‘Targeting’ Improved Outcomes with Antibody-Drug Conjugates in Non-Small Cell Lung Cancer—An Updated Review


Abstract
:1. Introduction
2. ADCs—Structure and Mechanism of Action
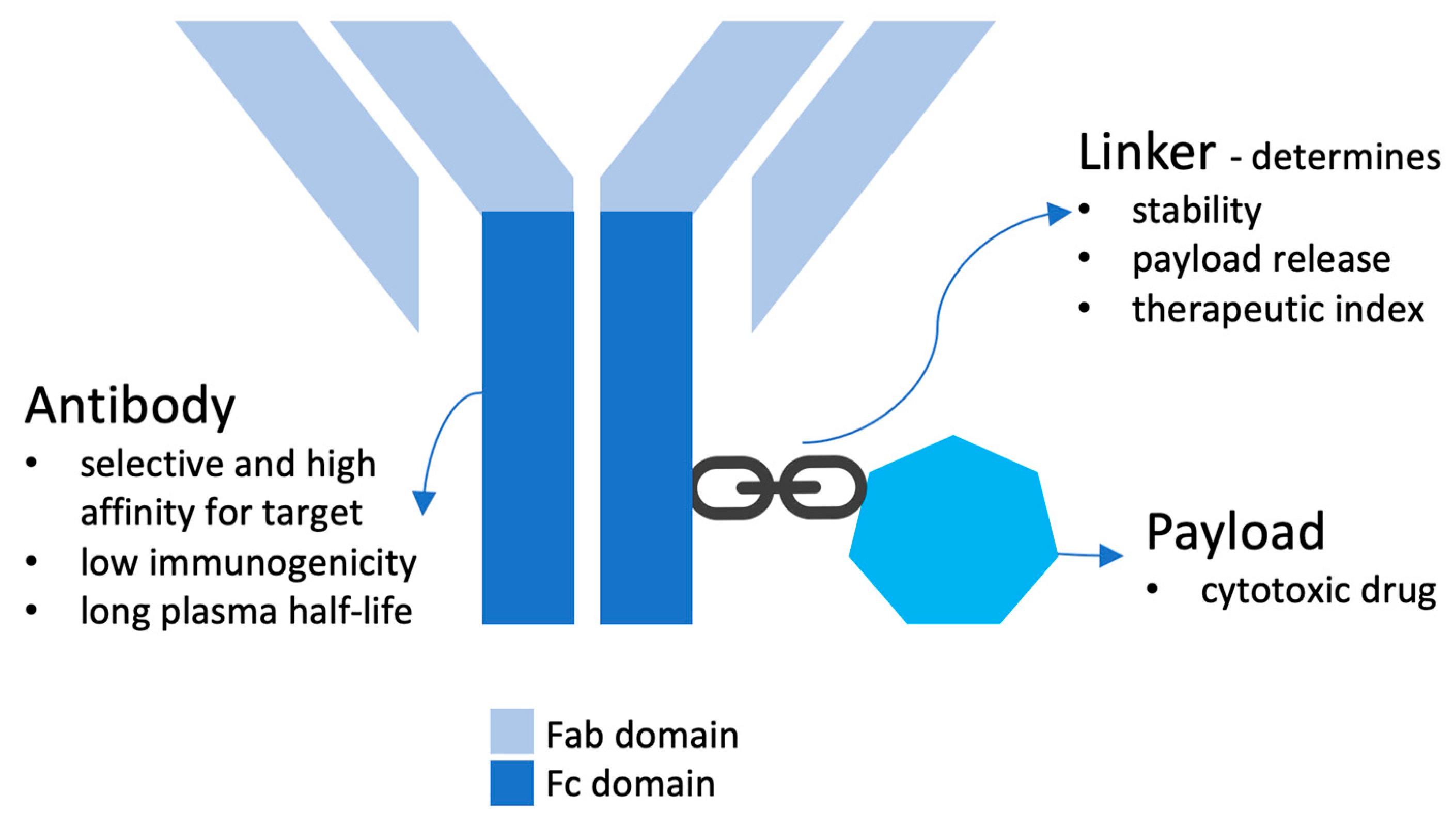
2.1. Structure
2.1.1. Antibody
2.1.2. Payload
2.1.3. Linker
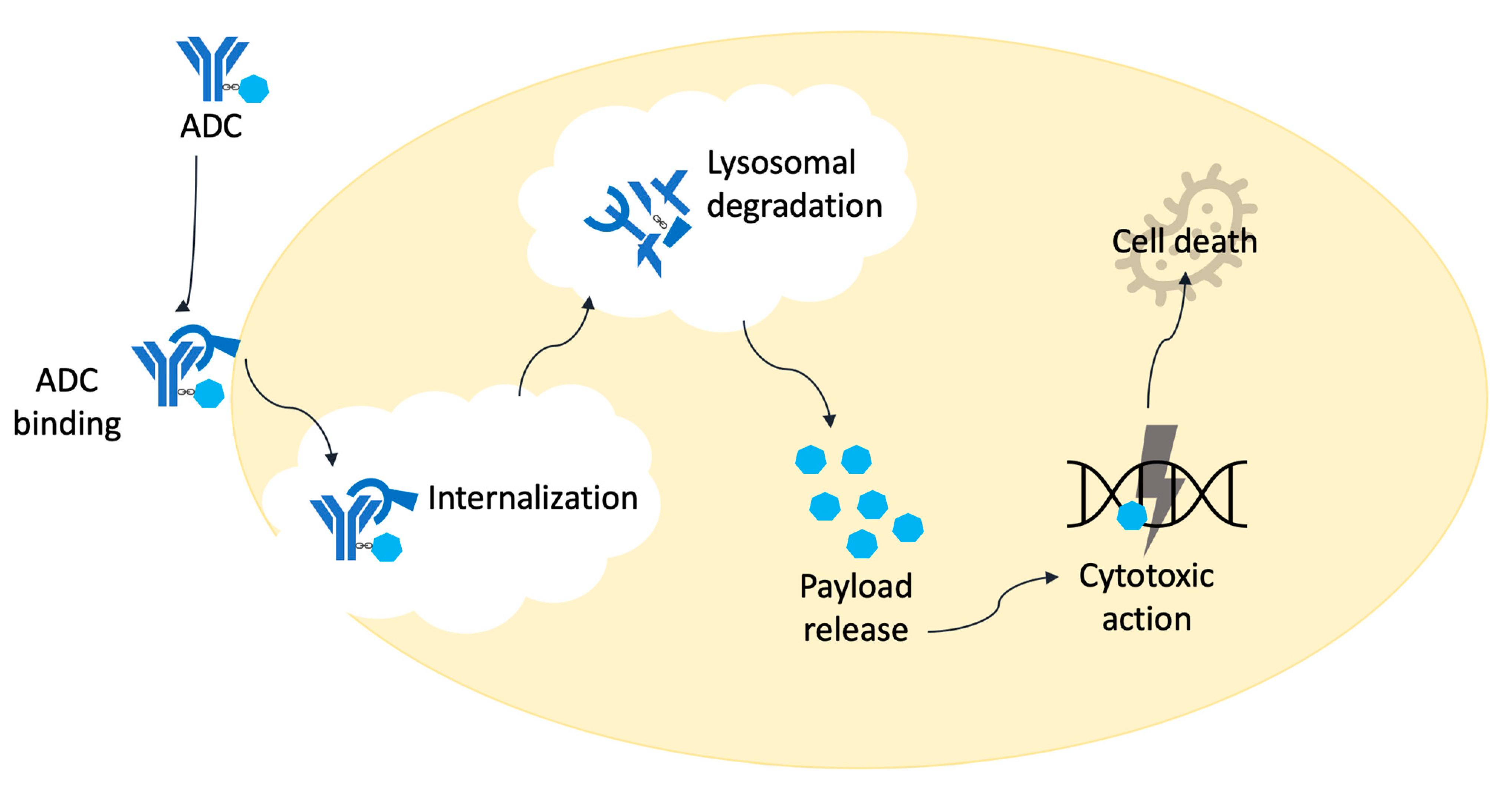
2.2. Mechanism of Action
2.3. Antigenic Targets
3. ADCs in NSCLC
3.1. Trastuzumab Deruxtecan
3.2. Ado-Trastuzumab Emtansine (TDM1)
3.3. Sacituzumab Govitecan
3.4. Datopotamab Deruxtecan (DS-1062)
3.5. Patritumab Deruxtecan (HER3-DXd, U3-1402)
3.6. Tusamitamab Ravtansine (SAR408701)
3.7. Telisotuzumab Vedotin (Teliso-V/ABBV399)
3.8. Zanidatamab Zovodotin (ZW49)
3.9. DS-7300
3.10. Enopotamab Vedotin (EnaV)
4. Toxicity
5. Biomarkers
6. Resistance Mechanisms
7. Future
8. Conclusions
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
References
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA A Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef] [PubMed]
- Fu, Z.; Li, S.; Han, S.; Shi, C.; Zhang, Y. Antibody drug conjugate: The “biological missile” for targeted cancer therapy. Signal Transduct. Target. Ther. 2022, 7, 93. [Google Scholar] [CrossRef] [PubMed]
- De Cecco, M.; Galbraith, D.N.; McDermott, L.L. What makes a good Antibody-Drug conjugate? Expert Opin. Biol. Ther. 2021, 21, 841–847. [Google Scholar] [CrossRef] [PubMed]
- Pysz, I.; Jackson, P.J.M.; Thurston, D.E. Introduction to Antibody-Drug Conjugates (ADCs). In Cytotoxic Payloads for Antibody—Drug Conjugates [Internet]; Thurston, D.E., Jackson, P.J.M., Eds.; The Royal Society of Chemistry: London, UK, 2019; pp. 1–30. Available online: https://books.rsc.org/books/book/725/chapter/444646/Introduction-to-Antibody-Drug-Conjugates-ADCs (accessed on 10 April 2023).
- Coleman, N.; Yap, T.A.; Heymach, J.V.; Meric-Bernstam, F.; Le, X. Antibody-drug conjugates in lung cancer: Dawn of a new era? NPJ Precis Oncol. 2023, 7, 5. [Google Scholar] [CrossRef]
- Ogitani, Y.; Aida, T.; Hagihara, K.; Yamaguchi, J.; Ishii, C.; Harada, N.; Soma, M.; Okamoto, H.; Oitate, M.; Arakawa, S.; et al. DS-8201a, A Novel HER2-Targeting ADC with a Novel DNA Topoisomerase I Inhibitor, Demonstrates a Promising Antitumor Efficacy with Differentiation from T-DM1. Clin. Cancer Res. 2016, 22, 5097–5108. [Google Scholar] [CrossRef]
- Lewis Phillips, G.D.; Li, G.; Dugger, D.L.; Crocker, L.M.; Parsons, K.L.; Mai, E.; Blättler, W.A.; Lambert, J.M.; Chari, R.V.J.; Lutz, R.J.; et al. Targeting HER2-Positive Breast Cancer with Trastuzumab-DM1, an Antibody–Cytotoxic Drug Conjugate. Cancer Res. 2008, 68, 9280–9290. [Google Scholar] [CrossRef] [PubMed]
- Jhaveri, K.; Han, H.; Dotan, E.; Oh, D.-Y.; Ferrario, C.; Tolcher, A.; Lee, K.-W.; Liao, C.-Y.; Kang, Y.-K.; Kim, Y.; et al. 460MO Preliminary results from a phase I study using the bispecific, human epidermal growth factor 2 (HER2)-targeting antibody-drug conjugate (ADC) zanidatamab zovodotin (ZW49) in solid cancers. Ann. Oncol. 2022, 33, S749–S750. [Google Scholar] [CrossRef]
- Hashimoto, Y.; Koyama, K.; Kamai, Y.; Hirotani, K.; Ogitani, Y.; Zembutsu, A.; Abe, M.; Kaneda, Y.; Maeda, N.; Shiose, Y.; et al. A Novel HER3-Targeting Antibody-Drug Conjugate, U3-1402, Exhibits Potent Therapeutic Efficacy through the Delivery of Cytotoxic Payload by Efficient Internalization. Clin. Cancer Res. 2019, 25, 7151–7161. [Google Scholar] [CrossRef]
- Goldenberg, D.M.; Cardillo, T.M.; Govindan, S.V.; Rossi, E.A.; Sharkey, R.M. Trop-2 is a novel target for solid cancer therapy with sacituzumab govitecan (IMMU-132), an antibody-drug conjugate (ADC). Oncotarget 2015, 6, 22496–22512. [Google Scholar] [CrossRef]
- Okajima, D.; Yasuda, S.; Yokouchi, Y.; Fujitani, T.; Sakurai, K.; Yamaguchi, J.; Kitamura, M.; Terauchi, T.; Shibutani, T.; Aida, T.; et al. Preclinical efficacy studies of DS-1062a, a novel TROP2-targeting antibody-drug conjugate with a novel DNA topoisomerase i inhibitor DXd. J. Clin. Oncol. 2018, 36, e24206. [Google Scholar] [CrossRef]
- Wang, J.; Anderson, M.G.; Oleksijew, A.; Vaidya, K.S.; Boghaert, E.R.; Tucker, L.; Zhang, Q.; Han, E.K.; Palma, J.P.; Naumovski, L.; et al. ABBV-399, a c-Met Antibody-Drug Conjugate that Targets Both MET–Amplified and c-Met–Overexpressing Tumors, Irrespective of MET Pathway Dependence. Clin. Cancer Res. 2017, 23, 992–1000. [Google Scholar] [CrossRef] [PubMed]
- Decary, S.; Berne, P.-F.; Nicolazzi, C.; Lefebvre, A.-M.; Dabdoubi, T.; Cameron, B.; Rival, P.; Devaud, C.; Prades, C.; Bouchard, H.; et al. Preclinical Activity of SAR408701: A Novel Anti-CEACAM5–maytansinoid Antibody-Drug Conjugate for the Treatment of CEACAM5-positive Epithelial Tumors. Clin. Cancer Res. 2020, 26, 6589–6599. [Google Scholar] [CrossRef] [PubMed]
- Yamato, M.; Hasegawa, J.; Maejima, T.; Hattori, C.; Kumagai, K.; Watanabe, A.; Nishiya, Y.; Shibutani, T.; Aida, T.; Hayakawa, I.; et al. DS-7300a, a DNA Topoisomerase I Inhibitor, DXd-Based Antibody-Drug Conjugate Targeting B7-H3, Exerts Potent Antitumor Activities in Preclinical Models. Mol. Cancer Ther. 2022, 21, 635–646. [Google Scholar] [CrossRef] [PubMed]
- Koopman, L.A.; Terp, M.G.; Zom, G.G.; Janmaat, M.L.; Jacobsen, K.; Heuvel, E.G.-V.D.; Brandhorst, M.; Forssmann, U.; De Bree, F.; Pencheva, N.; et al. Enapotamab vedotin, an AXL-specific antibody-drug conjugate, shows preclinical antitumor activity in non-small cell lung cancer. JCI Insight 2019, 4, e128199. [Google Scholar] [CrossRef] [PubMed]
- Seagen Inc. A Phase 2 Study of Brentuximab Vedotin in Combination with Pembrolizumab in Subjects with Metastatic Solid Malignancies after Progression on Prior PD-1 Inhibitor Treatment [Internet]. clinicaltrials.gov; 2023 Jan. Report No.: NCT04609566. Available online: https://clinicaltrials.gov/ct2/show/NCT04609566 (accessed on 27 February 2023).
- Astellas Pharma Global Development, Inc. An Open-label, Multicenter, Multicohort, Phase 2 Study to Evaluate Enfortumab Vedotin in Subjects With Previously Treated Locally Advanced or Metastatic Malignant Solid Tumors (EV-202) [Internet]. clinicaltrials.gov; 2023 Feb. Report No.: NCT04225117. Available online: https://clinicaltrials.gov/ct2/show/NCT04225117 (accessed on 27 February 2023).
- Muro, K.; Bruce, J.Y.; Baranda, J.; Feinstein, T.; Li, X.; Gorla, S.; Wu, C.; Braiteh, F. P47.02 EV-202: Phase 2 Study of Enfortumab Vedotin for Previously Treated Advanced Solid Tumors Including Non-Small Cell Lung Cancer. J. Thorac. Oncol. 2021, 16, S1096–S1097. [Google Scholar] [CrossRef]
- Hassan, R.; Blumenschein, G.R., Jr.; Moore, K.N.; Santin, A.D.; Kindler, H.L.; Nemunaitis, J.J.; Seward, S.M.; Thomas, A.; Kim, S.K.; Rajagopalan, P.; et al. First-in-Human, Multicenter, Phase I Dose-Escalation and Expansion Study of Anti-Mesothelin Antibody-Drug Conjugate Anetumab Ravtansine in Advanced or Metastatic Solid Tumors. J. Clin. Oncol. 2020, 38, 1824–1835. [Google Scholar] [CrossRef]
- Oh, S.Y.; Lim, S.M.; Lee, Y.W.; Lee, E.J.; Kim, J.H.; Heo, S.G.; Yu, M.R.; Hong, M.H.; Kim, H.R.; DaSilva, J.; et al. A MET targeting biparatopic antibody-drug conjugates (ADC), REGN5093-M114, has an antitumor efficacy in NSCLC harboring MET gene alterations. Cancer Res. 2022, 82, LB515A. [Google Scholar] [CrossRef]
- Johnson, M.; Ulahannan, S.; Vandross, A.; Park, H.; Faoro, L.; Faggioni, R.; Li, J.; Chang, Y.L.; Uttamsingh, S.; Tolcher, A. A first-in-human phase 1 study of the safety and pharmacokinetics of XB002 in patients with inoperable locally advanced or metastatic solid tumors. Cancer Res. 2022, 82 (Suppl. S12), CT254. [Google Scholar] [CrossRef]
- Calvo, E.; Cleary, J.M.; Moreno, V.; Gifford, M.; Roberts-Rapp, L.; Ansell, P.J.; Mittapalli, R.K.; Lee, H.J.; Hu, B.; Barch, D.; et al. Preliminary results from a phase 1 study of the antibody-drug conjugate ABBV- 221 in patients with solid tumors likely to express EGFR. J. Clin. Oncol. 2017, 35, 2510. [Google Scholar] [CrossRef]
- Thwaites, M.J.; Figueredo, R.; Tremblay, G.; Koropatnick, J.; Goldmacher, V.; O’Connor-McCourt, M. AVID100 is an anti-EGFR ADC that promotes DMI-meditated cytotoxicity on cancer cells but not on normal cells. Cancer Res. 2019, 79, 218. [Google Scholar] [CrossRef]
- Shenderov, E.; Mallesara, G.H.G.; Wysocki, P.J.; Xu, W.; Ramlau, R.; Weickhardt, A.J.; Zolnierek, J.; Spira, A.; Joshua, A.M.; Powderly, J.; et al. MGC018, an anti-B7-H3 antibody-drug conjugate (ADC), in patients with advanced solid tumors: Preliminary results of phase I cohort expansion. Ann. Oncol. 2021, 32, S657–S659. [Google Scholar] [CrossRef]
- Lakhani, N.J.; Braña, I.; Chiu, V.K.; Dowlati, A.; Lee, E.K.; McGoldrick, S.M.; Minchom, A.; Tian, X.; Patnaik, A. 556TiP A phase I study of SGN-STNV, a novel antibody-drug conjugate targeting sialyl-thomsen-nouveau antigen (STn), in adults with advanced solid tumors (SGNSTNV-001). Ann. Oncol. 2021, 32, S613–S614. [Google Scholar] [CrossRef]
- Tolaney, S.M.; Do, K.T.; Eder, J.P.; LoRusso, P.M.; Weekes, C.D.; Chandarlapaty, S.; Chang, C.W.; Chen, S.C.; Nazzal, D.; Schuth, E.; et al. A phase I study of DLYE5953A, an Anti-LY6E antibody covalently linked to monomethyl Auristatin E, in patients with refractory solid tumors. Clin. Cancer Res. 2021, 26, 5588–5597. [Google Scholar] [CrossRef] [PubMed]
- Nicolazzi, C.; Caron, A.; Tellier, A.; Trombe, M.; Pinkas, J.; Payne, G.; Carrez, C.; Guérif, S.; Maguin, M.; Baffa, R.; et al. An antibody-drug conjugate targeting MUC1-associated carbohydrate CA6 shows promising antitumor activities. Mol. Cancer Ther. 2020, 19, 1660–1669. [Google Scholar] [CrossRef]
- Staudacher, A.H.; Brown, M.P. Antibody drug conjugates and bystander killing: Is antigen-dependent internalisation required? Br. J. Cancer 2017, 117, 1736–1742. [Google Scholar] [CrossRef]
- Criscitiello, C.; Morganti, S.; Curigliano, G. Antibody-Drug conjugates in solid tumors: A look into novel targets. J. Hematol. Oncol. 2021, 14, 20. [Google Scholar] [CrossRef]
- Ogitani, Y.; Hagihara, K.; Oitate, M.; Naito, H.; Agatsuma, T. Bystander killing effect of DS-8201a, a novel anti-human epidermal growth factor receptor 2 Antibody-Drug conjugate, in tumors with human epidermal growth factor receptor 2 heterogeneity. Cancer Sci. 2016, 107, 1039–1046. [Google Scholar] [CrossRef]
- Modi, S.; Jacot, W.; Yamashita, T.; Sohn, J.; Vidal, M.; Tokunaga, E.; Tsurutani, J.; Ueno, N.T.; Prat, A.; Chae, Y.S.; et al. Trastuzumab Deruxtecan in Previously Treated HER2-Low Advanced Breast Cancer. N. Engl. J. Med. 2022, 387, 9–20. [Google Scholar] [CrossRef]
- Iwama, E.; Zenke, Y.; Sugawara, S.; Daga, H.; Morise, M.; Yanagitani, N.; Sakamoto, T.; Murakami, H.; Kishimoto, J.; Matsumoto, S.; et al. Trastuzumab emtansine for patients with non–small cell lung cancer positive for human epidermal growth factor receptor 2 exon-20 insertion mutations. Eur. J. Cancer 2021, 162, 99–106. [Google Scholar] [CrossRef]
- Peters, S.; Stahel, R.; Bubendorf, L.; Bonomi, P.; Villegas, A.; Kowalski, D.M.; Baik, C.S.; Isla, D.; Carpeno, J.D.C.; Garrido, P.; et al. Trastuzumab Emtansine (T-DM1) in Patients with Previously Treated HER2-Overexpressing Metastatic Non–Small Cell Lung Cancer: Efficacy, Safety, and Biomarkers. Clin. Cancer Res. 2019, 25, 64–72. [Google Scholar] [CrossRef]
- Li, B.T.; Smit, E.F.; Goto, Y.; Nakagawa, K.; Udagawa, H.; Mazières, J.; Nagasaka, M.; Bazhenova, L.; Saltos, A.N.; Felip, E.; et al. Trastuzumab Deruxtecan in HER2-Mutant Non–Small-Cell Lung Cancer. N. Engl. J. Med. 2022, 386, 241–251. [Google Scholar] [CrossRef]
- Li, B.; Smit, E.; Goto, Y.; Nakagawa, K.; Goto, K.; Mazieres, J.; Uprety, D.; Bazhenova, L.; Saltos, A.; Felip, E.; et al. 976P Phase II trial of trastuzumab deruxtecan (T-DXd) in patients (Pts) with HER2-mutated (HER2m) metastatic non-small cell lung cancer (NSCLC): Registrational data from DESTINY-Lung01. Ann. Oncol. 2022, 33, S995–S996. [Google Scholar] [CrossRef]
- Smit, E.; Felip, E.; Uprety, D.; Nakagawa, K.; Paz-Ares, L.; Pacheco, J.; Li, B.; Planchard, D.; Baik, C.; Goto, Y.; et al. 975P Trastuzumab deruxtecan in patients (pts) with HER2-overexpressing (HER2-OE) metastatic non-small cell lung cancer (NSCLC): Results from the DESTINY-Lung01 trial. Ann. Oncol. 2022, 33, S994–S995. [Google Scholar] [CrossRef]
- Enhertu Approved in the US as the First HER2-Directed Therapy for Patients with Previously Treated HER2-Mutant Metastatic Non-Small Cell Lung Cancer [Internet]. Available online: https://www.astrazeneca.com/media-centre/press-releases/2022/enhertu-approved-in-us-for-her2-mutant-nsclc.html (accessed on 12 September 2022).
- Daiichi Sankyo, Inc. A Phase 2, Multicenter, Randomized Study of Trastuzumab Deruxtecan in Subjects with HER2-Mutated Metastatic Non-Small Cell Lung Cancer (NSCLC) (DESTINY-LUNG02) [Internet]. clinicaltrials.gov; 2022. Report No.: NCT04644237. Available online: https://clinicaltrials.gov/ct2/show/NCT04644237 (accessed on 18 September 2022).
- Janne, P.A.; Baik, C.S.; Su, W.-C.; Johnson, M.L.; Hayashi, H.; Nishio, M.; Kim, D.-W.; Koczywas, M.; Gold, K.A.; Steuer, C.E.; et al. Efficacy and safety of patritumab deruxtecan (HER3-DXd) in EGFR inhibitor-resistant, EGFR-mutated (EGFRm) non-small cell lung cancer (NSCLC). J. Clin. Oncol. 2021, 39 (Suppl. S15), 9007. [Google Scholar] [CrossRef]
- Steuer, C.E.; Hayashi, H.; Su, W.C.; Nishio, M.; Johnson, M.L.; Kim, D.W.; Koczywas, M.; Felip, E.; Gold, K.A.; Murakami, H.; et al. Efficacy and safety of patritumab deruxtecan (HER3-DXd) in advanced/metastatic non-small cell lung cancer (NSCLC) without EGFR-activating mutations. JCO 2022, 40 (Suppl. S16), 9017. [Google Scholar] [CrossRef]
- Levy, B.; Paz-Ares, L.; Rixe, O.; Su, W.-C.; Yang, T.-Y.; Tolcher, A.; Lou, Y.; Zenke, Y.; Savvides, P.; Felip, E.; et al. MA13.07 TROPION-Lung02: Initial Results for Datopotamab Deruxtecan Plus Pembrolizumab and Platinum Chemotherapy in Advanced NSCLC. J. Thorac. Oncol. 2022, 17, S91. [Google Scholar] [CrossRef]
- Meric-Bernstam, F.; Spira, A.I.; Lisberg, A.E.; Sands, J.; Yamamoto, N.; Johnson, M.L.; Yoh, K.; Garon, E.B.; Heist, R.S.; Petrich, A.; et al. TROPION-PanTumor01: Dose analysis of the TROP2-directed antibody-drug conjugate (ADC) datopotamab deruxtecan (Dato-DXd, DS-1062) for the treatment (Tx) of advanced or metastatic non-small cell lung cancer (NSCLC). JCO 2021, 39 (Suppl. S15), 9058. [Google Scholar] [CrossRef]
- Garon, E.; Johnson, M.; Lisberg, A.; Spira, A.; Yamamoto, N.; Heist, R.; Sands, J.; Yoh, K.; Meric-Bernstam, F.; Kitazono, S.; et al. MA03.02 TROPION-PanTumor01: Updated Results From the NSCLC Cohort of the Phase 1 Study of Datopotamab Deruxtecan in Solid Tumors. J. Thorac. Oncol. 2021, 16, S892–S893. [Google Scholar] [CrossRef]
- Daiichi Sankyo Co., Ltd. Phase 1, Two-part, Multicenter, Open-label, Multiple Dose, First-in-human Study of DS-1062a in Subjects With Advanced Solid Tumors (TROPION-PanTumor01) [Internet]. clinicaltrials.gov; 2022 Jun. Report No.: NCT03401385. Available online: https://clinicaltrials.gov/ct2/show/NCT03401385 (accessed on 18 September 2022).
- Gilead Sciences. A Phase I/II Study of IMMU-132 (hRS7-SN38 Antibody Drug Conjugate) in Patients With Epithelial Cancer [Internet]. clinicaltrials.gov; 2021 Aug. Report No.: NCT01631552. Available online: https://clinicaltrials.gov/ct2/show/NCT01631552 (accessed on 18 September 2022).
- Heist, R.S.; Guarino, M.J.; Masters, G.; Purcell, W.T.; Starodub, A.N.; Horn, L.; Scheff, R.J.; Bardia, A.; Messersmith, W.A.; Berlin, J.; et al. Therapy of Advanced Non–Small-Cell Lung Cancer With an SN-38-Anti-Trop-2 Drug Conjugate, Sacituzumab Govitecan. JCO 2017, 35, 2790–2797. [Google Scholar] [CrossRef]
- Camidge, D.R.; Bar, J.; Horinouchi, H.; Goldman, J.W.; Moiseenko, F.V.; Filippova, E.; Cicin, I.; Bradbury, P.A.; Daaboul, N.; Tomasini, P.; et al. Telisotuzumab vedotin (Teliso-V) monotherapy in patients (pts) with previously treated c-Met–overexpressing (OE) advanced non-small cell lung cancer (NSCLC). J. Clin. Oncol. 2022, 40 (Suppl. S16), 9016. [Google Scholar] [CrossRef]
- Gazzah, A.; Bedard, P.; Hierro, C.; Kang, Y.-K.; Razak, A.A.; Ryu, M.-H.; Demers, B.; Fagniez, N.; Henry, C.; Hospitel, M.; et al. Safety, pharmacokinetics, and antitumor activity of the anti-CEACAM5-DM4 Antibody-Drug conjugate tusamitamab ravtansine (SAR408701) in patients with advanced solid tumors: First-in-human dose-escalation study. Ann. Oncol. 2022, 33, 416–425. [Google Scholar] [CrossRef] [PubMed]
- Doi, T.; Patel, M.; Falchook, G.; Koyama, T.; Friedman, C.; Piha-Paul, S.; Gutierrez, M.; Abdul-Karim, R.; Awad, M.; Adkins, D.; et al. 453O DS-7300 (B7-H3 DXd antibody-drug conjugate [ADC]) shows durable antitumor activity in advanced solid tumors: Extended follow-up of a phase I/II study. Ann. Oncol. 2022, 33, S744–S745. [Google Scholar] [CrossRef]
- Ramalingam, S.; Lopez, J.; Mau-Sorensen, M.; Thistlethwaite, F.; Piha-Paul, S.; Gadgeel, S.; Drew, Y.; Jänne, P.; Mansfield, A.; Chen, G.; et al. OA02.05 First-In-Human Phase 1/2 Trial of Anti-AXL Antibody-Drug Conjugate (ADC) Enapotamab Vedotin (EnaV) in Advanced NSCLC. J. Thorac. Oncol. 2019, 14, S209. [Google Scholar] [CrossRef]
- AstraZeneca. An Open-label, Randomized, Multicenter, Phase 3 Study to Assess the Efficacy and Safety of Trastuzumab Deruxtecan as First-line Treatment of Unresectable, Locally Advanced, or Metastatic NSCLC Harboring HER2 Exon 19 or 20 Mutations (DESTINY-Lung04) [Internet]. clinicaltrials.gov; 2022 Aug. Report No.: NCT05048797. Available online: https://clinicaltrials.gov/ct2/show/NCT05048797 (accessed on 6 September 2022).
- AstraZeneca. A Phase Ib Multicenter, Open-label Dose-Escalation Study to Evaluate the Safety and Tolerability of Trastuzumab Deruxtecan (T-DXd) and Durvalumab in Combination With Cisplatin, Carboplatin or Pemetrexed in First-line Treatment of Patients With Advanced or Metastatic Non-squamous Non-small Cell Lung Cancer (NSCLC) and Human Epidermal Growth Factor Receptor 2 Overexpression (HER2+) (DESTINY-Lung03) [Internet]. clinicaltrials.gov; 2022 Jul. Report No.: NCT04686305. Available online: https://clinicaltrials.gov/ct2/show/NCT04686305 (accessed on 9 September 2022).
- Daiichi Sankyo, Inc. A Phase 1b, Multicenter, Two-Part, Open-Label Study of Trastuzumab Deruxtecan (DS-8201a), An Anti-Human Epidermal Growth Factor Receptor-2 (HER2)-Antibody Drug Conjugate (ADC), In Combination With Pembrolizumab, An Anti-PD-1 Antibody, For Subjects With Locally Advanced/Metastatic Breast Or Non-Small Cell Lung Cancer (NSCLC) [Internet]. clinicaltrials.gov; 2022 May. Report No.: NCT04042701. Available online: https://clinicaltrials.gov/ct2/show/NCT04042701 (accessed on 9 September 2022).
- Daiichi Sankyo, Inc. A Phase 3, Randomized, Open-Label Study of Patritumab Deruxtecan Versus Platinum-Based Chemotherapy in Metastatic or Locally Advanced Epidermal Growth Factor Receptor-Mutated (EGFRm) Non-small Cell Lung Cancer (NSCLC) After Failure of Epidermal Growth Factor Receptor (EGFR) Tyrosine Kinase Inhibitor (TKI) Therapy (HERTHENA-Lung02) [Internet]. clinicaltrials.gov; 2022 Aug. Report No.: NCT05338970. Available online: https://clinicaltrials.gov/ct2/show/NCT05338970 (accessed on 1 September 2022).
- Mok, T.; Wu, Y.-L.; Nishio, M.; Reck, M.; Wu, E.; Sternberg, D.; Esker, S.; Yu, H. 1195TiP HERTHENA-Lung02: A randomized phase III study of patritumab deruxtecan vs platinum-based chemotherapy in locally advanced or metastatic EGFR-mutated NSCLC after progression with a third-generation EGFR TKI. Ann. Oncol. 2022, 33, S1095. [Google Scholar] [CrossRef]
- Daiichi Sankyo, Inc. A Phase 1 Open-Label Study of Patritumab Deruxtecan in Combination With Osimertinib in Subjects with Locally Advanced or Metastatic EGFR-mutated Non-Small Cell Lung Cancer (NSCLC) [Internet]. clinicaltrials.gov; 2021 Nov. Report No.: NCT04676477. Available online: https://clinicaltrials.gov/ct2/show/NCT04676477 (accessed on 9 September 2022).
- Yu, H.; Cantero, F.; Kim, B.; Lee, M.; Wu, E.; Sternberg, D.; Jänne, P. 1190TiP Pharmacokinetics, efficacy, and safety of patritumab deruxtecan (HER3-DXd) in EGFR inhibitor-resistant, EGFR-mutated (EGFRm) non-small cell lung cancer (NSCLC). Ann. Oncol. 2022, 33, S1092–S1093. [Google Scholar] [CrossRef]
- Janne, P.A.; Johnson, M.L.; Goto, Y.; Yang, J.C.-H.; Vigliotti, M.; Dong, Q.; Qiu, Y.; Yu, C.; Yu, H.A. HERTHENA-Lung01: A randomized phase 2 study of patritumab deruxtecan (HER3-DXd) in previously treated metastatic EGFR-mutated NSCLC. J. Clin. Oncol. 2021, 39 (Suppl. S15), TPS9139. [Google Scholar] [CrossRef]
- Daiichi Sankyo, Inc. HERTHENA-Lung01: A Phase 2 Randomized Open-Label Study of Patritumab Deruxtecan (U3-1402) in Subjects With Previously Treated Metastatic or Locally Advanced EGFR-mutated Non-Small Cell Lung Cancer (NSCLC) [Internet]. clinicaltrials.gov; 2022 Sep. Report No.: NCT04619004. Available online: https://clinicaltrials.gov/ct2/show/NCT04619004 (accessed on 18 September 2022).
- Daiichi Sankyo, Inc. Phase 3 Randomized Study of DS-1062a Versus Docetaxel in Previously Treated Advanced or Metastatic Non-Small Cell Lung Cancer (TROPION-LUNG01) [Internet]. clinicaltrials.gov; 2022 Jun. Report No.: NCT04656652. Available online: https://clinicaltrials.gov/ct2/show/NCT04656652 (accessed on 9 September 2022).
- Daiichi Sankyo, Inc. A Randomized, Open-label, Phase 3 Trial of Dato-DXd Plus Pembrolizumab vs Pembrolizumab Alone in Treatment-Naïve Subjects With Advanced or Metastatic PD-L1 High (TPS ≥50%) Non-small Cell Lung Cancer Without Actionable Genomic Alterations (TROPION-Lung08) [Internet]. clinicaltrials.gov; 2022 Aug. Report No.: NCT05215340. Available online: https://clinicaltrials.gov/ct2/show/NCT05215340 (accessed on 9 September 2022).
- AstraZeneca. A Phase 1b, Multicenter, 2-Part, Open-Label Study of Datopotamab Deruxtecan (Data-DXd) in Combination With Durvalumab With or Without Carboplatin in Subjects With Advanced or Metastatic Non-Small Cell Lung Cancer (TROPION-Lung04) [Internet]. clinicaltrials.gov; 2022 Sep. Report No.: NCT04612751. Available online: https://clinicaltrials.gov/ct2/show/NCT04612751 (accessed on 9 September 2022).
- Garassino, M.C.; Reznick, D.; Liu, S.Y.; Reinmuth, N.; Girard, N.; de Marinis, F.; Mekan, S.F.; Patel, R.; Ding, M.; Paz-Ares, L. EVOKE-01: A phase 3 study of sacituzumab govitecan (SG) versus docetaxel in patients with non–small cell lung cancer (NSCLC) progressing on or after platinum-based chemotherapy and checkpoint inhibitors. J. Clin. Oncol. 2022, 40 (Suppl. S16), TPS9149. [Google Scholar] [CrossRef]
- Reinmuth, N.; Reznick, D.; Liu, S.; Garassino, M.; Girard, N.; De Marinis, F.; Mekan, S.; Patel, R.; Ding, M.; Paz-Ares, L. P1.16-04 Phase 3 EVOKE-01 Study of Sacituzumab Govitecan vs Docetaxel in NSCLC After Prior Platinum and Checkpoint Inhibitors. J. Thorac. Oncol. 2022, 17, S128. [Google Scholar] [CrossRef]
- Reck, M.; Liu, S.; Owen, S.; Garon, E.; Neal, J.; Vicente, D.; Mekan, S.; Safavi, F.; Fernando, N.; Mok, T. EP08.02-098 Phase 2 EVOKE-02 Study of Sacituzumab Govitecan and Pembrolizumab±Platinum in First-Line Metastatic NSCLC. J. Thorac. Oncol. 2022, 17, S448. [Google Scholar] [CrossRef]
- Hoffmann-La Roche. A Phase Ib/II, Open-Label, Multicenter, Randomized Umbrella Study Evaluating the Efficacy And Safety of Multiple Immunotherapy-Based Treatment Combinations in Patients with Metastatic Non-Small Cell Lung Cancer (Morpheus-Lung) [Internet]. clinicaltrials.gov; 2022 Sep. Report No.: NCT03337698. Available online: https://clinicaltrials.gov/ct2/show/NCT03337698 (accessed on 9 September 2022).
- Sanofi. Randomized, Open Label Phase 3 Study of SAR408701 Versus Docetaxel in Previously Treated Metastatic Non- Squamous Non-Small Cell Lung Cancer Patients With CEACAM5 Positive Tumors [Internet]. clinicaltrials.gov; 2022 Jul. Report No.: NCT04154956. Available online: https://clinicaltrials.gov/ct2/show/NCT04154956 (accessed on 9 September 2022).
- Cousin, S.; Soufflet, C. EP08.02-030 Tusamitamab Ravtansine in Patients with NSQ NSCLC and Negative or Moderate CEACAM5 Expression Tumors and High Circulating CEA. J. Thorac. Oncol. 2022, 17, S411. [Google Scholar] [CrossRef]
- Sanofi. Open-label, Phase 2 Study, Evaluating the Efficacy and Safety of Tusamitamab Ravtansine in Non-squamous Non-small-cell Lung Cancer (NSQ NSCLC) Participants WITH Negative or Moderate CEACAM5 Expression Tumors and High Circulating CEA [Internet]. clinicaltrials.gov; 2022 Oct. Report No.: NCT05245071. Available online: https://clinicaltrials.gov/ct2/show/NCT05245071 (accessed on 20 November 2022).
- AbbVie. A Phase 3 Open-Label, Randomized, Controlled, Global Study of Telisotuzumab Vedotin (ABBV-399) Versus Docetaxel in Subjects with Previously Treated c-Met Overexpressing, EGFR Wildtype, Locally Advanced/Metastatic Non-Squamous Non-Small Cell Lung Cancer [Internet]. clinicaltrials.gov; 2022 Sep. Report No.: NCT04928846. Available online: https://clinicaltrials.gov/ct2/show/NCT04928846 (accessed on 9 September 2022).
- AbbVie. A Multicenter, Phase 1/1b, Open-Label, Dose-Escalation Study of ABBV-399, an Antibody Drug Conjugate, in Subjects With Advanced Solid Tumors [Internet]. clinicaltrials.gov; 2022 Aug. Report No.: NCT02099058. Available online: https://clinicaltrials.gov/ct2/show/NCT02099058 (accessed on 9 September 2022).
- Rotow, J.; Yoh, K.; Powderly, J.; Shimizu, T.; Perets, R.; Paz-Ares, L.; Phillips, A.; Souers, A.; Ansell, P.; Jin, J.; et al. 1185TiP First-in-human phase I study of ABBV-637 as monotherapy and in combination in patients with relapsed and refractory solid tumors. Ann. Oncol. 2022, 33, S1090. [Google Scholar] [CrossRef]
- Adjei, A.A.; Bekaii-Saab, T.S.; Berlin, J.; Philip, P.A.; Mercade, T.M.; Walter, A.; Cupit, L.; Liu, R.; Fields, S.Z.; Holynskyj, A. Phase 1b multi-indication study of the antibody drug conjugate anetumab ravtansine in patients with mesothelin-expressing advanced or recurrent malignancies. J. Thorac. Oncol. 2017, 36, TPS2607. [Google Scholar] [CrossRef]
- Modi, S.; Saura, C.; Yamashita, T.; Park, Y.H.; Kim, S.-B.; Tamura, K.; Andre, F.; Iwata, H.; Ito, Y.; Tsurutani, J.; et al. Trastuzumab Deruxtecan in Previously Treated HER2-Positive Breast Cancer. N. Engl. J. Med. 2020, 382, 610–621. [Google Scholar] [CrossRef] [PubMed]
- Shitara, K.; Bang, Y.-J.; Iwasa, S.; Sugimoto, N.; Ryu, M.-H.; Sakai, D.; Chung, H.-C.; Kawakami, H.; Yabusaki, H.; Lee, J.; et al. Trastuzumab Deruxtecan in Previously Treated HER2-Positive Gastric Cancer. N. Engl. J. Med. 2020, 382, 2419–2430. [Google Scholar] [CrossRef] [PubMed]
- Tsurutani, J.; Iwata, H.; Krop, I.; Jänne, P.A.; Doi, T.; Takahashi, S.; Park, H.; Redfern, C.; Tamura, K.; Wise-Draper, T.M.; et al. Targeting HER2 with Trastuzumab Deruxtecan: A Dose-Expansion, Phase I Study in Multiple Advanced Solid Tumors. Cancer Discov. 2020, 10, 688–701. [Google Scholar] [CrossRef]
- Li, B.T.; Michelini, F.; Misale, S.; Cocco, E.; Baldino, L.; Cai, Y.; Shifman, S.; Tu, H.-Y.; Myers, M.L.; Xu, C.; et al. HER2-Mediated Internalization of Cytotoxic Agents in ERBB2 Amplified or Mutant Lung Cancers. Cancer Discov. 2020, 10, 674–687. [Google Scholar] [CrossRef]
- Goto, K.; Sang-We, K.; Kubo, T.; Goto, Y.; Ahn, M.-J.; Planchard, D.; Kim, D.-W.; Yang, J.-H.; Yang, T.-Y.; Pereira, K.; et al. LBA55 Trastuzumab deruxtecan (T-DXd) in patients (Pts) with HER2-mutant metastatic non-small cell lung cancer (NSCLC): Interim results from the phase 2 DESTINY-Lung02 trial. Ann. Oncol. 2022, 33, S1422. [Google Scholar] [CrossRef]
- Research C for DE. FDA Grants Accelerated Approval to Fam-Trastuzumab Deruxtecan-Nxki for HER2-Mutant Non-Small Cell Lung Cancer. FDA [Internet]. 2022 Aug 16. Available online: https://www.fda.gov/drugs/resources-information-approved-drugs/fda-grants-accelerated-approval-fam-trastuzumab-deruxtecan-nxki-her2-mutant-non-small-cell-lung (accessed on 22 August 2022).
- Hotta, K.; Aoe, K.; Kozuki, T.; Ohashi, K.; Ninomiya, K.; Ichihara, E.; Kubo, T.; Ninomiya, T.; Chikamori, K.; Harada, D.; et al. A Phase II Study of Trastuzumab Emtansine in HER2-Positive Non–Small Cell Lung Cancer. J. Thorac. Oncol. 2018, 13, 273–279. [Google Scholar] [CrossRef]
- Li, B.T.; Shen, R.; Buonocore, D.; Olah, Z.T.; Ni, A.; Ginsberg, M.S.; Ulaner, G.A.; Offin, M.; Feldman, D.; Hembrough, T.; et al. Ado-Trastuzumab Emtansine for Patients With HER2-Mutant Lung Cancers: Results From a Phase II Basket Trial. JCO 2018, 36, 2532–2537. [Google Scholar] [CrossRef]
- Saxena, A.; Michel, L.S.; Hong, Q.; Hilsinger, K.; Kanwal, C.; Pichardo, C.; Goswami, T.; Santin, A. TROPiCS–03: A phase II open-label study of sacituzumab govitecan (SG) in patients with metastatic solid tumors. J. Clin. Oncol. 2020, 38 (Suppl. S15), TPS3648. [Google Scholar] [CrossRef]
- Scharpenseel, H.; Hanssen, A.; Loges, S.; Mohme, M.; Bernreuther, C.; Peine, S.; Lamszus, K.; Goy, Y.; Petersen, C.; Westphal, M.; et al. EGFR and HER3 expression in circulating tumor cells and tumor tissue from non-small cell lung cancer patients. Sci. Rep. 2019, 9, 7406. [Google Scholar] [CrossRef]
- Haikala, H.M.; Lopez, T.; Köhler, J.; Eser, P.O.; Xu, M.; Zeng, Q.; Teceno, T.J.; Ngo, K.; Zhao, Y.; Ivanova, E.V.; et al. EGFR inhibition enhances the cellular uptake and antitumor-activity of the HER3 antibody drug conjugate HER3-DXd. Cancer Res. 2021, 82, 130–141. [Google Scholar] [CrossRef] [PubMed]
- Zhu, Y.; Liu, K.; Wang, K.; Zhu, H. Treatment-Related Adverse Events of Antibody-Drug Conjugates in Clinical Trials: A Systematic Review and Meta-Analysis. Cancer [Internet]. n/a(n/a). Available online: https://onlinelibrary.wiley.com/doi/abs/10.1002/cncr.34507 (accessed on 29 November 2022).
- Powell, C.; Modi, S.; Iwata, H.; Takahashi, S.; Smit, E.; Siena, S.; Chang, D.-Y.; Macpherson, E.; Qin, A.; Singh, J.; et al. Pooled analysis of drug-related interstitial lung disease and/or pneumonitis in nine trastuzumab deruxtecan monotherapy studies. ESMO Open 2022, 7, 100554. [Google Scholar] [CrossRef] [PubMed]
- Matsuno, O. Drug-induced interstitial lung disease: Mechanisms and best diagnostic approaches. Respir. Res. 2012, 13, 39. [Google Scholar] [CrossRef]
- Kumagai, K.; Aida, T.; Tsuchiya, Y.; Kishino, Y.; Kai, K.; Mori, K. Interstitial pneumonitis related to trastuzumab deruxtecan, a human epidermal growth factor receptor 2-targeting Ab–drug conjugate, in monkeys. Cancer Sci. 2020, 111, 4636–4645. [Google Scholar] [CrossRef]
- Swain, S.M.; Nishino, M.; Lancaster, L.H.; Li, B.T.; Nicholson, A.G.; Bartholmai, B.J.; Naidoo, J.; Schumacher-Wulf, E.; Shitara, K.; Tsurutani, J.; et al. Multidisciplinary clinical guidance on trastuzumab deruxtecan (T-DXd)–related interstitial lung disease/pneumonitis—Focus on proactive monitoring, diagnosis, and management. Cancer Treat. Rev. 2022, 106, 102378. [Google Scholar] [CrossRef]
- Zhao, H.; Atkinson, J.; Gulesserian, S.; Zeng, Z.; Nater, J.; Ou, J.; Yang, P.; Morrison, K.; Coleman, J.; Malik, F.; et al. Modulation of Macropinocytosis-Mediated Internalization Decreases Ocular Toxicity of Antibody-Drug Conjugates. Cancer Res 2018, 78, 2115–2126. [Google Scholar] [CrossRef] [PubMed]
- Von Minckwitz, G.; Huang, C.-S.; Mano, M.S.; Loibl, S.; Mamounas, E.P.; Untch, M.; Wolmark, N.; Rastogi, P.; Schneeweiss, A.; Redondo, A.; et al. Trastuzumab Emtansine for Residual Invasive HER2-Positive Breast Cancer. N. Engl. J. Med. 2019, 380, 617–628. [Google Scholar] [CrossRef]
- Geraud, A.; Xu, H.P.; Beuzeboc, P.; Kirova, Y.M. Preliminary experience of the concurrent use of radiosurgery and T-DM1 for brain metastases in HER2-positive metastatic breast cancer. J. Neuro-Oncol. 2016, 131, 69–72. [Google Scholar] [CrossRef]
- Nguyen, T.D.; Bordeau, B.M.; Balthasar, J.P. Mechanisms of ADC Toxicity and Strategies to Increase ADC Tolerability. Cancers 2023, 15, 713. [Google Scholar] [CrossRef]
- Su, Z.; Xiao, D.; Xie, F.; Liu, L.; Wang, Y.; Fan, S.; Zhou, X.; Li, S. Antibody-Drug conjugates: Recent advances in linker chemistry. Acta Pharm. Sin. B 2021, 11, 3889–3907. [Google Scholar] [CrossRef] [PubMed]
- May, C.; Sapra, P.; Gerber, H.-P. Advances in bispecific biotherapeutics for the treatment of cancer. Biochem. Pharmacol. 2012, 84, 1105–1112. [Google Scholar] [CrossRef]
- Lin, J.; Sagert, J. Targeting Drug Conjugates to the Tumor Microenvironment: Probody Drug Conjugates. In Innovations for Next-Generation Antibody-Drug Conjugates [Internet]; Damelin, M., Ed.; Cancer Drug Discovery and Development; Springer International Publishing: Cham, Switzerland, 2018; pp. 281–298. Available online: http://link.springer.com/10.1007/978-3-319-78154-9_12 (accessed on 10 April 2022).
- Bordeau, B.M.; Nguyen, T.D.; Polli, J.R.; Chen, P.; Balthasar, J.P. Payload-Binding Fab Fragments Increase the Therapeutic Index of MMAE Antibody-Drug Conjugates. Mol. Cancer Ther. 2023, 22, 459–470. [Google Scholar] [CrossRef]
- LoRusso, P.M.; Weiss, D.; Guardino, E.; Girish, S.; Sliwkowski, M.X. Trastuzumab Emtansine: A Unique Antibody-Drug Conjugate in Development for Human Epidermal Growth Factor Receptor 2–Positive Cancer. Clin. Cancer Res. 2011, 17, 6437–6447. [Google Scholar] [CrossRef]
- LaPointe, N.; Hertle, N.; Hsu, S.C.; Kellis, J.; King, N.; Littrell, J.; Nguyen, Q.; Ren, J.; Srdanov, M.R.; Tanna, V.; et al. Validation of an immunohistochemical assay, CEACAM5 IHC 769, under development for use with the antibody-drug conjugate tusamitamab ravtansine (SAR408701). J. Clin. Oncol. 2021, 39 (Suppl. S16), e21030. [Google Scholar] [CrossRef]
- Calvo, E.; Cleary, J.M.; Moreno, V.; Gifford, M.; Roberts-Rapp, L.; Ansell, P.J.; Lee, H.-J.; Hu, B.; Barch, D.; Ocampo, C.; et al. Abstract A028: Biomarker analysis in a phase 1 study of the antibody-drug conjugate ABBV-221 in patients with solid tumors likely to overexpress the epidermal growth factor receptor (EGFR). Mol. Cancer Ther. 2018, 17 (Suppl. S1), A028. [Google Scholar] [CrossRef]
- Thyparambil, S.P.; Liao, W.L.; Heaton, R.; Zhang, G.; Strasbaugh, A.; Melkie, M.; Ling, X.B. Clinical survey of Trop2 antibody drug conjugate target and payload biomarkers in multiple cancer indications using multiplex mass spectrometry. Cancer Research. 2022, 82 (Suppl. S12), 4099. [Google Scholar] [CrossRef]
- Coats, S.; Williams, M.; Kebble, B.; Dixit, R.; Tseng, L.; Yao, N.-S.; Tice, D.A.; Soria, J.-C. Antibody-Drug Conjugates: Future Directions in Clinical and Translational Strategies to Improve the Therapeutic Index. Clin. Cancer Res. 2019, 25, 5441–5448. [Google Scholar] [CrossRef]
- Betts, A.M.; Haddish-Berhane, N.; Tolsma, J.; Jasper, P.; King, L.E.; Sun, Y.; Chakrapani, S.; Shor, B.; Boni, J.; Johnson, T.R. Preclinical to Clinical Translation of Antibody-Drug Conjugates Using PK/PD Modeling: A Retrospective Analysis of Inotuzumab Ozogamicin. AAPS J. 2016, 18, 1101–1116. [Google Scholar] [CrossRef]
- Collins, D.M.; Bossenmaier, B.; Kollmorgen, G.; Niederfellner, G. Acquired Resistance to Antibody-Drug Conjugates. Cancers 2019, 11, 394. [Google Scholar] [CrossRef]
- Loganzo, F.; Tan, X.; Sung, M.; Jin, G.; Myers, J.S.; Melamud, E.; Wang, F.; Diesl, V.; Follettie, M.T.; Musto, S.; et al. Tumor Cells Chronically Treated with a Trastuzumab–Maytansinoid Antibody-Drug Conjugate Develop Varied Resistance Mechanisms but Respond to Alternate Treatments. Mol. Cancer Ther. 2015, 14, 952–963. [Google Scholar] [CrossRef] [PubMed]
- Mazor, Y.; Sachsenmeier, K.F.; Yang, C.; Hansen, A.; Filderman, J.; Mulgrew, K.; Wu, H.; Dall’acqua, W.F. Enhanced tumor-targeting selectivity by modulating bispecific antibody binding affinity and format valence. Sci. Rep. 2017, 7, 40098. [Google Scholar] [CrossRef] [PubMed]
- Andre, F.; Fernanda, M.; Deluche, E.; Lusque, A.; Le-Bescond, L.; Filleron, T. Mechanism of Action and Resistance to Trastuzumab Deruxtecan in Patients with Metastatic Breast Cancer: The DAISY Tria [Internet]. 2022. Available online: https://www.researchsquare.com/article/rs-2083650/v1 (accessed on 11 April 2023).
- Sung, M.; Tan, X.; Lu, B.; Golas, J.; Hosselet, C.; Wang, F.; Tylaska, L.; King, L.; Zhou, D.; Dushin, R.; et al. Caveolae-Mediated Endocytosis as a Novel Mechanism of Resistance to Trastuzumab Emtansine (T-DM1). Mol. Cancer Ther. 2018, 17, 243–253. [Google Scholar] [CrossRef]
- Chen, Y.F.; Xu, Y.Y.; Shao, Z.M.; Yu, K.D. Resistance to antibody-drug conjugates in breast cancer: Mechanisms and solutions. Cancer Commun. 2023, 43, 297–337. [Google Scholar] [CrossRef]
- Tarantino, P.; Pestana, R.C.; Corti, C.; Modi, S.; Bardia, A.; Tolaney, S.M.; Cortes, J.; Soria, J.; Curigliano, G.; Bardia, A. Antibody-Drug conjugates: Smart chemotherapy delivery across tumor histologies. CA: A Cancer J. Clin. 2021, 72, 165–182. [Google Scholar] [CrossRef] [PubMed]
- Yamazaki, C.M.; Yamaguchi, A.; Anami, Y.; Xiong, W.; Otani, Y.; Lee, J.; Ueno, N.T.; Zhang, N.; An, Z.; Tsuchikama, K. Antibody-drug conjugates with dual payloads for combating breast tumor heterogeneity and drug resistance. Nat. Commun. 2021, 12, 3528. [Google Scholar] [CrossRef] [PubMed]
- Oganesyan, V.; Peng, L.; Bee, J.S.; Li, J.; Perry, S.R.; Comer, F.; Xu, L.; Cook, K.; Senthil, K.; Clarke, L.; et al. Structural insights into the mechanism of action of a biparatopic anti-HER2 antibody. J. Biol. Chem. 2018, 293, 8439–8448. [Google Scholar] [CrossRef]
- Maruani, A. Bispecifics and Antibody-Drug conjugates: A positive synergy. Drug Discov. Today Technol. 2018, 30, 55–61. [Google Scholar] [CrossRef]
- Walsh, S.J.; Bargh, J.D.; Dannheim, F.M.; Hanby, A.R.; Seki, H.; Counsell, A.J.; Ou, X.; Fowler, E.; Ashman, N.; Takada, Y.; et al. Site-selective modification strategies in Antibody-Drug conjugates. Chem. Soc. Rev. 2020, 50, 1305–1353. [Google Scholar] [CrossRef]
- Junutula, J.R.; Raab, H.; Clark, S.; Bhakta, S.; Leipold, D.D.; Weir, S.; Chen, Y.; Simpson, M.; Tsai, S.P.; Dennis, M.S.; et al. Site-specific conjugation of a cytotoxic drug to an antibody improves the therapeutic index. Nat. Biotechnol. 2008, 26, 925–932. [Google Scholar] [CrossRef]
- Polu, K.R.; Lowman, H.B. Probody therapeutics for targeting antibodies to diseased tissue. Expert Opin Biol Ther. 2014, 14, 1049–1053. [Google Scholar] [CrossRef] [PubMed]
- Autio, K.A.; Boni, V.; Humphrey, R.W.; Naing, A. Probody Therapeutics: An Emerging Class of Therapies Designed to Enhance On-Target Effects with Reduced Off-Tumor Toxicity for Use in Immuno-Oncology. Clin. Cancer Res. 2020, 26, 984–989. [Google Scholar] [CrossRef] [PubMed]
- Nicolò, E.; Giugliano, F.; Ascione, L.; Tarantino, P.; Corti, C.; Tolaney, S.M.; Cristofanilli, M.; Curigliano, G. Combining antibody-drug conjugates with immunotherapy in solid tumors: Current landscape and future perspectives. Cancer Treat. Rev. 2022, 106, 102395. [Google Scholar] [CrossRef] [PubMed]
- Boshuizen, J.; Koopman, L.A.; Krijgsman, O.; Shahrabi, A.; van den Heuvel, E.G.; A Ligtenberg, M.A.; Vredevoogd, D.W.; Kemper, K.; Kuilman, T.; Song, J.-Y.; et al. Cooperative targeting of melanoma heterogeneity with an AXL antibody-drug conjugate and BRAF/MEK inhibitors. Nat. Med. 2018, 24, 203–212. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| ADCs in Clinical Development | |||||
|---|---|---|---|---|---|
| ADC | Target | Antibody | Linker | Payload | DAR |
| Trastuzumab Deruxtecan (T-DXd) [6] | HER2 | Trastuzumab | Cleavable | Deruxtecan | 8 |
| Ado-trastuzumab Emtansine (T-DM1) [7] | Trastuzumab | Non-cleavable | Emtansine (DM1) | 3.5 | |
| Zanidatamab Zovodotin (ZW49) [8] | ZW25 | Cleavable | Novel Auristatin toxin | 2 | |
| Patritumab Deruxtecan (HER3-DXd) [9] | HER3 | Patritumab | Cleavable | Deruxtecan | 8 |
| Sacituzumab Govitecan (SG) [10] | Trop-2 | Sacituzumab | Cleavable | SN-38 | 7.6 |
| Datopotamab Deruxtecan (Dato-DXd) [11] | Datopotamab | Cleavable | Deruxtecan | 4 | |
| Telisotuzumab Vedotin (Teliso-V) [12] | MET | ABT-700 | Cleavable | Monomethyl auristatin E (MMAE) | 3.1 |
| Tusamitamab ravtansine [13] | CEACAM5 | Anti-CEACAM5 | Cleavable | DM4 | 3.8 |
| DS-7300 [14] | B7-H3 | Deruxtecan | 4 | ||
| Enapotamab vedotin (EnaV) [15] | AXL | AXL-specific IgG1 kappa | Cleavable | MMAE | 4 |
| Brentuximab vedotin [16] | CD30 | IgG1 kappa | Cleavable | MMAE | 4 |
| Enfortumab vedotin [17,18] | Nectin-4 | IgG1 kappa | Cleavable | MMAE | 3.8 |
| Anetumab ravtansine (BAY 94-9343) [19] | Mesothelin | IgG1 lambda | reducible SPDB linker | DM4 | 3.2 |
| ADCs in preclinical development | |||||
| ADC | Target | Payload | |||
| REGN5093-M114 [20] | MET | maytansinoid payload | |||
| XB002 [21] | Tissue Factor | Zymelink Auristatin | |||
| LY3076226 | Fibroblast growth factor receptor 3 (FGFR3) | DM4 | |||
| ABBV-221 [22] | EGFR | MMAE | |||
| AVID100 [23] | EGFR | DM1 | |||
| MGC018 [24] | B7-H3 | Duocarmycin | |||
| SGN-STNV [25] | STn | MMAE | |||
| DLYE5953A [26] | LYSE | MMAE | |||
| SAR566658 [27] | CA6 | DM4 | |||
| ADC | Study (Phase) | Sample Size (n) | Population | Intervention | Overall Response Rate (ORR) | Disease Control Rate | Median Progression-Free Survival in Months (mPFS) (95% CI) | Median Overall Survival in Months (mOS) (95% CI) | Median Duration of Response in Months (mDOR) (95% CI) | Common Grade Adverse Events (%) |
|---|---|---|---|---|---|---|---|---|---|---|
| HER-2 or ERBB2 | ||||||||||
| Ado-Trastuzumab Emtansine/TDM-1 | Iwama et al., 2021 Phase 2 [32] | 22 | Previously treated HER2 exon-20 insertion mutations | T-DM1 (3.6 mg/kg) intravenously every 21 days | 38.1% (23.0–55.9) | 52.4% (35.2–69%) | 2.8 (1.4–4.4) | 8.1 (3.5–13.2) | 3.5 (2.7–6.5) | Thrombocytopenia (63.6%) Transaminitis (AST—45.5%, ALT—40.9%) ILD (13.6%, no grade ¾) |
| Peters et al., 2019 [33] | 49 (29, IHC 2+, 20 IHC 3+) | Previously treated HER2-overexpressing (OE) advanced NSCLC | T-DM1 (3.6 mg/kg) intravenously every 21 days | IHC 2+, 0%; IHC 3+, 20% (5.7–43.7) | IHC 3+: 40% | IHC 2+, 2.6 (1.4–2.8); IHC 3+, 2.7 (1.4–8.3) | IHC 2+, 12.2 (3.8–23.3); IHC 3+, 15.3 (4.1-NE) | - | Hypersensitivity Peripheral neuropathy Thrombocytopenia Hepatotoxicity | |
| ZW49 | Jhaveri et al. [8], 2022 | 1 | Previously treated locally advanced/metastatic solid malignant tumors | ZW49 | 28% | 72% | - | - | - | Keratitis (42%) Alopecia (25%) Diarrhea (21%) |
| Trastuzumab Deruxtecan/T-DXd/DS-8201 | Li et al., 2022 DESTINY-Lung01 Phase 2 [34,35] | 91 | Previously treated HER2 mutant NSCLC | T-DXd (6.4 mg/kg) intravenously every 21 days | 54.9% (44.2–65.4) | 92% (85–97) | 8.2 (6–11.9) | 18.6 (13.8–25.8) | 10.6 (5.8–17.7) | Nausea (73%) Fatigue (53%) Neutropenia (35%) Anemia (33%) Diarrhoea (32%) |
| Smit et al., 2022 DESTINY-Lung01 [36] | Cohort 1—49 patients Cohort 1a—41 patients | Previously treated HER2-OE NSCLC | Cohort 1—T-DXd 6.4 mg/kg Cohort 1a—T-DXd 5.4 mg/kg | Cohort 1—26.5% (15–41.1) Cohort 1a—34.1 (20.1–50.6) | Cohort 1—69.4% (54.6-81.8) Cohort 1a—78.0% (62.4–89.4) | - | - | Cohort 1—5.8 (4.3-NE); Cohort 2—6.2 (4.2–9.8) | Cohort 1 vs. 1a Nausea (59.2% and 73.2%) Decreased appetite (44.9% and 46.3%) Fatigue (32.7% and 51.2%) ILD (20.4–4.9%) | |
| DESTINY-Lung02 2022 NCT04644237 [37,38] | 101 (6.4 mg/kg arm) 50 (5.4 mg/kg arm) | Previously treated HER2 mutant NSCLC | T-DXd (6.4 vs. 5.4 mg/kg) intravenously every 21 days | 6.4 mg/kg: 42.9% (24.5–62.8); 5.4 mg/kg: 53.8% (39.5–67.8) | 6.4 mg/kg: 92.9% (76.5–99.1); 5.4 mg/kg: 90.4% (79–96.8) | - | - | 6.4 mg/kg: 5.9 (2.8-NE); 5.4 mg/kg: NE (4.2-NE) | - | |
| HER-3 | ||||||||||
| Patrizumab Deruxtecan/HER3-DXd/U3-1402 | Janne et al., 2021 Phase 1 [39] NCT03260491 | 57 | Previously treated EGFR inhibitor-resistant, EGFR-mutated (EGFRm) NSCLC cohort | HER3-DXd 5.6 mg/kg IV Q3W | 39% (26–52.4) | 72% (58.5–83) | 8.2 (4.4–8.3) | - | - | Grade ≥ 3 AEs Thrombocytopenia (30%) Neutropenia (19%) Fatigue (14%) ILD (all grade: 7%) |
| Steuer et al., 2021 Phase 1 [40] NCT03260491 | 47 | Previously treated EGFR-unmutated (EGFR wild-type (WT)) NSCLC cohort | HER3-DXd 5.6 mg/kg IV Q3W | - | 28% (16–43) | 5.4 (3.9–12.7) | - | 5.7 (3.7–10.7) | Grade ≥ 3 AEs Thrombocytopenia (15%) Neutropenia (26%) Fatigue (15%) ILD (all grade: 9%) | |
| TROP2 | ||||||||||
| Datopotamab Deruxtecan/Dato-DXd/DS-1062 | Levy et al., 2022 TROPION-Lung02 Phase 1b [41] | 60 | Previously treated (cohort 1-2) and treatment naïve (cohort 3-6) advanced/metastatic NSCLC | Cohort 1-2: Doublet (Dato-DXd + Pembrolizumab) Cohort 3-6: Triplet (Dato-DXd + Pembrolizumab + Platinum) | 39% Doublet—62% Triplet—50% | 82.6% Doublet—100% Triplet—90% | - | - | - | Stomatitis (42%) Nausea (38%) Fatigue (27%) |
| Garon et al., 2021 TROPION-PanTumor01 Phase 1 NCT03401385 [42,43,44] | 180 | Previously treated advanced/metastatic NSCLC | Dato-DXD 8 mg/kg 6 mg/kg 4 mg/kg | 24% 26% 24% | - | 8.2 (1.5–11.8) mg et al. | - | - | Nausea (52%) Stomatitis (48%) Alopecia (39%) Fatigue (32%) Neutropenia (6%) ILD (11%) | |
| Sacituzumab Govitecan (IMMU-132) | Heist et al., 2017 Phase 1/2 [45,46] | 54 | Previously treated advanced/metastatic NSCLC | IMMU-132 8 or 10 mg/kg were given on days 1 and 8 of 21-day cycles | 19% | 68% | 5.2 (3.2–7.1) | 9.5 (5.9–16.7) | 6 (4.8–8.3) | Neutropenia (37%) Diarrhea (61%) Nausea (80%) Fatigue (46%) Pneumonia (13%) |
| MET | ||||||||||
| Telisotuzumab vedotin (Teliso-V) | Camidge et al., 2022 Phase 2 LUMINOSITY (M14-239) [47] | 136 | Previously treated c-Met–OE advanced/metastatic NSCLC | Teliso-V 1.9 mg/kg IV Q2W NSQ EGFR WT cohort SQ EGFR WT cohort | c-Met OE NSQ EGFR WT—36.5%. 52.2% in c-Met high group | - | - | - | c-Met OE NSQ EGFR WT—6.9 (4.1–NE); c-Met high–6.9 (2.4–NE) | Peripheral sensory neuropathy (25.0%) Nausea (22.1%) Hypoalbuminemia (20.6%) |
| CEACAM5 | ||||||||||
| Tusamitamab ravtansine (SAR408701) | Gazzah et al., 2022 Phase 1 [48] | 31 | Previously treated locally advanced/metastatic solid malignant tumors | Tusamitamab ravtansine ranging from 5 to 150 mg/m2 | 9.7% | 45.2% | - | - | - | Asthenia (28%) Decreased appetite (28%) Keratopathy (28%) Nausea (28%) |
| B7-H3 | ||||||||||
| DS-7300 | Doi et al., 2022 [49] | All cancers–127 SQ NSCLC–5 | Previously treated locally advanced/metastatic solid malignant tumors | DS-7300 | 40%; sq NSCLC | 80%; sq NSCLC | - | - | - | Nausea (61%) Infusion-related reaction (35%) Vomiting (31%) |
| AXL | ||||||||||
| Enapotamab vedotin (EnaV) | Ramalingam et al., 2019 [50] Phase 1 | 26 | Previously treated advanced/metastatic NSCLC; EGFR WT/ALK- cohort | EnaV 2.2 mg/kg Q3W | 19% | 50% | - | - | - | GI toxicities |
| Drug | Study | Phase | Population | Intervention | Primary Endpoint |
|---|---|---|---|---|---|
| HER-2 or ERBB2 | |||||
| Trastuzumab Deruxtecan/T-DXd/DS-8201 | DESTINY-Lung04 NCT05048797 [51] | 3 | Locally advanced/metastatic NSCLC with HER2 mutation | T-DXd vs. SOC | PFS |
| DESTINY-Lung03 NCT04686305 [52] | 1 | Advanced/metastatic HER2 + NSQ NSCLC | T-DXd and Durvalumab with Chemotherapy | Frequency of AEs and SAE | |
| NCT04042701 [53] | 1 | Locally advanced/metastatic HER2+ Breast or HER2+ or HER2m NSCLC | T-DXd with pembrolizumab | DLTs and ORR | |
| HER 3 | |||||
| Patritumab Deruxtecan/U3-1402 | HERTHENA-Lung02 NCT05338970 [54,55] | 3 | Previously treated advanced/metastatic EGFR-mutated NSCLC | HER3-DXd versus platinum-based chemotherapy | PFS |
| NCT04676477 [56] | 1 | EGFR-mutated advanced/metastatic NSCLC | HER3-DXd with Osimertinib | DLTs | |
| NCT03260491 [57] | 1 | Locally advanced/metastatic EGFRm NSCLC progressing after EGFR TKI therapy and ≥1 line of platinum-based chemotherapy | HER3-DXd | Pharmacokinetics, efficacy and safety | |
| HERTHENA-Lung01 [58,59] | 2 | Previously treated metastatic EGFR-mutated NSCLC | HER3-DXd | ORR | |
| Trop 2 | |||||
| Datopotamab Deruxtecan/Dato-DXd/DS-1062 | TROPION-LUNG01 NCT04656652 [60] | 3 | Previously treated EGFR-mutated locally advanced/metastatic NSCLC | Dato-DXD vs. Docetaxel | PFS, OS |
| TROPION-LUNG08 NCT05215340 [61] | 3 | First-line treatment for advanced/metastatic NSCLC | Dato-DXD plus pembrolizumab vs. pembrolizumab | PFS, OS | |
| TROPION-LUNG04 NCT04612751 [62] | 1 | Advanced/metastatic NSCLC | Dato-DXD plus Durvalumab with/without carboplatin | Number of Participants with DLTs and Treatment-emergent AEs | |
| Sacituzumab govitecan | EVOKE-01 [63,64] Garassino et al. | 3 | Previously treated advanced/metastatic NSCLC | SG vs. Docetaxel | OS |
| EVOKE 02 [65] | 2 | Advanced/metastatic NSCLC | SG and Pembrolizumab ± platinum in first-line metastatic NSCLC | ORR, DLTs | |
| Morpheus Lung [66] NCT03337698 | 1/2 | Previously treated/untreated metastatic NSCLC | Atezolizumab with SG | % Of patients with objective response | |
| CAECAM5 | |||||
| Tusamitamab ravtansine (SAR408701) | CARMEN-LC03 [67] NCT04154956 | 3 | Previously treated CAECAM5-positive metastatic NSCLC | SAR408701 vs. Docetaxel | PFS, OS |
| CARMEN-LC06 [68,69] (NCT05245071) | 3 | Previously treated patients with negative or moderate CEACAM5-expressing NSQ NSCLC tumors and high circulating CEA levels | SAR408701 | ORR | |
| c-MET | |||||
| Telisotuzumab vedotin (Teliso-V)/ABBV-399 | NCT04928846 [70] | 3 | Previously treated c-Met OE, EGFR WT metastatic NSQ-NSCLC | Teliso-V vs. Docetaxel | PFS, OS |
| NCT02099058 [71] | 1 | Previously treated c-Met OE/EGFRm metastatic NSCLC | ABBV-399 as monotherapy and in combination with Osimertinib, erlotinib, and nivolumab | Number of patients with AEs and RPTD | |
| EGFR | |||||
| ABBV-637 | NCT04721015 [72] | 1 | Relapsed and refractory solid tumors | ABBV-399 as monotherapy and in combination with osimertinib or docetaxel | DLTs, RPTD |
| Mesothelin | |||||
| Anetumab ravtansine | Adjei et al. [73] | 1b | Relapsed and refractory solid tumors, Mesothelin expressing | Anetumab ravtansine at 6.5 mg/kg IV Q3W | ORR |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Verma, S.; Breadner, D.; Raphael, J. ‘Targeting’ Improved Outcomes with Antibody-Drug Conjugates in Non-Small Cell Lung Cancer—An Updated Review. Curr. Oncol. 2023, 30, 4329-4350. https://doi.org/10.3390/curroncol30040330
Verma S, Breadner D, Raphael J. ‘Targeting’ Improved Outcomes with Antibody-Drug Conjugates in Non-Small Cell Lung Cancer—An Updated Review. Current Oncology. 2023; 30(4):4329-4350. https://doi.org/10.3390/curroncol30040330
Chicago/Turabian StyleVerma, Saurav, Daniel Breadner, and Jacques Raphael. 2023. "‘Targeting’ Improved Outcomes with Antibody-Drug Conjugates in Non-Small Cell Lung Cancer—An Updated Review" Current Oncology 30, no. 4: 4329-4350. https://doi.org/10.3390/curroncol30040330