Soluble Immune Checkpoint Molecules as Predictors of Efficacy in Immuno-Oncology Combination Therapy in Advanced Renal Cell Carcinoma

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients
2.2. ELISA
2.3. Immunohistochemical Analysis
2.4. Statistical Analysis
3. Results
3.1. Patient Characteristics
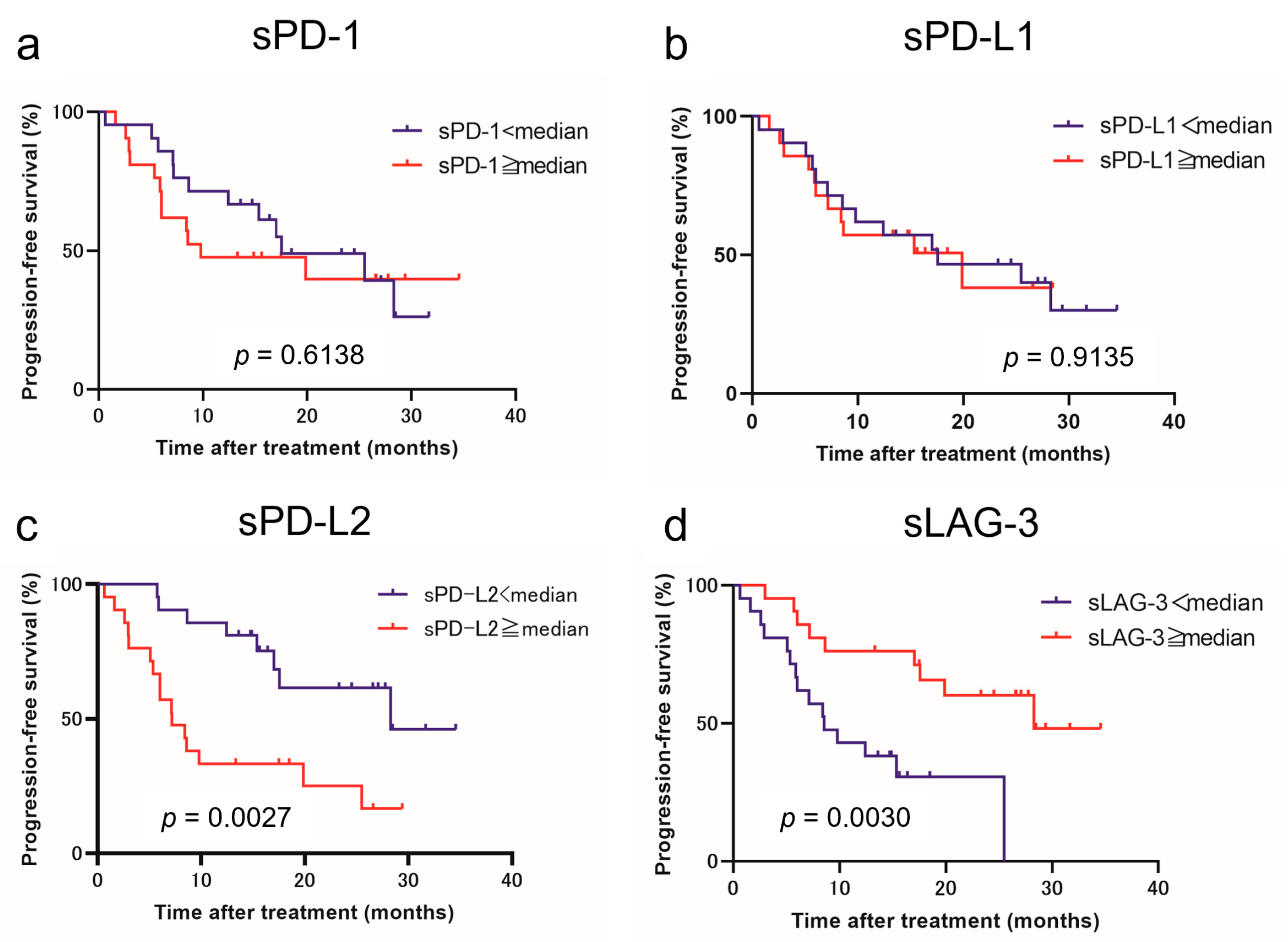
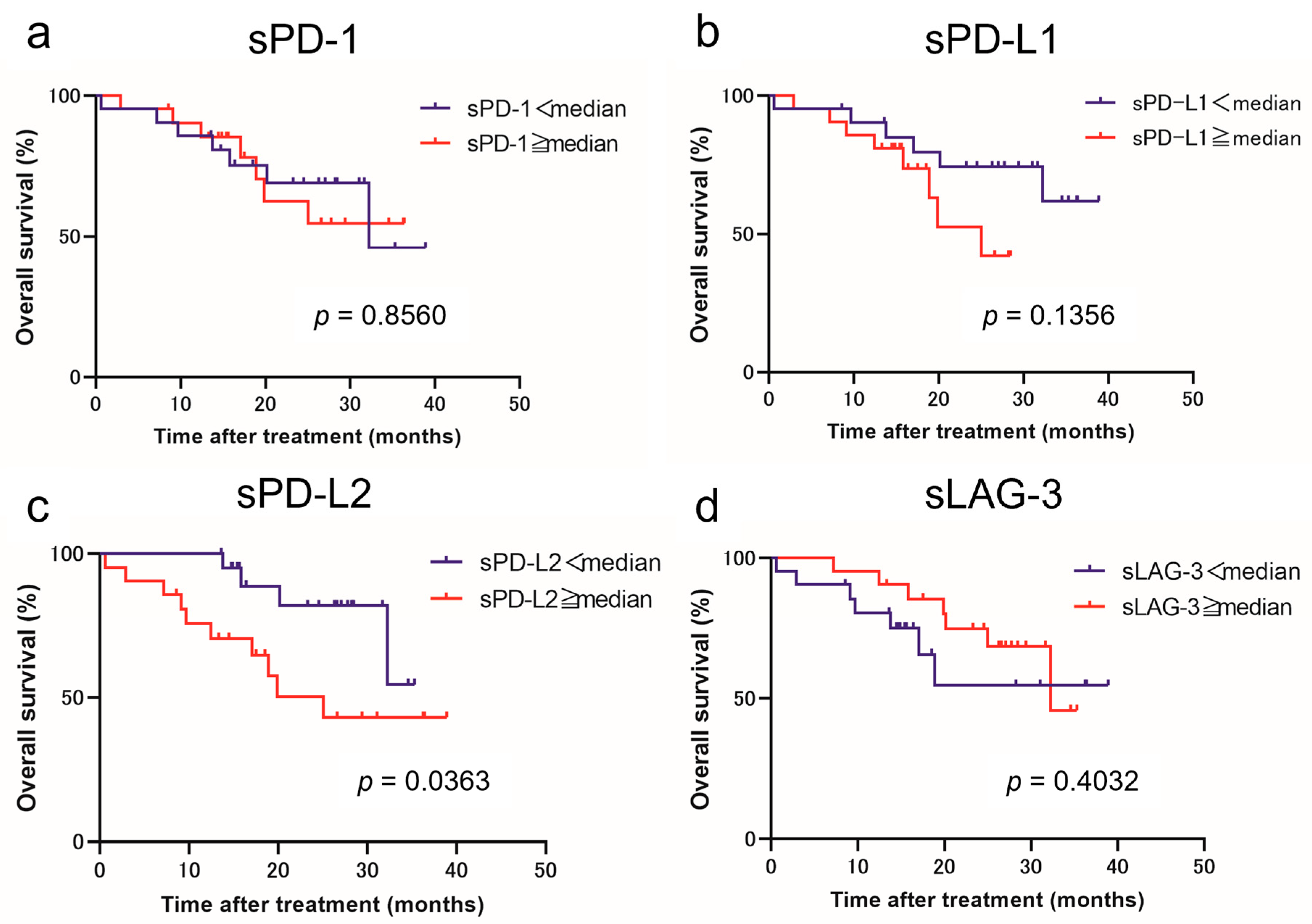
3.2. Baseline Soluble Immune Checkpoint Molecules as Predictive Biomarkers of IO Combination Therapy Outcome in Advanced RCC
3.3. Soluble Immune Checkpoint Molecules Expression and Clinical Course
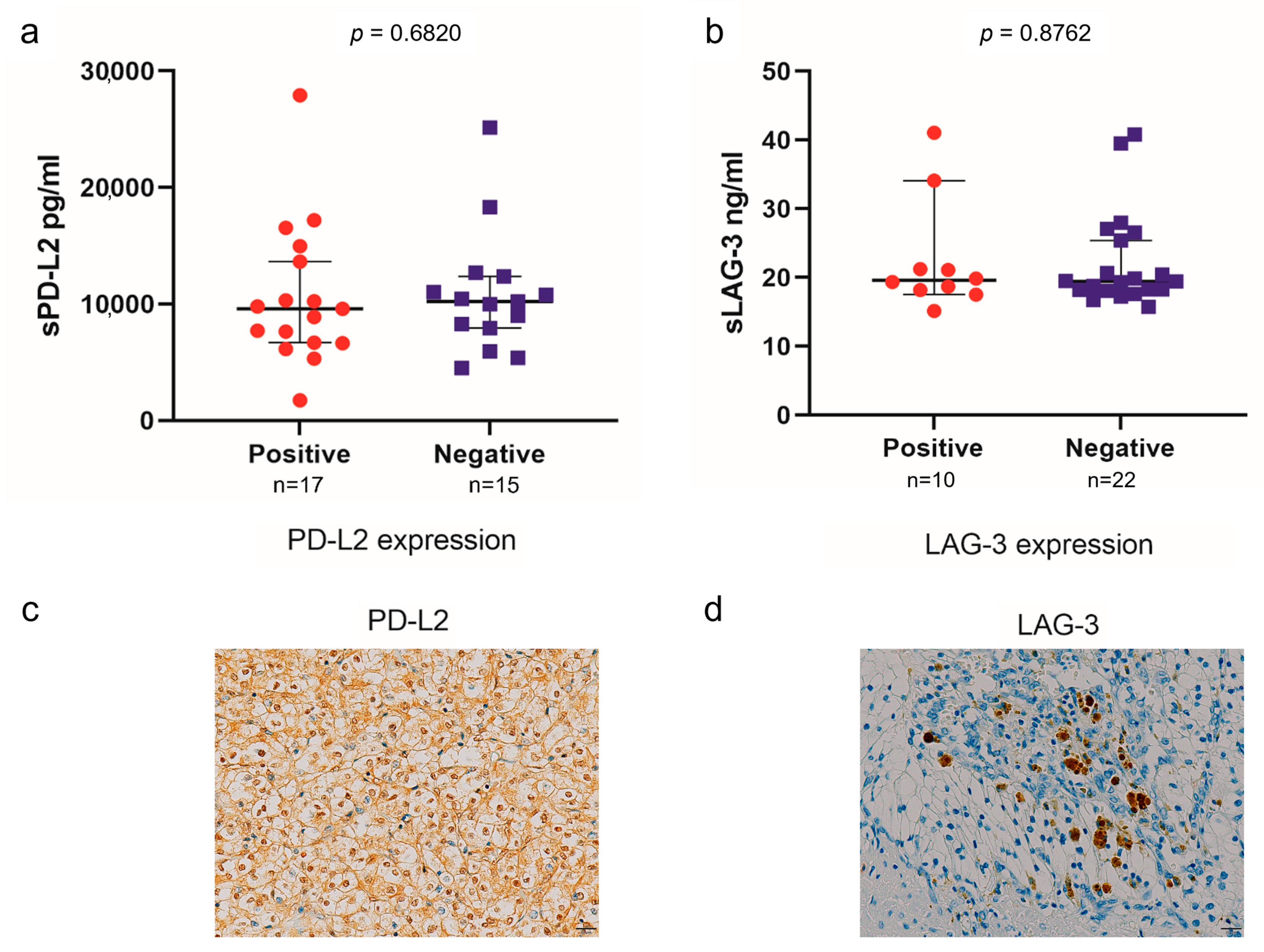
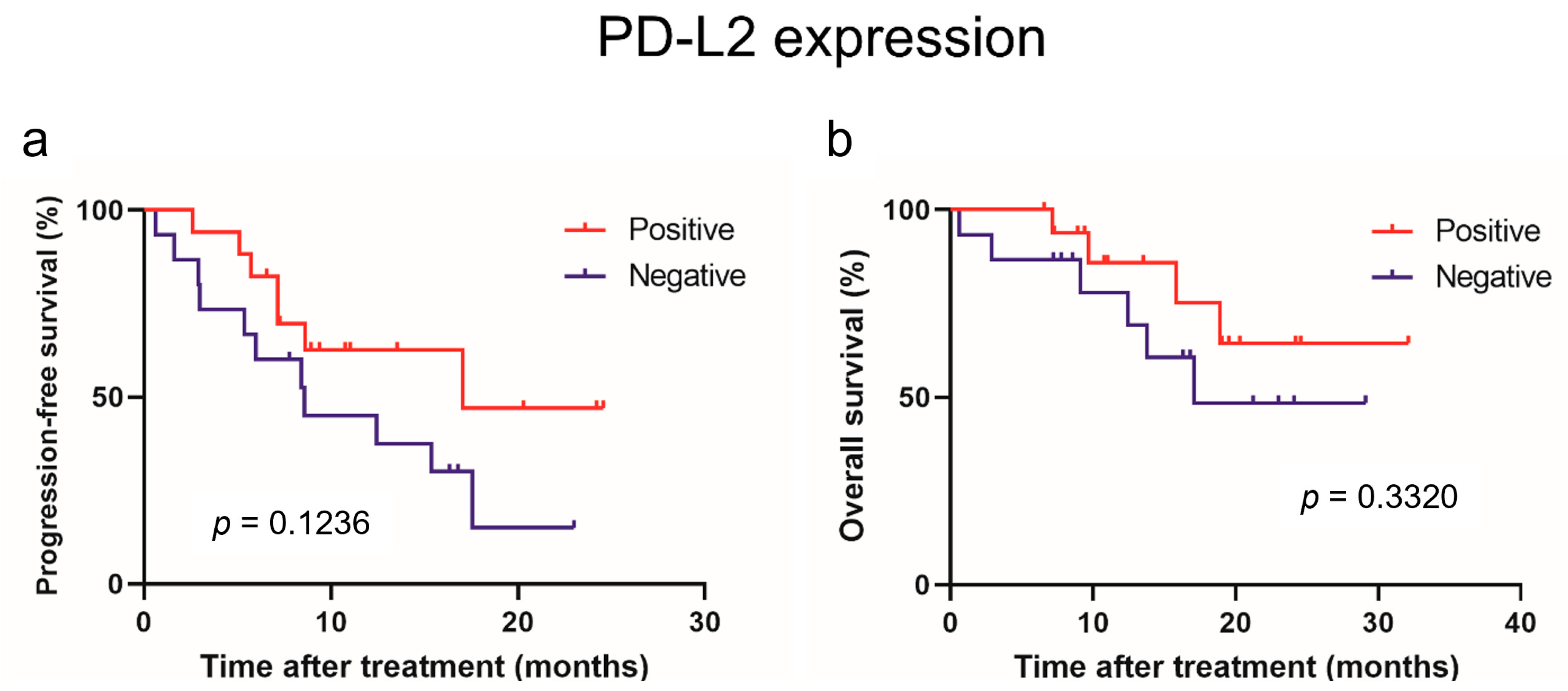
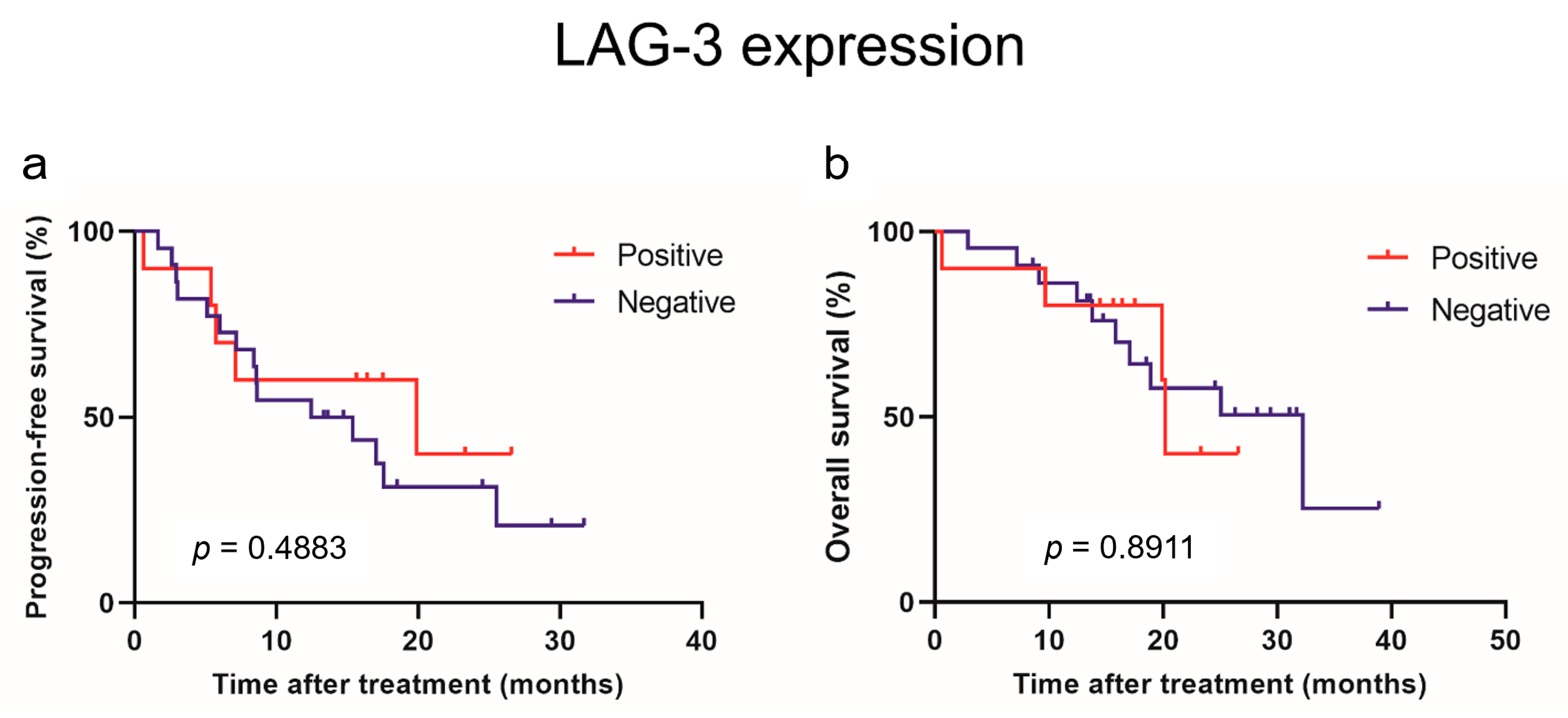
3.4. Association between Soluble Immune Checkpoint Molecule Levels and the Expression of Immune Checkpoint Molecules in Tumors
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Motzer, R.J.; Tannir, N.M.; McDermott, D.F.; Arén Frontera, O.; Melichar, B.; Choueiri, T.K.; Plimack, E.R.; Barthélémy, P.; Porta, C.; George, S.; et al. Nivolumab plus ipilimumab versus sunitinib in advanced renal-cell carcinoma. N. Engl. J. Med. 2018, 378, 1277–1290. [Google Scholar] [CrossRef] [PubMed]
- Motzer, R.J.; Penkov, K.; Haanen, J.; Rini, B.; Albiges, L.; Campbell, M.T.; Venugopal, B.; Kollmannsberger, C.; Negrier, S.; Uemura, M.; et al. Avelumab plus axitinib versus sunitinib for advanced renal-cell carcinoma. N. Engl. J. Med. 2019, 380, 1103–1115. [Google Scholar] [CrossRef] [PubMed]
- Rini, B.I.; Plimack, E.R.; Stus, V.; Gafanov, R.; Hawkins, R.; Nosov, D.; Pouliot, F.; Alekseev, B.; Soulières, D.; Melichar, B.; et al. Pembrolizumab plus axitinib versus sunitinib for advanced renal-cell carcinoma. N. Engl. J. Med. 2019, 380, 1116–1127. [Google Scholar] [CrossRef] [PubMed]
- Choueiri, T.K.; Powles, T.; Burotto, M.; Escudier, B.; Bourlon, M.T.; Zurawski, B.; Oyervides Juárez, V.M.; Hsieh, J.J.; Basso, U.; Shah, A.Y.; et al. Nivolumab plus cabozantinib versus sunitinib for advanced renal-cell carcinoma. N. Engl. J. Med. 2021, 384, 829–841. [Google Scholar] [CrossRef]
- Motzer, R.; Alekseev, B.; Rha, S.Y.; Porta, C.; Eto, M.; Powles, T.; Grünwald, V.; Hutson, T.E.; Kopyltsov, E.; Méndez-Vidal, M.J.; et al. Lenvatinib plus pembrolizumab or everolimus for advanced renal cell carcinoma. N. Engl. J. Med. 2021, 384, 1289–1300. [Google Scholar] [CrossRef] [PubMed]
- Ueda, K.; Suekane, S.; Kurose, H.; Chikui, K.; Nakiri, M.; Nishihara, K.; Matsuo, M.; Kawahara, A.; Yano, H.; Igawa, T. Prognostic value of PD-1 and PD-L1 expression in patients with metastatic clear cell renal cell carcinoma. Urol. Oncol. 2018, 36, 499.e9–499.e16. [Google Scholar] [CrossRef] [PubMed]
- Hara, T.; Miyake, H.; Fujisawa, M. Expression pattern of immune checkpoint-associated molecules in radical nephrectomy specimens as a prognosticator in patients with metastatic renal cell carcinoma treated with tyrosine kinase inhibitors. Urol. Oncol. 2017, 35, 363–369. [Google Scholar] [CrossRef] [PubMed]
- Mori, K.; Abufaraj, M.; Mostafaei, H.; Quhal, F.; Fajkovic, H.; Remzi, M.; Karakiewicz, P.I.; Egawa, S.; Schmidinger, M.; Shariat, S.F.; et al. The predictive value of programmed death ligand 1 in patients with metastatic renal cell carcinoma treated with immune-checkpoint inhibitors: A systematic review and meta-analysis. Eur. Urol. 2021, 79, 783–792. [Google Scholar] [CrossRef]
- Lee, C.H.; Jung, S.J.; Seo, W.I.; Chung, J.I.; Lee, D.S.; Jeong, D.H.; Jeon, Y.; Choi, I. Coexpression of lymphocyte-activation gene 3 and programmed death ligand-1 in tumor infiltrating immune cells predicts worse outcome in renal cell carcinoma. Int. J. Immunopathol. Pharmacol. 2022, 36, 3946320221125588. [Google Scholar] [CrossRef]
- Klümper, N.; Ralser, D.J.; Bawden, E.G.; Landsberg, J.; Zarbl, R.; Kristiansen, G.; Toma, M.; Ritter, M.; Hölzel, M.; Ellinger, J.; et al. LAG3 (LAG-3, CD223) DNA methylation correlates with LAG3 expression by tumor and immune cells, immune cell infiltration, and overall survival in clear cell renal cell carcinoma. J. Immunother. Cancer 2020, 8, e000552. [Google Scholar] [CrossRef]
- Martin, S.D.; Bhuiyan, I.; Soleimani, M.; Wang, G. Biomarkers for immune checkpoint inhibitors in renal cell carcinoma. J. Clin. Med. 2023, 12, 4987. [Google Scholar] [CrossRef]
- Shin, K.; Kim, J.; Park, S.J.; Lee, M.A.; Park, J.M.; Choi, M.G.; Kang, D.; Song, K.Y.; Lee, H.H.; Seo, H.S.; et al. Prognostic value of soluble PD-L1 and exosomal PD-L1 in advanced gastric cancer patients receiving systemic chemotherapy. Sci. Rep. 2023, 13, 6952. [Google Scholar] [CrossRef] [PubMed]
- Zhou, J.; Mahoney, K.M.; Giobbie-Hurder, A.; Zhao, F.; Lee, S.; Liao, X.; Rodig, S.; Li, J.; Wu, X.; Butterfield, L.H.; et al. Soluble PD-L1 as a biomarker in malignant melanoma treated with checkpoint blockade. Cancer Immunol. Res. 2017, 5, 480–492. [Google Scholar] [CrossRef] [PubMed]
- Zhu, X.; Lang, J. Soluble PD-1 and PD-L1: Predictive and prognostic significance in cancer. Oncotarget 2017, 8, 97671–97682. [Google Scholar] [CrossRef] [PubMed]
- Scirocchi, F.; Strigari, L.; Di Filippo, A.; Napoletano, C.; Pace, A.; Rahimi, H.; Botticelli, A.; Rughetti, A.; Nuti, M.; Zizzari, I.G. Soluble PD-L1 as a prognostic factor for immunotherapy treatment in solid tumors: Systematic review and meta-analysis. Int. J. Mol. Sci. 2022, 23, 14496. [Google Scholar] [CrossRef] [PubMed]
- Gide, T.N.; Paver, E.C.; Yaseen, Z.; Maher, N.; Adegoke, N.; Menzies, A.M.; Pires da Silva, I.; Wilmott, J.S.; Long, G.V.; Scolyer, R.A. Lag-3 expression and clinical outcomes in metastatic melanoma patients treated with combination anti-lag-3 + anti-PD-1-based immunotherapies. Oncoimmunology 2023, 12, 2261248. [Google Scholar] [CrossRef] [PubMed]
- Muraro, E.; Romanò, R.; Fanetti, G.; Vaccher, E.; Turturici, I.; Lupato, V.; La Torre, F.B.; Polesel, J.; Fratta, E.; Giacomarra, V.; et al. Tissue and circulating PD-L2: Moving from health and immune-mediated diseases to head and neck oncology. Crit. Rev. Oncol. Hematol. 2022, 175, 103707. [Google Scholar] [CrossRef]
- Chmielewska, I.; Grenda, A.; Krawczyk, P.; Frąk, M.; Kuźnar Kamińska, B.; Mitura, W.; Milanowski, J. The influence of plasma sPD-L1 concentration on the effectiveness of immunotherapy in advanced NSCLC patients. Cancer Immunol. Immunother. 2023, 72, 4169–4177. [Google Scholar] [CrossRef] [PubMed]
- Montemagno, C.; Hagege, A.; Borchiellini, D.; Thamphya, B.; Rastoin, O.; Ambrosetti, D.; Iovanna, J.; Rioux-Leclercq, N.; Porta, C.; Negrier, S.; et al. Soluble forms of PD-L1 and PD-1 as prognostic and predictive markers of sunitinib efficacy in patients with metastatic clear cell renal cell carcinoma. Oncoimmunology 2020, 9, 1846901. [Google Scholar] [CrossRef]
- Wakita, N.; Hinata, N.; Bando, Y.; Hara, T.; Terakawa, T.; Furukawa, J.; Nakano, Y.; Fujisawa, M. Prognostic value of serum soluble PD-L1 in metastatic renal cell carcinoma patients treated with nivolumab. Anticancer Res. 2023, 43, 841–847. [Google Scholar] [CrossRef]
- Shin, S.J.; Jeon, Y.K.; Cho, Y.M.; Lee, J.L.; Chung, D.H.; Park, J.Y.; Go, H. The association between PD-L1 expression and the clinical outcomes to vascular endothelial growth factor-targeted therapy in patients with metastatic clear cell renal cell carcinoma. Oncologist 2015, 20, 1253–1260. [Google Scholar] [CrossRef] [PubMed]
- Wang, Q.; Zhang, J.; Tu, H.; Liang, D.; Chang, D.W.; Ye, Y.; Wu, X. Soluble immune checkpoint-related proteins as predictors of tumor recurrence, survival, and T cell phenotypes in clear cell renal cell carcinoma patients. J. Immunother. Cancer 2019, 7, 334. [Google Scholar] [CrossRef] [PubMed]
- Costantini, A.; Julie, C.; Dumenil, C.; Hélias-Rodzewicz, Z.; Tisserand, J.; Dumoulin, J.; Giraud, V.; Labrune, S.; Chinet, T.; Emile, J.F.; et al. Predictive role of plasmatic biomarkers in advanced non-small cell lung cancer treated by nivolumab. Oncoimmunology 2018, 7, e1452581. [Google Scholar] [CrossRef] [PubMed]
- Ueda, K.; Suekane, S.; Kurose, H.; Ito, N.; Ogasawara, N.; Hiroshige, T.; Chikui, K.; Ejima, K.; Uemura, K.; Nakiri, M.; et al. Immune-related adverse events are clinical biomarkers to predict favorable outcomes in advanced renal cell carcinoma treated with nivolumab plus ipilimumab. Jpn. J. Clin. Oncol. 2022, 52, 479–485. [Google Scholar] [CrossRef] [PubMed]
- Maruhashi, T.; Sugiura, D.; Okazaki, I.M.; Okazaki, T. LAG-3: From molecular functions to clinical applications. J. Immunother. Cancer 2020, 8, e001014. [Google Scholar] [CrossRef] [PubMed]
- Anderson, A.C.; Joller, N.; Kuchroo, V.K. Lag-3, Tim-3, and TIGIT: Co-inhibitory receptors with specialized functions in immune regulation. Immunity 2016, 44, 989–1004. [Google Scholar] [CrossRef]
- He, Y.; Wang, Y.; Zhao, S.; Zhao, C.; Zhou, C.; Hirsch, F.R. sLAG-3 in non-small-cell lung cancer patients’ serum. Onco Targets Ther. 2018, 11, 4781–4784. [Google Scholar] [CrossRef]
- Li, N.; Jilisihan, B.; Wang, W.; Tang, Y.; Keyoumu, S. Soluble LAG3 acts as a potential prognostic marker of gastric cancer and its positive correlation with CD8+T cell frequency and secretion of IL-12 and INF-gamma in peripheral blood. Cancer Biomark. 2018, 23, 341–351. [Google Scholar] [CrossRef]
- Triebel, F.; Hacene, K.; Pichon, M.F. A soluble lymphocyte activation gene-3 (sLAG-3) protein as a prognostic factor in human breast cancer expressing estrogen or progesterone receptors. Cancer Lett. 2006, 235, 147–153. [Google Scholar] [CrossRef] [PubMed]
- Botticelli, A.; Zizzari, I.G.; Scagnoli, S.; Pomati, G.; Strigari, L.; Cirillo, A.; Cerbelli, B.; Di Filippo, A.; Napoletano, C.; Scirocchi, F.; et al. The role of soluble LAG3 and soluble immune checkpoints profile in advanced head and neck cancer: A pilot study. J. Pers. Med. 2021, 11, 651. [Google Scholar] [CrossRef] [PubMed]
- Pinato, D.J.; Shiner, R.J.; White, S.D.; Black, J.R.; Trivedi, P.; Stebbing, J.; Sharma, R.; Mauri, F.A. Intra-tumoral heterogeneity in the expression of programmed-death (PD) ligands in isogeneic primary and metastatic lung cancer: Implications for immunotherapy. Oncoimmunology 2016, 5, e1213934. [Google Scholar] [CrossRef] [PubMed]
- Casadevall, D.; Clavé, S.; Taus, Á.; Hardy-Werbin, M.; Rocha, P.; Lorenzo, M.; Menéndez, S.; Salido, M.; Albanell, J.; Pijuan, L.; et al. Heterogeneity of tumor and immune cell PD-L1 expression and lymphocyte counts in surgical NSCLC samples. Clin. Lung Cancer 2017, 18, 682–691.e5. [Google Scholar] [CrossRef] [PubMed]
- Teramoto, K.; Igarashi, T.; Kataoka, Y.; Ishida, M.; Hanaoka, J.; Sumimoto, H.; Daigo, Y. Prognostic impact of soluble PD-L1 derived from tumor-associated macrophages in non-small-cell lung cancer. Cancer Immunol. Immunother. 2023, 72, 3755–3764. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | All (n = 42) | |
|---|---|---|
| Age (years, range) | 69.5 (42–80) | |
| Sex, n (%) | Male | 34 (81.0) |
| Female | 8 (19.0) | |
| Histopathology, n (%) | Clear cell RCC | 34 (81.0) |
| Non-clear cell RCC | 5 (11.9) | |
| Unknown | 3 (7.1) | |
| Performance status, n (%) | 0, 1 | 39 (92.9) |
| ≥2 | 3 (7.1) | |
| Prior nephrectomy, n (%) | Presence | 19 (45.2) |
| Absence | 23 (54.8) | |
| IMDC risk classification, n (%) | Favorable | 6 (14.3) |
| Intermediate | 24 (57.1) | |
| Poor | 12 (28.6) | |
| First line treatment, n (%) | Nivolumab plus ipilimumab | 26 (61.9) |
| Axitinib plus avelumab | 13 (31.0) | |
| Lenvatinib plus pembrolizumab | 3 (7.1) | |
| sPD-1, pg/mL, median (range) | 291.3 (149.4–1649.9) | |
| sPD-L1, pg/mL, median (range) | 39.8 (8.0–395.8) | |
| sPD-L2, pg/mL, median (range) | 9291.6 (1726.1–27,900.8) | |
| sLAG-3, ng/mL, median (range) | 19.4 (15.2–41.1) | |
| CRP, mg/dl, median (range) | 0.71 (0.04–18.58) | |
| NLR, median (range) | 3.28 (1.44–12.04) |
| Progression-Free Survival (n = 42) | ||||
|---|---|---|---|---|
| Univariate Analysis | Multivariate Analysis | |||
| Variable | HR | p-Value | HR | p-Value |
| Age (≥70 years) | 0.577 (0.252–1.322) | 0.1936 | ||
| Sex (female) | 1.241 (0.460–3.347) | 0.6699 | ||
| Prior nephrectomy (no) | 2.659 (1.102–6.412) | 0.0295 | 2.337 (0.922–5.926) | 0.0737 |
| Performance status (≥2) | 0.514 (0.069–3.837) | 0.5166 | ||
| IMDC risk classification (intermediate) | 1.291 (0.370–4.510) | 0.6886 | ||
| (poor) | 1.602 (0.411–6.250) | 0.4975 | ||
| Histology (Non-CCRCC) | 0.894 (0.264–3.026) | 0.8564 | ||
| CRP (mg/dL) (≥median) | 1.802 (0.789–4.113) | 0.1620 | ||
| NLR (≥median) | 0.838 (0.375–1.874) | 0.6676 | ||
| sPD-1 (≥median) | 1.229 (0.551–2.741) | 0.6148 | ||
| sPD-L1 (≥median) | 1.046 (0.463–2.361) | 0.9136 | ||
| sPD-L2 (≥median) | 3.455 (1.463–8.158) | 0.0047 | 2.918 (1.201–7.085) | 0.0180 |
| sLAG-3 (≥median) | 0.270 (0.108–0.675) | 0.0051 | 0.387 (0.154–0.974) | 0.0438 |
| Overall Survival (n = 42) | ||||
|---|---|---|---|---|
| Univariate Analysis | Multivariate Analysis | |||
| Variable | HR | p-Value | HR | p-Value |
| Age (≥70 years) | 0.375 (0.117–1.196) | 0.0974 | ||
| Sex (female) | 1.093 (0.302–3.958) | 0.8920 | ||
| Prior nephrectomy (no) | 3.768 (1.049–13.533) | 0.0420 | 3.544 (0.982–12.788) | 0.0532 |
| Performance status (≥2) | 0.855 (0.111–6.614) | 0.8807 | ||
| IMDC risk classification (intermediate) | 1.952 (0.240–15.878) | 0.5319 | ||
| (poor) | 4.450 (0.529–37.446) | 0.1695 | ||
| Histology (non-CCRCC) | 0.727 (0.094–5.616) | 0.7601 | ||
| CRP (mg/dL) (≥median) | 3.036 (0.947–9.729) | 0.0617 | ||
| NLR (≥median) | 0.864 (0.299–2.494) | 0.7869 | ||
| sPD-1 (≥median) | 1.102 (0.386–3.148) | 0.8561 | ||
| sPD-L1 (≥median) | 2.330 (0.745–7.290) | 0.1460 | ||
| sPD-L2 (≥median) | 3.241 (1.012–10.375) | 0.0477 | 3.040 (0.944–9.793) | 0.0625 |
| sLAG-3 (≥median) | 0.635 (0.218–1.855) | 0.4068 | ||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ueda, K.; Uemura, K.; Ito, N.; Sakai, Y.; Ohnishi, S.; Suekane, H.; Kurose, H.; Hiroshige, T.; Chikui, K.; Nishihara, K.; et al. Soluble Immune Checkpoint Molecules as Predictors of Efficacy in Immuno-Oncology Combination Therapy in Advanced Renal Cell Carcinoma. Curr. Oncol. 2024, 31, 1701-1712. https://doi.org/10.3390/curroncol31040129
Ueda K, Uemura K, Ito N, Sakai Y, Ohnishi S, Suekane H, Kurose H, Hiroshige T, Chikui K, Nishihara K, et al. Soluble Immune Checkpoint Molecules as Predictors of Efficacy in Immuno-Oncology Combination Therapy in Advanced Renal Cell Carcinoma. Current Oncology. 2024; 31(4):1701-1712. https://doi.org/10.3390/curroncol31040129
Chicago/Turabian StyleUeda, Kosuke, Keiichiro Uemura, Naoki Ito, Yuya Sakai, Satoshi Ohnishi, Hiroki Suekane, Hirofumi Kurose, Tasuku Hiroshige, Katsuaki Chikui, Kiyoaki Nishihara, and et al. 2024. "Soluble Immune Checkpoint Molecules as Predictors of Efficacy in Immuno-Oncology Combination Therapy in Advanced Renal Cell Carcinoma" Current Oncology 31, no. 4: 1701-1712. https://doi.org/10.3390/curroncol31040129