
Smoking, Lung Cancer Stage, and Prognostic Factors—Findings from the National Lung Screening Trial

Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Outcome Variables
2.3. Statistical Methods
3. Results
3.1. Study Sample
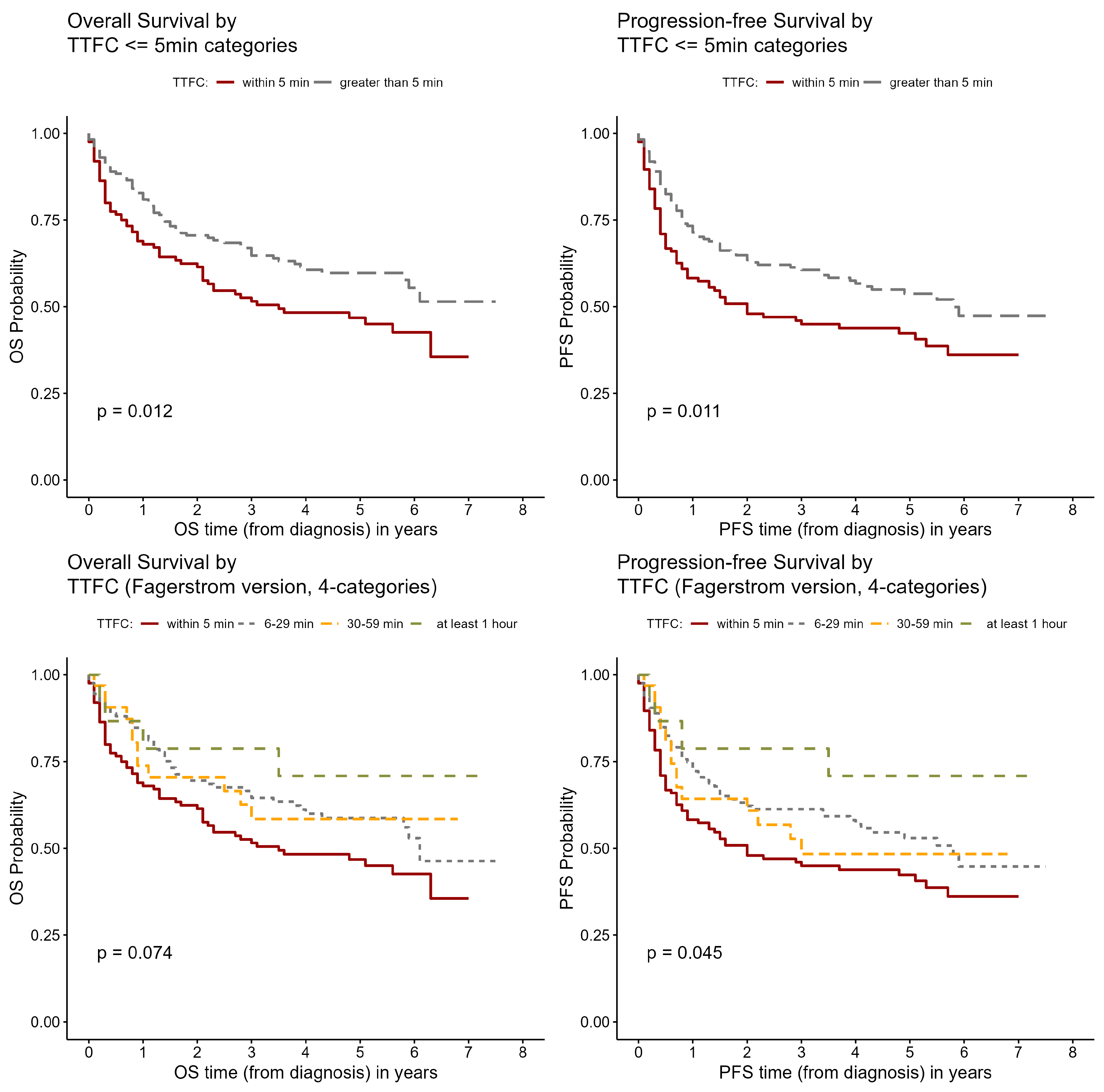
3.2. Survival Time Analysis
3.3. Multivariate Results
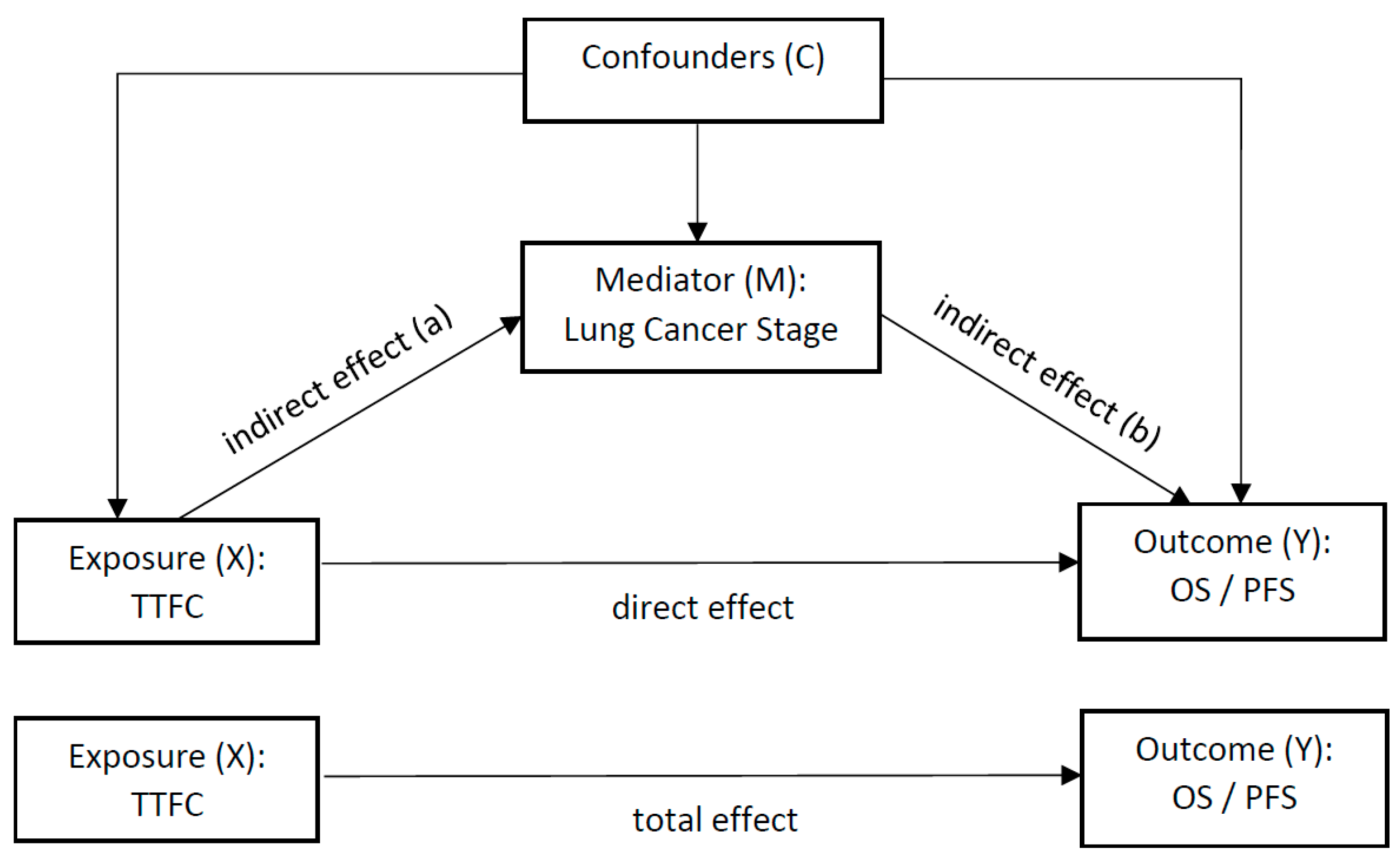
3.4. Mediation Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Chen, V.W.; Ruiz, B.A.; Hsieh, M.C.; Wu, X.C.; Ries, L.A.; Lewis, D.R. Analysis of stage and clinical/prognostic factors for lung cancer from SEER registries: AJCC staging and collaborative stage data collection system. Cancer 2014, 120 (Suppl. S23), 3781–3792. [Google Scholar] [CrossRef]
- Caini, S.; Del Riccio, M.; Vettori, V.; Scotti, V.; Martinoli, C.; Raimondi, S.; Cammarata, G.; Palli, D.; Banini, M.; Masala, G.; et al. Quitting smoking at or around diagnosis improves the overall survival of lung cancer patients: A systematic review and meta-analysis. J. Thorac. Oncol. 2021, 17, 623–636. [Google Scholar] [CrossRef] [PubMed]
- National Lung Screening Trial Researc Team; Church, T.R.; Black, W.C.; Aberle, D.R.; Berg, C.D.; Clingan, K.L.; Duan, F.; Fagerstrom, R.M.; Gareen, I.F.; Gierada, D.S.; et al. Results of initial low-dose computed tomographic screening for lung cancer. N. Engl. J. Med. 2013, 368, 1980–1991. [Google Scholar] [CrossRef] [PubMed]
- National Lung Screening Trial Researc Team; Aberle, D.R.; Adams, A.M.; Berg, C.D.; Black, W.C.; Clapp, J.D.; Fagerstrom, R.M.; Gareen, I.F.; Gatsonis, C.; Marcus, P.M.; et al. Reduced lung-cancer mortality with low-dose computed tomographic screening. N. Engl. J. Med. 2011, 365, 395–409. [Google Scholar] [CrossRef] [PubMed]
- Muscat, J.E.; Ahn, K.; Richie, J.P., Jr.; Stellman, S.D. Nicotine dependence phenotype and lung cancer risk. Cancer 2011, 117, 5370–5376. [Google Scholar] [CrossRef]
- Gu, F.; Wacholder, S.; Kovalchik, S.; Panagiotou, O.A.; Reyes-Guzman, C.; Freedman, N.D.; De Matteis, S.; Consonni, D.; Bertazzi, P.A.; Bergen, A.W.; et al. Time to smoke first morning cigarette and lung cancer in a case-control study. J. Natl. Cancer Inst. 2014, 106, dju118. [Google Scholar] [CrossRef] [PubMed]
- Ito, H.; Gallus, S.; Hosono, S.; Oze, I.; Fukumoto, K.; Yatabe, Y.; Hida, T.; Mitsudomi, T.; Negri, E.; Yokoi, K.; et al. Time to first cigarette and lung cancer risk in Japan. Ann. Oncol. 2013, 24, 2870–2875. [Google Scholar] [CrossRef]
- Muscat, J.E.; Ahn, K.; Richie, J.P., Jr.; Stellman, S.D. Nicotine dependence phenotype, time to first cigarette, and risk of head and neck cancer. Cancer 2011, 117, 5377–5382. [Google Scholar] [CrossRef]
- Muscat, J.E.; Liu, H.P.; Livelsberger, C.; Richie, J.P., Jr.; Stellman, S.D. The nicotine dependence phenotype, time to first cigarette, and larynx cancer risk. Cancer Causes Control 2012, 23, 497–503. [Google Scholar] [CrossRef]
- Thomas, S.; Carroll, J.C.; Brown, M.C.; Chen, Z.; Mirshams, M.; Patel, D.; Boyd, K.; Pierre, A.; Goldstein, D.P.; Giuliani, M.E.; et al. Nicotine dependence as a risk factor for upper aerodigestive tract (UADT) cancers: A mediation analysis. PLoS ONE 2020, 15, e0237723. [Google Scholar] [CrossRef]
- Pezzuto, A.; Citarella, F.; Croghan, I.; Tonini, G. The effects of cigarette smoking extracts on cell cycle and tumor spread: Novel evidence. Future Sci. OA 2019, 5, FSO394. [Google Scholar] [CrossRef] [PubMed]
- American Joint Committee on Cancer. AJCC Cancer Staging Manual, 6th ed.; Springer: New York, NY, USA, 2002. [Google Scholar]
- World Health Organization. International Classification of Diseases for Oncology, 3rd ed.; World Health Organization: Geneva, Switzerland, 2000.
- Heatherton, T.F.; Kozlowski, L.T.; Frecker, R.C.; Fagerstrom, K.O. The Fagerstrom Test for Nicotine Dependence: A revision of the Fagerstrom Tolerance Questionnaire. Br. J. Addict. 1991, 86, 1119–1127. [Google Scholar] [CrossRef] [PubMed]
- Woodard, G.A.; Jones, K.D.; Jablons, D.M. Lung Cancer Staging and Prognosis. Cancer Treat. Res. 2016, 170, 47–75. [Google Scholar] [CrossRef] [PubMed]
- Tingley, D.; Yamamoto, T.; Hirose, K.; Keele, L.; Imai, K. R package for causal mediation analysis. J. Stat. Softw. 2014, 595, 1–38. [Google Scholar]
- Ganti, A.K.; Klein, A.B.; Cotarla, I.; Seal, B.; Chou, E. Update of Incidence, Prevalence, Survival, and Initial Treatment in Patients With Non-Small Cell Lung Cancer in the US. JAMA Oncol. 2021, 7, 1824–1832. [Google Scholar] [CrossRef] [PubMed]
- Pineiro, B.; Simmons, V.N.; Palmer, A.M.; Correa, J.B.; Brandon, T.H. Smoking cessation interventions within the context of Low-Dose Computed Tomography lung cancer screening: A systematic review. Lung Cancer 2016, 98, 91–98. [Google Scholar] [CrossRef] [PubMed]
- Gu, F.; Cheung, L.C.; Freedman, N.D.; Katki, H.A.; Caporaso, N.E. Potential Impact of Including Time to First Cigarette in Risk Models for Selecting Ever-Smokers for Lung Cancer Screening. J. Thorac. Oncol. 2017, 12, 1646–1653. [Google Scholar] [CrossRef] [PubMed]
- Van Overmeire, I.P.; De Smedt, T.; Dendale, P.; Nackaerts, K.; Vanacker, H.; Vanoeteren, J.F.; Van Laethem, D.M.; Van Loco, J.; De Cremer, K.A. Nicotine Dependence and Urinary Nicotine, Cotinine and Hydroxycotinine Levels in Daily Smokers. Nicotine Tob. Res. 2016, 18, 1813–1819. [Google Scholar] [CrossRef] [PubMed]
- Muscat, J.E.; Stellman, S.D.; Caraballo, R.S.; Richie, J.P., Jr. Time to first cigarette after waking predicts cotinine levels. Cancer Epidemiol. Biomark. Prev. 2009, 18, 3415–3420. [Google Scholar] [CrossRef]
- Fu, M.; Martinez-Sanchez, J.M.; Agudo, A.; Pascual, J.A.; Borras, J.M.; Samet, J.M.; Fernandez, E.; Investigators, D.S. Association between time to first cigarette after waking up and salivary cotinine concentration. Nicotine Tob. Res. 2011, 13, 168–172. [Google Scholar] [CrossRef]
- Branstetter, S.A.; Muscat, J.E. Time to first cigarette and 4-(methylnitrosamino)-1-(3-pyridyl)-1-butanol (NNAL) levels in adult smokers; National Health and Nutrition Examination Survey (NHANES), 2007–2010. Cancer Epidemiol. Biomark. Prev. 2013, 22, 615–622. [Google Scholar] [CrossRef]
- Warren, G.W.; Singh, A.K. Nicotine and lung cancer. J. Carcinog. 2013, 12, 1. [Google Scholar] [CrossRef]
- Grando, S.A. Connections of nicotine to cancer. Nat. Rev. Cancer 2014, 14, 419–429. [Google Scholar] [CrossRef]
- Stone, E.; Marshall, H. Tobacco cessation in lung cancer screening-do we have the evidence? Transl. Lung Cancer Res. 2018, 7 (Suppl. S3), S270–S274. [Google Scholar] [CrossRef] [PubMed]
- Slatore, C.G.; Gould, M.K.; Au, D.H.; Deffebach, M.E.; White, E. Lung cancer stage at diagnosis: Individual associations in the prospective VITamins and lifestyle (VITAL) cohort. BMC Cancer 2011, 11, 228. [Google Scholar] [CrossRef]
- Forrest, L.F.; Sowden, S.; Rubin, G.; White, M.; Adams, J. Socio-economic inequalities in stage at diagnosis, and in time intervals on the lung cancer pathway from first symptom to treatment: Systematic review and meta-analysis. Thorax 2017, 72, 430–436. [Google Scholar] [CrossRef] [PubMed]
- National Lung Screening Trial Research, T.; Aberle, D.R.; Berg, C.D.; Black, W.C.; Church, T.R.; Fagerstrom, R.M.; Galen, B.; Gareen, I.F.; Gatsonis, C.; Goldin, J.; et al. The National Lung Screening Trial: Overview and study design. Radiology 2011, 258, 243–253. [Google Scholar] [CrossRef] [PubMed]
- Higuchi, R.; Goto, T.; Nakagomi, T.; Hirotsu, Y.; Oyama, T.; Amemiya, K.; Mochizuki, H.; Omata, M. Discrimination Between Primary Lung Cancer and Lung Metastases by Genomic Profiling. JTO Clin. Res. Rep. 2021, 2, 100255. [Google Scholar] [CrossRef]
- Tsai, L.L.; Chu, N.Q.; Blessing, W.A.; Moonsamy, P.; Colson, Y.L. Lung Cancer in Women. Ann. Thorac. Surg. 2021, 114, 1956–1973. [Google Scholar] [CrossRef]
- Marijon, H.; Bouyon, A.; Vignot, S.; Besse, B. Facteurs pronostiques et predictifs des cancers bronchiques [Prognostic and predictive factors in lung cancer]. Bull. Cancer 2009, 96, 391–404. [Google Scholar] [CrossRef]
- Petrelli, F.; Cortellini, A.; Indini, A.; Tomasello, G.; Ghidini, M.; Nigro, O.; Salati, M.; Dottorini, L.; Iaculli, A.; Varricchio, A.; et al. Association of Obesity with Survival Outcomes in Patients with Cancer: A Systematic Review and Meta-analysis. JAMA Netw. Open 2021, 4, e213520. [Google Scholar] [CrossRef] [PubMed]
- Lennon, H.; Sperrin, M.; Badrick, E.; Renehan, A.G. The Obesity Paradox in Cancer: A Review. Curr. Oncol. Rep. 2016, 18, 56. [Google Scholar] [CrossRef] [PubMed]
- Winer, E.S.; Cervone, D.; Bryant, J.; McKinney, C.; Liu, R.T.; Nadorff, M.R. Distinguishing Mediational Models and Analyses in Clinical Psychology: Atemporal Associations Do Not Imply Causation. J. Clin. Psychol. 2016, 72, 947–955. [Google Scholar] [CrossRef] [PubMed]
- Yuan, P.; Cao, J.L.; Rustam, A.; Zhang, C.; Yuan, X.S.; Bao, F.C.; Lv, W.; Hu, J. Time-to-Progression of NSCLC from Early to Advanced Stages: An Analysis of data from SEER Registry and a Single Institute. Sci. Rep. 2016, 6, 28477. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Variable | Statistics Type or Categories | Summarization |
|---|---|---|
| Age | Mean (SD) | 63.7 (5.6) |
| Sex | Female | 124 (41.5%) |
| Male | 175 (58.5%) | |
| Race | White | 280 (93.6%) |
| Black | 14 (4.7%) | |
| Other | 5 (1.7%) | |
| Ethnicity | Hispanic or Latino | 2 (0.7%) |
| Neither Hispanic nor Latino | 296 (99.3%) | |
| Education | High school or less | 93 (32.7%) |
| Some college | 118 (41.5%) | |
| Bachelor or higher | 73 (25.7%) | |
| Married or live together | Yes | 178 (59.7%) |
| BMI Categories | Underweight (BMI < 18.5) | 6 (2%) |
| Normal (18.5 ≤ BMI < 25) | 97 (32.7%) | |
| Overweight (25 ≤ BMI < 30) | 127 (42.8%) | |
| Obese (BMI ≥ 30) | 67 (22.6%) | |
| Smoking Status | Former Smokers | 120 (40.1%) |
| Current Smokers | 179 (59.9%) | |
| Any family history of lung cancer | Yes | 70 (23.4%) |
| No | 229 (76.6%) | |
| Lung Cancer stage | Early stage (1A-3A) | 193 (69.4%) |
| Advanced stage (3B-4) | 85 (30.6%) | |
| Lesion size of tumor in mm | Mean (SD) | 26.3 (20.5) |
| Lung Cancer Histology | Small cell LC | 34 (11.4%) |
| Non-small cell LC | 265 (88.6%) | |
| Lung Cancer Grade | 1 or 2 | 99 (47.6%) |
| 3 or 4 | 109 (52.4%) |
| Exposure Variables | OS | PFS |
|---|---|---|
| Tumor characteristics | ||
| Lung cancer stage: Advanced vs. early stage | 7.2 (4.94–10.6), p < 0.0001 * | 7.4 (5.18–10.7), p < 0.0001 * |
| Lung cancer histology: small cell vs. non-small cell | 3.6 (2.32–5.71), p < 0.0001 * | 3.5 (2.24–5.35), p < 0.0001 * |
| Lung cancer grade: 3/4 vs. 1/2 | 4.2 (2.51–6.91), p < 0.0001 * | 3.3 (2.07–5.18), p < 0.0001 * |
| Lesion size in mm (Continuous) | 1.03 (1.02–1.04), p < 0.0001 * | 1.03 (1.02–1.04), p < 0.0001 * |
| Personal characteristics/smoking | ||
| Sex: male vs. female | 1.5 (1.06–2.21), p = 0.0231 * | 1.4 (1–1.98), p = 0.0488 * |
| Age (continuous) | 0.99 (0.961–1.02), p = 0.61 | 0.98 (0.953–1.01), p = 0.22 |
| Race: Black vs. White | 1.0 (0.46–2.37), p = 0.9165 | 1.0 (0.474–2.17), p = 0.9737 |
| BMI: over weight vs. normal weight | 0.96 (0.631–1.45), p = 0.8353 | 1.1 (0.726–1.6), p = 0.7068 |
| BMI: obese vs. normal weight | 1.6 (0.982–2.47), p = 0.0597 | 1.7 (1.09–2.61), p = 0.0191 * |
| Any family history of lung cancer: yes vs. no | 1.3 (0.849–1.88), p = 0.2492 | 1.3 (0.916–1.92), p = 0.1346 |
| Smoking status: current vs. former smokers | 1.5 (1.02–2.12), p = 0.0373 * | 1.3 (0.935–1.84), p = 0.1165 |
| Smoking duration in years | 1.01 (0.99–1.04), p = 0.264 | 1.01 (0.99–1.04), p = 0.264 |
| Cigarettes per day (>1 pack vs. ≤1 pack) | 1.2 (0.84–1.72), p = 0.3124 | 1.24 (0.89–1.73), p = 0.2106 |
| Time to first cigarette (TTFC): ≤5 min vs. longer | 1.56 (1.1–2.2), p = 0.013 * | 1.53 (1.1–2.12), p = 0.01 * |
| TTFC (4 categories): ≤5 min vs. at least 1 h | 2.4 (0.859–6.49), p = 0.096 | 2.8 (1.02–7.63), p = 0.047 * |
| TTFC (4 categories): 6–29 min vs. at least 1 h | 1.6 (0.57–4.38), p = 0.380 | 1.9 (0.676–5.14), p = 0.229 |
| TTFC (4 categories): 30–59 min vs. at least 1 h | 1.5 (0.497–4.78), p = 0.454 | 2.1 (0.691–6.28), p = 0.193 |
| Predictor Variables | OS | PFS |
|---|---|---|
| Lung cancer stage: advanced vs. early stage | 7.2 (4.81–10.7), p < 0.0001 * | 7.5 (5.11–11.0), p < 0.0001 * |
| Sex: male vs. female | 1.7 (1.14–2.47), p = 0.0094 * | 1.5 (1.01–2.08), p = 0.0434 * |
| BMI: obese vs. normal weight | NA | 1.7 (1.09–2.75), p = 0.0209 * |
| Smoking status: current vs. former smokers | 1.3 (0.911–1.98), p = 0.136 | 1.3 (0.893–1.87), p = 0.1736 |
| Time to first cigarette (TTFC): ≤5 min vs. longer | 1.0 (0.687–1.46), p = 0.991 | 1.1 (0.753–1.52), p = 0.71 |
| OS | PFS | |||||
|---|---|---|---|---|---|---|
| Estimate | 95% CI | p | Estimate | 95% CI | p | |
| ACME | −746.47 | −1478, −115 | 0.02 * | −563.01 | −1135, −68 | 0.025 * |
| ADE | 62.29 | −1352, 1594 | 0.96 | −194.27 | −1234, 902 | 0.699 |
| TE | −684.18 | −2235, 886 | 0.38 | −757.28 | −1923, 410 | 0.192 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zhu, J.; Branstetter, S.; Lazarus, P.; Muscat, J.E. Smoking, Lung Cancer Stage, and Prognostic Factors—Findings from the National Lung Screening Trial. Int. J. Environ. Res. Public Health 2024, 21, 400. https://doi.org/10.3390/ijerph21040400
Zhu J, Branstetter S, Lazarus P, Muscat JE. Smoking, Lung Cancer Stage, and Prognostic Factors—Findings from the National Lung Screening Trial. International Journal of Environmental Research and Public Health. 2024; 21(4):400. https://doi.org/10.3390/ijerph21040400
Chicago/Turabian StyleZhu, Junjia, Steven Branstetter, Philip Lazarus, and Joshua E. Muscat. 2024. "Smoking, Lung Cancer Stage, and Prognostic Factors—Findings from the National Lung Screening Trial" International Journal of Environmental Research and Public Health 21, no. 4: 400. https://doi.org/10.3390/ijerph21040400