
Is There Somebody Looking out for Me? A Qualitative Analysis of Bullying Experiences of Individuals Diagnosed with Bipolar Disorder


Abstract
:1. Introduction
1.1. Navigating Bipolar Disorder in the Workplace: Challenges, Accommodations, and Societal Attitudes
1.2. Aim of the Current Research: Underexplored Risk of Bullying against Employees with Bipolar Disorder
2. Methods
2.1. Participants
2.2. Participant Recruitment Process
2.3. Interview Protocol and Process
2.4. Procedure and Data Analysis
3. Results
3.1. Various Forms of Negative Behaviours
3.2. Underlying Causes of Workplace Bullying
“The bully doesn’t have his own goals. He chose a profession he doesn’t like. He works at a job he dislikes or has no respect for his work. He finds pleasure in torturing people and being authoritarian. Or he’s just bored and has nothing else to do.”
“It depends on the character of the person. If there is no problem with his character, he already understands how the disease impacts us. However, if a person’s character is flawed, he will engage in bullying. He can mock others’ flaws, regardless of whether they have bipolar disorder, are healthy, or physically disabled.”
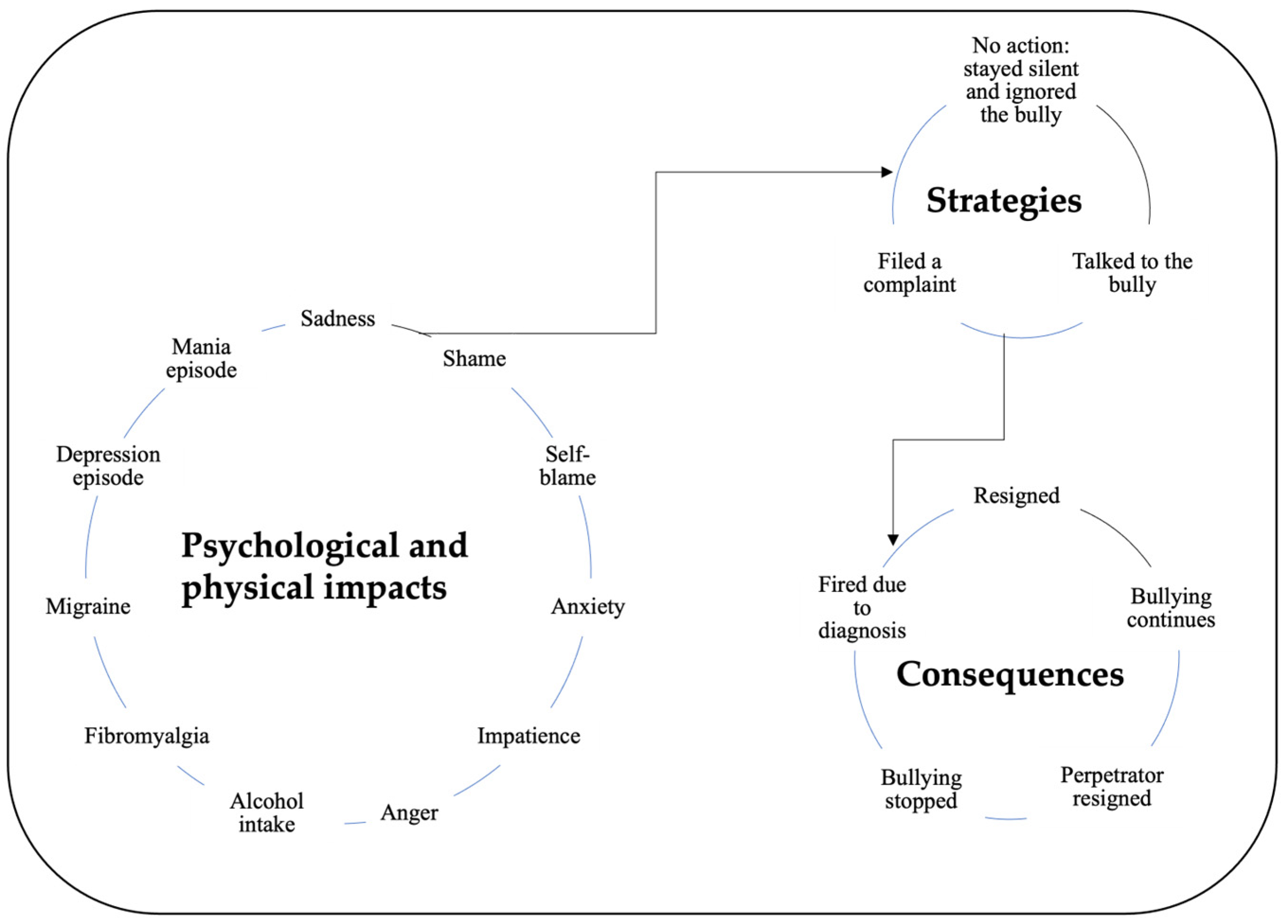
3.3. Impact, Strategies, and Consequences of Bullying
“The deterioration of human relations is tiring for me. In any episode, relationships are instantly broken. Episodes come and go if you manage them correctly. I have a disease. Treatment methods are clear. What makes me tired is that the social environment is affected too much. People leave me.”
“If the situation bothers me a lot, I go talk to my manager, ask their opinion. If still, things do not get back to normal, then I file a complaint, I do not hesitate.” (Participant 10)
“You need to draw your boundaries as much as possible.” (Participant 15)
“Tell the bully that it is wrong to act like this, that they should put themselves in the other person’s shoes, and empathise. It is best to have open communication and solve it.” (Participant 6)
“Do not respond to bullies.” (Participant 12)
3.4. Empowering Strategies to Combat Workplace Bullying towards Individuals with BD
3.4.1. Organisational Solutions
- (a)
- Public Training and Hotlines: Participant 11 recommended anonymous reporting through government hotlines, emphasising the need for confidentiality to encourage reporting of bullying incidents: “I think you should be able to report anonymously to the government’s hotline, but they ask your name. Unions can do it.” (Participant 11)
- (b)
- Organisational Audits: Participant 18 suggested governmental intervention through organisational audits to ensure the well-being of employees with bipolar disorder, highlighting the importance of state protection:
“If the state does not protect its citizens diagnosed with bipolar disorder, I do not think another person will defend their rights or treat them well. The state should visit workplaces to check on bipolar employees following up on their work conditions.” (Participant 18).
- (c)
- Mental Health Checks and Awareness: Participant 9 proposed incorporating mental health and disability tests into public health screening from early childhood, stressing the importance of early detection and support for mental health issues.
“Doctors come to schools for vision screening when we are kids. However, psychiatric and psychological tests are not done. Until military service, I did not know about my condition. Public health screening should include psychiatric disability tests from early childhood.” (Participant 9).
- (d)
- Leadership: Participant 4 emphasised the importance of effective leadership, suggesting that organisations seek leaders who can create a positive and harmonious environment for all stakeholders: “Find good leaders like orchestra chiefs, that could make all stakeholders happy.” (Participant 4).
- (e)
- Policies and Procedures: Participant 1 recommended organisational policies that foster communication, performance evaluations, and strict consequences, including the possibility of punishment or dismissal, for workplace bullies: “Organisations should establish an open communication environment, frequent performance reviews. Bullies should be punished or even dismissed.” (Participant 1).
3.4.2. Self-Employment or Public Sector Employment
“If you say ‘I am bipolar’ before you get hired, you will not be hired. If you say, ‘I am bipolar,’ after being hired, they will start looking for ways to fire you as soon as possible. I advise people with bipolar to choose jobs they can do themselves and be self-employed. Or get a job in the public sector. Whether you are bipolar or schizophrenic, they cannot fire you after the state hires you. Because you have serious legal rights.” (Participant 5).
3.4.3. Suggestions on Accommodations for Long-Term Employment
- (a)
- Creating a Supportive Environment: Open communication about bipolar disorder, understanding, and recognition of the unique challenges faced by employees with this condition is critical as Participant 8 mentioned: “(After the attack) there was no negative change (at work). Everyone supported me. Because they knew me very well.” As Participant 2 highlighted, “They know my diagnosis and manage it”; others need to manage this context. Participant 11′s articulation, “Bipolar employees’ views should be recognised; they should not be left out because of their illnesses,” showed the importance of inclusive social settings.
- (b)
- Flexible work arrangements: A supportive attitude from supervisors to accommodate the working hours, duration, and space according to the needs of individuals with bipolar disorder was proposed as a critical solution, as the following quotes depict:
“The head of the department handled me in a very fatherly way. He told me not to come to work if I had a problem…. I felt in balance there.” (Participant 15)
“Because my supervisor is very understanding, he knows what my diagnosis is. When I request to go to work late, he gives me an hour to be late. I use my disability rights.” (Participant 7)
“I shared it (bipolar diagnosis) when I started working. I told them that I may need to visit my doctor from time to time. It is not used as a negative thing against me, nor is it used positively.” (Participant 10)
“There are Community Mental Health Centres for patients who need support. Various events are held there. Employees may be allowed to attend the meetings held here. Occupational physicians may write to human resources or the employee’s manager, stating that they must give permission,” (Participant 19)
- (c)
- Allowing for Job Redesign/Replacement: Redesigning or replacing jobs based on individual needs helped maintain employment and prevent unnecessary stressors for employees with BD. Participant 15′s experience set an example for a redesign: “The work-travel was too much. They placed me in a better position afterwards.” Participant 8 described a positive replacement example: “After the attack, my boss supported me. He hired someone while I was gone. After I came back from sick leave, instead of firing him or me, he kept us both.”
- (d)
- Allowing for Frequent Breaks: According to participants of the current study, managing stress levels and maintaining mental well-being may easily be promoted by allowing for more breaks. Participant 13 said “When I was working, people were aware (bipolar diagnosis). When I felt the need, I used to step outside the office and be back after a while.”
- (e)
- Redesigning Performance Reviews: Redesigning performance reviews involves recognising and valuing the unique contributions of employees with bipolar disorder, emphasising the importance of effective management as Participant 5 portrayed: “When you say to the manager, this employee has a different personality, and we employed them knowingly. How well you manage this person will affect your performance; believe me, that person will stay in business life.”
4. Discussion
4.1. Navigating the Spectrum of Negative Behaviours: Gossip, Ridicule, and Exclusion as Forms of Workplace Bullying towards Individuals with BD
4.2. Roots of Workplace Bullying: Exploring Organisational Culture, Perpetrator Traits, and Individual Factors in the Onset of Workplace Bullying
4.3. The Devastating Impact of Workplace Bullying on Employees with BD: Ignored Complaints and Health Consequences
4.4. Towards a Bully-Free Workplace: Empowering Strategies for Individuals and Organisational Change
4.5. Building a Supportive Ecosystem: Accommodations for Prolonged Employment and Psychological Well-Being
4.6. Transformative Steps: Addressing Stigma, Enhancing Awareness, and Fostering Inclusive Work Environments for Individuals with BD
4.7. Limitations
4.8. Future Research
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Fevre, R.; Robinson, A.; Lewis, D.; Jones, T. The ill-treatment of employees with disabilities in British workplaces. Work Employ. Soc. 2013, 27, 288–307. [Google Scholar] [CrossRef]
- Leymann, H. The content and development of mobbing at work. Eur. J. Work Organ. Psychol. 1996, 5, 165–184. [Google Scholar] [CrossRef]
- Einarsen, S. Harassment and bullying at work. Aggress. Violent Behav. 2000, 5, 379–401. [Google Scholar] [CrossRef]
- León-Pérez, J.M.; Escartín, J.; Giorgi, G. The Presence of Workplace Bullying and Harassment Worldwide. In Concepts, Approaches and Methods. Handbooks of Workplace Bullying, Emotional Abuse and Harassment; D’Cruz, P., Noronha, E., Notelaers, G., Rayner, C., Eds.; Springer: Singapore, 2021; Volume 1. [Google Scholar] [CrossRef]
- Baillien, E.; Neyens, I.; De Witte, H.; De Cuyper, N. A qualitative study on the development of workplace bullying: Towards a three-way model. J. Community Appl. Soc. Psychol. 2009, 19, 1–16. [Google Scholar] [CrossRef]
- Van den Brande, W.; Baillien, E.; De Witte, H.; Vander Elst, T.; Godderis, L. The role of work stressors, coping strategies and coping resources in the process of workplace bullying: A systematic review and development of a comprehensive model. Aggress. Violent Behav. 2016, 29, 61–71. [Google Scholar] [CrossRef]
- Ågotnes, K.W.; Skogstad, A.; Hetland, J.; Olsen, O.K.; Espevik, R.; Bakker, A.B.; Einarsen, S.V. Daily work pressure and exposure to bullying-related negative acts: The role of daily transformational and laissez-faire leadership. Eur. Manag. J. 2020, 39, 423–433. [Google Scholar] [CrossRef]
- Glambek, M.; Skogstad, A.; Einarsen, S. Workplace bullying, the development of job insecurity and the role of laissez-faire leadership: A two-wave moderated mediation study. Work Stress 2018, 32, 297–312. [Google Scholar] [CrossRef]
- Fernández-del-Río, E.; Ramos-Villagrasa, J.; Escartín, J. The incremental effect of Dark personality over the Big Five in workplace bullying: Evidence from perpetrators and targets. Personal. Individ. Differ. 2021, 168, 110291. [Google Scholar] [CrossRef]
- Reknes, I.; Notelaers, G.; Iliescu, D.; Einarsen, S.V. The influence of target personality in the development of workplace bullying. J. Occup. Health Psychol. 2021, 26, 291–303. [Google Scholar] [CrossRef]
- Nielsen, M.B.; Knardahl, S. Is workplace bullying related to the personality traits of victims? A two-year prospective study. Work Stress 2015, 29, 128–149. [Google Scholar] [CrossRef]
- Einarsen, S.; Hoel, H.; Zapf, D.; Cooper, C.L. The concept of bullying and harassment at work: The European tradition. In Bullying and Harassment in the Workplace: Theory, Research, and Practice, 3rd ed.; Einarsen, S.V., Hoel, H., Zapf, D., Cooper, C.L., Eds.; CRC Press: Boca Raton, FL, USA, 2020; pp. 3–53. [Google Scholar]
- Mikkelsen, E.G.; Hansen, A.M.; Persson, R.; Byrgesen, E.M.; Hogh, A. Individual Consequences of being Exposed to Workplace Bullying. In Bullying and Harassment in the Workplace: Theory, Research and Practice, 3rd ed.; Einarsen, S.V., Hoel, H., Zapf, D., Cooper, C.L., Eds.; CRC Press: Boca Raton, FL, USA, 2020; pp. 163–208. [Google Scholar]
- Dollard, M.; Skinner, N.; Tuckey, M.R.; Bailey, T. National surveillance of psychosocial risk factors in the workplace: An international overview. Work Stress 2007, 21, 1–29. [Google Scholar] [CrossRef]
- Verkuil, B.; Atasayi, S.; Molendijk, M.L. Workplace Bullying and Mental Health: A Meta-Analysis on Cross-Sectional and Longitudinal Data. PLoS ONE 2015, 10, e0135225. [Google Scholar] [CrossRef] [PubMed]
- Ghebreyesus, T.A. Opening Speech. Mental Health at Work Panel. In Proceedings of the World Economic Forum, Davos, Switzerland, 16–20 January 2023. [Google Scholar]
- World Health Organization. World Mental Health Report: Transforming Mental Health for All. 2022. Available online: https://www.who.int/publications/i/item/9789240049338 (accessed on 25 January 2023).
- Humpston, C.S.; Bebbington, P.; Marwaha, S. Bipolar disorder: Prevalence, help-seeking and use of mental health care in England. Findings from the 2014 Adult Psychiatric Morbidity Survey. J. Affect. Disord. 2021, 282, 426–433. [Google Scholar] [CrossRef] [PubMed]
- Hirschfeld, R.M.; Calabrese, J.R.; Weissman, M.M. Screening for bipolar disorder in the community. J. Clin. Psychiatry 2003, 64, 53–59. [Google Scholar] [CrossRef]
- Mondimore, F.M. Bipolar Disorder: A Guide for Patients and Families; Johns Hopkins University Press: Baltimore, MD, USA, 2014. [Google Scholar]
- Akiskal, H.S.; Bourgeois, M.L.; Angst, J.; Post, R.; Möller, H.J.; Hirschfeld, R. Re-evaluating the prevalence of and diagnostic composition within the broad clinical spectrum of bipolar disorders. J. Affect. Disord. 2000, 59, S5–S30. [Google Scholar] [CrossRef] [PubMed]
- American Psychiatric Association, DSM-5 Task Force. Diagnostic and Statistical Manual of Mental Disorders: DSM-5™, 5th ed.; American Psychiatric Publishing, Inc.: Arlington, VA, USA, 2013. [Google Scholar] [CrossRef]
- Dominiak, M.; Jażdżyk, P.; Antosik-Wójcińska, A.Z.; Konopko, M.; Bieńkowski, P.; Świȩcicki, Ł.; Sienkiewicz-Jarosz, H. The impact of bipolar spectrum disorders on professional functioning: A systematic review. Front Psychiatry 2022, 13, 951008. [Google Scholar] [CrossRef]
- Americans with Disabilities Act of 1990, Title 42. 2008. Available online: https://www.ada.gov/law-and-regs/ada/ (accessed on 25 January 2023).
- European Disability Strategy 2010–2020, 1323 & 1324. 2010. Available online: https://eur-lex.europa.eu/LexUriServ/LexUriServ.do?uri=COM%3A2010%3A0636%3AFIN%3Aen%3APDF (accessed on 25 January 2023).
- Law on Disabled People and on Making Amendments in Some Laws and Decree Laws, 5378. 2005. Available online: https://www.un.org/development/desa/disabilities/wp-content/uploads/sites/15/2019/11/Turkey_Turkish-Disability-Act-TDA-No.-5378-of-2005.pdf (accessed on 25 January 2023).
- Holm, M.; Taipale, H.; Tanskanen, A.; Tiihonen, J.; Mitterdorfer-Rutz, E. Employment among people with schizophrenia or bipolar disorder: A population-based study using nationwide registers. Acta Psychiatr. Scand. 2020, 143, 61–71. [Google Scholar] [CrossRef]
- Kessler, R.; Akiskal, H.S.; Ames, M.; Birnbaum, H.; Greenberg, P.; Hirschfeld, R.; Jin, R.; Merikangas, K.R.; Wang, P.S. Prevalence and Effects of Mood Disorders on Work Performance in a Nationally Representative Sample of U.S. Workers. Am. J. Psychiatry 2006, 163, 1561. [Google Scholar] [CrossRef]
- McMorris, B.J.; Downs, K.E.; Panish, J.M.; Dirani, R. Workplace productivity, employment issues, and resource utilisation in patients with bipolar I disorder. J. Med. Econ. 2009, 13, 23–32. [Google Scholar] [CrossRef]
- Lomastro, M.J.; Valerio, M.P.; Blasco, M.B.; Tagni, M.F.; Martino, D.J. Predictors of High Psychosocial Functioning in Bipolar Disorder. J. Nerv. Ment. Dis. 2020, 208, 904–907. [Google Scholar] [CrossRef]
- Marwaha, S.; Durrani, A.; Singh, S. Employment outcomes in people with bipolar disorder: A systematic review. Acta Psychiatr. Scand. 2013, 128, 179–193. [Google Scholar] [CrossRef]
- Tse, S.; Chan, S.; Ng, K.L.; Yatham, L.N. Meta-analysis of predictors of favorable employment outcomes among individuals with bipolar disorder. Bipolar Disord. 2014, 16, 217–229. [Google Scholar] [CrossRef]
- Hakulinen, C.; Musliner, K.L.; Agerbo, E. Bipolar disorder and depression in early adulthood and long-term employment, income, and educational attainment: A nationwide cohort study of 2,390,127 individuals. Depress. Anxiety 2019, 36, 1080–1088. [Google Scholar] [CrossRef]
- Russinova, Z.; Bloch, P.; Wewiorski, N.; Shappell, H.; Rogers, E.S. Predictors of Sustained Employment Among Individuals With Serious Mental Illness. J. Nerv. Ment. Dis. 2018, 260, 669–679. [Google Scholar] [CrossRef]
- Kraiss, J.T.; ten Klooster, P.M.; Frye, E.; Kupka, R.W.; Bohlmeijer, E.T. Exploring factors associated with personal recovery in bipolar disorder. Psychol. Psychother. Theory Res. Pract. 2021, 94, 667–685. [Google Scholar] [CrossRef]
- Leufstadius, C.; Eklund, M.; Erlandsson, L.K. Meaningfulness in work—Experiences among employed individuals with persistent mental illness. Work 2009, 34, 21–32. [Google Scholar] [CrossRef] [PubMed]
- Dunn, E.C.; Wewiorski, N.J.; Rogers, E.S. The meaning and importance of employment to people in recovery from serious mental illness: Results of a qualitative study. Psychiatr. Rehabil. J. 2008, 32, 59–62. [Google Scholar] [CrossRef]
- Miller, J.N.; Black, D.W. Bipolar Disorder and Suicide: A Review. Curr. Psychiatry Rep. 2020, 22, 6. [Google Scholar] [CrossRef] [PubMed]
- Bessonova, L.; Ogden, K.; Doane, M.J.; O’Sullivan, A.K.; Tohen, M. The Economic Burden of Bipolar Disorder in the United States: A Systematic Literature Review. Clinicoecon Outcomes Res. 2020, 12, 481–497. [Google Scholar] [CrossRef] [PubMed]
- Marion-Paris, E.; Beetlestone, E.; Paris, R.; Bouhadfane, M.; Villa, A.; Lehucher-Michel, M.P. Job retention for people with bipolar disorder: A qualitative analysis. Scand. J. Psychol. 2022, 64, 171–178. [Google Scholar] [CrossRef]
- Reavley, N.J.; Morgan, A.J.; Jorm, A.F. Predictors of experiences of discrimination and positive treatment in people with mental health problems: Findings from an Australian national survey. Soc. Psychiatry Psychiatr. Epidemiol. 2016, 52, 269–277. [Google Scholar] [CrossRef]
- Lewis, D.; Deakin, R.; McGregor, F.L. Workplace Bullying, Disability and Chronic Ill Health. In Handbooks of Workplace Bullying, Emotional Abuse and Harassment; D’Cruz, P., Noronha, E., Caponecchia, C., Escartín, J., Salin, D., Tuckey, M.R., Eds.; Dignity and Inclusion at Work; Springer: Singapore, 2021; Volume 3. [Google Scholar] [CrossRef]
- Hawke, L.D.; Parikh, S.V.; Michalak, E.E. Stigma and bipolar disorder: A review of the literature. J. Affect. Disord. 2013, 150, 181–191. [Google Scholar] [CrossRef] [PubMed]
- Follmer, K.B.; Follmer, D.J. Longitudinal relations between workplace mistreatment and engagement—The role of suicidal ideation among employees with mood disorders. Organ. Behav. Hum. Decis. Process. 2021, 162, 206–217. [Google Scholar] [CrossRef]
- Gultekin, B.; Kesebir, S.; Tamam, L. Bipolar disorder in Turkey: A review. Psikiyatr. Guncel Yaklasimlar Curr. Approaches Psychiatry 2014, 6, 1. [Google Scholar] [CrossRef]
- Alyılmaz, A.İ. Tıpta Uzmanlık Öğrencisi Hekimlerde Mobbing, Ilişkili Faktörler ve Sonuçları; Bursa Uludağ Üniversitesi Örneği. Yayınlanmamış Tıpta Uzmanlık Tezi, Bursa Uludağ Üniversitesi Tıp Fakültesi, Bursa, Turkey, 2020. [Google Scholar]
- Kartal, M.T.; Depren, Ö.; Kılıç Depren, S. A Research upon Psychological Harassment (Mobbing) in Turkish Banking Sector. J. Yasar Univ. 2019, 14, 180–195. [Google Scholar]
- Yayak, A.; Top, O. Investigation of the Relationship Between Mobbing (Psychological Terror) and Motivation Perceptions with Sleep Quality in Healthcare Professionals: Edirne Sample. Turk. Klin. J. Forensic Med. Forensic Sci. 2020, 17, 264–276. [Google Scholar] [CrossRef]
- Zapf, D.; Escartín, J.; Scheppa-Lahyani, M.; Einarsen, S.V.; Hoel, H.; Vartia, M. Empirical findings on the prevalence and risk groups of bullying in the workplace. In Bullying and Harassment in the Workplace: Theory, Research, and practice, 3rd ed.; Einarsen, S.V., Hoel, H., Zapf, D., Cooper, C.L., Eds.; CRC Press: Boca Raton, FL, USA, 2020; pp. 105–162. [Google Scholar]
- D’Cruz, P.; Paull, M.; Omari, M.; Guneri-Cangarli, B. Target experiences of workplace bullying: Insights from Australia, India and Turkey. Empl. Relat. 2016, 38, 805–823. [Google Scholar] [CrossRef]
- Salin, D.; Cowan, R.; Adewumi, O.; Apospori, E.; Bochantin, J.; D’Cruz, P.; Djurkovic, N.; Durniat, K.; Escartín, J.; Guo, J.; et al. Workplace Bullying Across the Globe: A Cross-Cultural Comparison. Pers. Rev. 2019, 48, 204–219. [Google Scholar] [CrossRef]
- Hennink, M.; Kaiser, B.N. Sample sizes for saturation in qualitative research: A systematic review of empirical tests. Soc. Sci. Med. 2022, 292, 114523. [Google Scholar] [CrossRef]
- Musselwhite, K.; Cuff, L.; McGregor, L.; King, K.M. The telephone interview is an effective method of data collection in clinical nursing research: A discussion paper. Int. J. Nurs. Stud. 2007, 44, 1064–1070. [Google Scholar] [CrossRef]
- Marshall, C.; Rossman, G. Designing Qualitative Research; Sage: Thousand Oaks, CA, USA, 1999. [Google Scholar]
- Yüksel, P.; Yıldırım, S. Theoretical Frameworks, Methods, and Procedures for Conducting Phenomenological Studies. Turk. Online J. Qual. Inq. 2015, 6, 1–20. [Google Scholar] [CrossRef]
- Burr, H.; Berthelsen, H.; Moncada, S.; Nübling, M.; Dupret, E.; Demiral, Y.; Oudyk, J.; Kristensen, T.S.; Llorens, C.; Navarro, A.; et al. The third version of the Copenhagen Psychosocial Questionnaire. Saf. Health Work 2019, 10, 482–503. [Google Scholar] [CrossRef]
- Bingham, A.J. From Data Management to Actionable Findings: A Five-Phase Process of Qualitative Data Analysis. Int. J. Qual. Methods 2023, 22. [Google Scholar] [CrossRef]
- Collins, C.S.; Stockton, C.M. The Central Role of Theory in Qualitative Research. Int. J. Qual. Methods 2018, 17. [Google Scholar] [CrossRef]
- Georges, J.M. Linking Nursing Theory and Practice. Adv. Nurs. Sci. 2005, 28, 50–57. [Google Scholar] [CrossRef] [PubMed]
- Einarsen, S.; Hoel, H.; Notelaers, G. Measuring exposure to bullying and harassment at work: Validity, factor, structure and psychometric properties of the Negative Acts Questionnaire-Revised. Work Stress 2009, 23, 24–44. [Google Scholar] [CrossRef]
- Escartín, J.; Vranjes, I.; Baillien, E.; Notelaers, G. Workplace Bullying and Cyberbullying Scales: An overview. In Concepts, Approaches and Methods. Handbooks of Workplace Bullying, Emotional Abuse and Harassment; D’Cruz, P., Noronha, E., Notelaers, G., Rayner, C., Eds.; Springer: Singapore, 2021; Volume 1. [Google Scholar] [CrossRef]
- Feijó, F.R.; Gräf, D.D.; Pearce, N.; Fassa, A.G. Risk Factors for Workplace Bullying: A Systematic Review. Int. J. Environ. Res. Public Health 2019, 16, 1945. [Google Scholar] [CrossRef]
- Serafin, L.; Sak-Dankosky, N.; Czarkowska-Pączek, B. Bullying in nursing evaluated by the Negative Acts Questionnaire-Revised: A systematic review and meta-analysis. J. Adv. Nurs. 2020, 76, 1320–1333. [Google Scholar] [CrossRef]
- Nielsen, M.B.; Einarsen, S.V. What we know, what we do not know, and what we should and could have known about workplace bullying: An overview of the literature and agenda for future research. Aggress. Violent Behav. 2018, 42, 71–83. [Google Scholar] [CrossRef]
- Braun, V.; Clarke, V. Using thematic analysis in psychology. Qual. Res. Psychol. 2006, 3, 77–101. [Google Scholar] [CrossRef]
- Işık, İ. İş Hayatında Şiddetsizlik: Örgütlerde Şiddeti Fark Etme ve Önleme. Şiddetsiz Birey, Aİle ve Toplum; İstanbul Bilgi University Press: İstanbul, Turkey, in press.
- Skarpaas, L.S.; Ramvi, E.; Løvereide, L.; Aas, R.W. Maximising work integration in job placement of individuals facing mental health problems: Supervisor experiences. Work 2015, 53, 87–98. [Google Scholar] [CrossRef]
- Rai, A.; Agarwal, U.A. A review of literature on mediators and moderators of workplace bullying. Manag. Res. Rev. 2018, 41, 822–859. [Google Scholar] [CrossRef]
- Samnani, A.K.; Singh, P. 20 Years of workplace bullying research: A review of the antecedents and consequences of bullying in the workplace. Aggress. Violent Behav. 2012, 17, 581–589. [Google Scholar] [CrossRef]
- Salin, D.; Hoel, H. Organisational risk factors of workplace bullying. In Bullying and Harassment in the Workplace: Theory, Research and Practice, 3rd ed.; Einarsen, S.V., Hoel, H., Zapf, D., Cooper, C.L., Eds.; CRC Press: Boca Raton, FL, USA, 2020; pp. 305–330. [Google Scholar]
- Özer, G.; Escartín, J. The making and breaking of Workplace Bullying perpetration: A systematic review on the antecedents, moderators, and mediators of perpetration and suggestions for organisations. Aggress. Violent Behav. 2023, 69, 101823. [Google Scholar] [CrossRef]
- National Collaborating Centre for Mental Health (UK). Bipolar Disorder: The NICE Guideline on the Assessment and Management of Bipolar Disorder in Adults, Children and Young People in Primary and Secondary Care; National Clinical Guideline 185; The British Psychological Society and The Royal College of Psychiatrists: London, UK, 2017. [Google Scholar]
- Durand-Moreau, Q.; Le Deun, C.; Lodde, B.; Dewitte, J.D. The framework of clinical occupational medicine to provide new insight for workaholism. Ind. Health 2018, 56, 441–451. [Google Scholar] [CrossRef] [PubMed]
- Elliott, M.; Reuter, J.C. The Benefits and Challenges of Employment for Working Professionals Diagnosed with Mental Illness. Community Ment. Health J. 2022, 58, 645–656. [Google Scholar] [CrossRef]
- Hennekam, S.; Follmer, K.; Beatty, J.E. The paradox of mental illness and employment: A person-job fit lens. Int. J. Hum. Resour. Manag. 2020, 32, 3244–3271. [Google Scholar] [CrossRef]
- Nielsen, M.B.; Einarsen, S. Outcomes of exposure to workplace bullying: A meta-analytic review. Work Stress 2012, 26, 309–332. [Google Scholar] [CrossRef]
- Işık, İ. İnsan Kaynakları Yönetimi Profesyonellerinin İş Ortamındaki Zorbalık Davranışlarına Dair Perspektifleri: Zorbalığın Tanımı, Nedenleri ve Sonuçları. Çalışma Ve Toplum 2015, 4, 237–274. Available online: https://dergipark.org.tr/tr/pub/ct/issue/71829/1155529 (accessed on 25 January 2023).
- Michalak, E.E.; Yatham, L.N.; Maxwell, V.; Hale, S.; Lam, R.W. The impact of bipolar disorder upon work functioning: A qualitative analysis. Bipolar Disord. 2007, 9, 126–143. [Google Scholar] [CrossRef]
- Nolfe, G.; Petrella, C.; Zontini, G.; Uttieri, S.; Nolfe, G. Association between bullying at work and mental disorders: Gender differences in the Italian people. Soc. Psychiatry Psychiatr. Epidemiol. 2010, 45, 1037–1041. [Google Scholar] [CrossRef]
- Van de Vliert, E.; Einarsen, S.; Nielsen, M.B. Are national levels of employee harassment cultural covariations of climato-economic conditions? Work Stress 2013, 27, 106–122. [Google Scholar] [CrossRef]
- Gardner, H.H.; Kleinman, N.L.; Brook, R.A.; Rajagopalan, K.; Brizee, T.J.; Smeeding, J.E. The economic impact of bipolar disorder in an employed population from an employer perspective. J. Clin. Psychiatry 2006, 67, 1209–1218. [Google Scholar] [CrossRef] [PubMed]
- Laxman, K.E.; Lovibond, K.S.; Hassan, M.K. Impact of bipolar disorder in employed populations. Am. J. Manag. Care 2008, 14, 757–764. [Google Scholar] [PubMed]
- Zafar, N.; Rotenberg, M.; Rudnick, A. A systematic review of work accommodations for people with mental disorders. Work 2019, 64, 461–475. [Google Scholar] [CrossRef] [PubMed]
- Hastuti, R.; Timming, A.R. An inter-disciplinary review of the literature on mental illness disclosure in the workplace: Implications for human resource management. Int. J. Hum. Resour. Manag. 2021, 32, 3302–3338. [Google Scholar] [CrossRef]
- Fan, J.K.; Mustard, C.; Smith, P.M. Psychosocial Work Conditions and Mental Health: Examining Differences Across Mental Illness and Well-being Outcomes. Ann. Work Expo. Health 2019, 63, 546–559. [Google Scholar] [CrossRef] [PubMed]
- Thomas, T.L.; Prasad Muliyala, K.; Jayarajan, D.; Angothu, H.; Thirthalli, J. Vocational challenges in severe mental illness: A qualitative study in persons with professional degrees. Asian J. Psychiatry 2019, 42, 48–54. [Google Scholar] [CrossRef] [PubMed]
- Khairallah, C.; Kassab, A.; Damien, A.; Richa, S. Attitude of the employer in Lebanon toward candidates and employees with a stable chronic mental illness. Int. J. Soc. Psychiatry 2021, 002076402110138. [Google Scholar] [CrossRef]
- Kinn, L.G.; Holgersen, H.; Aas, R.W.; Davidson, L. “Balancing on Skates on the Icy Surface of Work”: A Metasynthesis of Work Participation for Persons with Psychiatric Disabilities. J. Occup. Rehabil. 2013, 24, 125–138. [Google Scholar] [CrossRef]
- MacDonald-Wilson, K.L.; Rogers, E.S.; Massaro, J.M.; Lyass, A.; Crean, T. An investigation of reasonable workplace accommodations for people with psychiatric disabilities: Quantitative findings from a multi-site study. Community Ment. Health J. 2002, 38, 35–50. [Google Scholar] [CrossRef]
- Høgh, A.; Clausen, T.; Bickmann, L.; Hansen, S.M.; Conway, P.M.; Baernholdt, M. Consequences of Workplace Bullying for Individuals, Organizations and Society. Pathw. Job-Relat. Negat. Behav. 2021, 2, 1–24. [Google Scholar] [CrossRef]
- Jones, K.P.; Peddie, C.I.; Gilrane, V.L.; King, E.B.; Gray, A.L. Not So Subtle. J. Manag. 2016, 42, 1588–1613. [Google Scholar] [CrossRef]
- EC. A Better Workplace for All: From Equal Opportunities Towards Diversity and Inclusion; Communication from the Commission to the European Parliament, the Council, the European Economic and Social Committee and the Committee of the Regions, COM 5300; EC: Brussels, Belgium, 2017. [Google Scholar]
- Mellifont, D. Facilitators and Inhibitors of Mental Discrimination in the Workplace: A Traditional Review. Stud. Soc. Justice 2021, 15, 59–80. [Google Scholar] [CrossRef]
- Scheepers, D.; Ellemers, N. Social Identity Theory. In Social Psychology in Action; Sassenberg, K., Vliek, M., Eds.; Springer: Cham, Switzerland, 2019. [Google Scholar] [CrossRef]
- Escartín, J.; Ullrich, J.; Zapf, D.; Schlüter, E.; van Dick, R. Individual- and group-level effects of social identification on workplace bullying. Eur. J. Work Organ. Psychol. 2013, 22, 182–193. [Google Scholar] [CrossRef]
- Brown, R. Social identity theory: Past achievements, current problems and future challenges. Eur. J. Soc. Psychol. 2000, 30, 745–778. [Google Scholar] [CrossRef]
- Moss, S.; Vemuri, S.R.; Hedley, D.; Uljarevic, M. Initiatives that diminish the biases of recruiters against people who disclose or demonstrate a diagnosed mental disorder. Equal. Divers. Incl. Int. J. 2017, 36, 2–16. [Google Scholar] [CrossRef]
- Yoshimura, Y.; Bakolis, I.; Henderson, C. Psychiatric diagnosis and other predictors of experienced and anticipated workplace discrimination and concealment of mental illness among mental health service users in England. Soc. Psychiatry Psychiatr. Epidemiol. 2018, 53, 1099–1109. [Google Scholar] [CrossRef] [PubMed]
- Filia, K.M.; Cotton, S.M.; Watson, A.E.; Jayasinghe, A.; Kerr, M.; Fitzgerald, P.B. Understanding the Barriers and Facilitators to Employment for People with Bipolar Disorder. Psychiatr. Q. 2021, 92, 1565–1579. [Google Scholar] [CrossRef]
- Brod, M.; Tesler, L.E.; Christensen, T.L. Qualitative research and content validity: Developing best practices based on science and experience. Qual. Life Res. Int. J. Qual. Life Asp. Treat. Care Rehabil. 2009, 18, 1263–1278. [Google Scholar] [CrossRef]


{kind=link}
| # | Gender | Age | D. Age | Exp. (Years) | # of Comp. | Education | Last Sector Worked | Job Title | Currently Working | Exposed to Bullying | Diagnosis Disclosed |
|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | F | 39 | 32 | 17 | 4 | GD-cont. | Manufacturing | Strategic planning manager | Yes | Yes | Yes |
| 2 * | M | 30 | 16 | 13 | 1 | Pre-UD | State org. | Clergyman | Yes | Yes | Yes |
| 3 * | M | 33 | 28 | 17 | 4 | UD | Retail | Department manager | Yes | No | Yes |
| 4 | M | 52 | 45 | 26 | 4 | UD | Manufacturing | Sales, marketing, and administration | No-seeking | Yes | No |
| 5 | F | 55 | 55 | 26 | 4 | UD | Manufacturing | Training manager | No-retired | Yes | No |
| 6 | M | 26 | 16 | 1 | 1 | UD | State org. | Data preparation and control | Yes | Yes | Yes |
| 7 | F | 32 | 14 | 2 | 2 | UD | State org. | Social worker | Yes | No | Yes |
| 8 | M | 35 | 29 | 11 | 3 | GD | Retail | Dealer manager | No-seeking | Yes | Yes |
| 9 | M | 23 | 19 | 4 | 1 | UD | NGO (Student) | Head of Council of Disabled Students | No-seeking | Yes | Yes |
| 10 * | M | 30 | 17 | 5 | 3 | UD-cont. | Retail | Office Manager | Yes | Yes | Yes |
| 11 | M | 34 | 34 | 8 | 1 | GD | State org. | Project manager | Yes | Yes | Yes |
| 12 | M | 41 | 21 | 21 | NA | JH | Manufacturing | Construction worker | Yes | No | Yes |
| 13 | F | 50 | 40 | 20 | NA | JH | Manufacturing | Sewing machine operator | No-retired | No | No |
| 14 | F | 25 | 23 | 6 | 3 | UD | Media | Designer | Yes | Yes | No |
| 15 | F | 37 | 19 | 16 | 3 | GD | State org. | Coordinator | Yes | Yes | Yes |
| 16 | F | 39 | 29 | 17 | 2 | GD | State org. | Food engineer | Yes | No | No |
| 17 | M | 35 | 28 | 10 | 6 | Pre-UD | Exports and Imports | Business owner | No | No | No |
| 18 | F | 27 | 24 | 1 | 1 | Pre-UD | Media | Business admin student | No | Yes | No |
| 19 | M | 34 | 32 | 10 | 3 | UD | State org. | Market research specialist | Yes | Yes | Yes |
| Types | Negative Acts * | Sample Quotes |
|---|---|---|
| Person-related bullying | ||
| Being insulted | Behind my back, they (colleagues) said, “is she retarded or crazy.” (Participant 18) | |
| Being ignored or excluded | They excluded me because of my depression. (Participant 5) | |
| Persistently criticised | People constantly criticised my personality, not how I did my job. (Participant 5) | |
| Excessively teased with sarcasm | It (diagnosis) was a matter of constant teasing behind my back. (Participant 18) | |
| Work-related bullying | ||
| Unmanageable workload | Unfortunately, in Turkey, the lack of clear working hours is very exhausting. Working under non-ideal conditions, with very long working hours and standing for extended periods, was very difficult, especially for someone like me. Did you also work on weekends? Yes, especially in real estate, we used to work on weekends and take one day off during the week. Potential buyers would visit on weekends. When you work for 10–11 h a day, trying to complete tasks that you couldn’t finish during the week, life becomes unbearable. This is very difficult even for healthy individuals, and for a bipolar person, it is much, much more challenging. Because I need to be able to clear the energy I put into my own situation. When I can’t do that, it becomes impossible to move. Participating in life becomes difficult. (Participant 10). | |
| Deprived of work rights | I was having trouble getting permission for annual leave. We could not use it to the end when we were given permission. (Participant 19) | |
| Working below level of competence | (When the CEO and HR learned about my diagnosis) They said, ‘You are an unstable person. You cannot manage a team. “You are not a manager anymore”, and they downgraded me. (Participant 1) | |
| Physically intimidating bullying | ||
| Being shouted at | When he suddenly enters the room shouting (supervisor), it feels like our hearts will burst (Participant 11) | |
| Themes | Example Quotes |
|---|---|
| Work environment | |
| Toxic environment | “I was excluded from others in my first job by my peers since I was a relative of the owner of the company.” (Participant 8) |
| “Bullying others is a learned behaviour. This is how they learn from others. They continue to practice it unconsciously or knowingly, like a tradition.”(Participant 11) | |
| “I was trying to get a disability report. Later, I found out that this was the subject of teasing in the company.” (Participant 18) | |
| Leadership | “If leadership is inadequate, anything could happen.” (Participant 4) |
| “I had conflicts with my manager on business issues. His comments were soul-crushing.” (Participant 19) | |
| Workload | “There was trouble on task distribution since the workload was too much.” (Participant 6) |
| “He was constantly putting pressure on us to finish the task at hand. We were constantly stressed. He was verbally abusive.” (Participant 11) | |
| Individual Characteristics | |
| “Ego problems” (Participant 6) | |
| Related to the bully | “People are ruthless and mean” (Participant 18) |
| “It is a power game” (Participant 2) | |
| “If the managers are not very confident, feel someone as a threat, know that an employee under them is actually better than them, do not want that person to come to the forefront, then they are targeted.” (Participant 15) | |
| “Managers have encountered such an attitude previously. So it is a chain thing. It is a learned behaviour. That is how they conduct their relationship with others. They continue with negative behaviours unconsciously or knowingly, like a tradition in the organisation. They probably also bully their spouses.” (Participant 11) | |
| Related to the victim | “If I am unhappy, I am unhappy. I cannot fake it, but everybody else is fake. We are different from them.” (Participant 9) |
| “You are already aware that you are different. Some people just cannot handle that difference. They are intimidated. When they meet a colourful personality, they see you as a threat in some way.” (Participant 10) | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Özer, G.; Işık, İ.; Escartín, J. Is There Somebody Looking out for Me? A Qualitative Analysis of Bullying Experiences of Individuals Diagnosed with Bipolar Disorder. Int. J. Environ. Res. Public Health 2024, 21, 137. https://doi.org/10.3390/ijerph21020137
Özer G, Işık İ, Escartín J. Is There Somebody Looking out for Me? A Qualitative Analysis of Bullying Experiences of Individuals Diagnosed with Bipolar Disorder. International Journal of Environmental Research and Public Health. 2024; 21(2):137. https://doi.org/10.3390/ijerph21020137
Chicago/Turabian StyleÖzer, Gülüm, İdil Işık, and Jordi Escartín. 2024. "Is There Somebody Looking out for Me? A Qualitative Analysis of Bullying Experiences of Individuals Diagnosed with Bipolar Disorder" International Journal of Environmental Research and Public Health 21, no. 2: 137. https://doi.org/10.3390/ijerph21020137