
Evaluation of a Childhood Obesity Program Serving a High-Need Population in Brooklyn, New York Using Survival Analysis

(This article belongs to the Section Children's Health)
Abstract
:1. Introduction
2. Materials and Methods
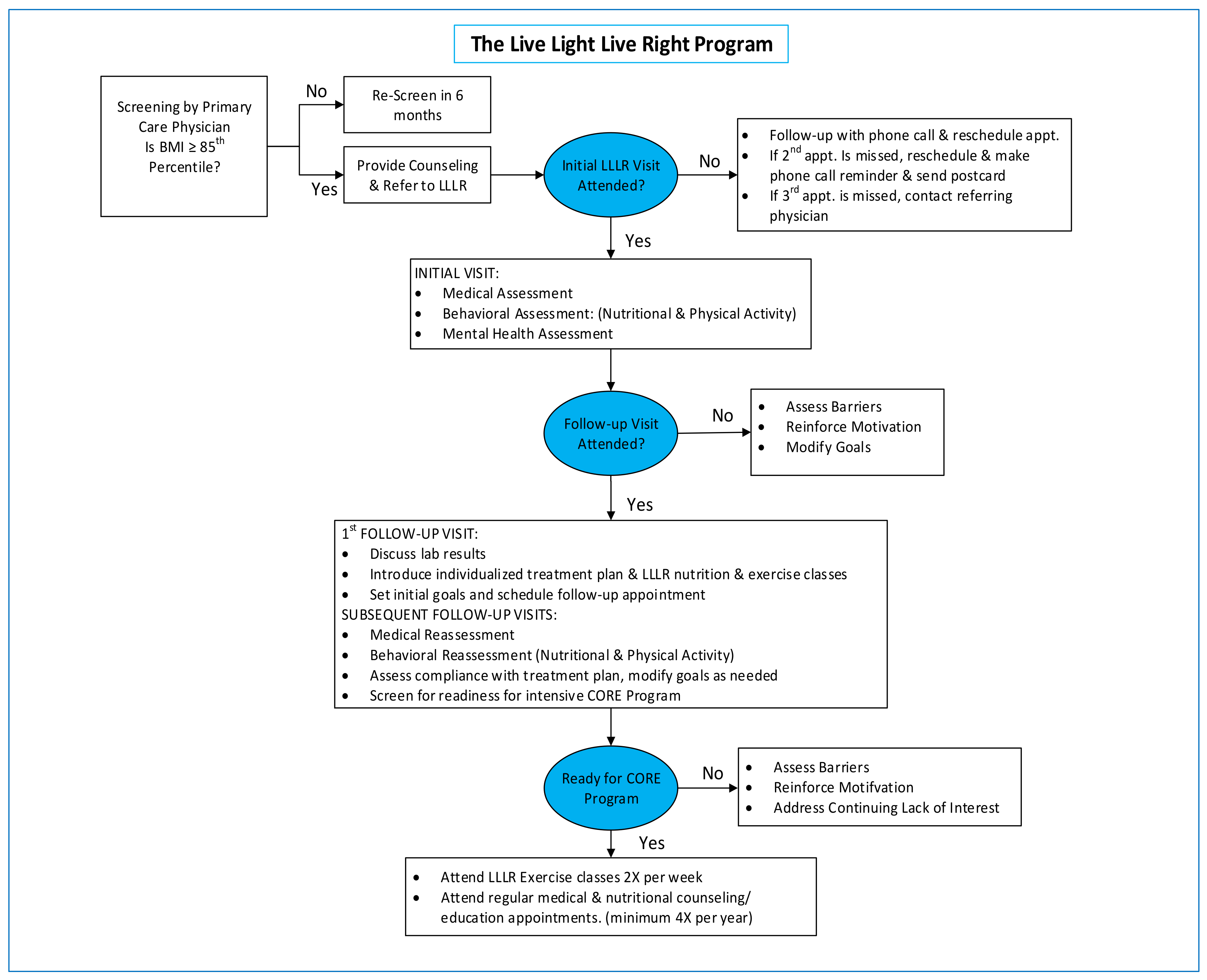
2.1. Intervention Methods
LLLR Individualized Treatment Model
2.2. Study Methods
Study Design
2.3. Subjects
2.3.1. Contact Hour Grouping (Main Predictor)
2.3.2. Event Endpoint (Primary Outcome)
2.3.3. Censoring
2.3.4. Measurement of Outcomes
2.3.5. Measurement of Covariates
2.4. Statistical Analysis
2.5. Survival Analysis
2.5.1. Bivariate Analysis
2.5.2. Multivariate Analysis
3. Results
3.1. Description of Sample
Distribution of Age in the Sample
3.2. Bivariate Analyses
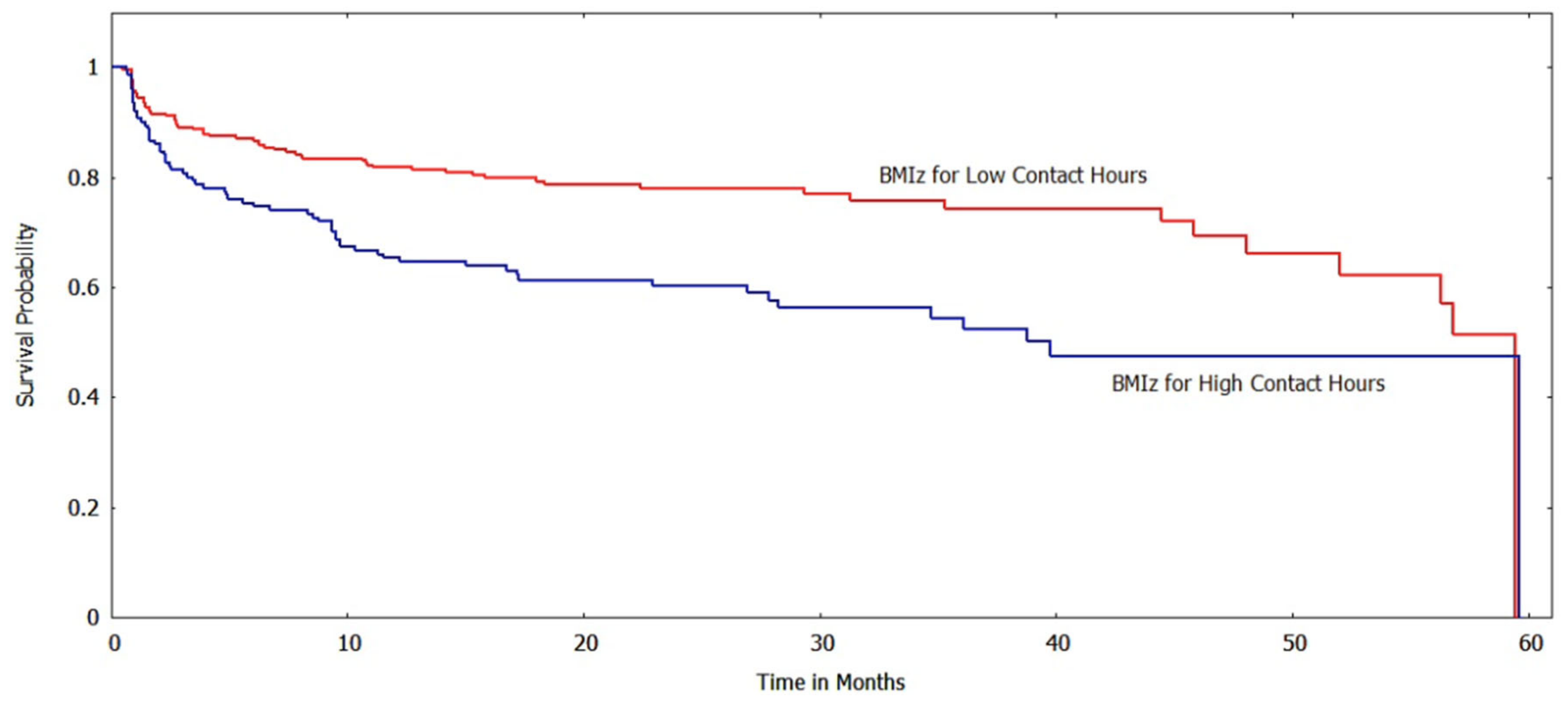
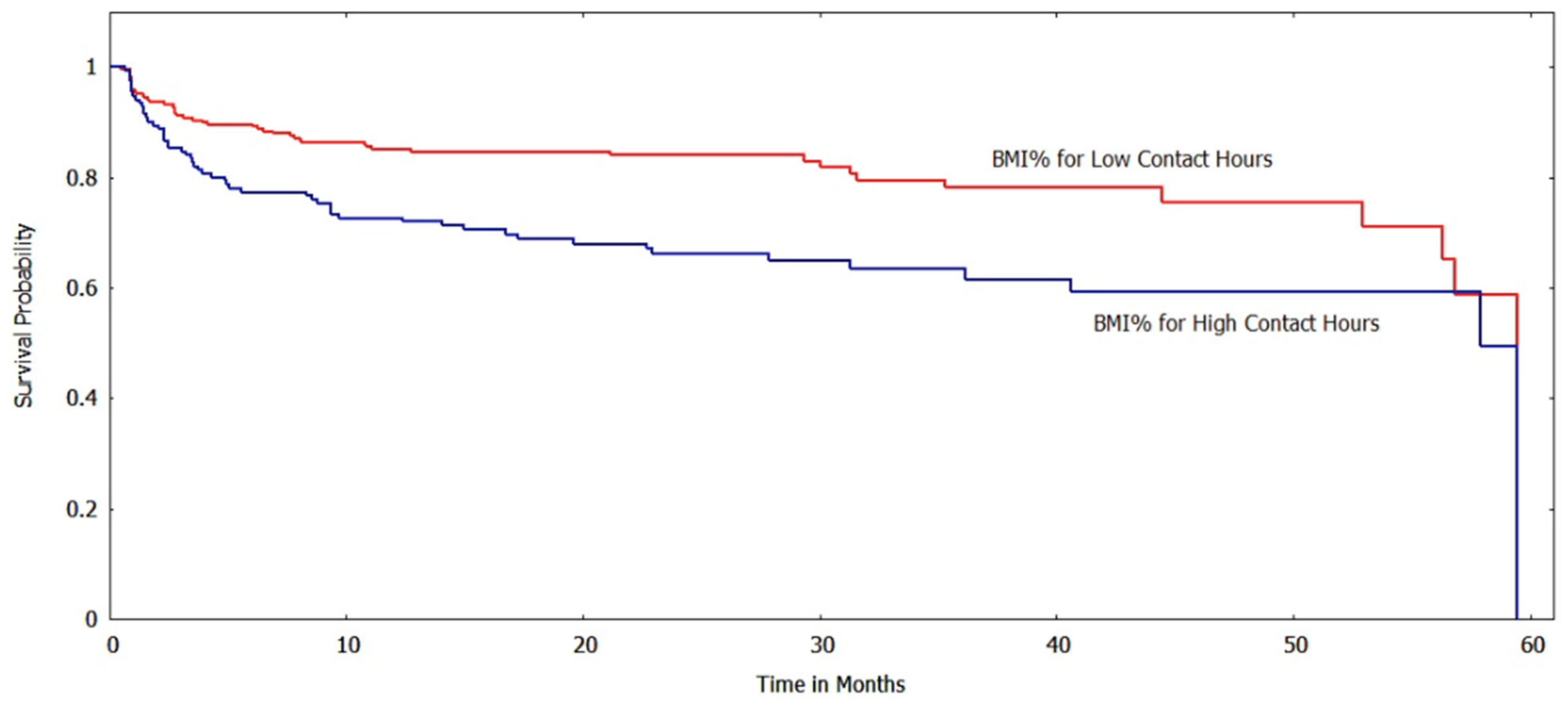
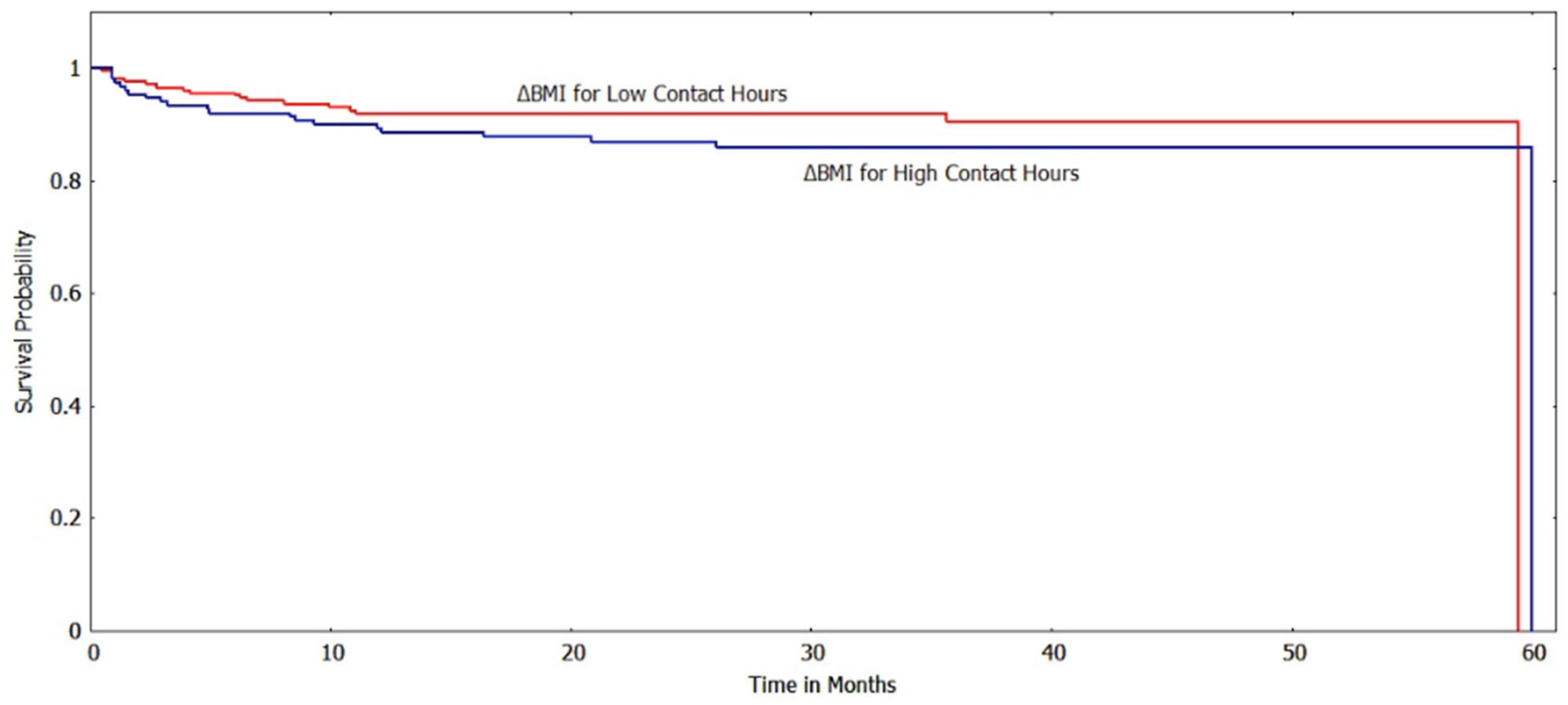
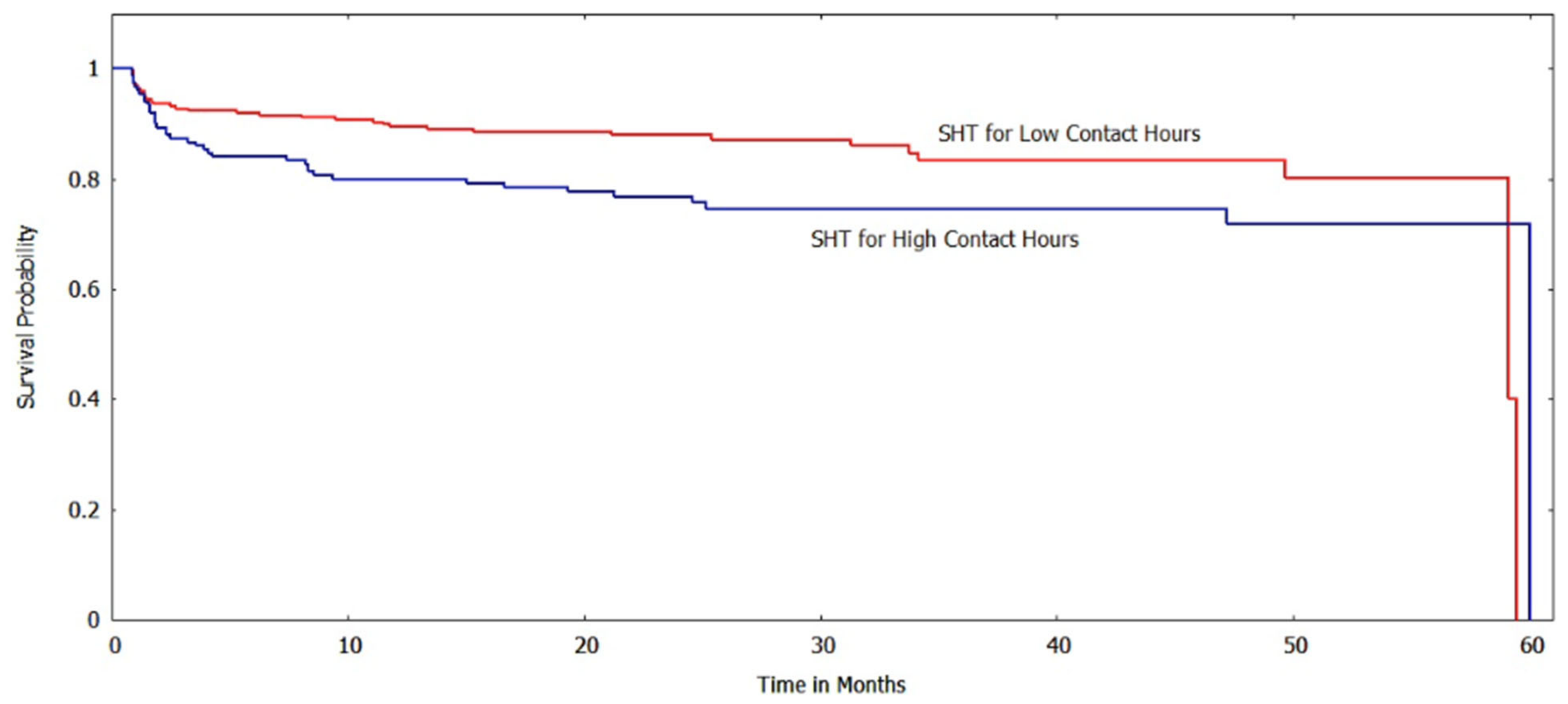
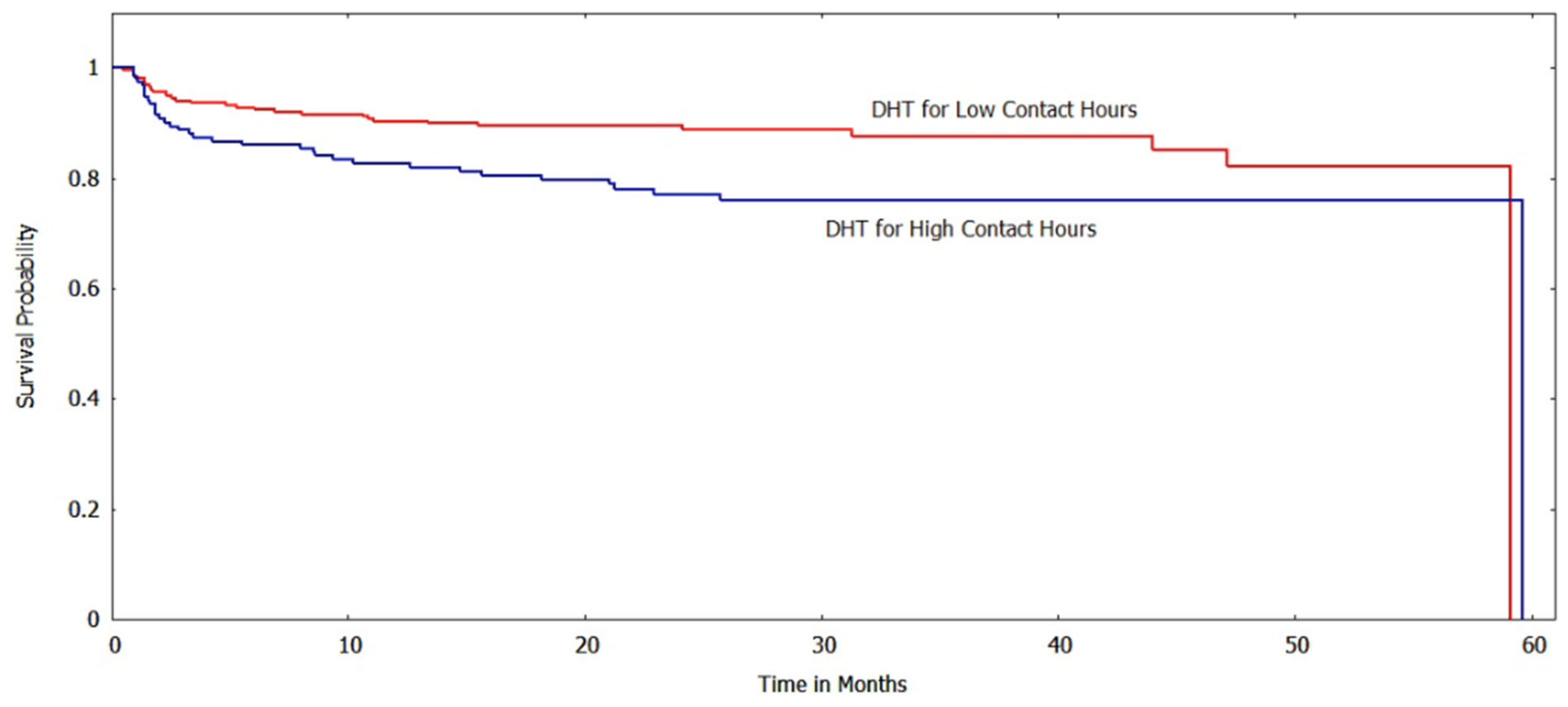
3.2.1. Kaplan-Meir Analyses
3.2.2. Mean Time Spent in the Improved State
3.2.3. Mean Times Getting to the Event
3.2.4. Multivariable Analyses
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Fryar, C.D.; Carroll, M.D.; Afful, J. Prevalence of Overweight, Obesity, and Severe Obesity among Children and Adolescents Aged 2–19 Years: United States, 1963–1965 through 2017–2018. NCHS Health E-Stats. 2020. Available online: https://www.cdc.gov/nchs/data/hestat/obesity-child-17-18/overweight-obesity-child-H.pdf (accessed on 14 March 2021).
- Day, S.E.; Konty, K.J.; Leventer-Roberts, M.; Nonas, C.; Harris, T.G. Severe Obesity Among Children in New York City Public Elementary and Middle Schools, School Years 2006–07 Through 2010–11. Prev. Chronic Dis. 2014, 11, E118. [Google Scholar] [CrossRef] [PubMed]
- King, L.; Hinterland, K.; Dragan, K.; Driver, C.; Harris, T.; Gwynn, R.; Bassett, M. Community Health Profiles 2018, Brooklyn Community District 16: Brownsville. 2018; 40, pp. 1–20. Available online: https://www.nyc.gov/assets/doh/downloads/pdf/data/2018chp-bk16.pdf (accessed on 4 January 2021).
- Hinterland, K.; Naidoo, M.; King, L.; Lewin, V.; Myerson, G.; Noumbissi, B.; Woodward, M.; Gould, L.H.; Gwynn, R.C.; Barbot, O.; et al. Community Health Profiles 2018, Brooklyn Community District 5: East New York and Starrett City. 2018; 29, pp. 1–20. Available online: https://www.nyc.gov/assets/doh/downloads/pdf/data/2018chp-bk5.pdf (accessed on 4 January 2021).
- Kelly, A.S.; Barlow, S.E.; Rao, G.; Inge, T.H.; Hayman, L.L.; Steinberger, J.; Urbina, E.M.; Ewing, L.J.; Daniels, S.R. Severe obesity in children and adolescents: Identification, associated health risks, and treatment approaches: A scientific statement from the American Heart Association. Circulation 2013, 128, 1689–1712. [Google Scholar] [CrossRef] [PubMed]
- Reilly, J.J.; Methven, E.; McDowell, Z.C.; Hacking, B.; Alexander, D.; Stewart, L.; Kelnar, C.J. Health consequences of obesity. Arch. Dis. Childhood. 2003, 88, 748–752. [Google Scholar] [CrossRef] [PubMed]
- Kim, D.D.; Basu, A. Estimating the Medical Care Costs of Obesity in the United States: Systematic Review, Meta-Analysis, and Empirical Analysis. Value Health 2016, 19, 602–613. [Google Scholar] [CrossRef] [PubMed]
- Kothandan, S.K. School based interventions versus family based interventions in the treatment of childhood obesity—A systematic review. Arch Public Health 2014, 72, 3. [Google Scholar] [CrossRef]
- Luttikhuis, H.O.; Baur, L.; Jansen, H.; Shrewsbury, V.A.; O’Malley, C.; Stolk, R.P.; Summerbell, C.D. Interventions for treating obesity in children. Cochrane Database Syst. Rev. 2019, 3, CD001872. [Google Scholar] [CrossRef]
- Summerbell, C.D.; Ashton, V.; Campbell, K.J.; Edmunds, L.; Kelly, S.; Waters, E. Interventions for treating obesity in children. Cochrane Database Syst. Rev. 2003, 3, CD001872. [Google Scholar] [CrossRef]
- Waters, E.; De Silva-Sanigorski, A.; Burford, B.J.; Brown, T.; Campbell, K.J.; Gao, Y.; Armstrong, R.; Prosser, L.; Summerbell, C.D. Interventions for preventing obesity in children. Cochrane Database Syst. Rev. 2011, 12, CD001871. [Google Scholar] [CrossRef]
- Vine, M.; Hargreaves, M.B.; Briefel, R.R.; Orfield, C. Expanding the role of primary care in the prevention and treatment of childhood obesity: A review of clinic- and community-based recommendations and interventions. J. Obes. 2013, 2013, 172035. [Google Scholar] [CrossRef]
- Knowler, W.C.; Barrett-Connor, E.; Fowler, S.E.; Hamman, R.F.; Lachin, J.M.; Walker, E.A.; Nathan, D.M.; Diabetes Prevention Program Research Group. Reduction in the incidence of type 2 diabetes with lifestyle intervention or metformin. N. Engl. J. Med. 2002, 346, 393–403. [Google Scholar] [CrossRef]
- Ali, M.K.; Echouffo-Tcheugui, J.; Williamson, D.F. How effective were lifestyle interventions in real-world settings that were modeled on the Diabetes Prevention Program? Health Aff. 2012, 31, 67–75. [Google Scholar] [CrossRef]
- Wing, R.R.; Look AHEAD Research Group. Long-term effects of a lifestyle intervention on weight and cardiovascular risk factors in individuals with type 2 diabetes mellitus: Four-year results of the Look AHEAD trial. Arch. Intern. Med. 2010, 170, 1566–1575. [Google Scholar] [CrossRef]
- US Preventive Services Task Force. Screening for Obesity in Children and Adolescents: US Preventive Services Task Force Recommendation Statement. JAMA 2017, 317, 2417–2426. [Google Scholar] [CrossRef]
- US Preventive Services Task Force. Behavioral Weight Loss Interventions to Prevent Obesity-Related Morbidity and Mortality in Adults: US Preventive Services Task Force Recommendation Statement. JAMA 2018, 320, 1163–1171. [Google Scholar] [CrossRef]
- Nápoles, A.M.; Stewart, A.L. Transcreation: An implementation science framework for community-engaged behavioral interventions to reduce health disparities. BMC Health Serv. Res. 2018, 18, 710. [Google Scholar] [CrossRef]
- Dietz, W.H.; Belay, B.; Bradley, D.; Kahan, S.; Muth, N.D.; Sanchez, E.; Solomon, L. A Model Framework That Integrates Community and Clinical Systems for the Prevention and Management of Obesity and Other Chronic Diseases; National Academy of Medicine: Washington, DC, USA, 2017. [Google Scholar]
- Linden, A.; Adams, J.L.; Roberts, N. An assessment of the total population approach for evaluating disease management program effectiveness. Dis. Manag. 2003, 6, 93–102. [Google Scholar] [CrossRef]
- Bayoumi, N.S.; Helzner, E.; Afable, A.; Joseph, M.A.; Dhuper, S. A real-world evaluation of a tertiary care childhood obesity intervention to reduce metabolic risk in a hard-to-reach urban population. BMC Pediatr. 2019, 19, 378. [Google Scholar] [CrossRef]
- Linden, A.; Adams, J.L.; Roberts, N. Evaluating disease management program effectiveness: An introduction to survival analysis. Dis. Manag. 2004, 7, 180–190. [Google Scholar] [CrossRef]
- George, B.; Seals, S.; Aban, I. Survival analysis and regression models. J. Nucl. Cardiol. 2014, 21, 686–694. [Google Scholar] [CrossRef]
- Kelley, C.P.; Sbrocco, G.; Sbrocco, T. Behavioral Modification for the Management of Obesity. Prim. Care 2016, 43, 159–175. [Google Scholar] [CrossRef]
- Centers for Disease Control and Prevention. Healthy Weight, Nutrition, and Physical Activity. Available online: https://www.cdc.gov/healthyweight/assessing/bmi/childrens_bmi/about_childrens_bmi.html (accessed on 10 March 2023).
- Centers for Disease Control and Prevention. Modified z-Scores in the CDC Growth Charts. Available online: https://www.cdc.gov/nccdphp/dnpa/growthcharts/resources/biv-cutoffs.pdf (accessed on 10 February 2021).
- Freedman, D.S.; Butte, N.F.; Taveras, E.M.; Lundeen, E.A.; Blanck, H.M.; Goodman, A.B.; Ogden, C.L. BMI z-Scores are a poor indicator of adiposity among 2- to 19-year-olds with very high BMIs, NHANES 1999–2000 to 2013–2014. Obesity 2017, 25, 739–746. [Google Scholar] [CrossRef] [PubMed]
- Zabarsky, G.; Beek, C.; Hagman, E.; Pierpont, B.; Caprio, S.; Weiss, R. Impact of Severe Obesity on Cardiovascular Risk Factors in Youth. J. Pediatr. 2018, 192, 105–114. [Google Scholar] [CrossRef]
- Baker, J.L.; Olsen, L.W.; Sørensen, T.I. Childhood body-mass index and the risk of coronary heart disease in adulthood. N. Engl. J. Med. 2007, 357, 2329–2337. [Google Scholar] [CrossRef] [PubMed]
- Dietz, W.H. Time to Adopt New Measures of Severe Obesity in Children and Adolescents. Pediatrics 2017, 140, e20172148. [Google Scholar] [CrossRef] [PubMed]
- Freedman, D.S.; Berenson, G.S. Tracking of BMI z Scores for Severe Obesity. Pediatrics 2017, 140, e20171072. [Google Scholar] [CrossRef]
- Danielsson, P.; Kowalski, J.; Ekblom, Ö.; Marcus, C. Response of severely obese children and adolescents to behavioral treatment. Arch. Pediatr. Adolesc. Med. 2012, 166, 1103–1108. [Google Scholar] [CrossRef]
- Knop, C.; Singer, V.; Uysal, Y.; Schaefer, A.; Wolters, B.; Reinehr, T. Extremely obese children respond better than extremely obese adolescents to lifestyle interventions. Pediatr. Obes. 2015, 10, 7–14. [Google Scholar] [CrossRef]
- Dhuper, S.; Bayoumi, N.; Dalvi, J.; Panzer, B. The Correlation Between Parental Perceptions and Readiness to Change with Participation in a Pediatric Obesity Program Serving a Predominantly Black Urban Community: A Retrospective Cohort Study. Matern. Child Health J. 2020, 25, 606–612. [Google Scholar] [CrossRef]
- O’Connor, E.A.; Evans, C.V.; Burda, B.U.; Walsh, E.S.; Eder, M.; Lozano, P. Screening for Obesity and Intervention for Weight Management in Children and Adolescents: Evidence Report and Systematic Review for the US Preventive Services Task Force. JAMA 2017, 317, 2427–2444. [Google Scholar] [CrossRef]
- Huang, T.T.; Glass, T.A. Transforming research strategies for understanding and preventing obesity. JAMA 2008, 300, 1811–1813. [Google Scholar] [CrossRef]
- Tate, D.F.; Lytle, L.A.; Sherwood, N.E.; Haire-Joshu, D.; Matheson, D.; Moore, S.M.; Loria, C.M.; Pratt, C.; Ward, D.S.; Belle, S.H.; et al. Deconstructing interventions: Approaches to studying behavior change techniques across obesity interventions. Transl. Behav. Med. 2016, 6, 236–243. [Google Scholar] [CrossRef]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Low Contact Hours | High Contact Hours | ||||
|---|---|---|---|---|---|
| Variable | N (total) | Mean ± SD or N (%) | N (total) | Mean ± SD or N (%) | p-Value |
| Age in years, mean ± SD | 256 | 11.0 ± 3.44 | 150 | 10.0 ± 2.66 | 0.00 |
| Sex | 256 | 150 | |||
| Male | 111 (43.4%) | 67 (44.7%) | 0.84 | ||
| Female | 145 (56.6%) | 83 (55.3%) | |||
| Race | 78 | 66 | |||
| Black | 60 (76.9%) | 58 (87.9%) | |||
| Hispanic | 15 (19.2%) | 8 (12.1%) | |||
| White | 0 (0.00%) | 0 (0.00%) | 0.12 | ||
| Asian | 0 (0.00%) | 0 (0.00%) | |||
| Other/Unknown | 3 (3.85%) | 0 (0.00%) | |||
| BMIz, mean ± SD | 256 | 2.43 ± 0.44 | 150 | 2.41 ± 0.42 | 0.72 |
| BMI%95, mean ± SD | 256 | 148.3 ± 28.4 | 150 | 146.8 ± 26.4 | 0.60 |
| Obesity Prevalence | 256 | 150 | |||
| Healthy weight | 0 (0.00%) | 1 (0.66%) | |||
| Overweight | 0 (0.00%) | 1 (0.66%) | 0.19 | ||
| Obese | 38 (14.8%) | 16 (10.7%) | |||
| Severely obese | 218 (85.2%) | 132 (88.0%) | |||
| Abnormal Waist circumference | 210 | 195 (92.9%) | 133 | 124 (93.2%) | 0.89 |
| Hypertension | |||||
| Systolic Hypertension | 237 | 70 (29.5%) | 145 | 48 (33.1%) | 0.49 |
| Diastolic Hypertension | 237 | 40 (16.9%) | 144 | 19 (13.2%) | 0.38 |
| Lipid Levels | |||||
| Abnormal Total cholesterol | 195 | 75 (38.5%) | 129 | 50 (38.8%) | 0.96 |
| Abnormal High-density lipoprotein | 189 | 65 (34.4%) | 122 | 34 (27.9%) | 0.23 |
| Abnormal Low-density lipoprotein | 185 | 56 (30.3%) | 121 | 33 (27.3%) | 0.57 |
| Abnormal Triglycerides | 188 | 62 (33.0%) | 120 | 30 (25.0%) | 0.14 |
| Elevated fasting glucose | 172 | 18 (10.5%) | 114 | 8 (7.02%) | 0.32 |
| Presence of 3 or more components of the Metabolic syndrome | 135 | 36 (26.0%) | 96 | 24 (25.0%) | 0.78 |
| Age | Frequency | Percent |
|---|---|---|
| 2 | 1 | 0.25 |
| 3 | 2 | 0.49 |
| 4 | 9 | 2.22 |
| 5 | 12 | 2.96 |
| 6 | 21 | 5.17 |
| 7 | 42 | 10.3 |
| 8 | 39 | 9.61 |
| 9 | 55 | 13.6 |
| 10 | 47 | 11.6 |
| 11 | 50 | 12.3 |
| 12 | 37 | 9.11 |
| 13 | 27 | 6.65 |
| 14 | 19 | 4.68 |
| 15 | 20 | 4.93 |
| 16 | 15 | 3.69 |
| 17 | 4 | 0.99 |
| 18 | 2 | 0.49 |
| 19 | 4 | 0.99 |
| Risk Factor | Contact Hour Group | N | Mean | Std. Dev. | Min | Max | p-Value |
|---|---|---|---|---|---|---|---|
| BMIz | Low | 61 | 26.2 | 15.3 | 12.7 | 103.6 | 0.00 |
| High | 65 | 34.8 | 17.1 | 12.2 | 79.3 | ||
| (Total) | 126 | 30.6 | 16.7 | 12.2 | 103.6 | ||
| BMI%95 | Low | 48 | 28.6 | 17.3 | 12.7 | 103.6 | 0.43 |
| High | 54 | 31.2 | 15.7 | 12.2 | 85.5 | ||
| (Total) | 102 | 30.0 | 16.5 | 12.2 | 103.6 | ||
| BMI | Low | 21 | 23.3 | 9.25 | 12.2 | 43.8 | 0.47 |
| High | 21 | 21.4 | 7.43 | 12.8 | 44.7 | ||
| (Total) | 42 | 22.4 | 8.34 | 12.2 | 44.7 |
| Risk Factor | Contact Hour Group | N | Mean | Std. Dev. | Min | Max | p-Value |
|---|---|---|---|---|---|---|---|
| BMIz | Low | 61 | 11.2 | 15.3 | 0.47 | 56.8 | 0.24 |
| High | 65 | 8.45 | 10.1 | 0.67 | 39.8 | ||
| (Total) | 126 | 9.78 | 12.9 | 0.47 | 56.8 | ||
| BMI%95 | Low | 48 | 11.2 | 15.7 | 0.47 | 56.8 | 0.39 |
| High | 54 | 8.88 | 11.7 | 0.07 | 57.9 | ||
| (Total) | 102 | 10.0 | 13.7 | 0.47 | 57.9 | ||
| ΔBMI | Low | 21 | 6.41 | 7.64 | 0.47 | 35.6 | 0.88 |
| High | 21 | 6.74 | 7.17 | 0.93 | 26.0 | ||
| (Total) | 42 | 6.58 | 7.32 | 0.47 | 35.6 |
| BMI%95 | BMIz | BMI | ||||
|---|---|---|---|---|---|---|
| Variable | HR (95% CI) | p-value | HR (95% CI) | p-value | HR (95% CI) | p-value |
| Contact Hour Group (Referent—Low) | 2.11 (1.41–3.17) | <0.001 | 1.81 (1.27–2.58) | 0.001 | 1.92 (1.03–3.60) | 0.042 |
| Age | 1.07 (1.001–1.13) | 0.047 | 0.929 (0.875–0.987) | 0.017 | 1.10 (0.994–1.21) | 0.07 |
| Sex (Referent—Male) | 0.929 (0.625–1.38) | 0.714 | 1.31 (0.908–1.88) | 0.149 | 1.26 (0.676–2.35) | 0.47 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
James, A.; Afable, A.; Bayoumi, N.; Dhuper, S. Evaluation of a Childhood Obesity Program Serving a High-Need Population in Brooklyn, New York Using Survival Analysis. Int. J. Environ. Res. Public Health 2023, 20, 5723. https://doi.org/10.3390/ijerph20095723
James A, Afable A, Bayoumi N, Dhuper S. Evaluation of a Childhood Obesity Program Serving a High-Need Population in Brooklyn, New York Using Survival Analysis. International Journal of Environmental Research and Public Health. 2023; 20(9):5723. https://doi.org/10.3390/ijerph20095723
Chicago/Turabian StyleJames, Alecia, Aimee Afable, Nagla Bayoumi, and Sarita Dhuper. 2023. "Evaluation of a Childhood Obesity Program Serving a High-Need Population in Brooklyn, New York Using Survival Analysis" International Journal of Environmental Research and Public Health 20, no. 9: 5723. https://doi.org/10.3390/ijerph20095723