earth Environ. Sci. 2021, 779, 012049. [Google Scholar] [CrossRef]
- Hasan, M.M.; Rahman, M.H. Assessment of Healthcare Waste Management Paradigms and Its Suitable Treatment Alternative: A Case Study. J. Environ. Public Health 2018, 2018, 6879751. [Google Scholar] [CrossRef] [Green Version]
- Hong, J.; Zhan, S.; Yu, Z.; Hong, J.; Qi, C. Life-cycle environmental and economic assessment of medical waste treatment. J. Clean. Prod. 2018, 174, 65–73. [Google Scholar] [CrossRef]
- Insa, E.; Zamorano, M.; Lopez, R. Critical review of medical waste legislation in Spain. Resour. Conserv. Recycl. 2010, 54, 1048–1059. [Google Scholar] [CrossRef]
- Jang, Y.C. Infectious/Medical/Hospital Waste: General Characteristics. In Encyclopedia of Environmental Health; Nriagu, J.O., Kacew, S., Kawamoto, T., Eds.; Elsevier: Amsterdam, The Netherland, 2011; pp. 227–231. [Google Scholar] [CrossRef]
- Jang, Y.-C.; Lee, C.; Yoon, O.-S.; Kim, H. Medical waste management in Korea. J. Environ. Manag. 2006, 80, 107–115. [Google Scholar] [CrossRef]
- Khadem Ghasemi, M.; Mohd Yusuff, R. Advantages and Disadvantages of Healthcare Waste Treatment and Disposal Alternatives: Malaysian Scenario. Pol. J. Environ. Stud. 2016, 25, 17–25. [Google Scholar] [CrossRef]
- Kwikiriza, S.; Stewart, A.G.; Mutahunga, B.; Dobson, A.E.; Wilkinson, E. A Whole Systems Approach to Hospital Waste Management in Rural Uganda. Front. Public Health 2019, 7, 136. [Google Scholar] [CrossRef]
- Lee, B.-K.; Ellenbecker, M.J.; Moure-Ersaso, R. Alternatives for treatment and disposal cost reduction of regulated medical waste. Waste Manag. 2004, 24, 143–151. [Google Scholar] [CrossRef]
- Li, C.; Jenq, F. Physical and Chemical Composition of Hospital Waste. Infect. Control Hosp. Epidemiol. 1993, 14, 145–150. [Google Scholar] [CrossRef]
- Mathure, P.; Pathan, S.; Shobhawat, A.S. Need of biomedical waste management system in hospitals–an emerging issue–a review. Curr. World Environ. 2016, 7, 117–124. [Google Scholar] [CrossRef] [Green Version]
- Mentzelou, P.; Vosniakos, F.; Dardavesis, T.; Papadakis, N.; Nikolaou, K.; Athansiadou, C. An information system for hospital waste management. J. Environ. Prot. Ecol. 2009, 10, 285–294. [Google Scholar]
- Prem Ananth, A.; Prashanthini, V.; Visvanathan, C. Healthcare waste management in Asia. Waste Manag. 2010, 30, 154–161. [Google Scholar] [CrossRef]
- Saxena, P.; Pradhan, I.P.; Kumar, D. Redefining bio medical waste management during COVID-19 in India: A way forward. Mater. Today Proc. 2021. [Google Scholar] [CrossRef]
- Phinney, S. ‘Greening’ Work in Canada—Adapting Canadian Work and Workplaces (ACW) and Canadian Labour Congress (CLC). Available online: https://www.academia.edu/38361995/Greening_Work_in_Canada_Adapting_Canadian_Work_and_Workplaces_ACW_and_Canadian_Labour_Congress_CLC (accessed on 15 November 2021).
- Zhao, W.; van der Voet, E.; Huppes, G. Comparative life cycle assessments of incineration and non-incineration treatments for medical waste. Int. J. Life Cycle Assess. 2008, 14, 114–121. [Google Scholar] [CrossRef]
- Abd El-Salam, M.M. Hospital waste management in El-Beheira Governorate, Egypt. J. Environ. Manag. 2010, 91, 618–629. [Google Scholar] [CrossRef]
- Mandal, S.K.; Dutta, J. Integrated Bio-Medical Waste Management Plan for Patna City; Institute of Town Planners: New Delhi, India, 2009; Available online: http://www.itpi.org.in/pdfs/apr1_09.pdf (accessed on 31 October 2021).
- Dehghani, M.H.; Azam, K.; Changani, F.; Fard, E.D. Assessment of medical waste management in educational hospitals of tehran university medical sciences. Iran. J. Environ. Health Sci. Eng. 2008, 5, 131–136. [Google Scholar]
- Rabeie, O.L.; Miranzadeh, M.B.; Fallah, S.H.; Dehqan, S.; Moulana, Z.; Amouei, A.; Mohammadi, A.A.; Ali Asgharnia, H.; Babaie, M. Determination of Hospital Waste Composition and Management in Amol City, Iran. Health Scope 2012, 1, 127–131. [Google Scholar] [CrossRef]
- Bazrafshan, E.; Kord Mostafapoor, F. Survey of medical waste characterization and management in Iran: A case study of Sistan and Baluchestan Province. Waste Manag. Res. 2010, 29, 442–450. [Google Scholar] [CrossRef]
- Wajs, J.; Bochniak, R.; Golabek, A. Proposal of a Mobile Medical Waste Incinerator with Application of Automatic Waste Feeder and Heat Recovery System as a Novelty in Poland. Sustainability 2019, 11, 4980. [Google Scholar] [CrossRef] [Green Version]
- Abdulla, F.; Abu Qdais, H.; Rabi, A. Site investigation on medical waste management practices in northern Jordan. Waste Manag. 2008, 28, 450–458. [Google Scholar] [CrossRef] [PubMed]
- Mohee, R. Medical wastes characterisation in healthcare institutions in Mauritius. Waste Manag. 2005, 25, 575–581. [Google Scholar] [CrossRef] [PubMed]
- Sustainability. Roadmap for Hospitals. A Guide to Achieve Your Sustainability Goals. Available online: http://www.sustainabilityroadmap.org/topics/waste.shtml#.YZIgF07P1PY (accessed on 15 November 2021).
- Liu, P.; Rani, P.; Mishra, A.R. A novel Pythagorean fuzzy combined compromise solution framework for the assessment of medical waste treatment technology. J. Clean. Prod. 2021, 292, 126047. [Google Scholar] [CrossRef]
- Zhao, H.-L.; Wang, L.; Liu, F.; Liu, H.Q.; Zhang, N.; Zhu, Y.W. Energy, environment and economy assessment of medical waste disposal technologies in China. Sci. Total Environ. 2021, 796, 148964. [Google Scholar] [CrossRef]
- Bucătaru, C.; Săvescu, D.; Repanovici, A.; Blaga, L.; Coman, E.; Cocuz, M.-E. The Implications and Effects of Medical Waste on Development of Sustainable Society—A Brief Review of the Literature. Sustainability 2021, 13, 3300. [Google Scholar] [CrossRef]
- Letho, Z.; Yangdon, T.; Lhamo, C.; Limbu, C.B.; Yoezer, S.; Jamtsho, T.; Chhetri, P.; Tshering, D. Awareness and practice of medical waste management among healthcare providers in National Referral Hospital. PLoS ONE 2021, 16, e0243817. [Google Scholar] [CrossRef]
- Ndejjo, R.; Musinguzi, G.; Yu, X.; Buregyeya, E.; Musoke, D.; Wang, J.-S.; Halage, A.A.; Whalen, C.; Bazeyo, W.; Williams, P.; et al. Occupational Health Hazards among Healthcare Workers in Kampala, Uganda. J. Environ. Public Health 2015, 2015, 913741. [Google Scholar] [CrossRef] [Green Version]
- Uddin, M.N.; Islam, M.R.; Yesmin, K. Knowledge on Hospital Waste Management among Senior Staff Nurses Working in a Selected Medical College Hospital of Bangladesh. J. Waste Manag. 2014, 2014, 73069. [Google Scholar] [CrossRef] [Green Version]
- Govindan, K.; Nasr, A.K.; Mostafazadeh, P.; Mina, H. Medical waste management during coronavirus disease 2019 (COVID-19) outbreak: A mathematical programming model. Comput. Ind. Eng. 2021, 162, 107668. [Google Scholar] [CrossRef]
- Mühlich, M.; Scherrer, M.; Daschner, F.D. Comparison of infectious waste management in European hospitals. J. Hosp. Infect. 2003, 55, 260–268. [Google Scholar] [CrossRef]
- Almuneef, M. Effective medical waste management: It can be done. Am. J. Infect. Control 2003, 31, 188–192. [Google Scholar] [CrossRef]
- Garcia, R. Effective cost-reduction strategies in the management of regulated medical waste. Am. J. Infect. Control 1999, 27, 165–175. [Google Scholar] [CrossRef]
- Blenkharn, J.I. Safe disposal and effective destruction of clinical wastes. J. Hosp. Infect. 2005, 60, 295–297. [Google Scholar] [CrossRef]
- Tata, A.; Beone, F. Hospital waste sterilization: A technical and economic comparison between radiation and microwaves treatments. Radiat. Phys. Chem. 1995, 46, 1153–1157. [Google Scholar] [CrossRef]
- Brichard, K. Out of sight, out of mind…the medical waste problem. Lancet 2002, 359, 56. [Google Scholar] [CrossRef]
- Solberg, K.E. Trade in medical waste causes deaths in India. Lancet 2009, 373, 1067. [Google Scholar] [CrossRef]
- Hantoko, D.; Li, X.; Pariatamby, A.; Yoshikawa, K.; Horttanainen, M.; Yan, M. Challenges and practices on waste management and disposal during COVID-19 pandemic. J. Environ. Manag. 2021, 286, 112140. [Google Scholar] [CrossRef]
- World Health Organization (WHO). Water, Sanitation, Hygiene, and Waste Management for the COVID-19 Virus: Interim Guidance. 2020. Available online: https://apps.who.int/iris/handle/10665/331499 (accessed on 29 October 2021).
- Rutala, W.A.; Mayhall, G. Medical waste. Infect. Control Hosp. Epidemiol. 1992, 13, 38–48. [Google Scholar] [CrossRef]
- Ozbay, G.; Jones, M.; Gadde, M.; Isah, S.; Attarwala, T. Design and Operation of Effective Landfills with Minimal Effects on the Environment and Human Health. J. Environ. Public Health 2021, 2021, 6921607. [Google Scholar] [CrossRef]
- Hereher, M.E.; Al-Awadhi, T.; Mansour, S.A. Assessment of the optimized sanitary landfill sites in Muscat, Oman. Egypt. J. Remote Sens. 2020, 23, 355–362. [Google Scholar] [CrossRef]
- Nik Ab Rahim, N.N.; Othman, J.; Hanim Mohd Salleh, N.; Chamhuri, N. A Non-Market Valuation Approach to Environmental Cost-Benefit Analysis for Sanitary Landfill Project Appraisal. Sustainability 2021, 13, 7718. [Google Scholar] [CrossRef]
- Kareem, S.L.; Al-Mamoori, S.K.; Al-Maliki, L.A.; Al-Dulaimi, M.Q.; Al-Ansari, N. Optimum location for landfills landfill site selection using GIS technique: Al-Naja city as a case study. Cogent Eng. 2021, 8, 1863171. [Google Scholar] [CrossRef]
- Diaz, L.F.; Savage, G.M.; Eggerth, L.L. Alternatives for the treatment and disposal of healthcare wastes in developing countries. Waste Manag. 2005, 25, 626–637. [Google Scholar] [CrossRef]
- Ilyas, S.; Srivastava, R.R.; Kim, H. Disinfection technology and strategies for COVID-19 hospital and bio-medical waste management. Sci. Total Environ. 2020, 749, 141652. [Google Scholar] [CrossRef]
- Datta, P.; Mohi, G.K.; Chander, J. Biomedical waste management in India: Critical appraisal. J. Lab. Phys. 2018, 10, 6–14. [Google Scholar] [CrossRef] [Green Version]
- Wang, J.; Shen, J.; Ye, D.; Yan, X.; Zhang, Y.; Yang, W.; Li, X.; Wang, J.; Zhang, L.; Pan, L. Disinfection technology of hospital wastes and wastewater: Suggestions for disinfection strategy during coronavirus disease 2019 (COVID-19) pandemic in China. Environ. Pollut. 2020, 262, 114665. [Google Scholar] [CrossRef]
- Karagiannidis, A.; Papageorgiou, A.; Perkoulidis, G.; Sanida, G.; Samaras, P. A multi-criteria assessment of scenarios on thermal processing of infectious hospital wastes: A case study for Central Macedonia. Waste Manag. 2010, 30, 251–262. [Google Scholar] [CrossRef]
- Voudrias, E.A. Technology selection for infectious medical waste treatment using the analytic hierarchy process. J. Air Waste Manag. Assoc. 2016, 66, 663–672. [Google Scholar] [CrossRef] [Green Version]
- Voudrias, E.; Graikos, A. Infectious Medical Waste Management System at the Regional Level. J. Hazard. Toxic Radioact. Waste 2014, 18, 04014020. [Google Scholar] [CrossRef]
- Lee, C.C.; Huffman, G.L. Review: Medical waste management/incineration. J. Hazard. Mater. 1996, 48, 1–30. [Google Scholar] [CrossRef]
- Schecter, A.; Birnbaum, L.; Ryan, J.J.; Constable, J.D. Dioxins: An overview. Environ. Res. 2006, 101, 419–428. [Google Scholar] [CrossRef]
- Pacyna, E.G.; Pacyna, J.M.; Steenhuisen, F.; Wilson, S. Global anthropogenic mercury emission inventory for 2000. Atmos. Environ. 2006, 40, 4048–4063. [Google Scholar] [CrossRef]
- Wolfe, M.F.; Schwarzbach, S.; Sulaiman, R.A. Effects of mercury on wildlife: A comprehensive review. Environ. Toxicol. Chem. 1998, 2, 146–160. [Google Scholar] [CrossRef]
- Kilgroe, J.D. Control of dioxin, furan, and mercury emissions from municipal waste combustors. J. Hazard. Mater. 1996, 47, 163–194. [Google Scholar] [CrossRef]
- Xu, L.; Dong, K.; Zhang, Y.; Li, H. Comparison and analysis of several medical waste treatment technologies. IOP Conf. Ser. Earth Environ. Sci. 2020, 615, 012031. [Google Scholar] [CrossRef]
- Dharmaraj, S.; Ashokkumar, V.; Pandiyan, R.; Halimatul Munawaroh, H.S.; Chew, K.W.; Chen, W.H.; Ngamcharussrivichai, C. Pyrolysis: An effective technique for degradation of COVID-19 medical wastes. Chemosphere 2021, 275, 130092. [Google Scholar] [CrossRef]
- Czajczyńska, D.; Anguilano, L.; Ghazal, H.; Krzyżyńska, R.; Reynolds, A.J.; Spencer, N.; Jouhara, H. Potential of pyrolysis processes in the waste management sector. Therm. Sci. Eng. Prog. 2017, 3, 171–197. [Google Scholar] [CrossRef]
- Khaskhachikh, V.V.; Kornil’eva, V.F.; Gerasimov, G.Y. Investigation into the Pyrolysis of Medical Waste in a Fixed-Bed Reactor. J. Eng. Phys. Thermophys. 2021, 94, 580–586. [Google Scholar] [CrossRef]
- Zimmermann, K. Microwave as an emerging technology for the treatment of biohazardous waste: A mini-review. Waste Manag. Res. 2017, 35, 471–479. [Google Scholar] [CrossRef] [Green Version]
- Mantzaras, G.; Voudrias, E.A. An optimization model for collection, haul, transfer, treatment and disposal of infectious medical waste: Application to a Greek region. Waste Manag. 2017, 69, 518–534. [Google Scholar] [CrossRef] [PubMed]
- Duarte, P.; Santana, V.T. Disinfection measures and control of SARS-COV-2 transmission. Glob. Biosecur. 2020, 2. [Google Scholar] [CrossRef]
- Cai, X.; Du, C. Thermal Plasma Treatment of Medical Waste. Plasma Chem. Plasma Process. 2021, 41, 1–46. [Google Scholar] [CrossRef]
- Aboughaly, M.; Gabbar, H.A.; Damideh, V.; Hassen, I. RF-ICP Thermal Plasma for Thermoplastic Waste Pyrolysis Process with High Conversion Yield and Tar Elimination. Processes 2020, 8, 281. [Google Scholar] [CrossRef] [Green Version]
- Erdogan, A.A.; Yilmazoglu, M.Z. Plasma gasification of the medical waste. Int. J. Hydrogen Energy 2021, 46, 29108–29125. [Google Scholar] [CrossRef] [PubMed]
- Cahyanti, M.N.; Doddapaneni, T.R.K.C.; Kikas, T. Biomass torrefaction: An overview on process parameters, economic and environmental aspects and recent advancements. Bioresour. Technol. 2020, 301, 122737. [Google Scholar] [CrossRef]
- Giakoumakis, G.E.; Sidiras, D.K. Torrefaction for Increasing Gross Heat of Combustion of Medical Cotton Waste. Int. J. Econ. Manag. Strategy 2017, 2, 350–355. Available online: https://www.iaras.org/iaras/filedownloads/ijems/2017/007-0049(2017).pdf (accessed on 31 October 2021).
- Giakoumakis, G.; Politi, D.V.; Sidiras, D.K. Torrefied medical cotton waste for industrial liquid waste cleaning. In Proceedings of the European Biomass Conference and Exhibition Proceedings, 2018 (26th EUBCE), Copenhagen, Denmark, 14–18 May 2018; pp. 1429–1433. [Google Scholar]
- Kale, R.D.; Gorade, V.G.; Parmaj, O. Waste Medical Cotton Reinforced Chitosan Biocomposite Film Using Tannic Acid as the Crosslinking Agent. J. Nat. Fibers 2018, 17, 1249–1256. [Google Scholar] [CrossRef]
- Emam, H.E.; Saleh, N.H.; Nagy, K.S.; Zahran, M.K. Functionalization of medical cotton by direct incorporation of silver nanoparticles. Int. J. Biol. Macromol. 2015, 78, 249–256. [Google Scholar] [CrossRef]
- Sheriteh, Z.; Hassan, T.; Sherriff, M.; Cobourne, M. Decontamination procedures for tungsten carbide debonding burs: A cross-sectional survey of hospital-based orthodontic departments. J. Orthod. 2010, 37, 174–180. [Google Scholar] [CrossRef]
- Sajjanshetty, S.; Hugar, D.; Hugar, S.; Ranjan, S.; Kadani, M. Decontamination Methods Used for Dental Burs–A Comparative Study. J. Clin. Diagn. Res. 2014, 8, 39–41. [Google Scholar] [CrossRef]
- Chen, H. Lignocellulose biorefinery feedstock engineering. In Lignocellulose Biorefinery Engineering, 1st ed.; Elsevier: Amsterdam, The Netherlands, 2015; pp. 37–86. [Google Scholar] [CrossRef]
- Giakoumakis, G.; Sidiras, D. Acid Hydrolysis Pretreated Recycled Medical Cotton Waste as Heating Energy Material. In Proceedings of the 27th European Biomass Conference and Exhibition, Lisbon, Portugal, 27–30 May 2019; pp. 1213–1217. [Google Scholar]
- Giakoumakis, G.; Sidiras, D. Acid Hydrolyzed Medical Cotton Waste as a Methylene Blue Low-Cost Adsorbent. In Proceedings of the 28th European Biomass Conference and Exhibition, e-EUBCE 2020, Marseille, France, 6–9 July 2020; pp. 660–664. [Google Scholar]
- Giakoumakis, G.; Karnaouri, A.; Topakas, E.; Sidiras, D. Simulation and optimization of combined acid pretreatment and enzymatic saccharification of medical cotton waste. Biomass Convers. Biorefin. 2021, 11, 515–526. [Google Scholar] [CrossRef]
- Sun, Y.; Cheng, J. Hydrolysis of lignocellulosic materials for ethanol production: A review. Bioresour. Technol. 2002, 83, 1–11. [Google Scholar] [CrossRef]
- Dimos, K.; Paschos, T.; LouLoudi, A.; Kalogiannis, K.; Lappas, A.A.; Papayannakos, N.; Kekos, D. Effect of various pretreatment methods on bioethanol production from cotton stalks. Fermentation 2019, 5, 5. [Google Scholar] [CrossRef] [Green Version]
- Andrić, P.; Meyer, A.S.; Jensen, P.A.; Dam-Johansen, K. Reactor design for minimizing product inhibition during enzymatic lignocellulose hydrolysis: I. Significance and mechanism of cellobiose and glucose inhibition on cellulolytic enzymes. Biotechnol. Adv. 2010, 28, 308–324. [Google Scholar] [CrossRef]
- Duff, S.J.B.; Murray, W.D. Bioconversion of forest products industry waste cellulosics to fuel ethanol: A review. Bioresour. Technol. 1996, 55, 1–33. [Google Scholar] [CrossRef]
- Yang, B.; Dai, Z.; Ding, S.Y.; Wyman, C.E. Enzymatic hydrolysis of cellulosic biomass. Biofuels 2011, 2, 421–449. [Google Scholar] [CrossRef] [Green Version]
- Cheung, S.W.; Anderson, B.C. Laboratory investigation of ethanol production from municipal primary wastewater solids. Bioresour. Technol. 1997, 59, 81–96. [Google Scholar] [CrossRef]
- Vignesh, N.; Chandraraj, K. Improved high solids loading enzymatic hydrolysis and fermentation of cotton microdust by surfactant addition and optimization of pretreatment. Process Biochem. 2021, 106, 60–69. [Google Scholar] [CrossRef]
- Rasul, S.B.; Som, U.; Hossain, M.S.; Rahman, M. Liquid fuel oil produced from plastic based medical wastes by thermal cracking. Sci. Rep. 2021, 11, 17048. [Google Scholar] [CrossRef]
- Som, U.; Rahman, F.; Hossain, S. Recovery of Pyrolytic Oil from Thermal Pyrolysis of Medical Waste. J. Eng. Sci. 2018, 5, H5–H8. [Google Scholar] [CrossRef]
- Shen, Y.; Yu, S.; Ge, S.; Chen, X.; Ge, X.; Chen, M. Hydrothermal carbonization of medical wastes and lignocellulosic biomass for solid fuel production from lab-scale to pilot-scale. Energy 2017, 118, 312–323. [Google Scholar] [CrossRef] [Green Version]
- Fang, S.; Jiang, L.; Li, P.; Bai, J.; Chang, C. Study on pyrolysis products characteristics of medical waste and fractional condensation of the pyrolysis oil. Energy 2020, 195, 16969. [Google Scholar] [CrossRef]
- Xin, S.; Huang, F.; Liu, X.; Mi, T.; Xu, Q. Torrefaction of herbal medicine wastes: Characterization of the physicochemical properties and combustion behaviors. Bioresour. Technol. 2019, 287, 121408. [Google Scholar] [CrossRef]
- Li, X.; Xu, Q.; Shen, H.; Guo, Y.; Wu, M.; Peng, Y.; Zhang, L.; Zhao, Z.K.; Liu, Y.; Xie, H. Capturing CO2 to reversible ionic liquids for dissolution pretreatment of cellulose towards enhanced enzymatic hydrolysis. Carbohydr. Polym. 2019, 204, 50–58. [Google Scholar] [CrossRef]
- Gan, J.; Peng, Y. Reversible covalent chemistry of carbon dioxide unlocks the recalcitrance of cellulose for its enzymatic saccharification. Bioresour. Technol. 2020, 295, 22230. [Google Scholar] [CrossRef]
- Dash, A.; Kumar, S.; Singh, R.K. Thermolysis of Medical Waste (Waste Syringe) to Liquid Fuel Using Semi Batch Reactor. Waste Biomass Valor 2015, 6, 507–514. [Google Scholar] [CrossRef]
- Baghdadi, M.; Alipour Soltani, B.; Nourani, M. Malachite green removal from aqueous solutions using fibrous cellulose sulfate prepared from medical cotton waste: Comprehensive batch and column studies. J. Ind. Eng. Chem. 2017, 55, 128–139. [Google Scholar] [CrossRef]
- Mohseni-Bandpei, A.; Majlesi, M.; Rafiee, M.; Nojavan, S.; Nowrouz, P.; Zolfagharpour, H. Polycyclic aromatic hydrocarbons (PAHs) formation during the fast pyrolysis of hazardous health-care waste. Chemosphere 2019, 227, 277–288. [Google Scholar] [CrossRef]
- Ismail, Z.Z.; Talib, A.R. Recycled medical cotton industry waste as a source of biogas recovery. J. Clean. Prod. 2016, 112, 4413–4418. [Google Scholar] [CrossRef]
- Arcuri, C.; Luciani, F.; Piva, P.; Bartuli, F.; Ottria, L.; Mecheri, B.; Licoccia, S. Medical waste to energy: Experimental study. Oral Implantol. 2014, 6, 83–88. [Google Scholar] [CrossRef]
- Alam, M.T.; Lee, J.-S.; Lee, S.Y.; Bhatta, D.; Yoshikawa, K.; Seo, Y.-C. Low Chlorine Fuel Pellets Production from the Mixture of Hydrothermally Treated Hospital Solid Waste, Pyrolytic Plastic Waste Residue and Biomass. Energies 2019, 12, 4390. [Google Scholar] [CrossRef] [Green Version]
- Manegdeg, F.; Coronado, L.O.; Paña, R. Medical waste treatment and electricity generation using pyrolyzer-rankine cycle for specialty hospitals in Quezon City, Philippines. IOP Conf. Ser. Earth Environ. Sci. 2020, 463, 012180. [Google Scholar] [CrossRef]
- Bujak, J. Thermal treatment of medical waste in a rotary kiln. J. Environ. Manag. 2015, 162, 139–147. [Google Scholar] [CrossRef]
- Bujak, J. Experimental study of the energy efficiency of an incinerator for medical waste. Appl. Energy 2009, 86, 2386–2393. [Google Scholar] [CrossRef]
- Bujak, J.W. Heat recovery from thermal treatment of medical waste. Energy 2015, 90, 1721–1732. [Google Scholar] [CrossRef]
- Świechowski, K.; Leśniak, M.; Białowiec, A. Medical Peat Waste Upcycling to Carbonized Solid Fuel in the Torrefaction Process. Energies 2021, 14, 6053. [Google Scholar] [CrossRef]
- Chaiyat, N. Energy, exergy, economic, and environmental analysis of an organic Rankine cycle integrating with infectious medical waste incinerator. Therm. Sci. Eng. Prog. 2021, 22, 100810. [Google Scholar] [CrossRef]
- Zroychikov, N.A.; Fadeev, S.A.; Bezruky, P.P. Development of an Environmentally Safe Process for Medical Waste Disposal Based on Pyrolysis. Therm. Eng. 2018, 65, 833–840. [Google Scholar] [CrossRef]
- Álvarez, A.M. Analysis of the Thermal Treatment of Plastic Medical Waste. Master’s Thesis, Comillas Pontifical University, Madrid, Spain, 2018. Available online: https://repositorio.comillas.edu/rest/bitstreams/143601/retrieve (accessed on 16 November 2021).
- Llewellyn, K. Incineration, Waste-to-Energy and Catalytic Gasification: The Past, Present and Future of Medical Waste Management. Master’s Thesis, Columbia University, New York, NY, USA, 2006. Available online: https://gwcouncil.org/wp-content/uploads/2020/10/llewellyn_thesis.pdf (accessed on 15 November 2021).
- Ökten, H.E.; Corum, A.; Demir, H.H. A comparative economic analysis for medical waste treatment options. Environ. Prot. Eng. 2015, 41, 138–145. [Google Scholar] [CrossRef]
- Soares, S.R.; Rodrigues, A.F.; Prudêncio da Silva, V.; Rodrigo, A.F. Applications of life cycle assessment and cost analysis in health care waste management. Waste Manag. 2013, 33, 175–183. [Google Scholar] [CrossRef] [PubMed]
- Kargar, S.; Pourmehdi, M.; Paydar, M.M. Reverse logistics network design for medical waste management in the epidemic outbreak of the novel coronavirus (COVID-19). Sci. Total. Environ. 2020, 746, 141183. [Google Scholar] [CrossRef] [PubMed]
- Liu, Z.; Liu, T.; Liu, X.; Wei, A.; Wang, X.; Yin, Y.; Li, Y. Research on Optimization of Healthcare Waste Management System Based on Green Governance Principle in the COVID 19 Pandemic. Int. J. Environ. Res. Public Health 2021, 18, 5316. [Google Scholar] [CrossRef] [PubMed]
- Torkayesh, A.E.; Vandchali, H.R.; Tirkolaee, E.B. Multi-Objective Optimization for Healthcare Waste Management Network Design with Sustainability Perspective. Sustainability 2021, 13, 8279. [Google Scholar] [CrossRef]
- Ghannadpour, S.F.; Zandieh, F.; Esmaeili, F. Optimizing triple bottom-line objectives for sustainable health-care waste collection and routing by a self-adaptive evolutionary algorithm: A case study from tehran province in Iran. J. Clean. Prod. 2021, 287, 125010. [Google Scholar] [CrossRef]
- Rolewicz-Kalińska, A. Logistic Constraints as a Part of a Sustainable Medical Waste Management System. Transp. Res. Proc. 2016, 16, 473–482. [Google Scholar] [CrossRef] [Green Version]
- Van Straten, B.; Dankelman, J.; Van der Eijk, A.; Horeman, T. A Circular Healthcare Economy; a feasibility study to reduce surgical stainless steel waste. Sustain. Prod. Consum. 2021, 27, 169–175. [Google Scholar] [CrossRef]
- Yao, L.; Xu, Z.; Zeng, Z. A Soft-Path Solution to Risk Reduction by Modeling Medical Waste Disposal Center Location-Allocation Optimization. Risk Anal. 2020, 40, 1863–1886. [Google Scholar] [CrossRef]
- Arun, K.P.; Wang, S.J. The Design Intervention Opportunities to Reduce Procedural-Caused Healthcare Waste Under the Industry 4.0 Context—A Scoping Review. In Interactivity and Game Creation; Brooks, A., Brooks, E.I., Jonathan, D., Eds.; Lecture Notes of the Institute for Computer Sciences, Social Informatics and Telecommunications Engineering; Springer: Cham, Switzerland, 2021; Volume 367. [Google Scholar] [CrossRef]
- Ranjbari, M.; Esfandabadi, Z.S.; Shevchenko, T.; Chassagnon-Haned, N.; Peng, W.; Tabatabaei, M.; Aghbashlo, M. Mapping healthcare waste management research: Past evolution, current challenges, and future perspectives towards a circular economy transition. J. Hazard. Mater. 2022, 422, 126724. [Google Scholar] [CrossRef]
- Chaerul, M.; Tanaka, M.; Shekdar, A.V. Resolving complexities in healthcare waste management: A goal programming approach. Waste Manag. Res. 2008, 26, 217–232. [Google Scholar] [CrossRef]
- Nursetyowati, P.; Nadifameidita, F.Q.; Fairus, S.; Surya Irawan, D.; Rohajawati, S. Optimization of medical hazardous waste management in community health centers of depok city using analytical hierarchy process (AHP) method. J. Phys. Conf. Ser. 2019, 1364, 012040. [Google Scholar] [CrossRef]
- Mei, X.; Hao, H.; Sun, Y.; Wang, X.; Zhou, Y. Optimization of medical waste recycling network considering disposal capacity bottlenecks under a novel coronavirus pneumonia outbreak. Environ. Sci. Pollut. Res. Int. 2021, 1–19. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Country | Total Medical Waste (Kg/Bed/Day) | Hazardous Medical Waste (Kg/Bed/Day) | References |
|---|---|---|---|
| Algeria | 1.0 | [8] | |
| Belgium | 1.4 | [33] | |
| Brazil | 4.4 | 2.3 | [34] |
| Bolivia | 0.5 | [8] | |
| Bulgaria | 2.0 | [8] | |
| Canada | 8.2 | [35] | |
| China | 0.6 | [8] | |
| Ecuador | 0.4 | [8] | |
| Egypt | 1.2 | [8] | |
| Ethiopia | 1.1 | 0.6 | [36] |
| Ethiopia | 6.03 | [37] | |
| France | 3.3 | [8] | |
| Germany | 3.6 | 1.4 | [38] |
| Greece | 0.26–0.89 | [39] | |
| Greece | 1.4 | [40] | |
| Greece | 1.5 | [41] | |
| Greece | 0.33 | [29] | |
| Greece | 0.4 | [30] | |
| India | 0.5 | [41] | |
| Iran | 3.5 | 1.039 | [42] |
| Ireland | 7.7 | [43] | |
| Italy | 1.0 | [33] | |
| Japan | 2.3 | [8] | |
| Kazakhstan | 5.34 | 1.2 | [44] |
| Kuwait | 3.8 | [31] | |
| Latvia | 1.18 | [45] | |
| Lebanon | 2.45 | 0.95 | [26] |
| Libya | 1.3 | [46] | |
| Netherlands | 1.7 | 0.7 | [38] |
| Nigeria | 2.5 | [8] | |
| Norway | 3.9 | [8] | |
| Pakistan | 2.2 | [47] | |
| Pakistan | 2 | [48] | |
| Palestine | 1.57 | 0.78 | [49] |
| Portugal | 1.5 | [33] | |
| Serbia | 1.9 | [8] | |
| Spain | 4.4 | [50] | |
| Taiwan | 1.9 | [8] | |
| UK | 3.3 | [50] | |
| USA | 8.4 | [8] | |
| Vietnam | 1.57 | 0.14 | [51] |
| Yemen | 2.41 | 0.63 | [52] |
| General | Recyclable | Hazardous | Radioactive | Plastics/Sharps | Pharmaceutical | Toxic | Chemical | Infectious | Blood Banks | Pathological | References |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Yes | Yes | Yes | Yes | Yes | [61] | ||||||
| Yes | Yes | Yes | Yes | Yes | Yes | Yes | [62] | ||||
| Yes | Yes | Yes | Yes | [63] | |||||||
| Yes | Yes | Yes | Yes | Yes | [64] | ||||||
| Yes | Yes | Yes | Yes | Yes | Yes | [65] | |||||
| Yes | Yes | Yes | Yes | Yes | [55] | ||||||
| Yes | Yes | Yes | [66] | ||||||||
| Yes | Yes | Yes | Yes | Yes | Yes | [67] | |||||
| Yes | Yes | Yes | Yes | Yes | [31] | ||||||
| Yes | Yes | Yes | Yes | Yes | [68] | ||||||
| Yes | Yes | Yes | [69] | ||||||||
| Yes | Yes | Yes | Yes | Yes | Yes | Yes | [70] | ||||
| Yes | Yes | Yes | Yes | [71] | |||||||
| Yes | Yes | Yes | [72] | ||||||||
| Yes | Yes | Yes | Yes | Yes | Yes | Yes | [57] | ||||
| Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | [5] | |
| Yes | Yes | Yes | Yes | Yes | Yes | Yes | [73] | ||||
| Yes | Yes | Yes | Yes | Yes | [74] | ||||||
| Yes | Yes | Yes | Yes | Yes | Yes | [75] | |||||
| Yes | Yes | Yes | Yes | [76] | |||||||
| Yes | Yes | Yes | Yes | Yes | Yes | Yes | [77] | ||||
| Yes | Yes | Yes | Yes | Yes | [78] | ||||||
| Yes | Yes | Yes | Yes | Yes | [79] | ||||||
| Yes | Yes | Yes | Yes | [46] | |||||||
| Yes | Yes | Yes | Yes | Yes | Yes | [80] | |||||
| Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | [8] | |||
| Yes | Yes | Yes | Yes | [40] | |||||||
| Yes | Yes | Yes | Yes | Yes | Yes | [41] | |||||
| Yes | Yes | Yes | Yes | [14] |
| Country | Source | Source No | General | Plastic | Textile | Glass | Metal | Paper | Organic | References |
|---|---|---|---|---|---|---|---|---|---|---|
| Canada | NA | 14% | 3% | 2% | 45% | 17% | [81] | |||
| China | MSWAC | 1 | 45% | 30% | 2.50% | 2.50% | 10% | [82] | ||
| China | NA | - | 56% | 36% | 4% | 4% | [8] | |||
| Egypt | H | 8 | 19% | 17% | 9% | 1% | 24% | 28% | [83] | |
| Greece | H | 29 | 18% | 8% | 9% | 47% | 16% | [40] | ||
| Greece | HF | 1 | 82% | 4% | 6% | [66] | ||||
| India | GH/AH | 2/1 | 54% | 10% | 15% | 4% | 1% | 15% | [84] | |
| Iran | EH | 12 | 29% | 16% | 8% | 2% | 14% | 31% | [85] | |
| Iran | EH/UH/MH/PH/GoH | 10 | 23% | 11% | 4% | 1% | 13% | 31% | [43] | |
| Iran | H | 3 | 30% | 14% | 4% | 1% | 19% | 18% | [86] | |
| Iran | H | 14 | 41% | 17% | 4% | 5% | 8% | 21% | [87] | |
| Italy | NA | 47% | 7% | 2% | 33% | [88] | ||||
| Jordan | H | 21 | 27% | 11% | 10% | 5% | 38% | [89] | ||
| Korea | HF | 478 | 47% | 6% | 37% | [72] | ||||
| Kuwait | PH | 2 | 18% | 11% | 10% | 9% | 32% | 12% | [31] | |
| Libya | UH/PC/HC/PrH/GH | 2/2/2/4 | 24% | 9% | 8% | 1% | 20% | 38% | [46] | |
| Mauritius | NH/GH/PrC | 1/1/1 | 24% | 8% | 3% | 24.00% | 13% | [90] | ||
| Pakistan | CH | 1 | 57% | 11.00% | 3.00% | [42] | ||||
| Palestine | GH | 3 | 30% | 2% | 8% | 2% | 33% | 25% | [49] | |
| Taiwan | UH | 1 | 50% | 10% | 16% | 22% | [76] | |||
| Turkey | GH/MH | 3/1 | 3% | 41% | 10.20% | 7.20% | 0.80% | 20.70% | 17.10% | [32] |
| UK | H | 21% | 2% | 47% | 14% | [33] | ||||
| USA | NA | 15% | 7% | 10% | 45% | 10% | [91] | |||
| Yemen | GH | 4 | 22% | 11% | 10% | 22% | 27% | [52] |
| Country | Material | Technology | Fuels/Materials | Energy Content | Energy/Recovery Efficiency | Reference |
|---|---|---|---|---|---|---|
| Bangladesh | plastic MW | Thermal cracking (Batch reactor) | Liquid 52% | 41.3MJ/kg | [153] | |
| Bangladesh | plastic MW | Pyrolysis | Liquid | 41.3 MJ/kg | [154] | |
| China | MW | Rotary kiln incineration | 64% | [93] | ||
| China | MW | Pyrolysis incineration | 55% | [93] | ||
| China | MW | Plasma melting | 19% | [93] | ||
| China | MW | Steam sterilization | 83% | [93] | ||
| China | MW | Microwave sterilization | 84% | [93] | ||
| China | MW | Incineration | 30% | [82] | ||
| China | MW | Autoclave | 10% | [82] | ||
| China | PVC MW | Hydrothermal carbonization | Hydrochar particles | 24.2 MJ/kg | [155] | |
| China | MW | Pyrolysis | Gas/liquid/solid | 46 MJ/Nm3, 37.6 MJ/kg, 22.8 MJ/kg | [156] | |
| China | medicine herbal waste | Torrefaction | Solid | 20.3 MJ/kg | [157] | |
| Greece | cotton MW | Acid/enzymatic hydrolysis | Bioethanol/sugars | [145] | ||
| Greece | cotton MW | Torrefaction | Solid | 20.1 MJ/kg | [136] | |
| Greece | cotton MW | Acid hydrolysis | Adsorbent | [144] | ||
| Greece | cotton MW | Torrefaction | Adsorbent | [137] | ||
| India | Medical syringes | Pyrolysis | Gas 17% | 42.5 MJ/kg | [160] | |
| India | plastic MW (PET) | Pyrolysis | Liquid/gas | [126] | ||
| India | plastic MW (HDPE) | Pyrolysis | Liquid/gas | [126] | ||
| India | plastic MW (LDPE) | Pyrolysis | Gas/liquid/solid | [126] | ||
| India | plastic MW (PVC) | Pyrolysis | Liquid/gas | [126] | ||
| India | plastic MW (PP) | Pyrolysis | Gas/liquid/solid | [126] | ||
| India | plastic MW (PS) | Pyrolysis | Liquid/gas | [126] | ||
| Iran | cotton MW | Sulfonation | Adsorbent | [161] | ||
| Iran | plastic MW | Pyrolysis | Solid 24%/gas 2.5% | [162] | ||
| Iraq | cotton MW | Anaerobic digestion | Biogas 51.6 mL/g | [163] | ||
| Italy | Blood/saliva MW | Enzymatic oxidation | Electric energy | [164] | ||
| Korea | solid MW | Hydrothermal treatment | Pellets | 28.3MJ/kg | [165] | |
| Philippines | noninfectious MW | Pyrolysis, Rankine cycle | 30 MJ/kg | [166] | ||
| Poland | MW | Rotary kiln incineration | 25 MJ/kg | [167] | ||
| Poland | MW | Incineration | 62% | [168] | ||
| Poland | MW | Incineration/Steam heat recovery system | 80% | [169] | ||
| Poland | peat MW | Torrefaction | Solid | 21.3 MJ/kg | [170] | |
| Russia | MW | Pyrolysis | Gas/solid | [172] | ||
| Spain | Plastic MW | Incineration | 30.7 MJ/kg | [173] | ||
| Thailand | Infectious MW | Incineration, Rankine cycle | 51240 kWh/y | [171] | ||
| Turkey | MW | Plasma gasification | H2 | 5.64 MJ/m3 | [134] | |
| USA | MW | gasification | syngas | [174] |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Giakoumakis, G.; Politi, D.; Sidiras, D. Medical Waste Treatment Technologies for Energy, Fuels, and Materials Production: A Review. Energies 2021, 14, 8065. https://doi.org/10.3390/en14238065
Giakoumakis G, Politi D, Sidiras D. Medical Waste Treatment Technologies for Energy, Fuels, and Materials Production: A Review. Energies. 2021; 14(23):8065. https://doi.org/10.3390/en14238065
Chicago/Turabian StyleGiakoumakis, Georgios, Dorothea Politi, and Dimitrios Sidiras. 2021. "Medical Waste Treatment Technologies for Energy, Fuels, and Materials Production: A Review" Energies 14, no. 23: 8065. https://doi.org/10.3390/en14238065