Nomogram Based on Liver Function Test Indicators for Survival Prediction in Nasopharyngeal Carcinoma Patients Receiving PD-1 Inhibitor Therapy


Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population and Study Design
2.2. Statistical Analysis
3. Results
3.1. Patient Characteristics
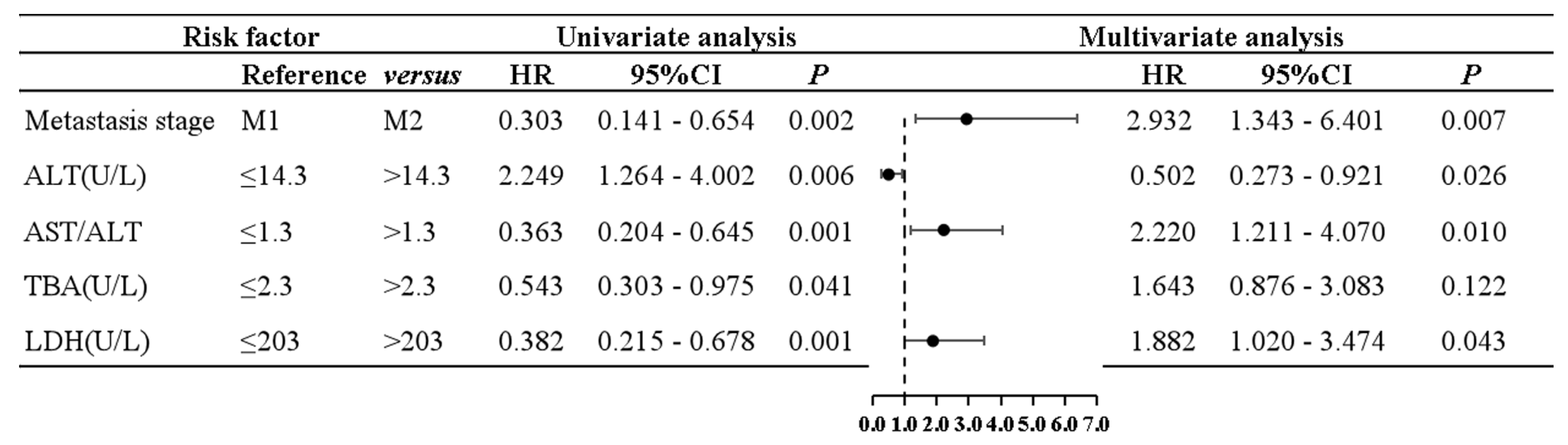
3.2. Univariate and Multivariate Cox Proportional Hazard Regression Analysis for PFS
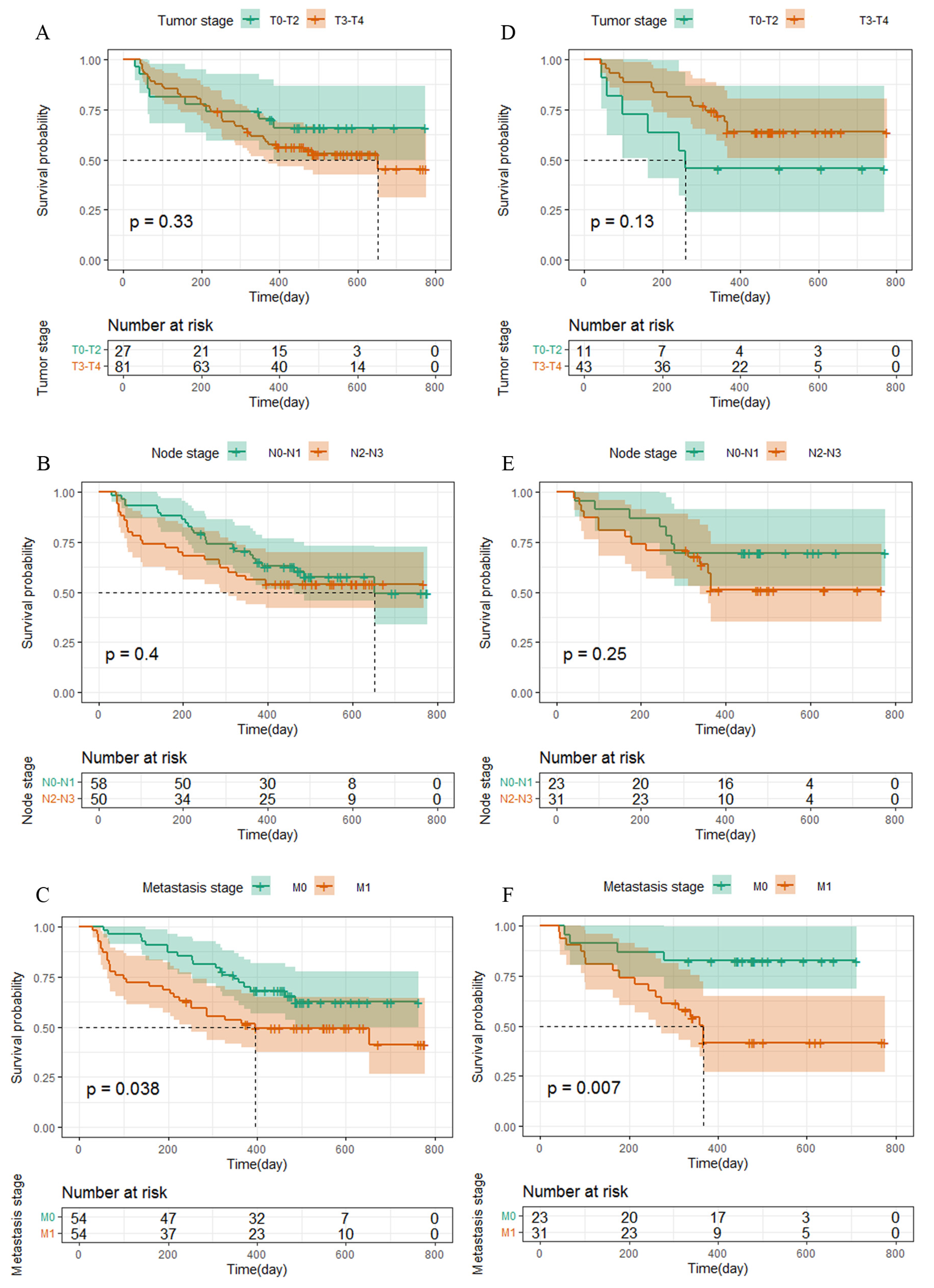
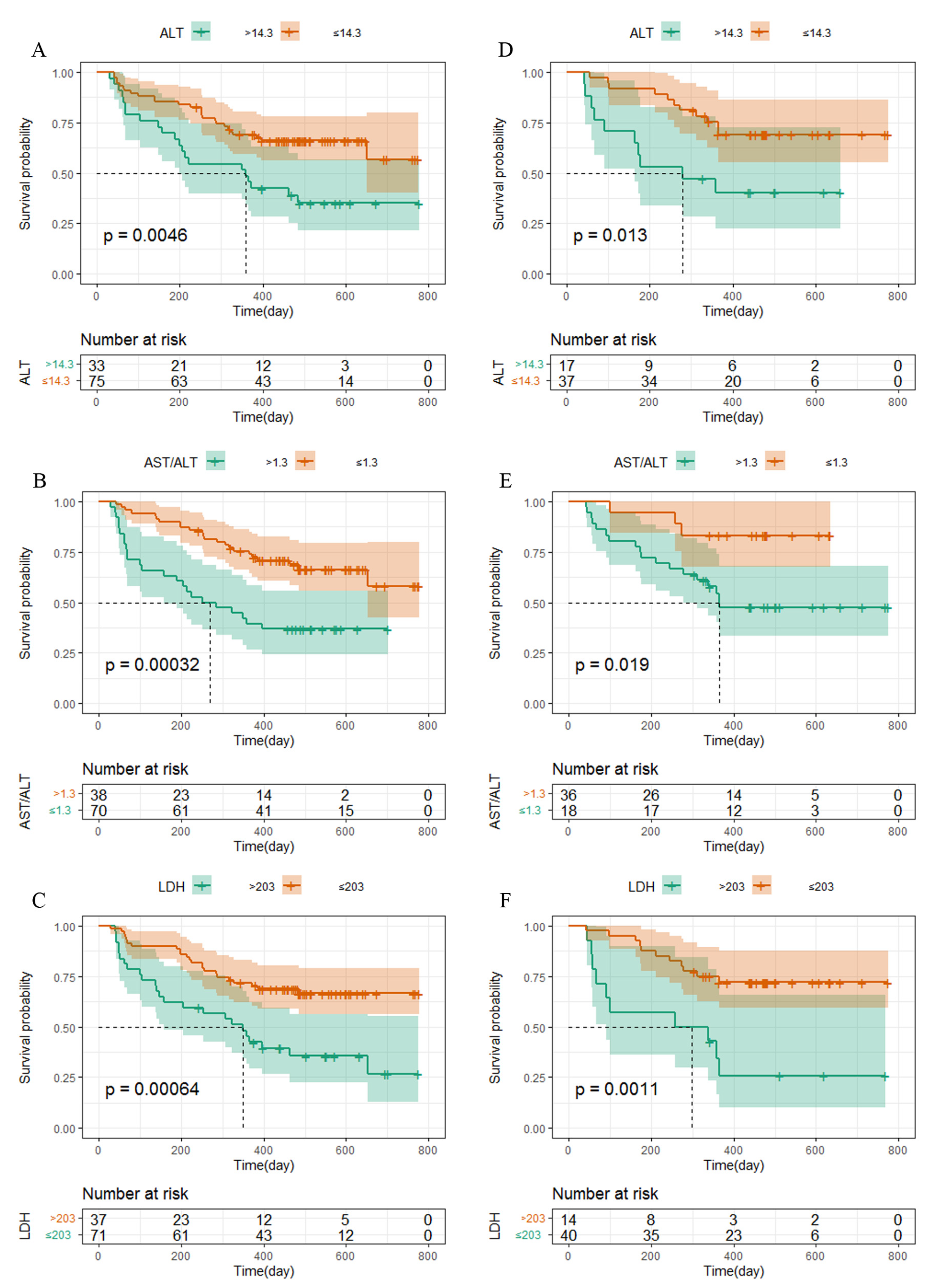
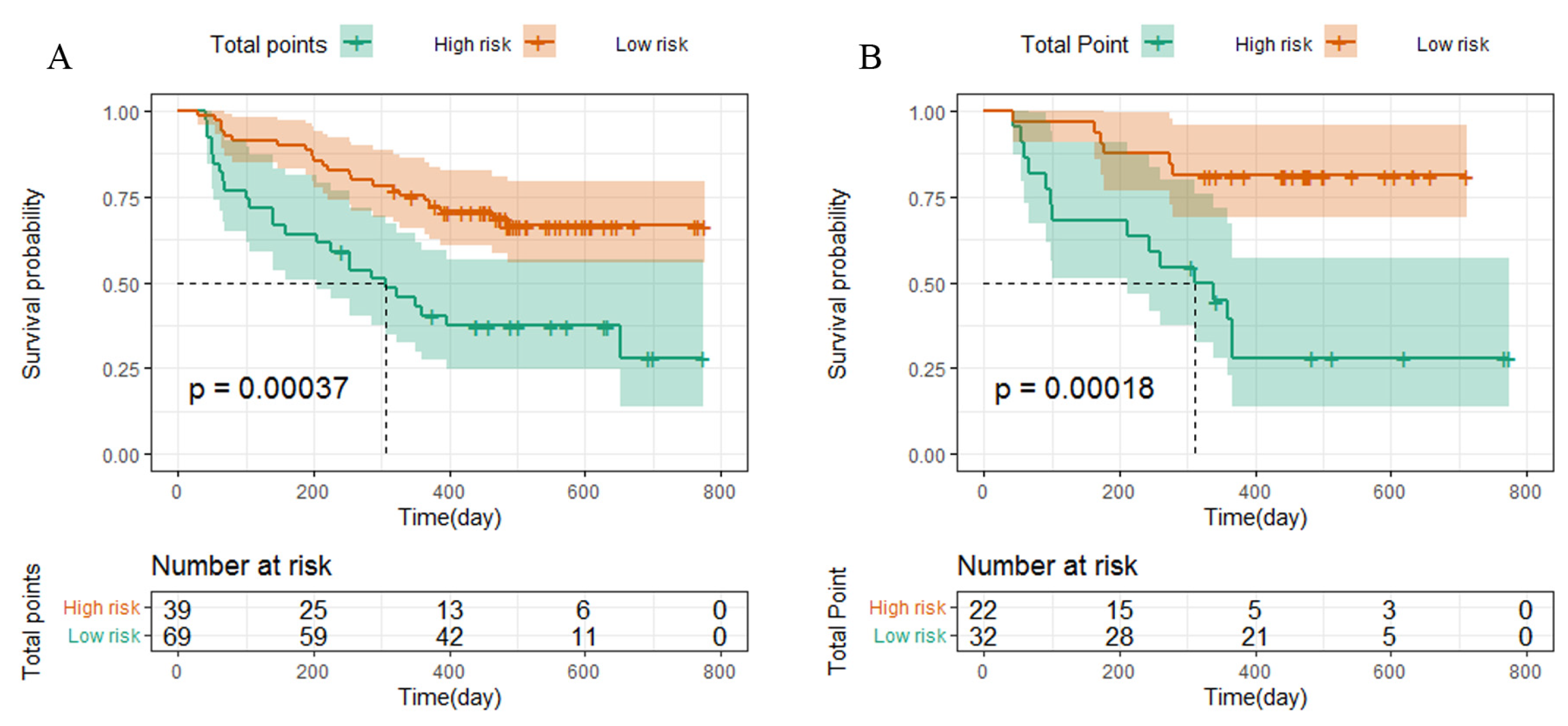
3.3. Survival Analysis
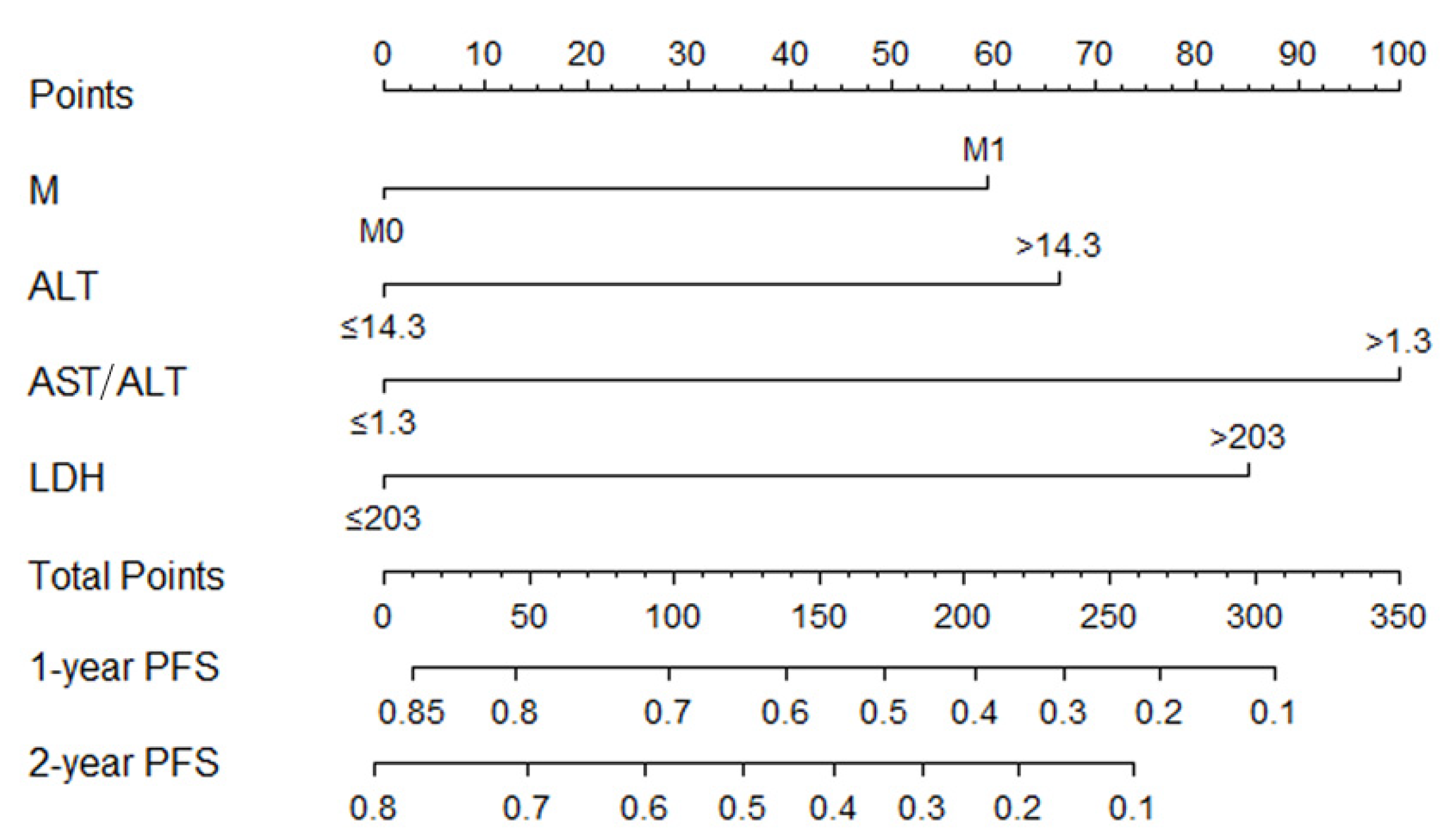
3.4. Constructing Nomogram
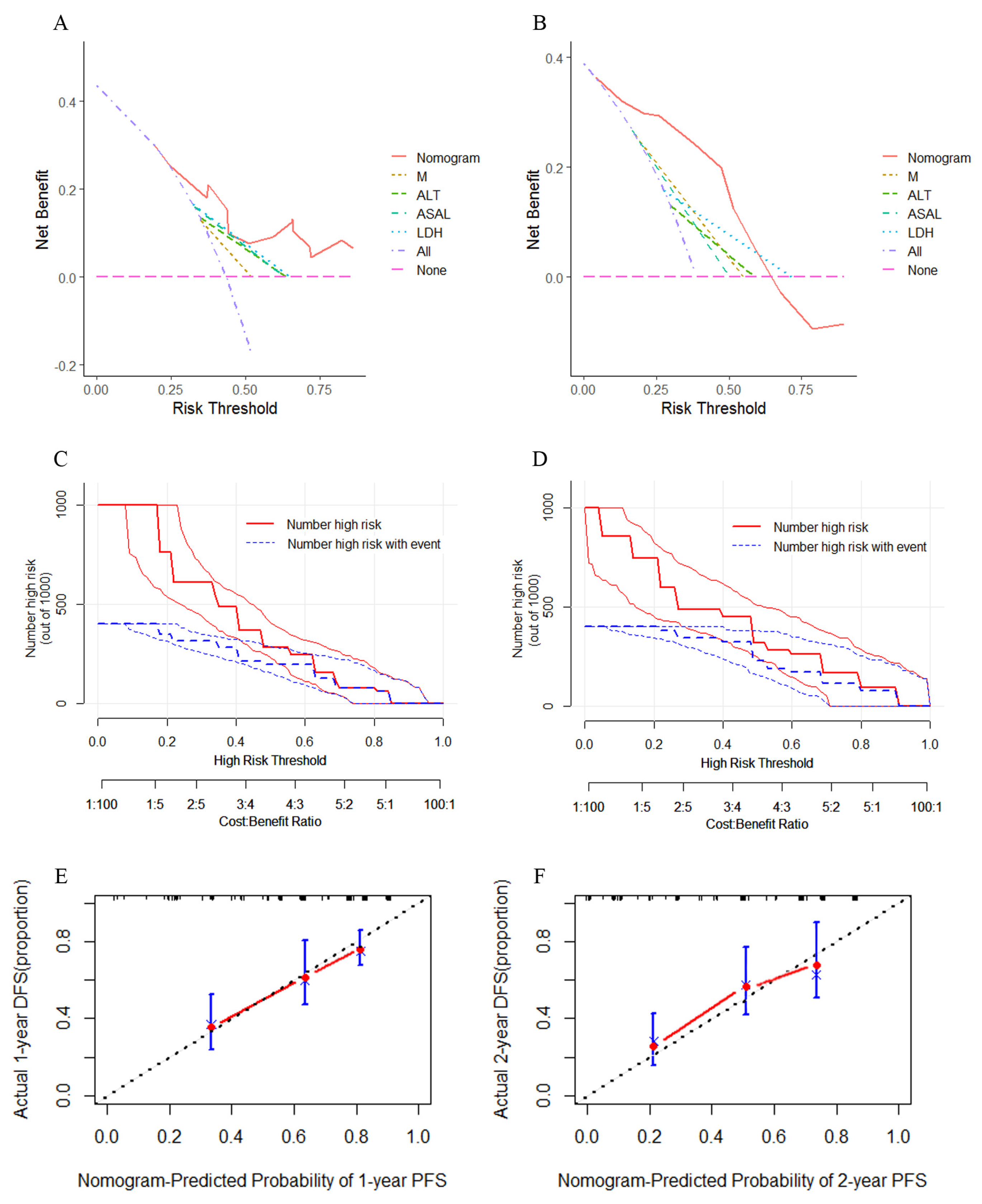
3.5. Nomogram Accuracy and Calibration
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Tang, L.L.; Chen, W.Q.; Xue, W.Q.; He, Y.Q.; Zheng, R.S.; Zeng, Y.X.; Jia, W.H. Global trends in incidence and mortality of nasopharyngeal carcinoma. Cancer Lett. 2016, 374, 22–30. [Google Scholar] [CrossRef] [PubMed]
- Torre, L.A.; Bray, F.; Siegel, R.L.; Ferlay, J.; Lortet-Tieulent, J.; Jemal, A. Global cancer statistics, 2012. CA Cancer J. Clin. 2015, 65, 87–108. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Huang, T.; Su, N.; Zhang, X.; Ma, S.; Zhong, G.; Tian, X.; Chen, Q.; Tang, L.; Lu, L.; Fang, Y.; et al. Systemic chemotherapy and sequential locoregional radiotherapy in initially metastatic nasopharyngeal carcinoma: Retrospective analysis with 821 cases. Head Neck 2020, 42, 1970–1980. [Google Scholar] [CrossRef] [PubMed]
- Lu, T.; Chen, Y.; Li, J.; Guo, Q.; Lin, W.; Zheng, Y.; Su, Y.; Zong, J.; Lin, S.; Ye, Y.; et al. High soluble programmed death-ligand 1predicts poor prognosis in patients with nasopharyngeal carcinoma. Oncol. Targets Ther. 2020, 13, 1757–1765. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhang, L.; Chen, Q.Y.; Liu, H.; Tang, L.Q.; Mai, H.Q. Emerging treatment options for nasopharyngeal carcinoma. Drug. Des. Dev. Ther. 2013, 7, 37–52. [Google Scholar]
- Wang, F.H.; Wei, X.L.; Feng, J.; Li, Q.; Xu, N.; Hu, X.C.; Liao, W.; Jiang, Y.; Lin, X.Y.; Zhang, Q.Y.; et al. Efficacy, Safety, and Correlative Biomarkers of Toripalimab in Previously Treated Recurrent or Metastatic Nasopharyngeal Carcinoma: A Phase II Clinical Trial (POLARIS-02). J. Clin. Oncol. 2021, 39, 704–712. [Google Scholar] [CrossRef]
- Gong, J.; Le, T.Q.; Massarelli, E.; Hendifar, A.E.; Richard, T. Radiation therapy and PD⁃1/PD⁃L1 blockade: The clinical development of an evolving anticancer combination. J. Immunother. Cancer 2018, 6, 46. [Google Scholar] [CrossRef]
- Disibio, G.; French, S.W. Metastatic patterns of cancers: Results from a large autopsy study. Arch. Pathol. Lab. Med. 2008, 132, 931–939. [Google Scholar] [CrossRef]
- Li, F.; Tian, Z. The liver works as a school to educate regulatory immune cells. Cell. Mol. Immunol. 2013, 10, 292–302. [Google Scholar] [CrossRef] [Green Version]
- Tumeh, P.C.; Hellmann, M.D.; Hamid, O.; Tsai, K.K.; Loo, K.L.; Gubens, M.A.; Rosenblum, M.; Harview, C.L.; Taube, J.M.; Handley, N.; et al. Liver Metastasis and Treatment Outcome with Anti-PD-1 Monoclonal Antibody in Patients with Melanoma and NSCLC. Cancer Immunol. Res. 2017, 5, 417–424. [Google Scholar] [CrossRef] [Green Version]
- Topalian, S.L.; Hodi, F.S.; Brahmer, J.R.; Gettinger, S.N.; Smith, D.C.; McDermott, D.F.; Powderly, J.D.; Sosman, J.A.; Atkins, M.B.; Leming, P.D.; et al. Five-Year Survival and Correlates Among Patients With Advanced Melanoma, Renal Cell Carcinoma, or Non-Small Cell Lung Cancer Treated With Nivolumab. JAMA Oncol. 2019, 5, 1411–1420. [Google Scholar] [CrossRef] [Green Version]
- Sasaki, A.; Nakamura, Y.; Mishima, S.; Kawazoe, A.; Kuboki, Y.; Bando, H.; Kojima, T.; Doi, T.; Ohtsu, A.; Yoshino, T.; et al. Predictive factors for hyperprogressive disease during nivolumab as anti-PD1 treatment in patients with advanced gastric cancer. Gastric Cancer 2019, 22, 793–802. [Google Scholar] [CrossRef] [Green Version]
- Bilen, M.A.; Shabto, J.M.; Martini, D.J.; Liu, Y.; Lewis, C.; Collins, H.; Akce, M.; Kissick, H.; Carthon, B.C.; Shaib, W.; et al. Sites of metastasis and association with clinical outcome (CO) in advanced stage cancer patients (pts) treated with immunotherapy (IO). BMC Cancer 2019, 19, 857. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schmid, S.; Diem, S.; Li, Q.; Krapf, M.; Flatz, L.; Leschka, S.; Desbiolles, L.; Klingbiel, D.; Jochum, W.; Früh, M. Organ-specific response to nivolumab in patients with non-small cell lung cancer (NSCLC). Cancer Immunol. Immunother. 2018, 67, 1825–1832. [Google Scholar] [CrossRef]
- Pires da Silva, I.; Lo, S.; Quek, C.; Gonzalez, M.; Carlino, M.S.; Long, G.V.; Menzies, A.M. Site-specific response patterns, pseudoprogression, and acquired resistance in patients with melanoma treated with ipilimumab combined with anti-PD-1 therapy. Cancer 2020, 126, 86–97. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Halabi, S.; Kelly, W.K.; Ma, H.; Zhou, H.; Solomon, N.C.; Fizazi, K.; Tangen, C.M.; Rosenthal, M.; Petrylak, D.P.; Hussain, M.; et al. Meta-analysis evaluating the impact of site of metastasis on overall survival in men with castration-resistant prostate cancer. J. Clin. Oncol. 2016, 34, 1652–1659. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Budczies, J.; Winterfeld, M.; Klauschen, F.; Bockmayr, M.; Lennerz, J.; Denkert, C.; Wolf, T.; Warth, A.; Dietel, M.; Anagnostopoulos, I.; et al. The landscape of metastatic progression patterns across major human cancers. Oncotarget 2014, 6, 570–583. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Iasonos, A.; Schrag, D.; Raj, G.V.; Panageas, K.S. How to build and interpret a nomogram for cancer prognosis. J. Clin. Oncol. 2008, 26, 1364–1370. [Google Scholar] [CrossRef] [PubMed]
- Bendifallah, S.; Ballester, M.; Uzan, C.; Fauvet, R.; Morice, P.; Darai, E. Nomogram to predict recurrence in patients with early-and advanced-stage mucinous and serous borderline ovarian tumors. Am. J. Obstet. Gynecol. 2014, 211, e1–e6. [Google Scholar] [CrossRef]
- Tang, L.Q.; Li, C.F.; Li, J.; Chen, W.H.; Chen, Q.Y.; Yuan, L.X.; Lai, X.P.; He, Y.; Xu, Y.X.X.; Hu, D.P.; et al. Establishment and validation of prognostic nomograms for endemic nasopharyngeal carcinoma. J. Natl. Cancer Inst. 2015, 108, djv291. [Google Scholar] [CrossRef] [Green Version]
- Liang, W.; Zhang, L.; Jiang, G.; Wang, Q.; Liu, L.; Liu, D.; Wang, W.; Zhu, Z.; Deng, Q.; Xiong, X.; et al. Development and validation of a nomogram for predicting survival in patients with resected non-small-cell lung cancer. J. Clin. Oncol. 2015, 33, 861–869. [Google Scholar] [CrossRef] [Green Version]
- Lin, C.; Sun, X.S.; Liu, S.L.; Li, X.Y.; Lu, N.; Li, X.L.; Tang, L.Q.; Guo, L. Establishment and Validation of a Nomogram for Nasopharyngeal Carcinoma Patients Concerning the Prognostic Effect of Parotid Lymph Node Metastases. Cancer Res. Treat. 2020, 52, 855–866. [Google Scholar] [CrossRef]
- Zhang, L.L.; Xu, F.; He, W.T.; Huang, M.Y.; Song, D.; Li, Y.Y.; Deng, Q.L.; Huang, Y.S.; Wang, T.; Shao, J.Y. Development and validation of a prognostic nomogram for the pre-treatment prediction of early metachronous metastasis in endemic nasopharyngeal carcinoma: A bigdata intelligence platform-based analysis. Adv. Med. Oncol. 2020, 12, 1758835920978132. [Google Scholar] [CrossRef]
- Lai, C.; Zhang, C.; Lv, H.; Huang, H.; Ke, X.; Zhou, C.; Chen, H.; Chen, S.; Zhou, L. A novel prognostic model predicts overall survival in patients with nasopharyngeal carcinoma based on clinical features and blood biomarkers. Cancer Med. 2021, 10, 3511–3523. [Google Scholar] [CrossRef]
- Mao, Y.P.; Tang, L.L.; Chen, L.; Sun, Y.; Qi, Z.Y.; Zhou, G.Q.; Liu, L.Z.; Li, L.; Lin, A.H.; Ma, J. Prognostic factors and failure patterns in non-metastatic nasopharyngeal carcinoma after intensity modulated radiotherapy. Chin. J. Cancer 2016, 35, 103. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rahmioglu, N.; Andrew, T.; Cherkas, L.; Surdulescu, G.; Swaminathan, R.; Spector, T.; Ahmadi, K.R. Epidemiology and Genetic Epidemiology of the Liver Function Test Proteins. PLoS ONE 2009, 4, e4435. [Google Scholar] [CrossRef] [Green Version]
- Chen, S.-L.; Xue, N.; Wu, M.-T.; Chen, H.; He, X.; Li, J.-P.; Liu, W.L.; Dai, S.Q. Influence of Preoperative Serum Aspartate Aminotransferase (AST) Level on the Prognosis of Patients with Non-Small Cell Lung Cancer. Int. J. Mol. Sci. 2016, 17, 1474. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bezan, A.; Mrsic, E.; Krieger, D.; Stojakovic, T.; Pummer, K.; Zigeuner, R.; Hutterer, G.C.; Pichler, M. The Preoperative AST/ALT (De Ritis) Ratio Represents a Poor Prognostic Factor in a Cohort of Patients with Nonmetastatic Renal Cell Carcinoma. J. Urol. 2015, 194, 30–35. [Google Scholar] [CrossRef]
- Shen, S.L.; Fu, S.J.; Chen, B.; Kuang, M.; Li, S.Q.; Hua, Y.P.; Liang, L.J.; Guo, P.; Hao, Y.; Peng, B.G. Preoperative aspartate aminotransferase to platelet ratio is an independent prognostic factor for hepatitis B-induced hepatocellular carcinoma after hepatic resection. Ann. Surg. Oncol. 2014, 21, 3802–3809. [Google Scholar] [CrossRef]
- Huang, H.; Wang, X.P.; Li, X.H.; Chen, H.; Zheng, X.; Lin, J.H.; Kang, T.; Zhang, L.; Chen, P.S. Prognostic value of pretreatment serum alanine aminotransferase/aspartate aminotransferase (ALT/AST) ratio and gamma glutamyltransferase (GGT) in patients with esophageal squamous cell carcinoma. BMC Cancer 2017, 17, 544. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liu, X.; Meng, Q.H.; Ye, Y.; Hildebrandt, M.A.T.; Gu, J.; Wu, X. Prognostic significance of pretreatment serum levels of albumin, LDH and total bilirubin in patients with non-metastatic breast cancer. Carcinogenesis 2015, 36, 243–248. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stocken, D.D.; Hassan, A.B.; Altman, D.G.; Billingham, L.J.; Bramhall, S.R.; Johnson, P.J.; Freemantle, N. Modelling prognostic factors in advanced pancreatic cancer. Br. J. Cancer 2008, 99, 883–893. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shen, J.; Dai, J.; Zhang, Y.; Xie, F.; Yu, Y.; Li, C.; Wen, T. Baseline HBV-DNA load plus AST/ALT ratio predicts prognosis of HBV- related hepatocellular carcinoma after hepatectomy: A multicentre study. J. Viral Hepat. 2021, 28, 1587–1596. [Google Scholar] [CrossRef] [PubMed]
- Augoff, K.; Hryniewicz-Jankowska, A.; Tabola, R. Lactate dehydrogenase 5: An old friend and a new hope in the war on cancer. Cancer Lett. 2015, 358, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Wan, X.B.; Wei, L.; Li, H.; Dong, M.; Lin, Q.; Ma, X.K.; Huang, P.Y.; Wen, J.Y.; Li, X.; Chen, J.; et al. High pretreatment serum lactate dehydrogenase level correlates with disease relapse and predicts an inferior outcome in locally advanced nasopharyngeal carcinoma. Eur. J. Cancer 2013, 49, 2356–2364. [Google Scholar] [CrossRef]
- Jin, Y.; Ye, X.; Shao, L.; Lin, B.; He, C.; Zhang, B.; Zhang, Y. Serum lactic dehydrogenase strongly predicts survival in metastatic nasopharyngeal carcinoma treated with palliative chemotherapy. Eur. J. Cancer 2013, 49, 1619–1626. [Google Scholar] [CrossRef]
- Freedman, A.; Jacobsen, E. Follicular lymphoma: 2020 update on diagnosis and management. Am. J. Hematol. 2020, 95, 316–327. [Google Scholar] [CrossRef] [Green Version]
- De Martin, E.; Michot, J.M.; Papouin, B.; Champiat, S.; Mateus, C.; Lambotte, O.; Roche, B.; Antonini, T.M.; Coilly, A.; Laghouati, S.; et al. Characterization of liver injury induced by cancer immunotherapy using immune checkpoint inhibitors. J. Hepatol. 2018, 68, 1181–1190. [Google Scholar] [CrossRef]
- Huffman, B.M.; Kottschade, L.A.; Kamath, P.S.; Markovic, S.N. Hepatotoxicity after immune checkpoint inhibitor therapy in melanoma: Natural progression and management. Am. J. Clin. Oncol. 2017, 41, 760–765. [Google Scholar] [CrossRef]
- Remash, D.; Prince, D.S.; McKenzie, C.; Strasser, S.I.; Kao, S.; Liu, K. Immune checkpoint inhibitor-related hepatotoxicity: A review. World J. Gastroenterol. 2021, 27, 5376–5391. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | Total Cohort N (%) | Training Cohort N (%) | Validation Cohort N (%) |
|---|---|---|---|
| Gender | |||
| Male | 115 (71.0) | 79 (73.1) | 36 (66.7) |
| Female | 47 (29.0) | 29 (26.9) | 18 (33.3) |
| Age (years) | |||
| ≤41 | 60 (37.0) | 41 (38.0) | 19 (35.2) |
| >41 | 102 (63.0) | 67 (62.0) | 35 (64.8) |
| BMI | |||
| ≤22.3 | 84 (51.9) | 56 (51.9) | 28 (51.9) |
| >22.3 | 78 (48.1) | 52 (48.1) | 26 (48.1) |
| Smoking history | |||
| Non-smoker | 121 (74.7) | 80 (74.1) | 41 (75.9) |
| Current or former smoker | 41 (25.3) | 28 (25.9) | 13 (24.1) |
| Drinking history | |||
| Non-drinker | 143 (88.3) | 98 (90.7) | 45 (83.3) |
| Current or former drinker | 19 (11.7) | 10 (9.3) | 9 (16.7) |
| Histological differentiation | |||
| Undifferentiated | 153 (94.4) | 100 (92.6) | 53 (98.1) |
| Poorly differentiated | 9 (5.6) | 8 (7.4) | 1 (1.9) |
| Clinical stages | |||
| II | 11 (6.8) | 9 (8.3) | 2 (3.7) |
| III | 46 (28.4) | 36 (33.3) | 10 (18.5) |
| IV | 105 (64.8) | 63 (58.4) | 42 (77.8) |
| Tumor stage | |||
| T0–T2 | 38 (23.5) | 27 (25.0) | 11 (20.4) |
| T3–T4 | 124 (76.5) | 81 (75.0) | 43 (79.6) |
| Node stage | |||
| N0–N1 | 70 (43.2) | 47 (43.5) | 23 (42.6) |
| N2–N3 | 92 (56.8) | 61 (56.5) | 31 (57.4) |
| Metastasis stage | |||
| M0 | 77 (47.5) | 54 (50.0) | 23 (42.6) |
| M1 | 85 (52.5) | 54 (50.0) | 31 (57.4) |
| Distant metastasis (One or multiple) | |||
| Distant lymph nodes | 63 (38.9) | 46 (42.6) | 17 (31.5) |
| Liver | 26 (16.1) | 17 (15.7) | 9 (16.7) |
| Lung | 36 (22.2) | 21 (19.4) | 15 (2.8) |
| Bone | 45 (27.8) | 28 (25.9) | 17 (31.5) |
| Previous chemotherapy | |||
| Radiotherapy | 14 (8.6) | 10 (9.2) | 4 (7.5) |
| Chemotherapy | 73 (45.1) | 49 (45.4) | 24 (44.4) |
| Chemoradiotherpy | 75 (46.3) | 49 (45.4) | 26 (48.1) |
| Recurrence | |||
| Yes | 74 (45.7) | 40 (37.0) | 34 (62.9) |
| No | 88 (54.3) | 68 (63.0) | 20 (37.1) |
| Outcomes | |||
| CR | 1 (0.6) | 1 (0.9) | 0 |
| PR | 52 (32.1) | 45 (41.7) | 7 (13.0) |
| SD | 35 (21.6) | 9 (8.3) | 26 (48.1) |
| PD | 74 (45.7) | 53 (49.1) | 21 (38.9) |
| PD-1 Blockade | |||
| Camrelizumab | 18 (11.1) | 10 (9.3) | 8 (14.8) |
| Toripalimab | 119 (73.5) | 81 (75.0) | 38 (70.4) |
| Pembrolizumb | 3 (1.9) | 3 (2.8) | 0 |
| Sintilimab | 22 (13.5) | 14 (12.9) | 8 (14.8) |
| Factor | Training Cohort | Validation Cohort | ||
|---|---|---|---|---|
| C-Index (95%CI) | p | C-Index (95%CI) | p | |
| Nomogram | 0.732 (0.540–0.924) | 0.847 (0.545–1.049) | ||
| M | 0.585 (0.397–0.773) | 0.693 (0.455–0.930) | ||
| ALT | 0.625 (0.451–0.799) | 0.632 (0.377–0.887) | ||
| AST/ALT | 0.641 (0.463–0.819) | 0.656 (0.428–0.883) | ||
| LDH | 0.649 (0.473–0.825) | 0.677 (0.436–0.918) | ||
| TNM stage | 0.617 (0.411–0.823) | 0.727 (0.462–0.992) | ||
| Nomogram vs. M | 0.046 | 0.002 | ||
| Nomogram vs. ALT | 0.005 | 0.043 | ||
| Nomogram vs. AST/ALT | 0.002 | 0.007 | ||
| Nomogram vs. LDH | <0.001 | 0.004 | ||
| Nomogram vs. TNM stage | 0.026 | <0.001 | ||
| Factor | Training Cohort | Validation Cohort | ||||
|---|---|---|---|---|---|---|
| NRI% | IDI% | p | NRI% | IDI% | p | |
| Nomogram vs. M | 22.3 | 17.6 | <0.001 | 33.5 | 14.1 | <0.001 |
| Nomogram vs. ALT | 27.7 | 16.5 | <0.001 | 54.1 | 17.7 | 0.01 |
| Nomogram vs. AST/ALT | 32.2 | 10.3 | <0.001 | 25.0 | 18.0 | <0.001 |
| Nomogram vs.LDH | 25.7 | 13.5 | <0.001 | 41.7 | 13.6 | 0.03 |
| Nomogram vs. TNM stage | 27.8 | 13.2 | 0.01 | 21.7 | 11.6 | 0.026 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Liang, L.; Li, Y.; Hong, Y.; Ji, T.; Chen, H.; Lin, Z. Nomogram Based on Liver Function Test Indicators for Survival Prediction in Nasopharyngeal Carcinoma Patients Receiving PD-1 Inhibitor Therapy. Curr. Oncol. 2023, 30, 7189-7202. https://doi.org/10.3390/curroncol30080521
Liang L, Li Y, Hong Y, Ji T, Chen H, Lin Z. Nomogram Based on Liver Function Test Indicators for Survival Prediction in Nasopharyngeal Carcinoma Patients Receiving PD-1 Inhibitor Therapy. Current Oncology. 2023; 30(8):7189-7202. https://doi.org/10.3390/curroncol30080521
Chicago/Turabian StyleLiang, Lixia, Yan Li, Yansui Hong, Tianxing Ji, Hao Chen, and Zhifang Lin. 2023. "Nomogram Based on Liver Function Test Indicators for Survival Prediction in Nasopharyngeal Carcinoma Patients Receiving PD-1 Inhibitor Therapy" Current Oncology 30, no. 8: 7189-7202. https://doi.org/10.3390/curroncol30080521