In-Clinic versus Hybrid Cancer Rehabilitation Service Delivery during the COVID-19 Pandemic: An Outcome Comparison Study


Abstract
:1. Introduction
2. Materials and Methods
2.1. Cancer Rehabilitation Service Delivery
2.2. Case Identification and Data Extraction
2.3. Outcome Measures
2.3.1. Patient-Reported Outcome Measures
2.3.2. Patient Experience Measures
2.4. Statistical Analysis
3. Results
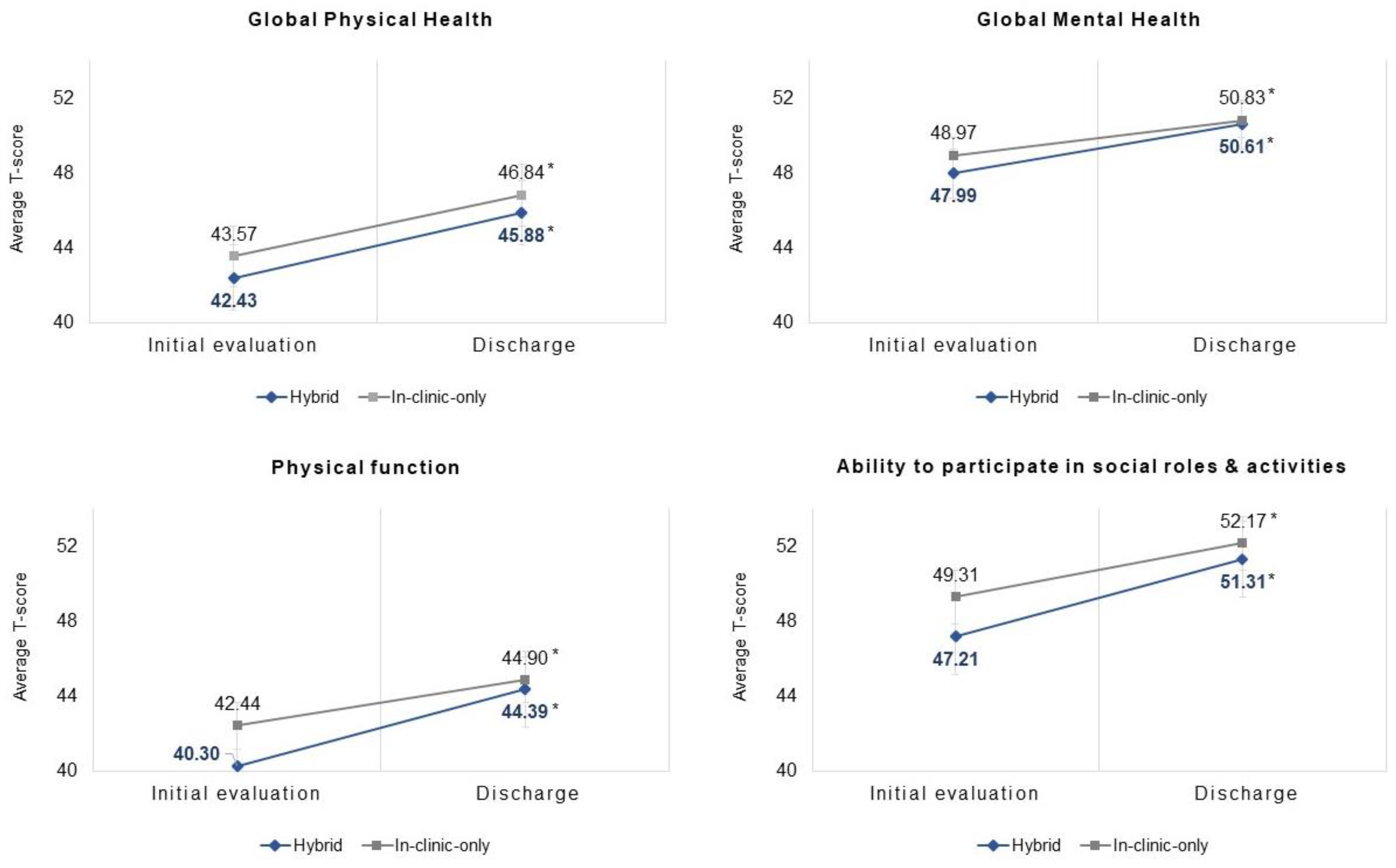
3.1. PROMIS® HRQOL Measures
3.2. Patient-Reported Experience Measures (PREM)
4. Discussion
4.1. Limitations
4.2. Implications for Clinical Practice and Future Directions
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Richmond, T.; Peterson, C.; Cason, J.; Billings, M.; Terrell, E.A.; Lee, A.C.W.; Towey, M.; Parmanto, B.; Saptono, A.; Cohn, E.R.; et al. American Telemedicine Association’s Principles for Delivering Telerehabilitation Services. Int. J. Telerehabilitation 2017, 9, 63. [Google Scholar] [CrossRef] [PubMed]
- Jette, A.M. The Promise and Potential of Telerehabilitation in Physical Therapy. Phys. Ther. 2021, 101, pzab081. [Google Scholar] [CrossRef]
- Lee, A.; Finnin, K.; Holdsworth, L.; Millette, D.; Peterson, C. Report of the World Confederation for Physical Therapy/International Network of Physiotherapy Regulatory Authorities Digital Physical Therapy Practice Task Force. 2020, pp. 1–24. Available online: https://world.physio/sites/default/files/2020-06/WCPT-INPTRA-Digital-Physical-Therapy-Practice-Task-force-March2020.pdf (accessed on 1 June 2023).
- Siegel, R.L.; Miller, K.D.; Fuchs, H.E.; Jemal, A. Cancer statistics, 2022. CA Cancer J. Clin. 2022, 72, 7–33. [Google Scholar] [CrossRef] [PubMed]
- Mazariego, C.G.; Juraskova, I.; Campbell, R.; Smith, D.P. Long-term unmet supportive care needs of prostate cancer survivors: 15-year follow-up from the NSW Prostate Cancer Care and Outcomes Study. Support. Care Cancer 2020, 28, 5511–5520. [Google Scholar] [CrossRef] [PubMed]
- Lisy, K.; Langdon, L.; Piper, A.; Jefford, M. Identifying the most prevalent unmet needs of cancer survivors in Australia: A systematic review. Asia-Pac. J. Clin. Oncol. 2019, 15, e68–e78. [Google Scholar] [CrossRef] [PubMed]
- Vu, J.V.T.; Matusko, N.; Hendren, S.; Regenbogen, S.E.; Hardiman, K.M. Patient-Reported Unmet Needs in Colorectal Cancer Survivors After Treatment for Curative-Intent. Dis. Colon Rectum 2019, 62, 815. [Google Scholar] [CrossRef] [PubMed]
- Pergolotti, M.; Deal, A.M.; Lavery, J.; Reeve, B.B.; Muss, H.B. The prevalence of potentially modifiable functional deficits and the subsequent use of occupational and physical therapy by older adults with cancer. J. Geriatr. Oncol. 2015, 6, 194–201. [Google Scholar] [CrossRef] [PubMed]
- Cespedes Feliciano, E.M.; Vasan, S.; Luo, J.; Binder, A.M.; Rowan, S.; Chlebowski, T.; Quesenberry, C.; Banack, H.R.; Caan, B.J.; Paskett, E.D.; et al. Long-term Trajectories of Physical Function Decline in Women with and Without Cancer. JAMA Oncol. 2023, 9, 395–403. [Google Scholar] [CrossRef]
- Cheville, A.L.; Kornblith, A.B.; Basford, J.R. An examination of the causes for the underutilization of rehabilitation services among people with advanced cancer. Am. J. Phys. Med. Rehabil. 2011, 90 (Suppl. 1), S27–S37. [Google Scholar] [CrossRef]
- Pergolotti, M.; Deal, A.M.; Williams, G.R.; Bryant, A.L.; McCarthy, L.; Nyrop, K.A.; Covington, K.R.; Reeve, B.B.; Basch, E.; Muss, H.B. Older Adults with Cancer: A Randomized Controlled Trial of Occupational and Physical Therapy. J. Am. Geriatr. Soc. 2019, 67, 953–960. [Google Scholar] [CrossRef]
- Lopez, C.J.; Edwards, B.; Langelier, D.M.; Chang, E.K.; Chafranskaia, A.; Jones, J.M. Delivering virtual cancer rehabilitation programming during the first 90 days of the COVID-19 pandemic: A multimethod study. Arch. Phys. Med. Rehabil. 2021, 102, 1283–1293. [Google Scholar] [CrossRef] [PubMed]
- Loubani, K.; Schreuer, N.; Kizony, R. Telerehabilitation for Managing Daily Participation among Breast Cancer Survivors during COVID-19: A Feasibility Study. J. Clin. Med. 2022, 11, 1022. [Google Scholar] [CrossRef] [PubMed]
- Loubani, K.; Kizony, R.; Milman, U.; Schreuer, N. Hybrid Tele and In-Clinic Occupation Based Intervention to Improve Women’s Daily Participation after Breast Cancer: A Pilot Randomized Controlled Trial. Int. J. Environ. Res. Public Health 2021, 18, 5966. [Google Scholar] [CrossRef]
- Morrison, K.S.; Paterson, C.; Toohey, K. The Feasibility of Exercise Interventions Delivered via Telehealth for People Affected by Cancer: A Rapid Review of the Literature. Semin. Oncol. Nurs. 2020, 36, 151092. [Google Scholar] [CrossRef] [PubMed]
- Dennett, A.; Harding, K.E.; Reimert, J.; Morris, R.; Parente, P.; Taylor, N.F. Telerehabilitation’s Safety, Feasibility, and Exercise Uptake in Cancer Survivors: Process Evaluation. JMIR Cancer 2021, 7, e33130. [Google Scholar] [CrossRef] [PubMed]
- Zheng, J.; Hou, M.; Liu, L.; Wang, X. Knowledge Structure and Emerging Trends of Telerehabilitation in Recent 20 Years: A Bibliometric Analysis via CiteSpace. Front. Public Health 2022, 10, 904855. [Google Scholar] [CrossRef]
- Chang, P.J.; Jay, G.M.; Kalpakjian, C.; Andrews, C.; Smith, S. Patient and Provider-Reported Satisfaction of Cancer Rehabilitation Telemedicine Visits during the COVID-19 Pandemic. PM R 2021, 13, 1362–1368. [Google Scholar] [CrossRef]
- Keikha, L.; Maserat, E.; Mohammadzadeh, Z. Telerehabilitation and Monitoring Physical Activity in Patient with Breast Cancer: Systematic Review. Iran. J. Nurs. Midwifery Res. 2022, 27, 8. [Google Scholar] [CrossRef]
- Wu, F.; Rotimi, O.; Laza Cagigas, R.; Rampal, T. The Feasibility and Effects of a Telehealth-Delivered Home-Based Prehabilitation Program for Cancer Patients during the Pandemic. Curr. Oncol. 2021, 28, 2248–2259. [Google Scholar] [CrossRef]
- Brick, R.; Padgett, L.; Jones, J.; Wood, K.C.; Pergolotti, M.; Marshall, T.F.; Campbell, G.; Eilers, R.; Keshavarzi, S.; Flores, A.M.; et al. The influence of telehealth-based cancer rehabilitation interventions on disability: A systematic review. J. Cancer Surviv. 2022, 17, 1725–1750. [Google Scholar] [CrossRef]
- Pearl, R.; Wayling, B. The Telehealth Era Is Just Beginning: More Gains in Quality, Affordability, and Accessibility Are on the Way. Harvard Business Review. 2022. Available online: https://hbr.org/2022/05/the-telehealth-era-is-just-beginning (accessed on 1 June 2023).
- Dickinson, R.; Hall, S.; Sinclair, J.E.; Bond, C.; Murchie, P. Using technology to deliver cancer follow-up: A systematic review. BMC Cancer 2014, 14, 311. [Google Scholar] [CrossRef]
- Kaye, R.; Rosen-zvi, M.; Ron, R. Digitally-Enabled Remote Care for Cancer Patients: Here to Stay. Semin. Oncol. Nurs. 2020, 36, 151091. [Google Scholar] [CrossRef]
- Saaei, F.; Klappa, S.G. Rethinking Telerehabilitation: Attitudes of Physical Therapists and Patients. J. Patient Exp. 2021, 8, 23743735211034335. [Google Scholar] [CrossRef]
- Van De Poll-Franse, L.V.; De Rooij, B.H.; Horevoorts, N.J.E.; May, A.M.; Vink, G.R.; Koopman, M.; Van Laarhoven, H.W.M.; Besselink, M.G.; Oerlemans, S.; Husson, O.; et al. Perceived Care and Well-being of Patients with Cancer and Matched Norm Participants in the COVID-19 Crisis: Results of a Survey of Participants in the Dutch PROFILES Registry. JAMA Oncol. 2021, 7, 279–284. [Google Scholar] [CrossRef] [PubMed]
- Ackroyd, S.A.; Walls, M.; Kim, J.S.; Lee, N.K. Lessons learned: Telemedicine patterns and clinical application in patients with gynecologic cancers during COVID-19. Gynecol. Oncol. Rep. 2022, 41, 100986. [Google Scholar] [CrossRef] [PubMed]
- Zhang, H.; Cha, E.E.; Lynch, K.; Cahlon, O.; Gomez, D.R.; Shaverdian, N.; Gillespie, E.F. Radiation Oncologist Perceptions of Telemedicine from Consultation to Treatment Planning: A Mixed-Methods Study. Int. J. Radiat. Oncol. 2020, 108, 421–429. [Google Scholar] [CrossRef]
- Motheral, B.; Brooks, J.; Clark, M.A.; Crown, W.H.; Davey, P.; Hutchins, D.; Martin, B.C.; Stang, P. A Checklist for Retrospective Database Studies—Report of the ISPOR Task Force on Retrospective Databases. Value Health 2003, 6, 90–97. [Google Scholar] [CrossRef] [PubMed]
- Cella, D.; Yount, S.; Rothrock, N.; Gershon, R.; Cook, K.; Reeve, B.; Ader, D.; Fries, J.F.; Bruce, B.; Rose, M.; et al. The Patient-Reported Outcomes Measurement Information System (PROMIS): Progress of an NIH Roadmap cooperative group during its first two years. Med. Care 2007, 45, S3–S11. [Google Scholar] [CrossRef] [PubMed]
- Al Obaidi, M.; Giri, S.; Mir, N.; Kenzik, K.; McDonald, A.M.; Smith, C.Y.; Gbolahan, O.B.; Paluri, R.K.; Bhatia, S.; Williams, G.R. Use of self-rated health to identify frailty and predict mortality in older adults with cancer. Results from the care study. J. Clin. Oncol. 2020, 38, 12046. [Google Scholar] [CrossRef]
- Williams, G.R.; Deal, A.M.; Sanoff, H.K.; Nyrop, K.A.; Guerard, E.J.; Pergolotti, M.; Shachar, S.S.; Reeve, B.B.; Bensen, J.T.; Choi, S.K.; et al. Frailty and health-related quality of life in older women with breast cancer. Support. Care Cancer 2019, 27, 2693–2698. [Google Scholar] [CrossRef]
- Polo, K.M.; Moore, E.S.; Sommers, S.H. Exploring the Impact of the Occupational Therapy Health and Wellness Program (OT-HAWP) on Performance and the Health-Related Quality of Life of Cancer Survivors. Occup. Ther. Health Care 2021, 36, 168–183. [Google Scholar] [CrossRef] [PubMed]
- Pergolotti, M.; Covington, K.R.; Lightner, A.N.; Bertram, J.; Thess, M.; Sharp, J.; Spraker, M.; Williams, G.R.; Manning, P. Association of Outpatient Cancer Rehabilitation with Patient-Reported Outcomes and Performance-Based Measures of Function. Rehabil. Oncol. 2021, 39, 137–142. [Google Scholar] [CrossRef]
- Terwee, C.B.; Peipert, J.D.; Chapman, R.; Lai, J.S.; Terluin, B.; Cella, D.; Griffith, P.; Mokkink, L.B. Minimal important change (MIC): A conceptual clarification and systematic review of MIC estimates of PROMIS measures. Qual. Life Res. 2021, 30, 2729–2754. [Google Scholar] [CrossRef]
- Adams, C.; Walpola, R.; Schembri, A.M.; Harrison, R. The ultimate question? Evaluating the use of Net Promoter Score in healthcare: A systematic review. Health Expect. 2022, 25, 2328–2339. [Google Scholar] [CrossRef]
- Cook, C.E.; Pergolotti, M.; Garcia, A.N.; Hopwood, D. Creation and Validation of the Select Medical Patient Reported Experience Measure (SM-PREM©) for physical and occupational therapy outpatient clinics. Arch. Phys. Med. Rehabil. 2023. [Google Scholar] [CrossRef] [PubMed]
- Klepps, R. NPS® in Health Care: Leveraging Loyal Patients to Drive New Business and Improve Revenue. In WebPT. Available online: https://www.webpt.com/blog/nps-in-health-care-leveraging-loyal-patients-to-drive-new-business-and-improve-revenue/ (accessed on 1 June 2023).
- Wood, K.C.; Bertram, J.J.; Kendig, T.D.; Pergolotti, M. Understanding Patient Experience with Outpatient Cancer Rehabilitation Care. Healthcare 2023, 11, 348. [Google Scholar] [CrossRef] [PubMed]
- Guo, Y.; Ding, L.; Miao, X.; Jiang, X.; Xu, T.; Xu, X.; Zhu, S.; Xu, Q.; Hu, J. Effects of prehabilitation on postoperative outcomes in frail cancer patients undergoing elective surgery: A systematic review and meta-analysis. Support. Care Cancer 2023, 31, 1–14. [Google Scholar] [CrossRef]
- Helm, E.E.; Crowley, B.; Crowell, T.L.; Galantino, M. Lou Effect of Telerehabilitation Versus In-Clinic Rehabilitation Delivery on Self-Efficacy in Breast Cancer–Related Lymphedema. Rehabil. Oncol. 2023, 41, 82–88. [Google Scholar] [CrossRef]
- Moffet, H.; Tousignant, M.; Nadeau, S.; Mérette, C.; Boissy, P.; Corriveau, H.; Marquis, F.; Cabana, F.; Belzile, É.L.; Ranger, P.; et al. Patient Satisfaction with In-Home Telerehabilitation After Total Knee Arthroplasty: Results from a Randomized Controlled Trial. Telemed. e-Health 2017, 23, 80–87. [Google Scholar] [CrossRef]
- Kim, B.I.; Peairs, E.; Lander, S.; Antonelli, C.; Lau, B.C. Telehealth Physical Therapy for Sports Medicine Rehabilitation What Is Its Role in the Postpandemic Era? Orthop. J. Sports Med. 2022, 10, 23259671221127721. [Google Scholar] [CrossRef]
- Brennan, K.; Curran, J.; Barlow, A.; Jayaraman, A. Telerehabilitation in neurorehabilitation: Has it passed the COVID test? Expert Rev. Neurother. 2021, 21, 833–836. [Google Scholar] [CrossRef] [PubMed]
- Harper, K.J.; Fitzgerald, S.; Xiyin, P.; Kuzich, J.; Leow, S.H.; Biostat, A.J.M.; Harris, C. Does the Integration of Telehealth into Occupational Therapy Practice Impact Clinical Outcomes for Hand and Upper Limb Rehabilitation? A Matched Case Control Study. Int. J. Telerehabilitation 2022, 14. [Google Scholar] [CrossRef]
- Pergolotti, M.; Covington, K.R.; Lightner, A.N.; Bertram, J.; Thess, M.; Sharp, J.L.; Spraker, M.B.; Williams, G.R.; Manning, P. Outpatient cancer rehabilitation to improve patient reported and objective measures of function. J. Clin. Oncol. 2020, 38, e19325. [Google Scholar] [CrossRef]


{kind=link}
| Hybrid (n = 60) | In-Clinic Only (n = 2551) | Between-Group Comparison, p-Value | |
|---|---|---|---|
| Age (Mean ± SD) | 59.92 ± 13.08 | 60.82 ± 12.90 | 0.53 |
| Sex (N, %) | 0.63 | ||
| Female | 50, 83.3 | 2047, 80.2 | |
| Male | 10, 16.7 | 504, 19.8 | |
| Cancer type (N, %) | 0.40 | ||
| Breast | 34, 56.7 | 1270, 57.6 | |
| Gastrointestinal, genitourinary, colorectal, or gynecologic | 9, 15.0 | 334, 13.1 | |
| Heme or lymphoid | 8, 13.3 | 177, 6.9 | |
| Other | 7, 11.7 | 294, 11.5 | |
| U.S. Region (N, %) | <0.001 * | ||
| Midwest | 5, 8.3 | 294, 11.5 | |
| Northeast | 29, 48.3 | 456, 17.9 | |
| South | 13, 21.7 | 1173, 46.0 | |
| Southeast | 10, 16.7 | 466, 18.0 | |
| West | 3, 5.0 | 162, 6.4 | |
| Payer type (N, %) | 0.97 | ||
| Federally funded | 1223, 47.9 | 28, 46.7 | |
| Private | 1279, 50.1 | 31, 51.7 | |
| Other | 49, 1.9 | 1, 1.7 | |
| Rehabilitation discipline (N, %) | 0.80 | ||
| Physical Therapy | 53, 88.3 | 2219, 87.0 | |
| Occupational Therapy | 7, 11.7 | 332, 13.0 | |
| Length of care, weeks (Median, IQR) | 14.79 (10.18, 26.21) | 9.00 (5.42, 14.14) | <0.001 * |
| Visits (Median, IQR) | 18.00 (10.0, 23.5) | 10.00 (6.00, 16.00) | <0.001 * |
| Outcome Measure | Unadjusted Model | Adjusted Model * | ||
|---|---|---|---|---|
| β, 95% CI | p-Value | Β (95% CI) | p-Value | |
| Global physical health | 0.19 (−1.67, 2.06) | 0.840 | −0.17 (−2.05, 1.71) | 0.857 |
| Global mental health | 0.76 (−1.07, 2.60) | 0.415 | 0.73 (−1.14, 2.60) | 0.445 |
| Physical function | 1.63 (−0.33, 3.58) | 0.103 | 1.16 (−0.799, 3.13) | 0.245 |
| Ability to participate in social roles and activities | 1.24 (−1.17, 3.65) | 0.312 | 0.51 (−1.93, 2.95) | 0.682 |
| Outcome Measure | Unadjusted Model | Adjusted Model * | ||
|---|---|---|---|---|
| Odds Ratio, 95% CI | p-Value | Odds Ratio, 95% CI | p-Value | |
| Global physical health | 1.07 (0.63–1.8) | 0.794 | 0.85 (0.49–1.49) | 0.574 |
| Global mental health | 0.84 (0.50–1.41) | 0.507 | 1.19 (0.69–2.04) | 0.694 |
| Physical function | 1.52 (0.74–2.31) | 0.130 | 1.45 (0.80–2.63) | 0.215 |
| Ability to participate in social roles and activities | 0.91 (0.53–1.57) | 0.739 | 1.03 (0.57–1.85) | 0.931 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wood, K.C.; Giri, S.; Kendig, T.D.; Pergolotti, M. In-Clinic versus Hybrid Cancer Rehabilitation Service Delivery during the COVID-19 Pandemic: An Outcome Comparison Study. Curr. Oncol. 2023, 30, 8916-8927. https://doi.org/10.3390/curroncol30100644
Wood KC, Giri S, Kendig TD, Pergolotti M. In-Clinic versus Hybrid Cancer Rehabilitation Service Delivery during the COVID-19 Pandemic: An Outcome Comparison Study. Current Oncology. 2023; 30(10):8916-8927. https://doi.org/10.3390/curroncol30100644
Chicago/Turabian StyleWood, Kelley C., Smith Giri, Tiffany D. Kendig, and Mackenzi Pergolotti. 2023. "In-Clinic versus Hybrid Cancer Rehabilitation Service Delivery during the COVID-19 Pandemic: An Outcome Comparison Study" Current Oncology 30, no. 10: 8916-8927. https://doi.org/10.3390/curroncol30100644