Survival Benefits of Radiotherapy and Surgery in Lung Cancer Brain Metastases with Poor Prognosis Factors

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Patients
2.2. Outcome Measurement and Follow-Up
2.3. Statistical Analysis
3. Results
3.1. Clinical Characteristics and Survival Benefits of Surgery and Radiotherapy in All Patients
3.2. Survival Benefits of Surgery and Radiotherapy in Patients with Poor Prognosis Factors
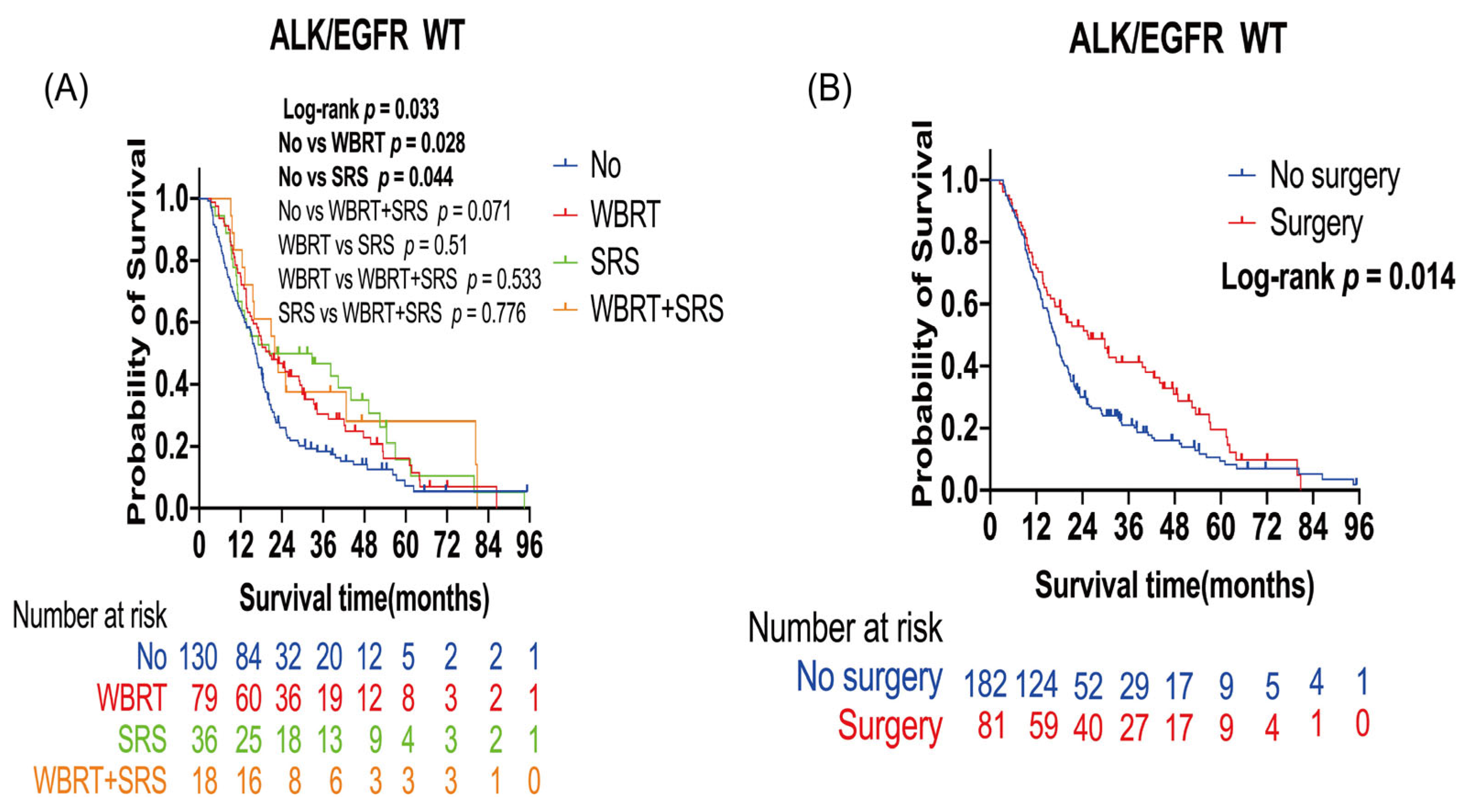
3.2.1. Survival Benefits of Surgery and Radiotherapy in Patients with Lung Cancer BMs with ALK/EGFR Wild Type
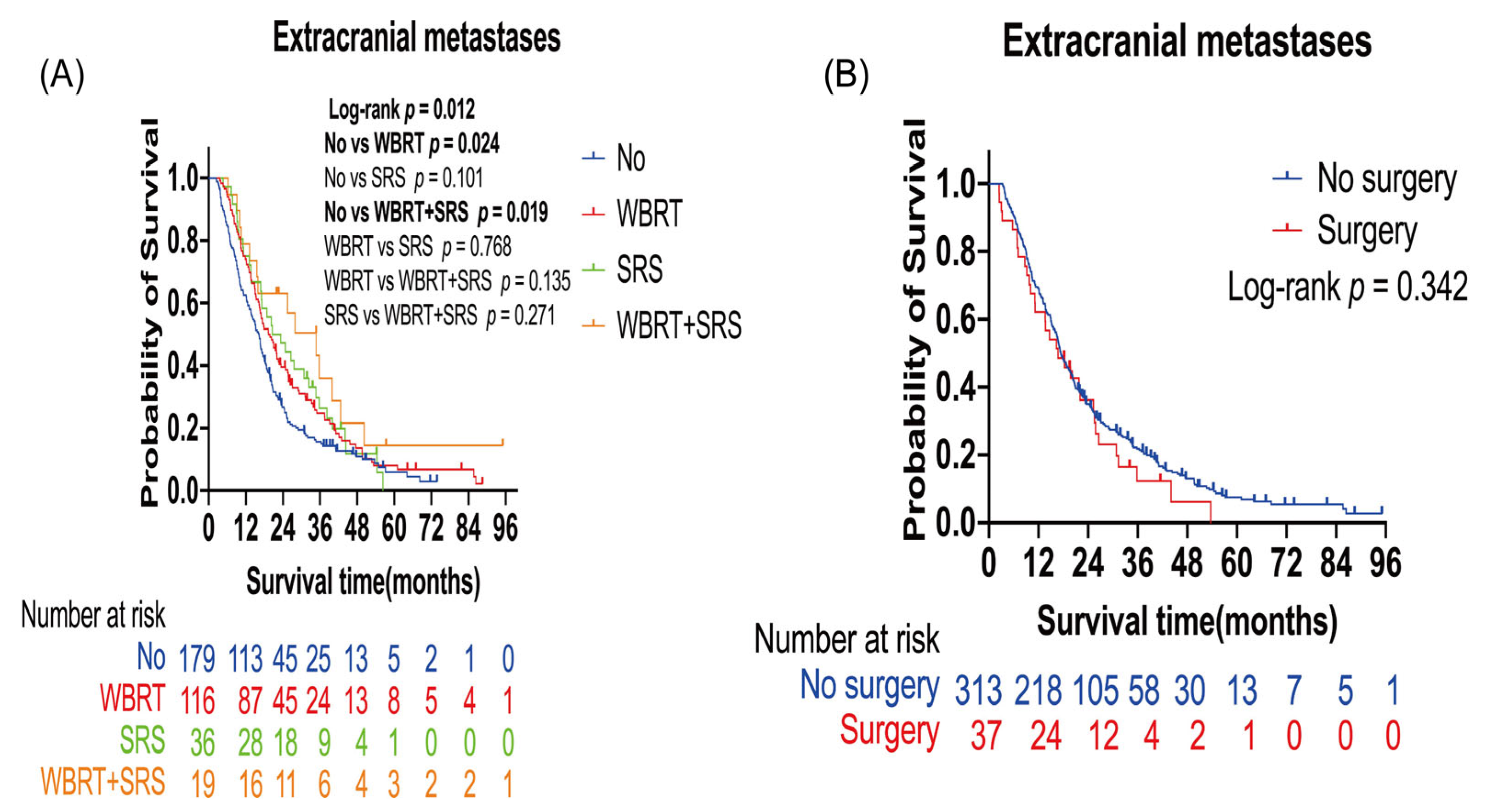
3.2.2. Survival Benefits of Surgery and Radiotherapy in Patients with Lung Cancer BMs with Extracranial Metastases
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Achrol, A.S.; Rennert, R.C.; Anders, C.; Soffietti, R.; Chang, S.D. Brain metastases. Nat. Rev. Dis. Prim. 2019, 5, 5. [Google Scholar] [CrossRef] [PubMed]
- Goldberg, S.B.; Contessa, J.N.; Omay, S.B.; Chiang, V. Lung Cancer Brain Metastases. Cancer J. 2015, 21, 398. [Google Scholar] [CrossRef] [PubMed]
- Kocher, M.; Soffietti, R.; Abacioglu, U.; Villà, S.; Fauchon, F.; Baumert, B.G.; Fariselli, L.; Tzuk-Shina, T.; Kortmann, R.-D.; Carrie, C.; et al. Adjuvant Whole-Brain Radiotherapy Versus Observation After Radiosurgery or Surgical Resection of One to Three Cerebral Metastases: Results of the EORTC 22952–26001 Study. J. Clin. Oncol. 2011, 29, 134–141. [Google Scholar] [CrossRef] [PubMed]
- Mahajan, A.; Ahmed, S.; McAleer, M.F.; Weinberg, J.S.; Li, J.; Brown, P.; Settle, S.; Prabhu, S.S.; Lang, F.F.; Levine, N.; et al. Post-operative stereotactic radiosurgery versus observation for completely resected brain metastases: A single-centre, randomised, controlled, phase 3 trial. Lancet Oncol. 2017, 18, 1040–1048. [Google Scholar] [CrossRef]
- Patchell, R.A.; Tibbs, P.A.; Walsh, J.W.; Dempsey, R.J.; Maruyama, Y.; Kryscio, R.J.; Markesbery, W.R.; Macdonald, J.S.; Young, B. A Randomized Trial of Surgery in the Treatment of Single Metastases to the Brain. N. Engl. J. Med. 1990, 322, 494–500. [Google Scholar] [CrossRef]
- Chamberlain, M.C.; Baik, C.S.; Gadi, V.K.; Bhatia, S.; Chow, L.Q. Systemic therapy of brain metastases: Non–small cell lung cancer, breast cancer, and melanoma. Neuro-Oncology 2017, 19, i1–i24. [Google Scholar] [CrossRef]
- Gogineni, E.; Vargo, J.A.; Glaser, S.M.; Flickinger, J.C.; Burton, S.A.; Engh, J.A.; Amankulor, N.M.; Beriwal, S.; Quinn, A.E.; Ozhasoglu, C.; et al. Long-Term Survivorship Following Stereotactic Radiosurgery Alone for Brain Metastases: Risk of Intracranial Failure and Implications for Surveillance and Counseling. Neurosurgery 2017, 83, 203–209. [Google Scholar] [CrossRef]
- Sperduto, P.W.; Yang, T.J.; Beal, K.; Pan, H.; Brown, P.D.; Bangdiwala, A.; Shanley, R.; Yeh, N.; Gaspar, L.E.; Braunstein, S.; et al. Estimating Survival in Patients with Lung Cancer and Brain Metastases An Update of the Graded Prognostic Assessment for Lung Cancer Using Molecular Markers (Lung-molGPA). JAMA Oncol. 2017, 3, 827–831. [Google Scholar] [CrossRef]
- Sperduto, P.W.; Chao, S.T.; Sneed, P.K.; Luo, X.; Suh, J.; Roberge, D.; Bhatt, A.; Jensen, A.W.; Brown, P.D.; Shih, H.; et al. Diagnosis-Specific Prognostic Factors, Indexes, and Treatment Outcomes for Patients with Newly Diagnosed Brain Metastases: A Multi-Institutional Analysis of 4259 Patients. Int. J. Radiat. Oncol. 2010, 77, 655–661. [Google Scholar] [CrossRef]
- Sahgal, A.; Aoyama, H.; Kocher, M.; Neupane, B.; Collette, S.; Tago, M.; Shaw, P.; Beyene, J.; Chang, E.L. Phase 3 Trials of Stereotactic Radiosurgery with or without Whole-Brain Radiation Therapy for 1 to 4 Brain Metastases: Individual Patient Data Meta-Analysis. Int. J. Radiat. Oncol. 2015, 91, 710–717. [Google Scholar] [CrossRef] [Green Version]
- Mulvenna, P.; Nankivell, M.; Barton, R.; Faivre-Finn, C.; Wilson, P.; McColl, E.; Moore, B.; Brisbane, I.; Ardron, D.; Holt, T.; et al. Dexamethasone and supportive care with or without whole brain radiotherapy in treating patients with non-small cell lung cancer with brain metastases unsuitable for resection or stereotactic radiotherapy (QUARTZ): Results from a phase 3, non-inferiority, randomised trial. Lancet 2016, 388, 2004–2014. [Google Scholar] [CrossRef]
- Chen, L.; Shen, C.; Redmond, K.J.; Page, B.; Kummerlowe, M.; Mcnutt, T.; Bettegowda, C.; Rigamonti, D.; Lim, M.; Kleinberg, L. Use of Stereotactic Radiosurgery in Elderly and Very Elderly Patients with Brain Metastases to Limit Toxicity Associated with Whole Brain Radiation Therapy. Int. J. Radiat. Oncol. Biol. Phys. 2017, 98, 939–947. [Google Scholar] [CrossRef]
- Higuchi, Y.; Yamamoto, M.; Serizawa, T.; Sato, Y.; Shuto, T.; Akabane, A.; Jokura, H.; Yomo, S.; Nagano, O.; Kawagishi, J.; et al. Stereotactic radiosurgery in elderly patients with brain metastases: Comparison with non-elderly patients using database of a multi-institutional prospective observational study (JLGK0901-Elderly). J. Neuro-Oncol. 2019, 144, 393–402. [Google Scholar] [CrossRef]
- Minniti, G.; Esposito, V.; Clarke, E.; Scaringi, C.; Bozzao, A.; Lanzetta, G.; De Sanctis, V.; Valeriani, M.; Osti, M.; Enrici, R.M. Stereotactic radiosurgery in elderly patients with brain metastases. J. Neuro-Oncol. 2013, 111, 319–325. [Google Scholar] [CrossRef]
- Yomo, S.; Hayashi, M. Is upfront stereotactic radiosurgery a rational treatment option for very elderly patients with brain metastases? A retrospective analysis of 106 consecutive patients age 80 years and older. BMC Cancer 2016, 16, 948. [Google Scholar] [CrossRef]
- Noordijk, E.M.; Vecht, C.J.; Haaxma-Reiche, H.; Padberg, G.W.; Voormolen, J.H.; Hoekstra, F.H.; Tans, J.T.; Lambooij, N.; Metsaars, J.A.; Wattendorff, A.; et al. The choice of treatment of single brain metastasis should be based on extracranial tumor activity and age. Int. J. Radiat. Oncol. 1994, 29, 711–717. [Google Scholar] [CrossRef]
- Nabors, L.B.; Portnow, J.; Ahluwalia, M.; Baehring, J.; Darlow, S.D. Central Nervous System Cancers, Version 3.2020, NCCN Clinical Practice Guidelines in Oncology. J. Natl. Compr. Cancer Netw. JNCCN 2020, 18, 1537–1570. [Google Scholar] [CrossRef]
- Aoyama, H.; Shirato, H.; Tago, M.; Nakagawa, K.; Toyoda, T.; Hatano, K.; Kenjyo, M.; Oya, N.; Hirota, S.; Shioura, H.; et al. Stereotactic Radiosurgery Plus Whole-Brain Radiation Therapy vs Stereotactic Radiosurgery Alone for Treatment of Brain Metastases: A randomized controlled trial. JAMA 2006, 295, 2483–2491. [Google Scholar] [CrossRef]
- Brown, P.D.; Jaeckle, K.; Ballman, K.V.; Farace, E.; Cerhan, J.H.; Anderson, S.K.; Carrero, X.W.; Barker, F.G.; Deming, R.; Burri, S.H.; et al. Effect of Radiosurgery Alone vs Radiosurgery with Whole Brain Radiation Therapy on Cognitive Function in Patients with 1 to 3 Brain Metastases: A Randomized Clinical Trial. JAMA 2016, 316, 401–409. [Google Scholar] [CrossRef]
- Chang, E.L.; Wefel, J.S.; Hess, K.R.; Allen, P.K.; Lang, F.F.; Kornguth, D.G.; Arbuckle, R.B.; Swint, J.M.; Shiu, A.S.; Maor, M.H.; et al. Neurocognition in patients with brain metastases treated with radiosurgery or radiosurgery plus whole-brain irradiation: A randomised controlled trial. Lancet Oncol. 2009, 10, 1037–1044. [Google Scholar] [CrossRef]
- Tsao, M.N.; Xu, W.; Wong, R.K.; Lloyd, N.; Laperriere, N.; Sahgal, A.; Rakovitch, E.; Chow, E. Whole brain radiotherapy for the treatment of newly diagnosed multiple brain metastases. Cochrane Database Syst. Rev. 2018, 1, CD003869. [Google Scholar] [CrossRef] [PubMed]
- Vogelbaum, M.A.; Brown, P.D.; Messersmith, H.; Brastianos, P.K.; Burri, S.; Cahill, D.; Dunn, I.F.; Gaspar, L.E.; Gatson, N.T.N.; Gondi, V.; et al. Treatment for Brain Metastases: ASCO-SNO-ASTRO Guideline. J. Clin. Oncol. 2022, 40, 492–516. [Google Scholar] [CrossRef] [PubMed]
- Soffietti, R.; Abacioglu, U.; Baumert, B.; Combs, S.E.; Kinhult, S.; Kros, J.M.; Marosi, C.; Metellus, P.; Radbruch, A.; Freixa, S.S.V.; et al. Diagnosis and treatment of brain metastases from solid tumors: Guidelines from the European Association of Neuro-Oncology (EANO). Neuro-Oncology 2017, 19, 162–174. [Google Scholar] [CrossRef] [PubMed]
- Patchell, R.A.; Tibbs, P.A.; Regine, W.F.; Dempsey, R.J.; Mohiuddin, M.; Kryscio, R.J.; Markesbery, W.R.; Foon, K.A.; Young, B. Postoperative Radiotherapy in the Treatment of Single Metastases to the Brain: A randomized trial. JAMA 1998, 280, 1485–1489. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Characteristics | Radiotherapy No. (%) | Surgery No. (%) | ||||||
|---|---|---|---|---|---|---|---|---|
| No (n = 380) | WBRT (n = 215) | SRS (n = 79) | WBRT + SRS (n = 40) | p-Value | No (n = 503) | Surgery (n = 211) | p-Value | |
| Age | ||||||||
| <65 years | 310 (81.6) | 181 (84.2) | 65 (82.3) | 32 (80) | 0.85 | 421 (83.7) | 167 (79.1) | 0.15 |
| ≥65 years | 70 (18.4) | 34 (15.8) | 14 (17.7) | 8 (20) | 82 (16.3) | 44 (20.9) | ||
| Gender | ||||||||
| Male | 246 (64.7) | 122 (56.7) | 55 (69.6) | 23 (57.5) | 0.11 | 305 (60.6) | 141 (66.8) | 0.12 |
| Female | 134 (35.3) | 93 (43.3) | 24 (30.4) | 17 (42.5) | 198 (39.4) | 70 (33.2) | ||
| History of smoking | ||||||||
| No | 221 (58.2) | 129 (60) | 42 (53.2) | 24 (60) | 0.76 | 290 (57.7) | 126 (59.7) | 0.61 |
| Yes | 159 (41.8) | 86 (40) | 37 (46.8) | 16 (40) | 213 (42.3) | 85 (40.3) | ||
| Pretreatment KPS | ||||||||
| ≤70 | 39 (10.3) | 18 (8.4) | 5 (6.3) | 0 (0) | 0.11 | 24 (4.8) | 38 (18) | <0.001 |
| >70 | 341 (89.7) | 197 (91.6) | 74 (93.7) | 40 (100) | 479 (95.2) | 173 (82) | ||
| Histology | ||||||||
| LUAD | 324 (85.3) | 198 (92.1) | 64 (81) | 32 (80) | 0.02 | 454 (90.3) | 164 (77.7) | <0.001 |
| Others | 56 (14.7) | 17 (7.9) | 15 (19) | 8 (20) | 49 (9.7) | 47 (22.3) | ||
| ALK/EGFR status | ||||||||
| WT | 130 (34.2) | 79 (36.7) | 36 (45.6) | 18 (45) | 0.40 | 182 (36.2) | 81 (38.4) | <0.001 |
| MT | 165 (43.4) | 94 (43.7) | 30 (38) | 17 (42.5) | 241 (47.9) | 65 (30.8) | ||
| NOS | 85 (22.4) | 42 (19.5) | 13 (16.5) | 5 (12.5) | 80 (15.9) | 65 (30.8) | ||
| Synchronous metastases | ||||||||
| No | 242 (63.7) | 145 (67.4) | 52 (65.8) | 31 (77.5) | 0.33 | 380 (75.5) | 90 (42.7) | <0.001 |
| Yes | 138 (36.3) | 70 (32.6) | 27 (34.2) | 9 (22.5) | 123 (24.5) | 121 (57.3) | ||
| Extracranial metastases | ||||||||
| No | 201 (52.9) | 99 (46) | 43 (54.4) | 21 (52.5) | 0.38 | 190 (37.8) | 174 (82.5) | <0.001 |
| Yes | 179 (47.1) | 116 (54) | 36 (45.6) | 19 (47.5) | 313 (62.2) | 37 (17.5) | ||
| Location of BMs | ||||||||
| Supratentorial | 292 (76.8) | 162 (75.3) | 60 (75.9) | 28 (70) | 0.83 | 381 (75.7) | 161 (76.3) | <0.001 |
| Subtentorial | 19 (5) | 12 (5.6) | 5 (6.3) | 1 (2.5) | 14 (2.8) | 23 (10.9) | ||
| Both | 69 (18.2) | 41 (19.1) | 14 (17.7) | 11 (27.5) | 108 (21.5) | 27 (12.8) | ||
| Number of BMs | ||||||||
| Single | 161 (42.4) | 82 (38.1) | 30 (38) | 16 (40) | 0.78 | 146 (29) | 143 (67.8) | <0.001 |
| Multiple | 219 (57.6) | 133 (61.9) | 49 (62) | 24 (60) | 357 (71) | 68 (32.2) | ||
| Surgery | ||||||||
| No | 248 (65.3) | 161 (74.9) | 59 (74.7) | 35 (87.5) | 0.004 | |||
| Yes | 132 (34.7) | 54 (25.1) | 20 (25.3) | 5 (12.5) | ||||
| Radiotherapy | / | |||||||
| No | 248 (49.3) | 132 (62.6) | 0.004 | |||||
| WBRT | 161 (32) | 54 (25.6) | ||||||
| SRS | 59 (11.7) | 20 (9.5) | ||||||
| WBRT + SRS | 35 (7) | 5 (2.4) | ||||||
| Characteristics | Level | Median OS (Month) | Logrank p-Value | Univariate Cox Regression | Multivariate Cox Regression | ||
|---|---|---|---|---|---|---|---|
| HR (95% CI) | p-Value | HR (95% CI) | p-Value | ||||
| Age | <65 years | 20.37 | 0.002 | Ref | Ref | ||
| ≥65 years | 15.67 | 1.39 (1.13–1.72) | 0.002 | 1.40 (1.13–1.73) | 0.002 | ||
| Gender | Male | 18.2 | 0.44 | Ref | |||
| Female | 20.57 | 0.94 (0.79–1.11) | 0.44 | ||||
| History of smoking | No | 20.6 | 0.06 | Ref | |||
| Yes | 17.07 | 1.17 (0.99–1.38) | 0.061 | ||||
| Pretreatment KPS | ≤70 | 11.83 | <0.001 | Ref | Ref | ||
| >70 | 20.37 | 0.49 (0.37–0.65) | <0.001 | 0.48 (0.36–0.64) | <0.001 | ||
| Histology | LUAD | 20.23 | 0.04 | Ref | Ref | ||
| Others | 16.7 | 1.29 (1.02–1.64) | 0.04 | 1.38 (1.07–1.78) | 0.01 | ||
| EGFR/ALK status | WT | 18.1 | Ref | Ref | |||
| MT | 23.67 | 0.008 | 0.78 (0.65–0.94) | 0.009 | 0.74 (0.61–0.89) | 0.002 | |
| Synchronous metastases | No | 19.57 | 0.75 | Ref | |||
| Yes | 18.1 | 1.03 (0.87–1.22) | 0.75 | ||||
| Extracranial metastases | No | 22.07 | <0.001 | Ref | Ref | ||
| Yes | 17.4 | 1.47 (1.25–1.74) | <0.001 | 1.45 (1.21–1.74) | <0.001 | ||
| Location of BMs | Supratentorial | 18.87 | Supratentorial vs. Subtentorial 0.45 | Ref | |||
| Subtentorial | 18.7 | Supratentorial vs. Both 0.93 | 0.87 (0.60–1.26) | 0.46 | |||
| Both | 20.87 | Subtentorial vs. Both 0.53 | 0.99 (0.80–1.22) | 0.92 | |||
| Number of BMs | Single | 20.17 | 0.08 | Ref | |||
| Multiple | 18.5 | 1.16 (0.98–1.37) | 0.08 | ||||
| Radiotherapy | No | 17.27 | No vs. WBRT 0.24 | Ref | Ref | ||
| WBRT | 19.33 | No vs. SRS 0.04 | 0.89 (0.74–1.07) | 0.22 | 0.84 (0.69–1.01) | 0.06 | |
| SRS | 28.2 | No vs. WBRT + SRS 0.001 | 0.75 (0.57–0.99) | 0.4 | 0.70 (0.53–0.92) | 0.01 | |
| WBRT + SRS | 28.87 | WBRT vs. SRS 0.222 | 0.51 (0.35–0.76) | 0.01 | 0.48 (0.32–0.71) | <0.001 | |
| WBRT vs. WBRT + SRS 0.009 | |||||||
| SRS vs. WBRT + SRS 0.092 | |||||||
| Surgery | No | 18.43 | 0.001 | Ref | Ref | ||
| Yes | 25.1 | 0.73 (0.61–0.88) | 0.001 | 0.65 (0.53–0.81) | <0.001 |
| Covariates | Level | Univariate Analysis | Multivariate Analysis | ||
|---|---|---|---|---|---|
| HR (95% CI) | p-Value | HR (95% CI) | p-Value | ||
| Age | <65 years | Ref | |||
| ≥65 years | 1.17 (0.84–1.63) | 0.34 | |||
| Gender | Male | Ref | |||
| Female | 0.95 (0.70–1.29) | 0.74 | |||
| History of smoking | No | Ref | |||
| Yes | 1.06 (0.82–1.39) | 0.65 | |||
| Pretreatment KPS | ≤70 | Ref | |||
| >70 | 0.79 (0.49–1.29) | 0.35 | |||
| History of smoking | LUAD | Ref | |||
| Others | 1.24 (0.87–1.76) | 0.24 | |||
| Synchronous metastases | No | Ref | |||
| Yes | 0.79 (0.69–1.05) | 0.10 | |||
| Extracranial metastases | No | Ref | Ref | ||
| Yes | 1.56 (1.20–2.05) | 0.001 | 1.44 (1.07–1.94) | 0.02 | |
| Location of BMs | Supratentorial | Ref | |||
| Subtentorial | 0.74 (0.43–1.28) | 0.29 | |||
| Both | 1.51 (1.08–2.12) | 0.17 | |||
| Number of BMs | Single | Ref | |||
| Multiple | 1.22 (0.93–1.59) | 0.15 | |||
| Radiotherapy | No | Ref | Ref | ||
| WBRT | 0.72 (0.53–0.97) | 0.03 | 0.67 (0.49–0.92) | 0.01 | |
| SRS | 0.64 (0.43–0.97) | 0.03 | 0.65 (0.43–0.99) | 0.04 | |
| WBRT + SRS | 0.60 (0.34–1.04) | 0.07 | 0.60 (0.34–1.05) | 0.07 | |
| Surgery | No | Ref | Ref | ||
| Yes | 0.69 (0.52–0.93) | 0.02 | 0.78 (0.56–1.08) | 0.14 | |
| Covariates | Level | Univariate Analysis | Multivariate Analysis | ||
|---|---|---|---|---|---|
| HR (95% CI) | p-Value | HR (95% CI) | p-Value | ||
| Age | <65 years | Ref | Ref | ||
| ≥65 years | 1.44 (1.07–1.95) | 0.02 | 1.45 (1.07–2.00) | 0.02 | |
| Gender | Male | Ref | |||
| Female | 0.94 (0.75–1.18) | 0.59 | |||
| History of smoking | No | Ref | |||
| Yes | 1.17 (0.93–1.47) | 0.14 | |||
| Pretreatment KPS | ≤70 | Ref | Ref | ||
| >70 | 0.48 (0.30–0.75) | 0.001 | 0.53 (0.33–0.85) | 0.008 | |
| Histology | LUAD | Ref | |||
| Others | 1.27 (0.87–1.86) | 0.22 | |||
| Synchronous metastases | No | Ref | |||
| Yes | 1.23 (0.96–1.54) | 0.11 | |||
| ALK/EGFR status | WT | Ref | Ref | ||
| MT | 0.71 (0.55–0.91) | 0.006 | 0.73 (0.57–0.94) | 0.02 | |
| NOS | 1.29 (0.93–1.80) | 0.13 | 1.32 (0.95–1.84) | 0.10 | |
| Location of BMs | Supratentorial | Ref | |||
| Subtentorial | 1.34 (0.73–2.46) | 0.34 | |||
| Both | 0.79 (0.60–1.05) | 0.10 | |||
| Number of BMs | Single | Ref | |||
| Multiple | 0.93 (0.72–1.19) | 0.55 | |||
| Radiotherapy | No | Ref | Ref | ||
| WBRT | 0.73 (0.59–0.96) | 0.03 | 0.74 (0.58–0.95) | 0.02 | |
| SRS | 0.71 (0.49–1.04) | 0.08 | 0.72 (0.49–1.06) | 0.09 | |
| WBRT + SRS | 0.50 (0.29–0.86) | 0.01 | 0.50 (0.29–0.87) | 0.01 | |
| Surgery | No | Ref | |||
| Yes | 1.20 (0.83–1.73) | 0.34 | |||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Liang, L.; Wang, Z.; Duan, H.; He, Z.; Lu, J.; Jiang, X.; Hu, H.; Li, C.; Yu, C.; Zhong, S.; et al. Survival Benefits of Radiotherapy and Surgery in Lung Cancer Brain Metastases with Poor Prognosis Factors. Curr. Oncol. 2023, 30, 2227-2236. https://doi.org/10.3390/curroncol30020172
Liang L, Wang Z, Duan H, He Z, Lu J, Jiang X, Hu H, Li C, Yu C, Zhong S, et al. Survival Benefits of Radiotherapy and Surgery in Lung Cancer Brain Metastases with Poor Prognosis Factors. Current Oncology. 2023; 30(2):2227-2236. https://doi.org/10.3390/curroncol30020172
Chicago/Turabian StyleLiang, Lun, Zhenning Wang, Hao Duan, Zhenqiang He, Jie Lu, Xiaobing Jiang, Hongrong Hu, Chang Li, Chengwei Yu, Sheng Zhong, and et al. 2023. "Survival Benefits of Radiotherapy and Surgery in Lung Cancer Brain Metastases with Poor Prognosis Factors" Current Oncology 30, no. 2: 2227-2236. https://doi.org/10.3390/curroncol30020172