
Oral Preparation of Hyaluronic Acid, Chondroitin Sulfate, Curcumin, and Quercetin (Ialuril® Soft Gels) for the Prevention of LUTS after Intravesical Chemotherapy

 ,
,  , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
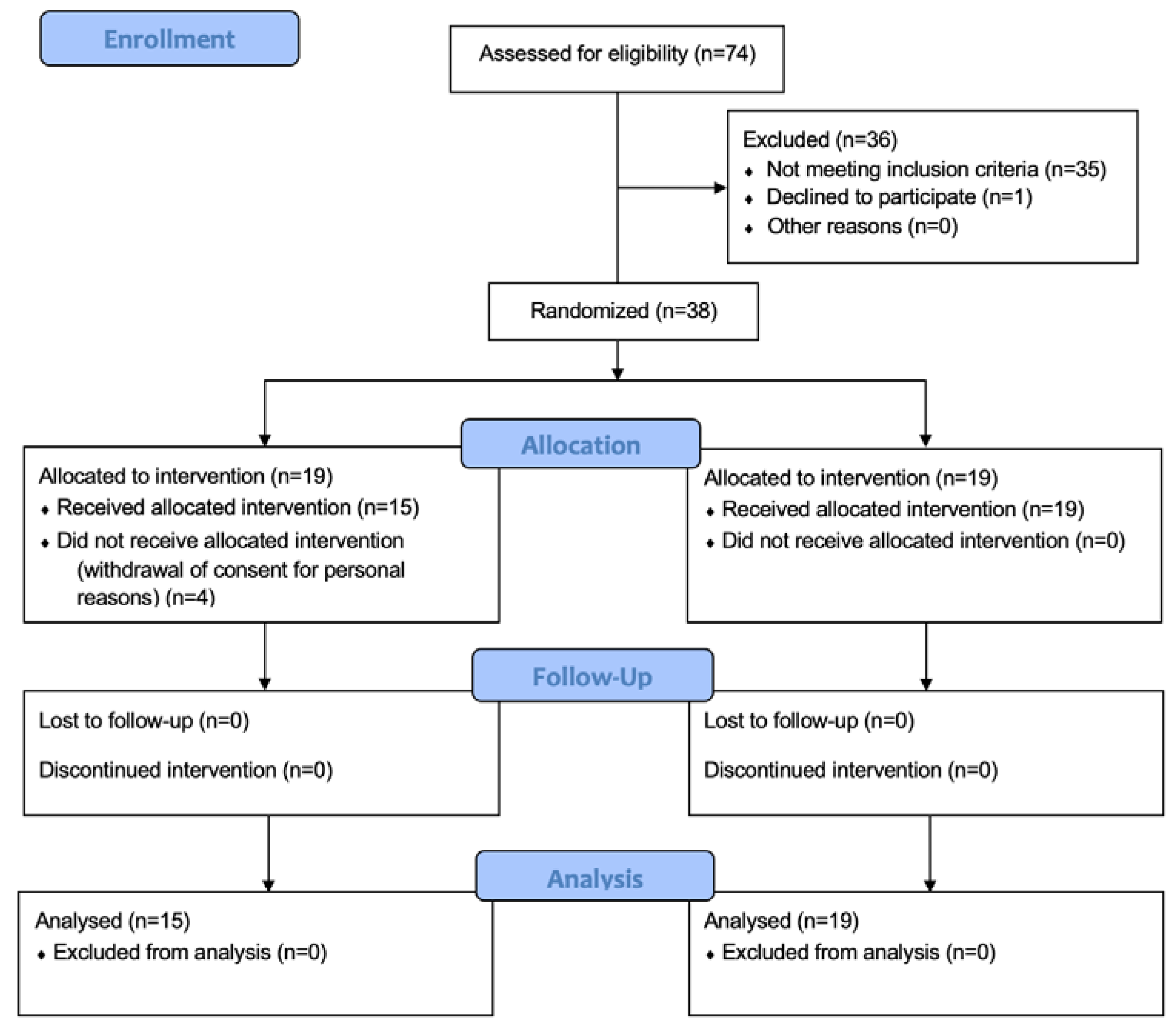
2.1. Study Design
2.2. Inclusion and Exclusion Criteria
2.3. Patient Assessment and Data Collection
2.4. Treatment Protocol
2.5. Statistics
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- IARC. Estimated Number of New Cases in 2020, Worldwide, Both Sexes, All Ages. Available online: https://gco.iarc.fr/today/data/factsheets/populations/900-world-fact-sheets.pdf (accessed on 25 May 2022).
- Freedman, N.D.; Silverman, D.T.; Hollenbeck, A.R.; Schatzkin, A.; Abnet, C.C. Association between smoking and risk of bladder cancer among men and women. JAMA 2011, 306, 737. [Google Scholar] [CrossRef] [PubMed]
- Crocetto, F.; Arcaniolo, D.; Napolitano, L.; Barone, B.; La Rocca, R.; Capece, M.; Caputo, V.F.; Imbimbo, C.; De Sio, M.; Calace, F.P.; et al. Impact of Sexual Activity on the Risk of Male Genital Tumors: A Systematic Review of the Literature. Int. J. Environ. Res. Public Health 2021, 18, 8500. [Google Scholar] [CrossRef] [PubMed]
- Veskimäe, E.; Espinos, E.L.; Bruins, H.M.; Yuan, Y.; Sylvester, R.; Kamat, A.M.; Shariat, S.F.; Witjes, J.A.; Comperat, E.M. What Is the Prognostic and Clinical Importance of Urothelial and Nonurothelial Histological Variants of Bladder Cancer in Predicting Oncological Outcomes in Patients with Muscle-invasive and Metastatic Bladder Cancer? A European Association of Urology Muscle Invasive and Metastatic Bladder Cancer Guidelines Panel Systematic Review. Eur. Urol. Oncol. 2019, 2, 625. [Google Scholar] [PubMed]
- Babjuk, M.; Oosterlinck, W.; Sylvester, R.; Kaasinen, E.; Böhle, A.; Palou, J.; Rouprêt, M. EAU Guidelines on Non-Muscle-Invasive Bladder Cancer (TaT1 and CIS); EAU Guidelines Office: Arnhem, The Netherlands, 2022; ISBN 978–94–92671–16–5. [Google Scholar]
- Balasubramanian, A.; Gunjur, A.; Weickhardt, A.; Papa, N.; Bolton, D.; Lawrentschuk, N.; Perera, M. Adjuvant therapies for non-muscle-invasive bladder cancer: Advances during BCG shortage. World J. Urol. 2022, 40, 1111–1124. [Google Scholar] [CrossRef]
- Califano, G.; Ouzaid, I.; Verze, P.; Stivalet, N.; Hermieu, J.F.; Xylinas, E. New immunotherapy treatments in non-muscle invasive bladder cancer. Arch. Esp. Urol. 2020, 73, 945–953. [Google Scholar]
- Deng, T.; Liu, B.; Duan, X.; Zhang, T.; Cai, C.; Zeng, G. Systematic Review and Cumulative Analysis of the Combination of Mitomycin C plus Bacillus Calmette-Guérin (BCG) for Non-Muscle-Invasive Bladder Cancer. Sci. Rep. 2017, 7, 3172. [Google Scholar] [CrossRef] [Green Version]
- Addeo, R.; Caraglia, M.; Bellini, S.; Abbruzzese, A.; Vincenzi, B.; Montella, L.; Miragliuolo, A.; Guarrasi, R.; Lanna, M.; Cennamo, G.; et al. Randomized phase III trial on gemcitabine versus mytomicin in recurrent superficial bladder cancer: Evaluation of efficacy and tolerance. J. Clin. Oncol. 2010, 28, 543–548. [Google Scholar] [CrossRef]
- Thrasher, J.B.; Crawford, E.D. Complications of intravesical chemotherapy. Urol. Clin. North Am. 1992, 19, 529–539. [Google Scholar] [CrossRef]
- Petca, R.C.; Popescu, R.I.; Toma, C.; Dumitrascu, M.C.; Petca, A.; Sandru, F.; Sandru, F.; Chibelean, C.B. Chemical hemorrhagic cystitis: Diagnostic and therapeutic pitfalls (Review). Exp. Ther. Med. 2021, 21, 624. [Google Scholar] [CrossRef]
- Wei, L.; Li, Q.; Liang, H.; Jianbo, L. The quality of life in patients during intravesical treatment and correlation with local symptoms. J. Chemother. 2014, 26, 165–168. [Google Scholar] [CrossRef]
- Ustundağ, Y.; Huysal, K.; Guzelsoy, M.; Genim, C.E.; Yavuz, A. Urine and serum glycosaminoglycan levels in the diagnosis of urological diseases and conditions: A narrative review of the literature. Urologia 2021, 88, 103–109. [Google Scholar] [CrossRef] [PubMed]
- Klingler, C.H. Glycosaminoglycans: How much do we know about their role in the bladder? Urologia 2016, 83 (Suppl. 1), 11–14. [Google Scholar] [CrossRef] [PubMed]
- Imperatore, V.; Creta, M.; Di Meo, S.; Buonopane, R.; Longo, N.; Fusco, F.; Spirito, L.; Imbimbo, C.; Mirone, V. Intravesical administration of combined hyaluronic acid and chondroitin sulfate can improve symptoms in patients with refractory bacillus Calmette-Guerin-induced chemical cystitis: Preliminary experience with one-year follow-up. Arch. Ital. Urol. Androl. 2018, 90, 11–14. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lazzeri, M.; Hurle, R.; Casale, P.; Buffi, N.; Lughezzani, G.; Fiorini, G.; Peschechera, R.; Pasini, L.; Zandegiacomo, S.; Benetti, A.; et al. Managing chronic bladder diseases with the administration of exogenous glycosaminoglycans: An update on the evidence. Ther. Adv. Urol. 2016, 8, 91–99. [Google Scholar] [CrossRef] [Green Version]
- Manfredi, C.; Calace, F.P.; Fusco, F.; Quattrone, C.; Giordano, D.; Crocetto, F.; Creta, M.; De Sio, M.; Arcaniolo, D. Escherichia coli Nissle 1917 as adjuvant therapy in patients with chronic bacterial prostatitis: A non-blinded, randomized, controlled trial. World J. Urol. 2021, 39, 4373–4379. [Google Scholar] [CrossRef]
- Nissenkorn, I.; Herrod, H.; Soloway, M.S. Side effects associated with intravesical mitomycin. J. Urol. 1981, 126, 596–597. [Google Scholar] [CrossRef]
- Sahiner, I.F.; Soylu, H.; Ates, E.; Acar, N.; Ustunel, I.; Danisman, A. Impact of intravesical hyaluronic acid treatment on bladder inflammation in interstitial cystitis rat model. Int. Braz. J. Urol. 2018, 44, 1014–1022. [Google Scholar] [CrossRef]
- Sahebkar, A.; Serban, M.C.; Ursoniu, S.; Banach, M. Effect of curcuminoids on oxidative stress: A systematic review and meta-analysis of randomized controlled trials. J. Funct. Foods 2015, 18, 898–909. [Google Scholar] [CrossRef]
- Grill, A.E.; Koniar, B.; Panyam, J. Co-delivery of natural metabolic inhibitors in a self-microemulsifying drug delivery system for improved oral bioavailability of curcumin. Drug Deliv. Transl. Res. 2014, 4, 344–352. [Google Scholar] [CrossRef] [Green Version]
- Sperlongano, P.; Sperlongano, S.; Foroni, F.; De Lucia, F.P.; Pezzulo, C.; Manfredi, C.; Esposito, E.; Sperlongano, R. Postoperative hypocalcemia: Assessment timing. Int. J. Surg. 2014, 12 (Suppl. 1), S95–S97. [Google Scholar] [CrossRef] [Green Version]
- Redorta, J.P.; Sanguedolce, F.; Pardo, G.S.; Romancik, M.; Vittori, G.; Minervini, A.; Di Maida, F.; Lunik, R.; Colombo, R.; Serretta, V.; et al. Multicentre International Study for the Prevention with iAluRil of Radio-induced Cystitis (MISTIC): A Randomised Controlled Study. Eur. Urol. Open Sci. 2021, 26, 45–54. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Intervention Group (n = 15) | Control Group (n = 19) | p-Value | |
|---|---|---|---|
| Age | 0.082 | ||
| Median (IQR) | 73 (65–78.5) | 69 (61–73.5) | |
| Gender N (%) | 0.118 | ||
| Males Females | 13 (86.7) 2 (13.3) | 15 (79.0) 4 (21.0) | |
| VAS | 0.103 | ||
| Median (IQR) | 21.0 (6.7–41.0) | 28.0 (7.5–59.0) | |
| IPSS | 0.061 | ||
| Median (IQR) | 14.0 (8.0–16.7) | 14.0 (8.5–18.0) | |
| IPSS-QoL | 0.088 | ||
| Median (IQR) | 3 (1.0–4.0) | 3 (2.0–4.0) | |
| Qmax | 0.213 | ||
| Median (IQR) | 13.5 (7.2–19.4) | 14.1 (8.1–18.9) | |
| PVR | 0.191 | ||
| Median (IQR) | 10.0 (0–15.0) | 7.0 (3.7–12.5) |
| Intervention Group (n = 15) | Control Group (n = 19) | p-Value | |
|---|---|---|---|
| Type N (%) | 0.012 | ||
| Primary Recurrent | 13 (86.7) 2 (13.3) | 16 (84.2) 3 (15.8) | |
| Focality N (%) | 0.233 | ||
| Monofocal Multifocal | 8 (53.3) 7 (46.7) | 10 (53.6) 9 (47.4) | |
| Histotype N (%) | 0.087 | ||
| Urothelial Non-urothelial | 15 (100) 0 (0) | 19 (100) 0 (0) | |
| Grading N (%) | 0.122 | ||
| Low-grade High-grade | 11 (73.3) 4 (26.7) | 15 (79.0) 4 (21.0) | |
| Pathologic Stage N (%) | 0.093 | ||
| TaT1 | 9 (60.0) 6 (40.0) | 12 (63.2) 7 (36.8) | |
| EAU Risk group N (%) | 0.321 | ||
| Low risk Intermediate risk | 12 (80) 3 (20) | 14 (73.7) 5 (26.3) |
| Baseline | 1 Month | 4 Months | 7 Months | 13 Months | p-Value * | |
|---|---|---|---|---|---|---|
| Intervention group (n = 15) | 14.0 (8.0–16.7) | 16 (9–18.5) | 13 (9.2–17.5) | 10 (9–15) | 10 (8–16) | 0.067 a 0.322 b 0.001 c (I) 0.001 d (I) |
| Control group (n = 19) | 14.0 (8.5–18.0) | 18 (13–23.7) | 17 (14.2–22.7) | 18 (14–22.7) | 17 (14–21.5) | <0.001 a (W) 0.026 b (W) <0.001 c (W) 0.003 d (W) |
| p-value ** | 0.061 | 0.139 | 0.038 | <0.001 | 0.002 |
| Baseline | 1 Month | 4 Months | 7 Months | 13 Months | p-Value * | |
|---|---|---|---|---|---|---|
| Intervention group (n = 15) | 21.0 (6.7–41.0) | 25 (16.2–45.7) | 20 (11.2–38.75) | 22 (8.5–37.25) | 20 (10–29.2) | 0.342 a 0.054 b 0.077 c 0.328d |
| Control group (n = 19) | 28.0 (7.5–59.0) | 45 (20.5–67.2) | 40 (17–75.7) | 37 (17.7–67.2) | 35 (15.7–60) | <0.001 a (W) <0.001 b (W) 0.001 c (W) 0.001 d (W) |
| p-value ** | 0.103 | 0.145 | 0.092 | 0.021 | 0.024 |
| Local Adverse Event | Intervention Group (n = 15) | Control Group (n = 19) | p-Value |
|---|---|---|---|
| Hematuria N (%) | 3 (20.0) | 5 (26.3) | 0.078 |
| Dysuria N (%) | 4 (26.7) | 7 (36.8) | 0.029 |
| Urinary tract infection N (%) | 0 (0) | 1 (5.3) | 0.433 |
| Component | Dosage | Mechanism of Action |
|---|---|---|
| HA | 20 mg | To restore the GAG layer on the urothelial surface of the bladder |
| CS | 200 mg | To restore the GAG layer on the urothelial surface of the bladder |
| Quercetin | 200 mg | Anti-inflammatory effects due to antioxidant capacity |
| Curcumin | 200 mg | Anti-inflammatory effects due to antioxidant capacity |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Manfredi, C.; Spirito, L.; Calace, F.P.; Balsamo, R.; Terribile, M.; Stizzo, M.; Romano, L.; Napolitano, L.; Califano, G.; Cirillo, L.; et al. Oral Preparation of Hyaluronic Acid, Chondroitin Sulfate, Curcumin, and Quercetin (Ialuril® Soft Gels) for the Prevention of LUTS after Intravesical Chemotherapy. Pathophysiology 2022, 29, 365-373. https://doi.org/10.3390/pathophysiology29030028
Manfredi C, Spirito L, Calace FP, Balsamo R, Terribile M, Stizzo M, Romano L, Napolitano L, Califano G, Cirillo L, et al. Oral Preparation of Hyaluronic Acid, Chondroitin Sulfate, Curcumin, and Quercetin (Ialuril® Soft Gels) for the Prevention of LUTS after Intravesical Chemotherapy. Pathophysiology. 2022; 29(3):365-373. https://doi.org/10.3390/pathophysiology29030028
Chicago/Turabian StyleManfredi, Celeste, Lorenzo Spirito, Francesco Paolo Calace, Raffaele Balsamo, Marco Terribile, Marco Stizzo, Lorenzo Romano, Luigi Napolitano, Gianluigi Califano, Luigi Cirillo, and et al. 2022. "Oral Preparation of Hyaluronic Acid, Chondroitin Sulfate, Curcumin, and Quercetin (Ialuril® Soft Gels) for the Prevention of LUTS after Intravesical Chemotherapy" Pathophysiology 29, no. 3: 365-373. https://doi.org/10.3390/pathophysiology29030028