Conversion in a Resectable Tumor after Denosumab Neoadjuvant in a Large Dorsal Giant Cells Tumor: A Case Report and a Literature Review

Abstract
:1. Introduction
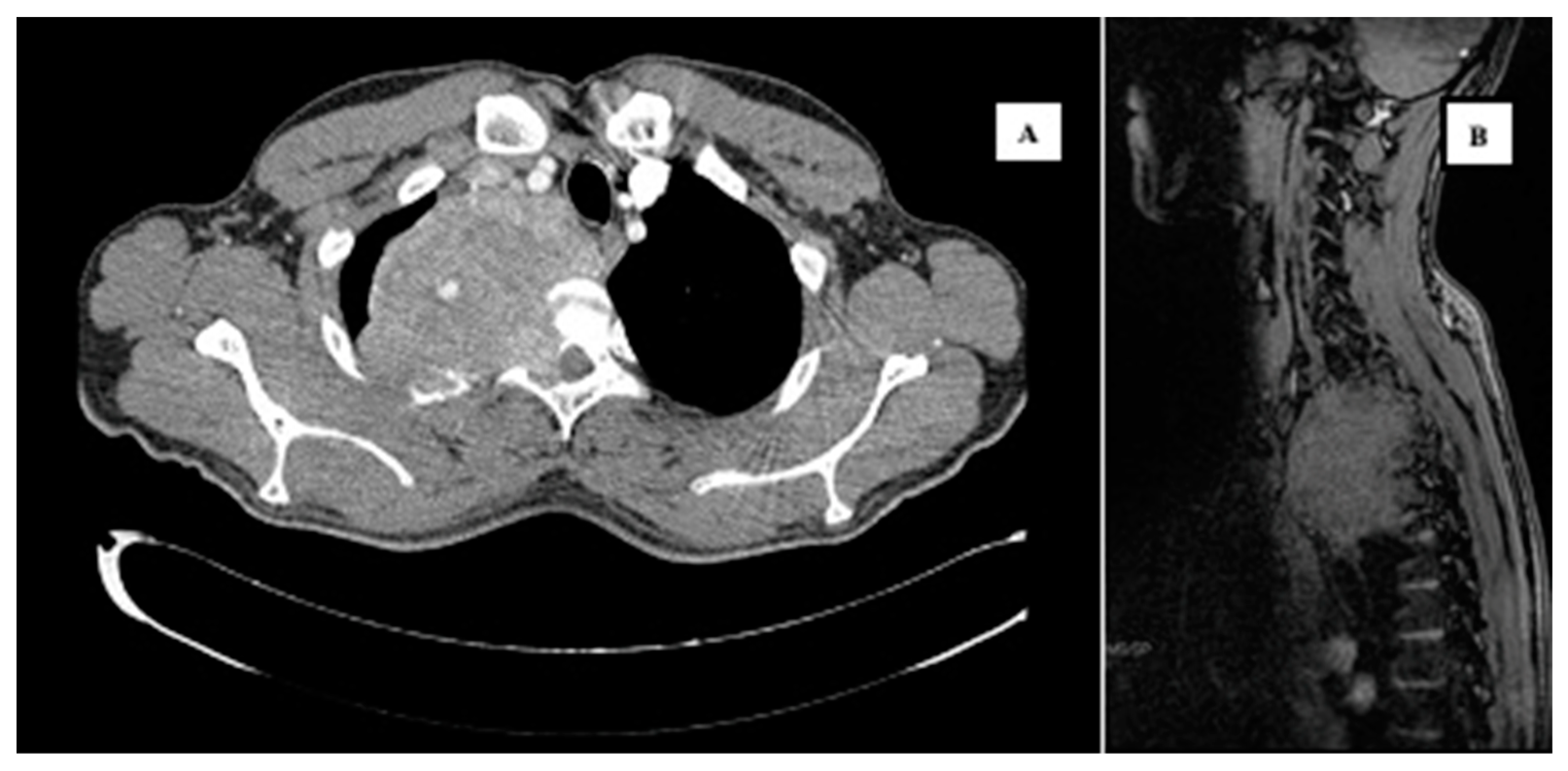
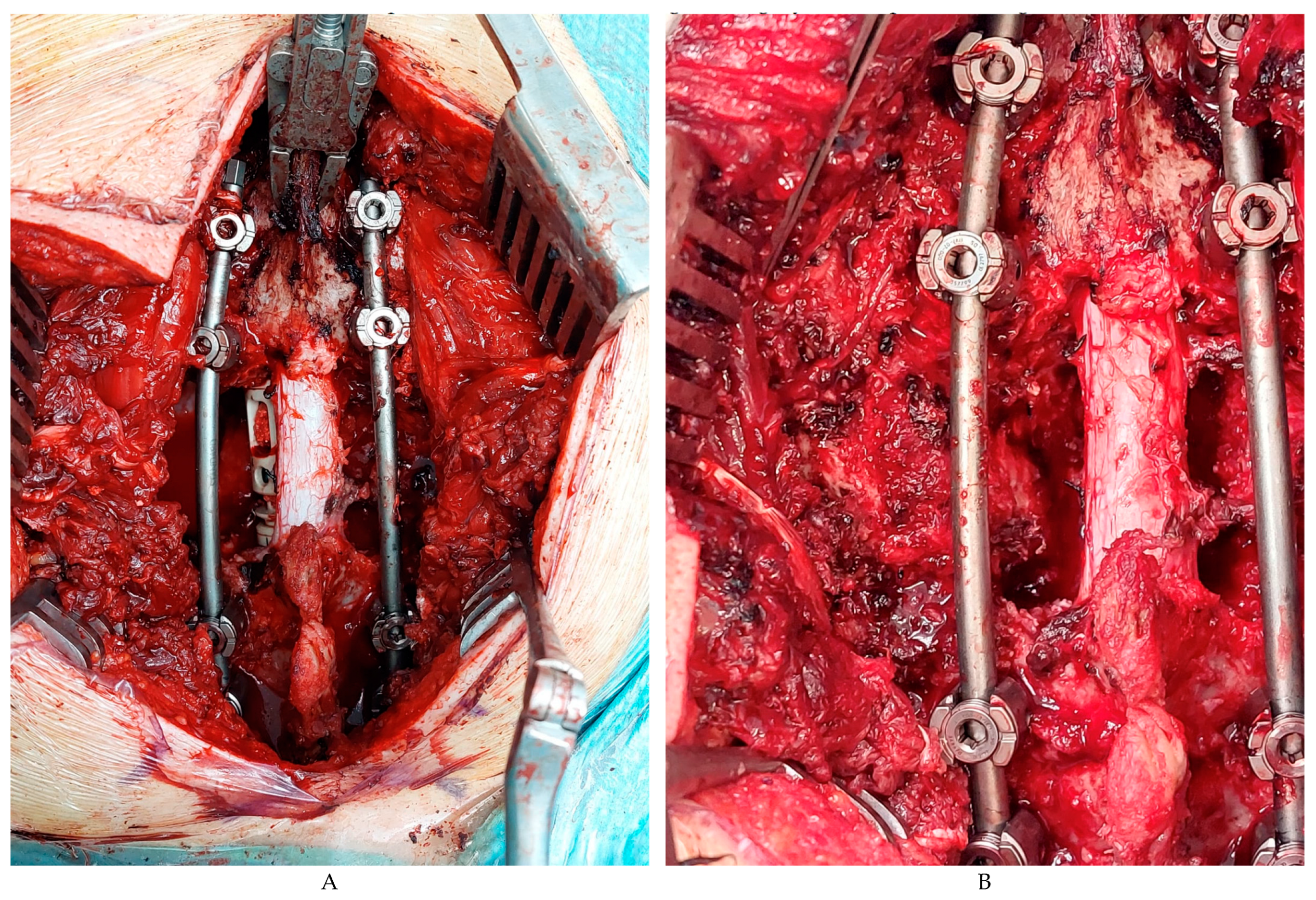
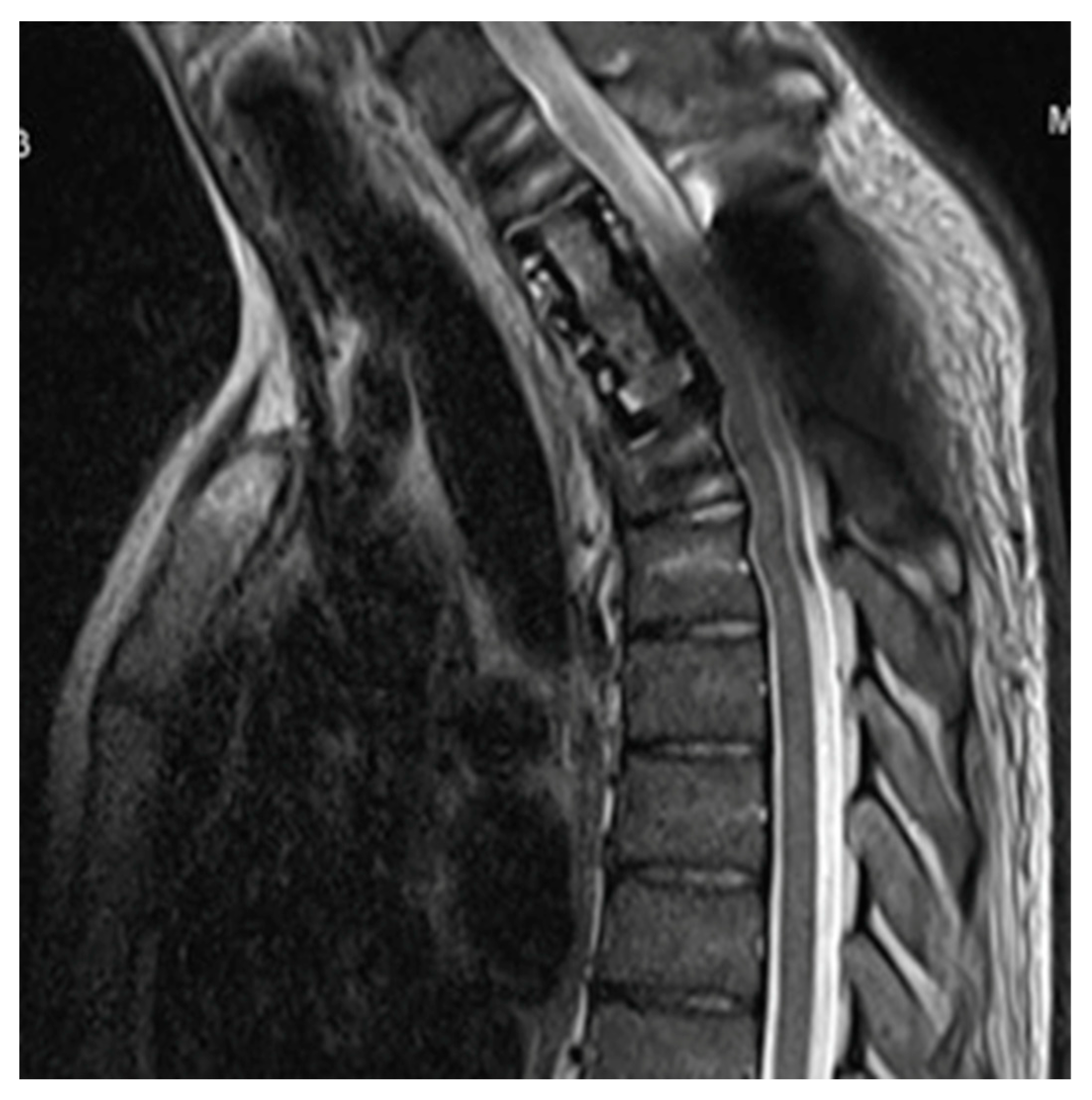
2. Case Report
3. Discussion
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| BGCT | Bone giant cell tumors |
| SGTC | Spine giant cell tumors |
| RANK | Receptor Activator of Nuclear Factor κ B |
| RANK-L | Receptor Activator of Nuclear Factor κ B Ligand |
| RT | Radiation therapy |
| AD | Adjuvant |
| NA | Neoadjuvant |
| FDA | US Food and Drug Administration |
| EMA | European Medicines Agency |
| CT | Computerized tomography |
| PET CT | Positron emission tomography computerized tomography |
References
- Del Baena-Ocampo, L.C.; Ramirez-Perez, E.; Linares-Gonzalez, L.M.; Delgado-Chavez, R. Epidemiology of bone tumors in Mexico City: Retrospective clinicopathologic study of 566 patients at a referral institution. Ann. Diagn. Pathol. 2009, 13, 16–21. [Google Scholar] [CrossRef] [PubMed]
- Amelio, J.M.; Rockberg, J.; Hernandez, R.K.; Sobocki, P.; Stryker, S.; Bach, B.A.; Engellau, J.; Liede, A. Population-based study of giant cell tumor of bone in Sweden (1983–2011). Cancer Epidemiol. 2016, 42, 82–89. [Google Scholar] [CrossRef] [PubMed]
- Rendina, D.; Mossetti, G.; Soscia, E.; Sirignano, C.; Insabato, L.; Viceconti, R.; Ignarra, R.; Salvatore, M.; Nunziata, V. Giant cell tumor and Paget’s disease of bone in one family: Geographic clustering. Clin. Orthop. Relat. Res. 2004, 421, 212–218. [Google Scholar] [CrossRef] [PubMed]
- Li, H.; Gao, J.; Gao, Y.; Lin, N.; Zheng, M.; Ye, Z. Denosumab in Giant Cell Tumor of Bone: Current Status and Pitfalls. Front. Oncol. 2020, 10, 580605. [Google Scholar] [CrossRef]
- Campanacci, M.; Baldini, N.; Boriani, S.; Sudanese, A. Giant-cell tumor of bone. J. Bone Joint Surg. Am. 1987, 69, 106–114. [Google Scholar] [CrossRef]
- Boriani, S.; Bandiera, S.; Casadei, R.; Boriani, L.; Donthineni, R.; Gasbarrini, A. Giant cell tumor of the mobile spine: A review of 49 cases. Spine 2012, 37, E37–E45. [Google Scholar] [CrossRef]
- Boriani, S.; Bandiera, S.; Donthineni, R.; Amendola, L.; Cappuccio, M.; De Iure, F. Morbidity of en bloc resections in the spine. Eur. Spine J. 2010, 19, 231–241. [Google Scholar] [CrossRef]
- Rock, M.G.; Sim, F.H.; Unni, K.K.; Witrak, G.A.; Frassica, F.J.; Schray, M.F.; Beabout, J.W.; Dahlin, D.C. Secondary malignant giant-cell tumor of bone. Clinicopathological assessment of nineteen patients. J. Bone Joint Surg. Am. 1986, 68, 1073–1079. [Google Scholar] [CrossRef]
- Chawla, S.; Henshaw, R.; Seeger, L.; Choy, E.; Blay, J.Y.; Ferrari, S.; Kroep, J.; Grimer, R.; Reichardt, P.; Rutkowski, P.; et al. Safety and efficacy of Denosumab for adults and skeletally mature adolescents with giant cell tumor of bone: Interim analysis of an open-label, parallel-group, phase 2 study. Lancet Oncol. 2013, 14, 901–908. [Google Scholar] [CrossRef]
- Harding, D.; Giles, S.L.; Brown, M.R.D.; Ter Haar, G.R.; van den Bosch, M.; Bartels, L.W.; Kim, Y.S.; Deppe, M.; deSouza, N.M. Evaluation of Quality of Life Outcomes Following Palliative Treatment of Bone Metastases with Magnetic Resonance-guided High Intensity Focused Ultrasound: An International Multicentre Study. Clin. Oncol. R. Coll. Radiol. 2018, 30, 233–242. [Google Scholar] [CrossRef]
- Bongiovanni, A.; Foca, F.; Oboldi, D.; Diano, D.; Bazzocchi, A.; Fabbri, L.; Mercatali, L.; Vanni, S.; Maltoni, M.; Bianchini, D.; et al. 3-T magnetic resonance-guided high-intensity focused ultrasound (3 T-MR-HIFU) for the treatment of pain from bone metastases of solid tumors. Support. Care Cancer. 2022, 30, 5737–5745. [Google Scholar] [CrossRef] [PubMed]
- Napoli, A.; Anzidei, M.; Marincola, B.C.; Brachetti, G.; Ciolina, F.; Cartocci, G.; Marsecano, C.; Zaccagna, F.; Marchetti, L.; Cortesi, E.; et al. Primary pain palliation and local tumor control in bone metastases treated with magnetic resonance-guided focused ultrasound. Invest. Radiol. 2013, 48, 351–358. [Google Scholar] [CrossRef] [PubMed]
- Tsai, Y.C.; Lee, H.L.; Kuo, C.C.; Chen, C.Y.; Hsieh, K.L.; Wu, M.H.; Wen, Y.C.; Yu, H.W.; Hsu, F.C.; Tsai, J.T.; et al. Prognostic and predictive factors for clinical and radiographic responses in patients with painful bone metastasis treated with magnetic resonance-guided focused ultrasound surgery. Int. J. Hyperthermia. 2019, 1, 932–937. [Google Scholar] [CrossRef] [PubMed]
- Gaston, C.L.; Grimer, R.J.; Parry, M.; Stacchiotti, S.; Dei Tos, A.P.; Gelderblom, H.; Ferrari, S.; Baldi, G.G.; Jones, R.L.; Chawla, S.; et al. Current status and unanswered questions on the use of Denosumab in giant cell tumor of bone. Clin. Sarcoma Res. 2016, 6, 15. [Google Scholar] [CrossRef]
- Liede, A.; Bach, B.A.; Stryker, S.; Hernandez, R.K.; Sobocki, P.; Bennett, B.; Wong, S.S. Regional variation and challenges in estimating the incidence of giant cell tumor of bone. J. Bone Joint Surg. Am. 2014, 96, 1999–2007. [Google Scholar] [CrossRef]
- Goldschlager, T.; Dea, N.; Boyd, M.; Reynolds, J.; Patel, S.; Rhines, L.D.; Mendel, E.; Pacheco, M.; Ramos, E.; Mattei, T.A.; et al. Giant cell tumors of the spine: Has Denosumab changed the treatment paradigm? J. Neurosurg. Spine 2015, 22, 526–533. [Google Scholar] [CrossRef]
- Caudell, J.J.; Ballo, M.T.; Zagars, G.K.; Lewis, V.O.; Weber, K.L.; Lin, P.P.; Marco, R.A.; El-Naggar, A.K.; Benjamin, R.S.; Yasko, A.W. Radiotherapy in the management of giant cell tumor of bone. Int. J. Radiat. Oncol. Biol. Phys. 2013, 57, 158–165. [Google Scholar] [CrossRef]
- Atkins, G.J.; Kostakis, P.; Vincent, C.; Farrugia, A.N.; Houchins, J.P.; Findlay, D.M.; Evdokiou, A.; Zannettino, A.C. RANK expression as a cell surface marker of human osteoclast precursors in peripheral blood, bone marrow, and giant cell tumors of bone. J. Bone Miner. Res. 2006, 21, 1339–1349. [Google Scholar] [CrossRef]
- Thomas, D.; Henshaw, R.; Skubitz, K.; Chawla, S.; Staddon, A.; Blay, J.Y.; Roudier, M.; Smith, J.; Ye, Z.; Sohn, W.; et al. Denosumab in patients with giant-cell tumor of bone: An open-label, phase 2 study. Lancet Oncol. 2010, 11, 275–280. [Google Scholar] [CrossRef]
- Xará-Leite, F.; Coutinho, L.; Fleming, C.; Magalhães, M.; Oliveira, V.; Rodrigues-Pinto, R.; Cardoso, P. Can Denosumab cure giant cell tumors of the spine? A case report and literature review. Eur. J. Orthop. Surg. Traumatol. 2020, 30, 19. [Google Scholar] [CrossRef]
- Rutkowski, P.; Ferrari, S.; Grimer, R.J.; Stalley, P.D.; Dijkstra, S.P.; Pienkowski, A.; Vaz, G.; Wunder, J.S.; Seeger, L.L.; Feng, A.; et al. Surgical downstaging in an open-label phaseII trial of Denosumab in patients with giant cell tumor of bone. Ann. Surg. Oncol. 2015, 22, 2860–2868. [Google Scholar] [CrossRef] [PubMed]
- De Vita, A.; Vanni, S.; Miserocchi, G.; Fausti, V.; Pieri, F.; Spadazzi, C.; Cocchi, C.; Liverani, C.; Calabrese, C.; Casadei, R.; et al. A Rationale for the Activity of Bone Target Therapy and Tyrosine Kinase Inhibitor Combination in Giant Cell Tumor of Bone and Desmoplastic Fibroma: Translational Evidences. Biomedicines. 2022, 10, 372. [Google Scholar] [CrossRef] [PubMed]
- Dubory, A.; Missenard, G.; Domont, J.; Court, C. Interest of Denosumab for the Treatment of Giant-cells Tumors and Aneurysmal Bone Cysts of the Spine. About Nine Cases. Spine 2016, 41, E654–E660. [Google Scholar] [CrossRef] [PubMed]
- Hindiskere, S.; Errani, C.; Doddarangappa, S.; Ramaswamy, V.; Rai, M.; Chinder, P.S. Is a short-course of preoperative Denosumab as effective as prolonged therapy for giant cell tumor of bone? Clin. Orthop. Relat. Res. 2020; Epub ahead of print. [Google Scholar]
- Errani, C.; Tsukamoto, S.; Mavrogenis, A.F. How safe and effective is Denosumab for bone giant cell tumor? Int. Orthop. 2017, 41, 2397–2400. [Google Scholar] [CrossRef] [PubMed]
- Yang, Y.; Li, Y.; Liu, W.; Xu, H.; Niu, X. A nonrandomized controlled study of sacral giant cell tumors with preoperative treatment of denosumab. Medicine 2018, 97, e13139. [Google Scholar] [CrossRef]
- Traub, F.; Singh, J.; Dickson, B.C.; Leung, S.; Mohankumar, R.; Blackstein, M.E.; Razak, A.R.; Griffin, A.M.; Ferguson, P.C.; Wunder, J.S. Efficacy of Denosumab in joint preservation for patients with giant cell tumor of the bone. Eur. J. Cancer 2016, 59, 1–12. [Google Scholar] [CrossRef]
- Errani, C.; Tsukamoto, S.; Leone, G.; Righi, A.; Akahane, M.; Tanaka, Y.; Donati, D.M. Denosumab may increase the risk of local recurrence in patients with giant cell tumor of bone treated with curettage. J. Bone Joint Surg. Am. 2018, 100, 496–504. [Google Scholar] [CrossRef]
- Behjati, S.; Tarpey, P.S.; Presneau, N.; Scheipl, S.; Pillay, N.; Van Loo, P.; Wedge, D.C.; Cooke, S.L.; Gundem, G.; Davies, H.; et al. Distinct H3F3A and H3F3B driver mutations define chondroblastoma and giant cell tumor of bone. Nat. Genet. 2013, 45, 1479–1482. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Author’s | Study | N of Patients | Location | Resectability | Treatment | Pathology |
|---|---|---|---|---|---|---|
| Thomas et al. [15] | Serial cases | 37 | Spine and other locations | Unresectable, recurrent disease | Denosumab: loading dose and monthly dose | 100% biopsies and 66% radiological responses |
| Goldschlager T [16] | Case report | 1 | T9 | Potential resectable | Neoadjuvant and adjuvant Denosumab 9 months | Complete response |
| Rutkowski P [17] | Phase II | 222 | Spine and other locations | 116 patients | Neoadjuvant Denosumab | 99 complete response 17 recurrence (median TTR 13.6 m) |
| Chawla et al. [9] | Phase II | 282 | Spine and other locations | Cohort 1: resectable Cohort 2: unresectable | Cohort 1: neoadjuvant Denosumab and 6 months adjuvant Denosumab Cohort 2: Denosumab till progression | Cohort 1: 5% complete response Cohort 2: radiological 18% complete response |
| Dubory et al. [18] | Serial cases | 9 | Spine and other locations | Resectable or potentially resectable | Neoadjuvant Denosumab | 10% complete response |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sereno, M.; Franco, S.R.; de la Reina, L.; Campo-Cañaveral de la Cruz, J.L.; Muñoz de Legaría, M.; Casado Saénz, E. Conversion in a Resectable Tumor after Denosumab Neoadjuvant in a Large Dorsal Giant Cells Tumor: A Case Report and a Literature Review. Curr. Oncol. 2023, 30, 9335-9345. https://doi.org/10.3390/curroncol30100675
Sereno M, Franco SR, de la Reina L, Campo-Cañaveral de la Cruz JL, Muñoz de Legaría M, Casado Saénz E. Conversion in a Resectable Tumor after Denosumab Neoadjuvant in a Large Dorsal Giant Cells Tumor: A Case Report and a Literature Review. Current Oncology. 2023; 30(10):9335-9345. https://doi.org/10.3390/curroncol30100675
Chicago/Turabian StyleSereno, María, Silvia Roa Franco, Laura de la Reina, José Luis Campo-Cañaveral de la Cruz, Marta Muñoz de Legaría, and Enrique Casado Saénz. 2023. "Conversion in a Resectable Tumor after Denosumab Neoadjuvant in a Large Dorsal Giant Cells Tumor: A Case Report and a Literature Review" Current Oncology 30, no. 10: 9335-9345. https://doi.org/10.3390/curroncol30100675