
Changes in Sexual Behavior and Satisfaction and Violent Behavior during COVID-19 Lockdown: Explorative Results from the Italian Cross-Sectional Study of the I-SHARE Multi-Country Project



Abstract
:1. Introduction
2. Aims
3. Materials and Methods
3.1. Study Design and Participants
3.2. Data Collection
3.3. Data Analysis
4. Results
5. Discussion
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Violato, M.; Pollard, J.; Lloyd, A.; Roope, L.S.J.; Duch, R.; Becerra, M.F.; Clarke, P.M. The COVID-19 Pandemic and Health-Related Quality of Life across 13 High- and Low-Middle-Income Countries: A Cross-Sectional Analysis. PLoS Med. 2023, 20, e1004146. [Google Scholar] [CrossRef] [PubMed]
- González-Monroy, C.; Gómez-Gómez, I.; Olarte-Sánchez, C.M.; Motrico, E. Eating Behaviour Changes during the COVID-19 Pandemic: A Systematic Review of Longitudinal Studies. Int. J. Environ. Res. Public Health 2021, 18, 11130. [Google Scholar] [CrossRef] [PubMed]
- van Doremalen, N.; Bushmaker, T.; Morris, D.H.; Holbrook, M.G.; Gamble, A.; Williamson, B.N.; Tamin, A.; Harcourt, J.L.; Thornburg, N.J.; Gerber, S.I.; et al. Aerosol and Surface Stability of SARS-CoV-2 as Compared with SARS-CoV-1. N. Engl. J. Med. 2020, 382, 1564–1567. [Google Scholar] [CrossRef]
- Eleuteri, S.; Terzitta, G. Sexuality during the COVID-19 Pandemic: The Importance of Internet. Sexologies 2021, 30, e55–e60. [Google Scholar] [CrossRef]
- Balzarini, R.N.; Muise, A.; Zoppolat, G.; Bartolomeo, A.A.D.; Rodrigues, D.L.; Alonso-Ferres, M.; Urganci, B.; Debrot, A.; Pichayayothin, N.; Dharma, C.; et al. Love in the Time of COVID: Perceived Partner Responsiveness Buffers People from Lower Relationship Quality Associated with COVID-Related Stressors. Soc. Psychol. Personal. Sci. 2023, 14, 342–355. [Google Scholar] [CrossRef]
- Luetke, M.; Hensel, D.; Herbenick, D.; Rosenberg, M. Romantic Relationship Conflict Due to the COVID-19 Pandemic and Changes in Intimate and Sexual Behaviors in a Nationally Representative Sample of American Adults. J. Sex Marital Ther. 2020, 46, 747–762. [Google Scholar] [CrossRef]
- Qaderi, K.; Yazdkhasti, M.; Zangeneh, S.; Behbahani, B.M.; Kalhor, M.; Shamsabadi, A.; Jesmani, Y.; Norouzi, S.; Kajbafvala, M.; Khodavirdilou, R.; et al. Changes in Sexual Activities, Function, and Satisfaction during the COVID-19 Pandemic Era: A Systematic Review and Meta-Analysis. Sex. Med. 2023, 11, qfad005. [Google Scholar] [CrossRef] [PubMed]
- Omar, S.S.; Dawood, W.; Eid, N.; Eldeeb, D.; Munir, A.; Arafat, W. Psychological and Sexual Health During the COVID-19 Pandemic in Egypt: Are Women Suffering More? Sex. Med. 2021, 9, 100295. [Google Scholar] [CrossRef]
- Hessami, K.; Sayegh, N.; Abdolmaleki, A.S.; Bakht, S.; Qaderi, S.; Darabi, M.; Shamsi, T.; Bagheri, F. Women’s Sexual Function before and during COVID-19 Pandemic: A Systematic Review and Meta-analysis. J. Obstet. Gynaecol. Res. 2022, 48, 2285–2295. [Google Scholar] [CrossRef]
- Ibarra, F.P.; Mehrad, M.; Di Mauro, M.; Godoy, M.F.P.; Cruz, E.G.; Nilforoushzadeh, M.A.; Russo, G.I. Impact of the COVID-19 Pandemic on the Sexual Behavior of the Population. The Vision of the East and the West. Int. Braz J. Urol Off. J. Braz. Soc. Urol. 2020, 46, 104–112. [Google Scholar] [CrossRef]
- Hall, B.J.; Tucker, J.D. Surviving in Place: The Coronavirus Domestic Violence Syndemic. Asian J. Psychiatry 2020, 53, 102179. [Google Scholar] [CrossRef]
- Fawole, O.I.; Okedare, O.O.; Reed, E. Home Was Not a Safe Haven: Women’s Experiences of Intimate Partner Violence during the COVID-19 Lockdown in Nigeria. BMC Womens Health 2021, 21, 32. [Google Scholar] [CrossRef]
- Walsh, A.R.; Sullivan, S.; Stephenson, R. Intimate Partner Violence Experiences during COVID-19 among Male Couples. J. Interpers. Violence 2022, 37, NP14166–NP14188. [Google Scholar] [CrossRef] [PubMed]
- Toller Erausquin, J.; Tan, R.K.J.; Uhlich, M.; Francis, J.M.; Kumar, N.; Campbell, L.; Zhang, W.H.; Hlatshwako, T.G.; Kosana, P.; Shah, S.; et al. The International Sexual Health And REproductive Health during COVID-19 (I-SHARE) Study: A Multicountry Analysis of Adults from 30 Countries Prior to and During the Initial Coronavirus Disease 2019 Wave. Clin. Infect. Dis. Off. Publ. Infect. Dis. Soc. Am. 2022, 75, e991–e999. [Google Scholar] [CrossRef]
- Ojeahere, M.I.; Kumswa, S.K.; Adiukwu, F.; Plang, J.P.; Taiwo, Y.F. Intimate Partner Violence and Its Mental Health Implications Amid COVID-19 Lockdown: Findings Among Nigerian Couples. J. Interpers. Violence 2022, 37, NP15434–NP15454. [Google Scholar] [CrossRef]
- Huldani, H.; Kamal Abdelbasset, W.; Abdalkareem Jasim, S.; Suksatan, W.; Turki Jalil, A.; Thangavelu, L.; Fakri Mustafa, Y.; Karami, M. Intimate Partner Violence against Pregnant Women during the COVID-19 Pandemic: A Systematic Review and Meta-Analysis. Women Health 2022, 62, 556–564. [Google Scholar] [CrossRef]
- McNeil, A.; Hicks, L.; Yalcinoz-Ucan, B.; Browne, D.T. Prevalence & Correlates of Intimate Partner Violence During COVID-19: A Rapid Review. J. Fam. Violence 2023, 38, 241–261. [Google Scholar] [CrossRef] [PubMed]
- ISTAT. Istat La Violenza Contro Le Donne Dentro e Fuori La Famiglia [Violence against Women inside and Outside the Family]; ISTAT: Rome, Italy, 2015.
- Pomicino, L.; Beltramini, L.; Romito, P. Freeing Oneself From Intimate Partner Violence: A Follow-Up of Women Who Contacted an Anti-Violence Center in Italy. Violence Women 2019, 25, 925–944. [Google Scholar] [CrossRef] [PubMed]
- Romito, P.; Pellegrini, M.; Saurel-Cubizolles, M.-J. Intimate Partner Violence Against Women During the COVID-19 Lockdown in Italy: A Multicenter Survey Involving Anti-Violence Centers. Violence Women 2022, 28, 2186–2203. [Google Scholar] [CrossRef]
- Mitchell, K.R.; Lewis, R.; O’Sullivan, L.F.; Fortenberry, J.D. What is Sexual Wellbeing and Why Does it Matter for Public Health? Lancet Public Health 2021, 6, e608–e613. [Google Scholar] [CrossRef]
- Michielsen, K.; Larrson, E.C.; Kågesten, A.; Erausquin, J.T.; Griffin, S.; de Velde, S.V.; Tucker, J.D. International Sexual Health And REproductive Health (I-SHARE) Survey during COVID-19: Study Protocol for Online National Surveys and Global Comparative Analyses. Sex. Transm. Infect. 2021, 97, 88–92. [Google Scholar] [CrossRef]
- DPCM 09 Marzo 2020, Ulteriori Disposizioni Attuative Del Decreto-Legge 23 Febbraio 2020, n. 6, Recante Misure Urgenti in Materia di Contenimento e Gestione Dell’emergenza Epidemiologica da COVID-19, Applicabili Sull’intero Territorio Nazionale. Available online: https://www.gazzettaufficiale.it/eli/id/2020/03/09/20A01558/sg (accessed on 5 December 2023).
- Longobardi, C.; Morese, R.; Fabris, M.A. COVID-19 Emergency: Social Distancing and Social Exclusion as Risks for Suicide Ideation and Attempts in Adolescents. Front. Psychol. 2020, 11, 551113. [Google Scholar] [CrossRef]
- Brooks, S.K.; Webster, R.K.; Smith, L.E.; Woodland, L.; Wessely, S.; Greenberg, N.; Rubin, G.J. The Psychological Impact of Quarantine and How to Reduce It: Rapid Review of the Evidence. Lancet 2020, 395, 912–920. [Google Scholar] [CrossRef] [PubMed]
- World Economic Forum One in Two People Globally Lost Income due to the Pandemic. Available online: https://www.weforum.org/agenda/2021/05/how-many-people-experienced-a-lower-income-due-to-covid-19/ (accessed on 5 December 2023).
- Moynihan, R.; Sanders, S.; Michaleff, Z.A.; Scott, A.M.; Clark, J.; To, E.J.; Jones, M.; Kitchener, E.; Fox, M.; Johansson, M.; et al. Impact of COVID-19 Pandemic on Utilisation of Healthcare Services: A Systematic Review. BMJ Open 2021, 11, e045343. [Google Scholar] [CrossRef] [PubMed]
- Panzeri, M.; Ferrucci, R.; Cozza, A.; Fontanesi, L. Changes in Sexuality and Quality of Couple Relationship During the COVID-19 Lockdown. Front. Psychol. 2020, 11, 565823. [Google Scholar] [CrossRef]
- Masoudi, M.; Maasoumi, R.; Bragazzi, N.L. Effects of the COVID-19 Pandemic on Sexual Functioning and Activity: A Systematic Review and Meta-Analysis. BMC Public Health 2022, 22, 189. [Google Scholar] [CrossRef]
- Nimbi, F.M.; Tripodi, F.; Rossi, R.; Michetti, P.M.; Simonelli, C. Which Psychosocial Variables Affect Drive the Most? Analysis of Sexual Desire in a Group of Italian Men. Int. J. Impot. Res. 2019, 31, 410–423. [Google Scholar] [CrossRef] [PubMed]
- Galizia, R.; Theodorou, A.; Simonelli, C.; Lai, C.; Nimbi, F.M. Sexual Satisfaction Mediates the Effects of the Quality of Dyadic Sexual Communication on the Degree of Perceived Sexual Desire Discrepancy. Healthcare 2023, 11, 648. [Google Scholar] [CrossRef] [PubMed]
- Räuchle, J.; Briken, P.; Schröder, J.; Ivanova, O. Sexual and Reproductive Health during the COVID-19 Pandemic: Results from a Cross-Sectional Online Survey in Germany. Int. J. Environ. Res. Public Health 2022, 19, 1428. [Google Scholar] [CrossRef] [PubMed]
- Mercer, C.H.; Clifton, S.; Riddell, J.; Tanton, C.; Freeman, L.; Copas, A.J.; Dema, E.; Bosó Pérez, R.; Gibbs, J.; Macdowall, W.; et al. Impacts of COVID-19 on Sexual Behaviour in Britain: Findings from a Large, Quasi-Representative Survey (Natsal-COVID). Sex. Transm. Infect. 2022, 98, 469–477. [Google Scholar] [CrossRef] [PubMed]
- Hensel, D.J.; Rosenberg, M.; Luetke, M.; Fu, T.; Herbenick, D. The Impact of Household Context on Self-Perceived Changes in Solo and Partnered Sexual Behaviors during the COVID-19 Pandemic: Findings from a U.S. Probability Survey. Arch. Sex. Behav. 2023, 52, 655–667. [Google Scholar] [CrossRef] [PubMed]
- Lau, W.K.-W.; Ngan, L.H.-M.; Chan, R.C.-H.; Wu, W.K.-K.; Lau, B.W.-M. Impact of COVID-19 on Pornography Use: Evidence from Big Data Analyses. PLoS ONE 2021, 16, e0260386. [Google Scholar] [CrossRef] [PubMed]
- Wodda, A. Stranger Danger! J. Fam. Strengths 2018, 18, 3. [Google Scholar] [CrossRef]
- Campbell, L.; Tan, R.K.J.; Uhlich, M.; Francis, J.M.; Mark, K.; Miall, N.; Eleuteri, S.; Gabster, A.; Shamu, S.; Plášilová, L.; et al. Intimate Partner Violence During COVID-19 Restrictions: A Study of 30 Countries From the I-SHARE Consortium. J. Interpers. Violence 2023, 38, 7115–7142. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Variables | Participants (n = 329) | |
|---|---|---|
| M ± ds (Min–Max) | ||
| Age | 32.26 ± 10.27 (19–79) Q3–Q1: 25–38 | |
| n (%) | ||
| Sex Assigned at Birth | Female | 216 (65.65) |
| Male | 113 (34.35) | |
| Gender | Female | 207 (62.92) |
| Male | 110 (33.43) | |
| Both | 10 (3.04) | |
| Neither of the two | 2 (0.61) | |
| Sexual Orientation | Heterosexual | 237 (71.17) |
| Bisexual | 31 (9.31) | |
| Homosexual | 50 (15.02) | |
| Pansexual | 11 (3.34) | |
| Asexual | 4 (1.22) | |
| Relationship Status | Single | 105 (31.91) |
| In a relationship | 224 (68.09) | |
| Number of Children | 0 | 284 (86.32) |
| 1 | 27 (8.21) | |
| 2 | 15 (4.56) | |
| 3+ | 3 (0.91) | |
| Education Level | Middle School | 4 (1.22) |
| High School | 48 (14.59) | |
| University and Postgrad courses | 277 (84.19) | |
| Work Status | Employed | 120 (36.47) |
| Freelance | 40 (12.16) | |
| Unemployed | 22 (6.69) | |
| Fragmentary work | 37 (11.25) | |
| Retired | 2 (0.61) | |
| Student | 105 (32.11) | |
| Socio-economic status (1 year before COVID-19 pandemic) | Low | 17 (5.17) |
| Low/Middle | 62 (18.84) | |
| Middle | 130 (39.51) | |
| Middle/High | 89 (27.05) | |
| High | 12 (3.65) | |
| Prefer not to say | 19 (5.78) | |
| Income status changes in first COVID-19 wave | Decrease | 112 (34.04) |
| No change | 205 (62.31) | |
| Increase | 12 (3.65) | |
| Residence | Metropolis | 102 (31) |
| City | 108 (32.83) | |
| Suburbs | 15 (4.56) | |
| Small town/village | 98 (29.79) | |
| Rural/remote area | 6 (1.82) | |
| Ethnicity | White/Caucasian | 321 (97.57) |
| Latin-American/Hispanic | 4 (1.22) | |
| Black/African/Afroamerican | 2 (0.61) | |
| Prefer not to say | 2 (0.61) |
| Variables | Participants (n = 329) | |
|---|---|---|
| n (%) | ||
| Have you ever had a sexual experience? | No | 16 (4.86) |
| By “sexual experience” we mean any kind of experience that you felt was sexually arousing. It could be kissing, touching, intercourse, masturbation, watching sexually explicit images, or any other form of sex | Yes | 313 (95.14) |
| Sexual problems | Hypoactive/low sexual desire | 100 (30.40) |
| Hyperactive/increase in sexual desire | 20 (6.08) | |
| Low sexual excitation/arousal | 9 (2.74) | |
| Persistent and not wanted genital arousal (in absence of sexual interest) | 4 (1.22) | |
| Erection difficulties | 7 (2.13) | |
| Orgasm difficulties/delayed/impossible ejaculation | 12 (3.65) | |
| Premature ejaculation | 6 (1.82) | |
| Pain during intercourses | 10 (3.04) | |
| Difficulties in allowing vaginal/anal penetration | 3 (0.91) | |
| No sexual problems | 156 (47.42) | |
| Other problems (no specified) | 2 (0.61) | |
| Sexual Distress | No problem | 176 (53.50) |
| Did this difficulty represent a problem for you? | A little problem | 56 (17.02) |
| A problem | 54 (16.41) | |
| A significant problem | 29 (8.81) | |
| A very important problem | 15 (4.56) | |
| Did the COVID-19 social distancing measures make it more difficult to access condoms? | No | 128 (38.91) |
| Yes | 11 (3.34) | |
| Not applicable to my experience—I do not normally use condoms | 138 (41.95) | |
| Missing | 52 (15.81) | |
| Are you or your partner currently doing something to avoid or delay a pregnancy, including condoms, contraceptive methods, traditional methods, etc.? | No | 39 (11.85) |
| Yes, always | 99 (30.09) | |
| Yes, most of the times | 17 (5.17) | |
| Yes, sometimes | 5 (1.52) | |
| Missing | 196 (59.57) | |
| During the COVID-19 social distancing measures have you wanted a test for HIV or another sexually transmitted infection? | No | 276 (83.89) |
| Yes | 21 (6.38) | |
| Missing | 32 (9.73) | |
| Has the COVID-19 situation stopped or hindered you from accessing a test for HIV or another sexually transmitted infection? | No | 131 (39.82) |
| Yes | 13 (3.95) | |
| Missing | 185 (56.23) |
| Variable | Pre-COVID-19 (about 3 Months before) | During COVID-19 Lockdown | After COVID-19 Lockdown | F (1,312) | Sign | |
|---|---|---|---|---|---|---|
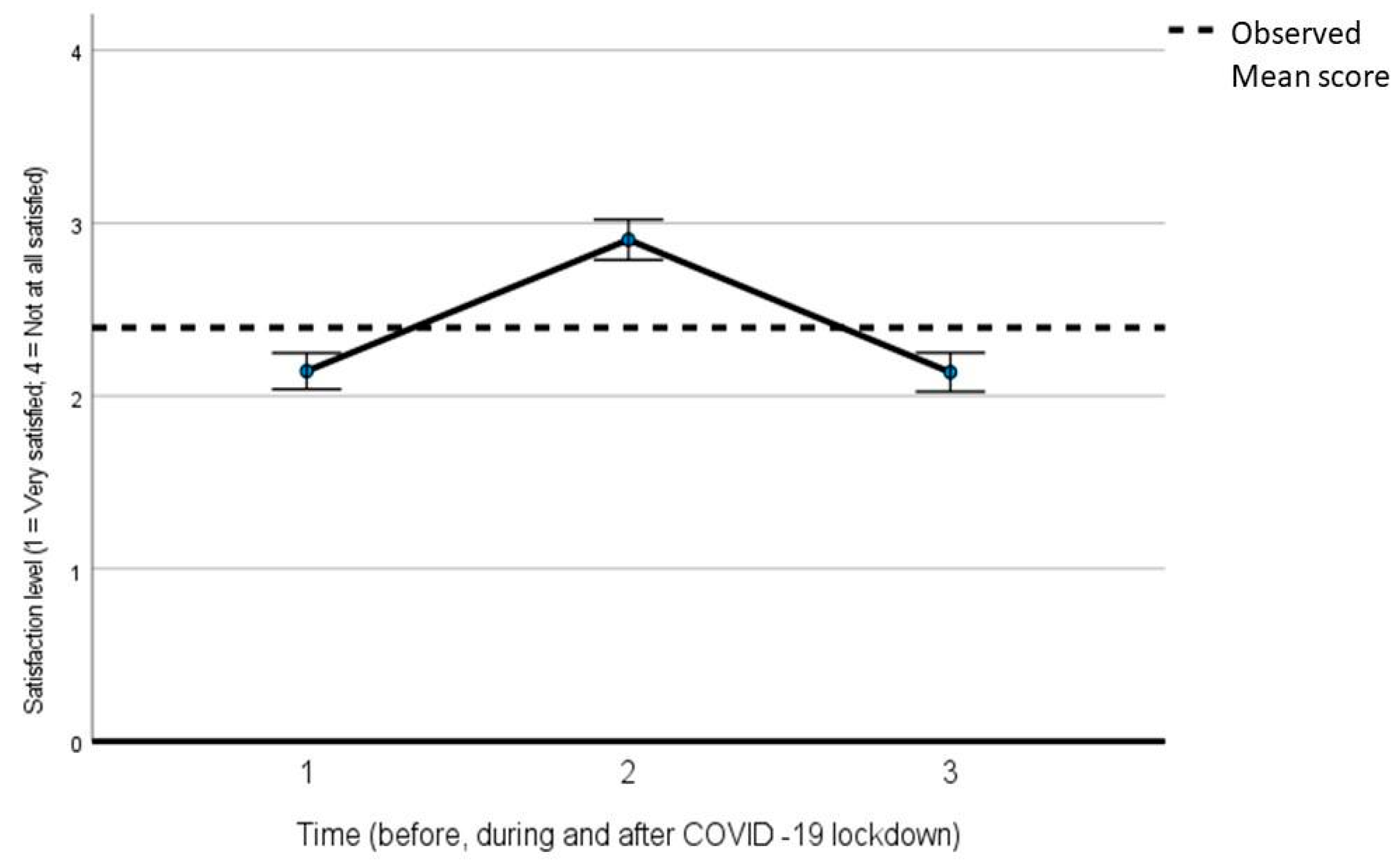
| Satisfaction with Sexual Life | Very satisfied | 88 (26.75) | 37 (11.25) | 100 (30.40) | 175.463 | <0.001 |
| Quite satisfied | 124 (37.59) | 77 (23.40) | 112 (34.04) | |||
| Not very satisfied | 69 (20.97) | 78 (23.71) | 59 (17.93) | |||
| Not at all satisfied | 32 (9.73) | 121 (36.78) | 42 (12.77) | |||
| Missing | 16 (4.86) | 16 (4.86) | 16 (4.86) | |||
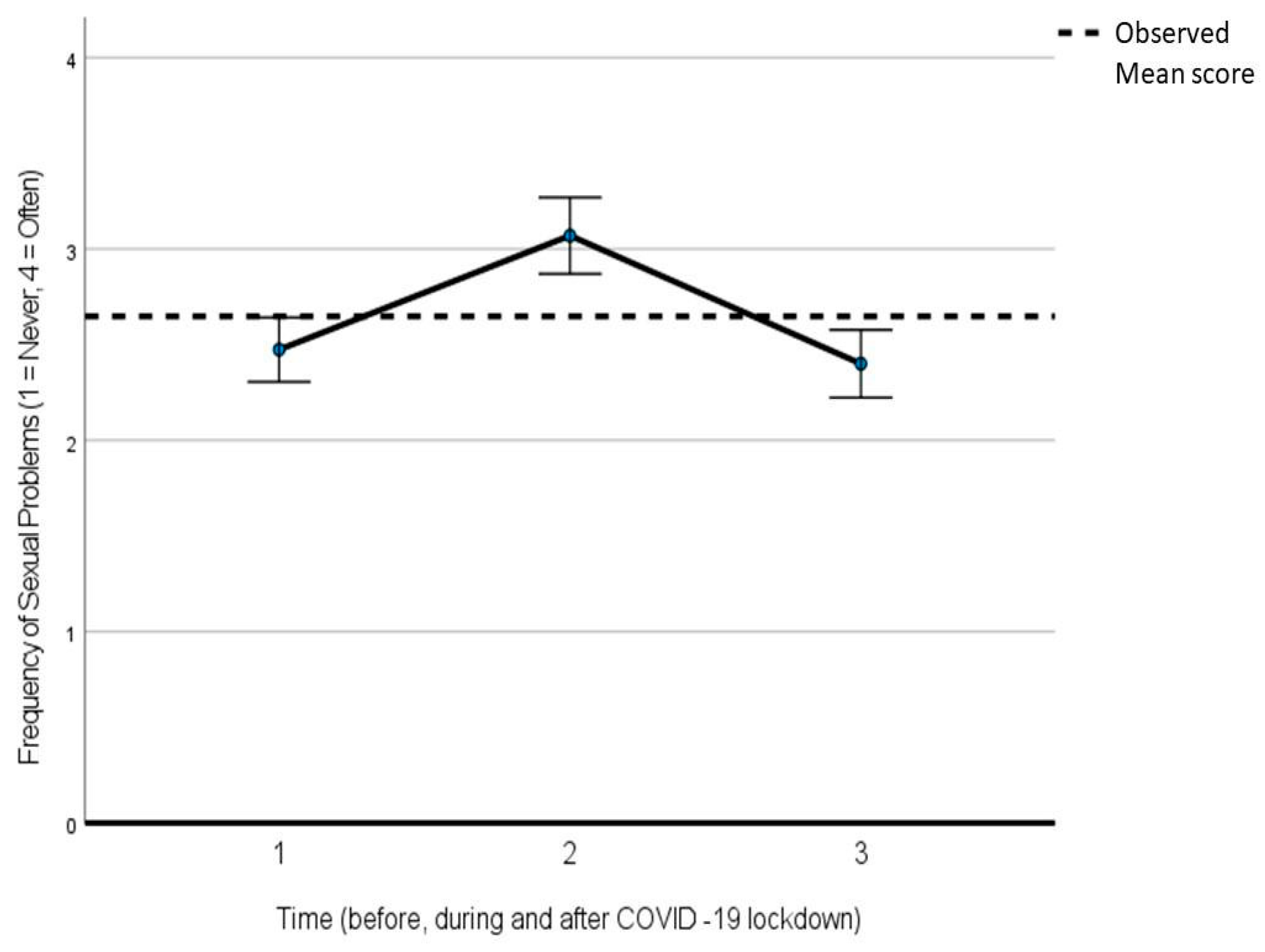
| Frequency of Sexual problems | Never | 105 (31.91) | 88 (26.75) | 123 (37.39) | 50.494 | <0.001 |
| Once | 29 (8.81) | 14 (4.26) | 19 (5.78) | |||
| Sometimes | 86 (26.14) | 54 (16.41) | 68 (20.67) | |||
| Often | 18 (5.47) | 24 (7.29) | 23 (6.99) | |||
| Not applicable to my situation | 41 (12.46) | 93 (28.27) | 43 (13.07) | |||
| Missing | 50 (15.20) | 56 (17.02) | 53 (16.11) |
| Pre-COVID-19 (about 3 Months before) | During COVID-19 Lockdown (Compared to before COVID-19) | After COVID-19 Lockdown (Compared to during Lockdown) | ||||
|---|---|---|---|---|---|---|
| Hugged, kissed, held hands with, or cuddled with your steady partner | Never | 12 (3.65) | Much less | 86 (26.14) | Much less | 13 (3.95) |
| Once a month or less | 8 (2.43) | A bit less | 32 (9.73) | A bit less | 30 (9.12) | |
| 2–4 times per month | 27 (8.21) | No difference from before | 58 (17.63) | No difference from before | 80 (24.32) | |
| 2–3 times per week | 50 (15.20) | A bit more | 29 (8.81) | A bit more | 49 (14.89) | |
| 4 or more times per week | 140 (42.55) | Much more | 23 (6.99) | Much more | 62 (18.84) | |
| Missing | 92 (27.96) | Missing | 101 (30.70) | Missing | 95 (28.88) | |
| Engaged in sexual activities with your steady partner | Never | 17 (5.17) | Much less | 94 (28.57) | Much less | 20 (6.08) |
| Once a month or less | 15 (4.56) | A bit less | 31 (9.42) | A bit less | 29 (8.81) | |
| 2–4 times per month | 97 (29.48) | No difference from before | 75 (22.80) | No difference from before | 82 (24.92) | |
| 2–3 times per week | 78 (23.71) | A bit more | 19 (5.78) | A bit more | 59 (17.93) | |
| 4 or more times per week | 33 (10.03) | Much more | 8 (2.43) | Much more | 44 (13.37) | |
| Missing | 89 (27.05) | Missing | 102 (31) | Missing | 95 (28.88) | |
| Used condoms/contraceptives when you had sex with your steady partner | Never | 104 (31.61) | Much less | 26 (7.90) | Much less | 20 (6.08) |
| Rarely | 9 (2.74) | A bit less | 5 (1.52) | A bit less | 3 (0.91) | |
| Sometimes | 17 (5.17) | No difference from before | 175 (53.19) | No difference from before | 186 (56.53) | |
| Most of the time | 17 (5.17) | A bit more | 2 (0.61) | A bit more | 7 (2.13) | |
| Always | 86 (26.14) | Much more | 2 (0.61) | Much more | 10 (3.04) | |
| Missing | 96 (29.18) | Missing | 119 (36.17) | Missing | 103 (31.31) | |
| Masturbation | Never | 52 (15.81) | Much less | 26 (7.90) | Much less | 33 (10.03) |
| Once a month or less | 45 (13.68) | A bit less | 43 (13.07) | A bit less | 64 (19.45) | |
| 2–4 times per month | 81 (24.62) | No difference from before | 128 (38.91) | No difference from before | 129 (39.21) | |
| 2–3 times per week | 85 (25.84) | A bit more | 67 (20.36) | A bit more | 54 (16.41) | |
| 4 or more times per week | 33 (10.03) | Much more | 31 (9.42) | Much more | 14 (4.26) | |
| Missing | 33 (10.03) | Missing | 34 (10.33) | Missing | 35 (10.64) | |
| Engaged in sexual activities with casual partners | Never | 231 (70.21) | Much less | 55 (16.72) | Much less | 19 (5.78) |
| Once a month or less | 26 (7.90) | A bit less | 4 (1.22) | A bit less | 4 (1.22) | |
| 2–4 times per month | 27 (8.21) | No difference from before | 212 (64.44) | No difference from before | 211 (64.13) | |
| 2–3 times per week | 7 (2.13) | A bit more | 2 (0.61) | A bit more | 35 (10.64) | |
| 4 or more times per week | 0 | Much more | 3 (0.91) | Much more | 8 (2.43) | |
| Missing | 38 (11.55) | Missing | 53 (16.11) | Missing | 52 (15.81) | |
| Used condoms/contraceptives when you had sex with casual partners | Never | 42 (12.77) | Much less | 10 (3.04) | Much less | 10 (3.04) |
| Rarely | 11 (3.34) | A bit less | 0 | A bit less | 3 (0.91) | |
| Sometimes | 11 (3.34) | No difference from before | 91 (27.66) | No difference from before | 91 (27.66) | |
| Most of the time | 20 (6.08) | A bit more | 2 (0.61) | A bit more | 3 (0.91) | |
| Always | 36 (10.94) | Much more | 1 (0.30) | Much more | 4 (1.22) | |
| Missing | 209 (63.53) | Missing | 225 (68.39) | Missing | 218 (66.26) | |
| Sent or received naked/semi-naked pictures or videos | Never | 170 (51.67) | Much less | 19 (5.78) | Much less | 43 (13.07) |
| Once a month or less | 65 (19.76) | A bit less | 10 (3.04) | A bit less | 34 (10.33) | |
| 2–4 times per month | 30 (9.12) | No difference from before | 169 (51.37) | No difference from before | 175 (53.19) | |
| 2–3 times per week | 20 (6.08) | A bit more | 56 (17.02) | A bit more | 25 (7.60) | |
| 4 or more times per week | 8 (2.43) | Much more | 30 (9.12) | Much more | 7 (2.13) | |
| Missing | 36 (10.94) | Missing | 45 (13.68) | Missing | 45 (13.68) | |
| Had sex in exchange for money, material goods, favors, drugs, or shelter | Never | 291 (88.45) | Much less | 7 (2.13) | Much less | 5 (1.52) |
| Once a month or less | 2 (0.61) | A bit less | 0 | A bit less | 0 | |
| 2–4 times per month | 1 (0.30) | No difference from before | 264 (80.24) | No difference from before | 266 (80.85) | |
| 2–3 times per week | 0 | A bit more | 0 | A bit more | 1 (0.30) | |
| 4 or more times per week | 1 (0.30) | Much more | 1 (0.30) | Much more | 0 | |
| Missing | 34 (10.33) | Missing | 57 (17.33) | Missing | 57 (17.33) | |
| Watched sexually explicit videos (pornography) | Never | 73 (22.19) | Much less | 27 (8.21) | Much less | 36 (10.94) |
| Once a month or less | 86 (26.14) | A bit less | 22 (6.69) | A bit less | 44 (13.37) | |
| 2–4 times per month | 64 (19.45) | No difference from before | 159 (48.33) | No difference from before | 176 (53.50) | |
| 2–3 times per week | 50 (15.20) | A bit more | 69 (20.97) | A bit more | 30 (9.12) | |
| 4 or more times per week | 27 (8.21) | Much more | 21 (6.38) | Much more | 12 (3.65) | |
| Missing | 29 (8.81) | Missing | 31 (9.42) | Missing | 31 (9.42) | |
| Performed/watched sexual acts on a webcam | Never | 268 (81.46) | Much less | 11 (3.34) | Much less | 19 (5.78) |
| Once a month or less | 21 (6.38) | A bit less | 2 (0.61) | A bit less | 6 (1.82) | |
| 2–4 times per month | 7 (2.13) | No difference from before | 241 (73.25) | No difference from before | 244 (74.16) | |
| 2–3 times per week | 1 (0.30) | A bit more | 17 (5.17) | A bit more | 5 (1.52) | |
| 4 or more times per week | 2 (0.61) | Much more | 8 (2.43) | Much more | 4 (1.22) | |
| Missing | 30 (9.12) | Missing | 50 (15.20) | Missing | 51 (15.50) | |
| Violence-Related Variables | Pre-COVID-19 (about 3 Months before) | During COVID-19 Lockdown | After COVID-19 Lockdown | F (1,312) | Sign | |
|---|---|---|---|---|---|---|
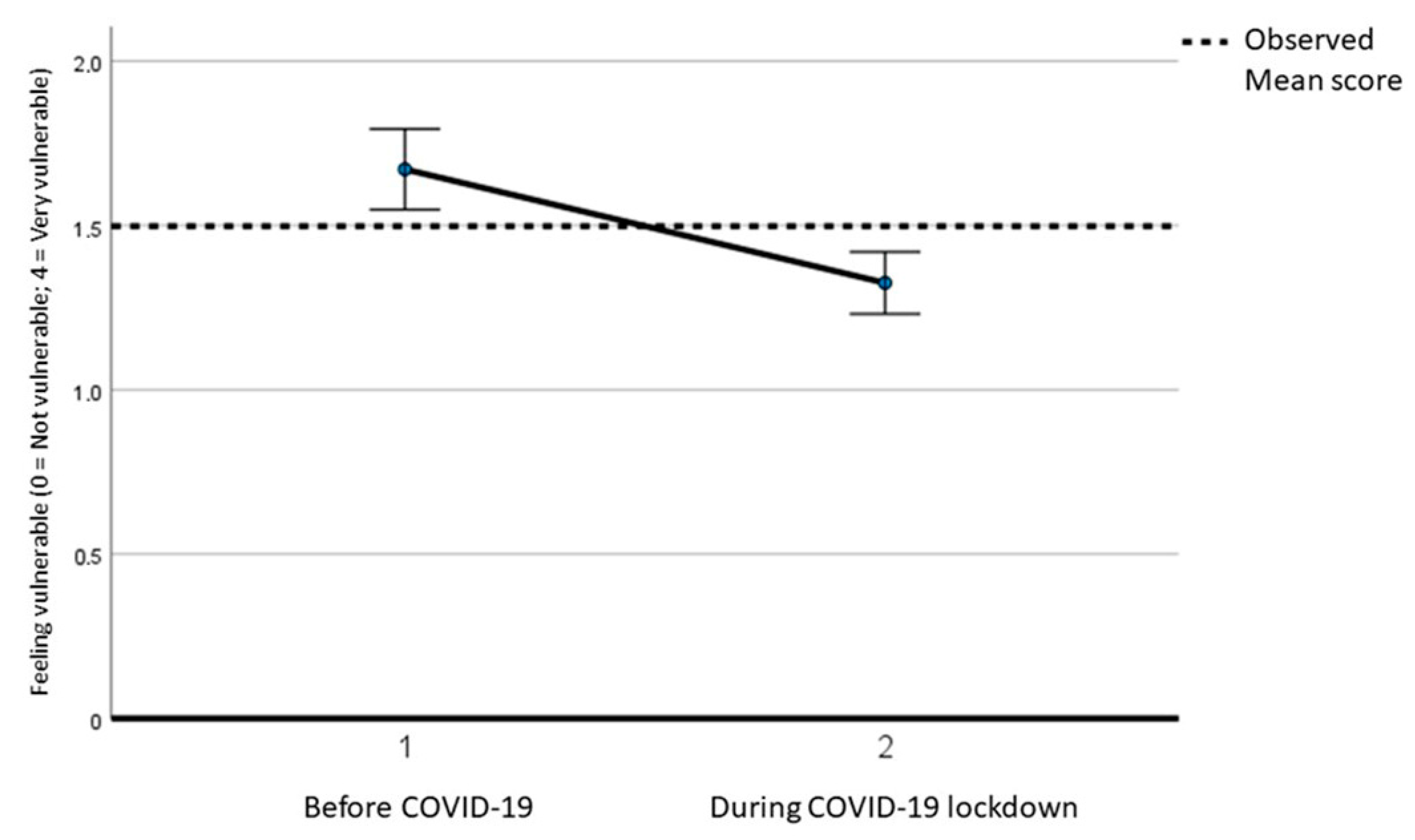
| How vulnerable did you feel for sexual harassment or sexual, physical, or emotional assault by someone who does not live in your house? | Not vulnerable | 194 (58.97) | 250 (75.99) | - | 37.574 | <0.001 |
| Slightly vulnerable | 46 (13.98) | 15 (4.65) | - | |||
| Neutral | 25 (7.60) | 21 (6.38) | - | |||
| A bit vulnerable | 28 (8.51) | 8 (2.43) | - | |||
| Very vulnerable | 5 (1.52) | 4 (1.22) | - | |||
| Missing | 31 (9.42) | 31 (9.42) | - | |||
| Has a partner tried to restrict (online or phone) contact with your family? | No | 243 (73.86) | 239 (72.64) | 244 (74.16) | 1.516 | 0.219 |
| Yes, once | 1 (0.30) | 2 (0.61) | 1 (0.30) | |||
| Yes, more than once | 3 (0.91) | 1 (0.30) | 1 (0.30) | |||
| Not applicable to my situation | 53 (16.11) | 55 (16.72) | 51 (15.50) | |||
| Missing | 29 (8.81) | 32 (9.73) | 32 (9.73) | |||
| Has a partner insulted you or made you feel bad about yourself? | No | 206 (62.61) | 206 (62.61) | 212 (64.44) | 2.156 | 0.143 |
| Yes, once | 38 (11.55) | 28 (8.51) | 30 (9.12) | |||
| Yes, more than once | 14 (4.26) | 20 (6.08) | 17 (5.17) | |||
| Not applicable to my situation | 39 (11.86) | 41 (12.46) | 38 (11.55) | |||
| Missing | 32 (9.73) | 34 (10.33) | 32 (9.73) | |||
| Has a partner ever not provided money to run the house or look after the children, but has money for other things? | No | 131 (39.82) | 127 (38.60) | 129 (39.21) | 0.106 | 0.745 |
| Yes, once | 1 (0.30) | 4 (1.22) | 1 (0.30) | |||
| Yes, more than once | 5 (1.52) | 1 (0.30) | 2 (0.61) | |||
| Not applicable to my situation | 141 (42.86) | 142 (43.16) | 143 (43.47) | |||
| Missing | 51 (15.50) | 55 (16.72) | 54 (16.41) | |||
| Has a partner slapped, pushed, hit, kicked, or choked you or thrown something at you that could hurt you? | No | 239 (72.64) | 218 (66.26) | 236 (71.73) | 0.199 | 0.656 |
| Yes, once | 4 (1.22) | 3 (0.91) | 5 (1.52) | |||
| Yes, more than once | 1 (0.30) | 1 (0.30) | 0 | |||
| Not applicable to my situation | 47 (14.29) | 68 (20.67) | 50 (15.20) | |||
| Missing | 38 (11.55) | 39 (11.85) | 38 (11.55) | |||
| Has a partner physically forced you to have sexual intercourse when you did not want to? | No | 240 (72.95) | 222 (67.48) | 242 (73.56) | 0 | 1 |
| Yes, once | 3 (0.91) | 4 (1.22) | 3 (0.91) | |||
| Yes, more than once | 0 | 0 | 1 (0.30) | |||
| Not applicable to my situation | 43 (13.07) | 61 (18.54) | 40 (12.16) | |||
| Missing | 43 (13.07) | 42 (12.77) | 43 (13.07) | |||
| Has a partner made you have sexual intercourse when you did not want to because you were afraid of what your partner might do? | No | 245 (74.47) | 218 (66.26) | 241 (73.25) | 1.604 | 0.207 |
| Yes, once | 7 (2.13) | 2 (0.61) | 5 (1.52) | |||
| Yes, more than once | 1 (0.30) | 1 (0.30) | 0 | |||
| Not applicable to my situation | 35 (10.64) | 63 (19.15) | 40 (12.16) | |||
| Missing | 41 (12.46) | 45 (13.68) | 43 (13.07) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nimbi, F.M.; Cavagnis, S.; Eleuteri, S. Changes in Sexual Behavior and Satisfaction and Violent Behavior during COVID-19 Lockdown: Explorative Results from the Italian Cross-Sectional Study of the I-SHARE Multi-Country Project. Int. J. Environ. Res. Public Health 2024, 21, 96. https://doi.org/10.3390/ijerph21010096
Nimbi FM, Cavagnis S, Eleuteri S. Changes in Sexual Behavior and Satisfaction and Violent Behavior during COVID-19 Lockdown: Explorative Results from the Italian Cross-Sectional Study of the I-SHARE Multi-Country Project. International Journal of Environmental Research and Public Health. 2024; 21(1):96. https://doi.org/10.3390/ijerph21010096
Chicago/Turabian StyleNimbi, Filippo Maria, Sara Cavagnis, and Stefano Eleuteri. 2024. "Changes in Sexual Behavior and Satisfaction and Violent Behavior during COVID-19 Lockdown: Explorative Results from the Italian Cross-Sectional Study of the I-SHARE Multi-Country Project" International Journal of Environmental Research and Public Health 21, no. 1: 96. https://doi.org/10.3390/ijerph21010096