
Tides of Change—Barriers and Facilitators to Beach Accessibility for Older People and People with Disability: An Australian Community Survey


Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Recruitment and Participants
2.3. Survey Instrument
2.4. Sample Size Calculation
2.5. Analysis
3. Results
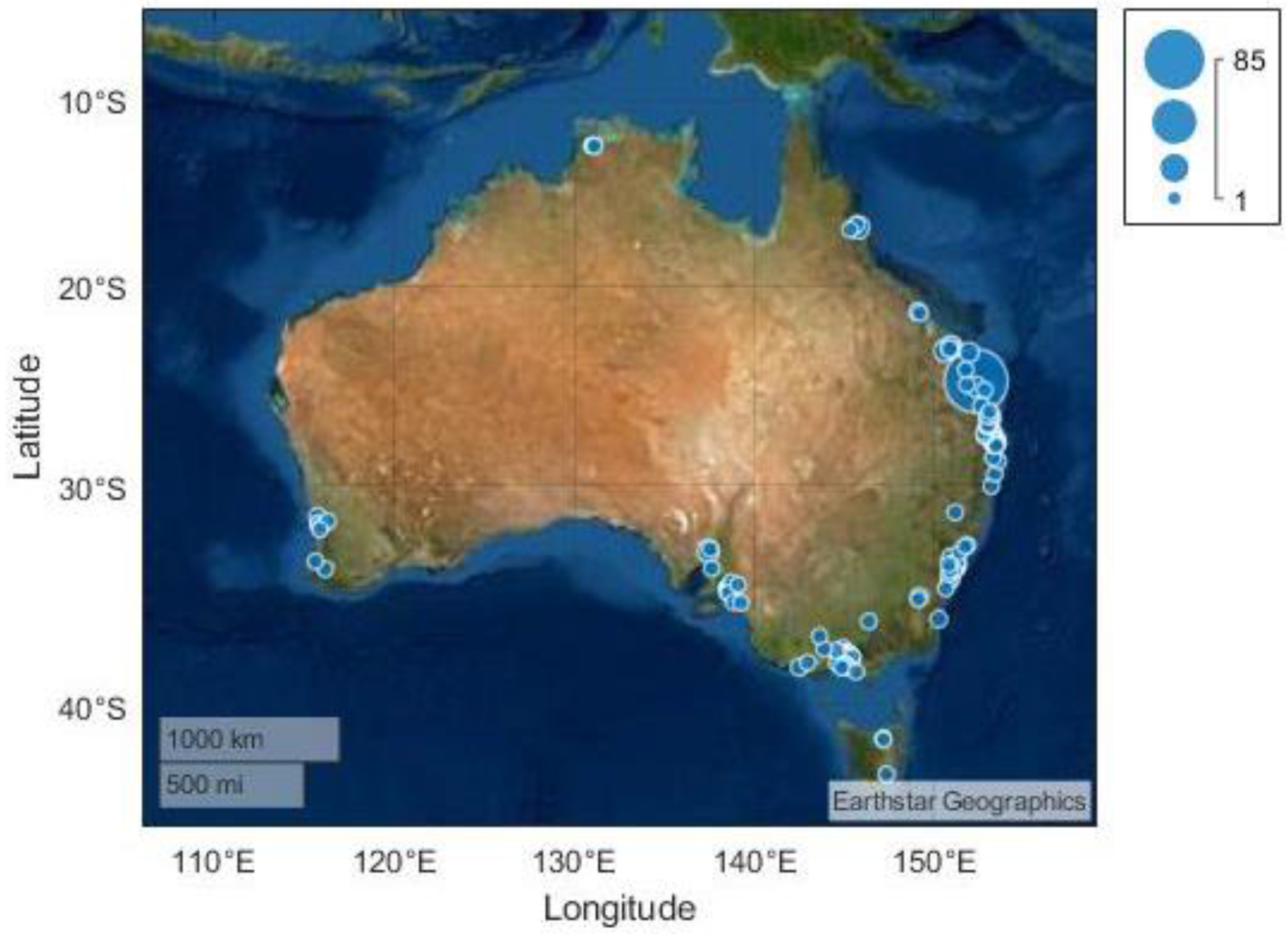
3.1. Respondent Characteristics
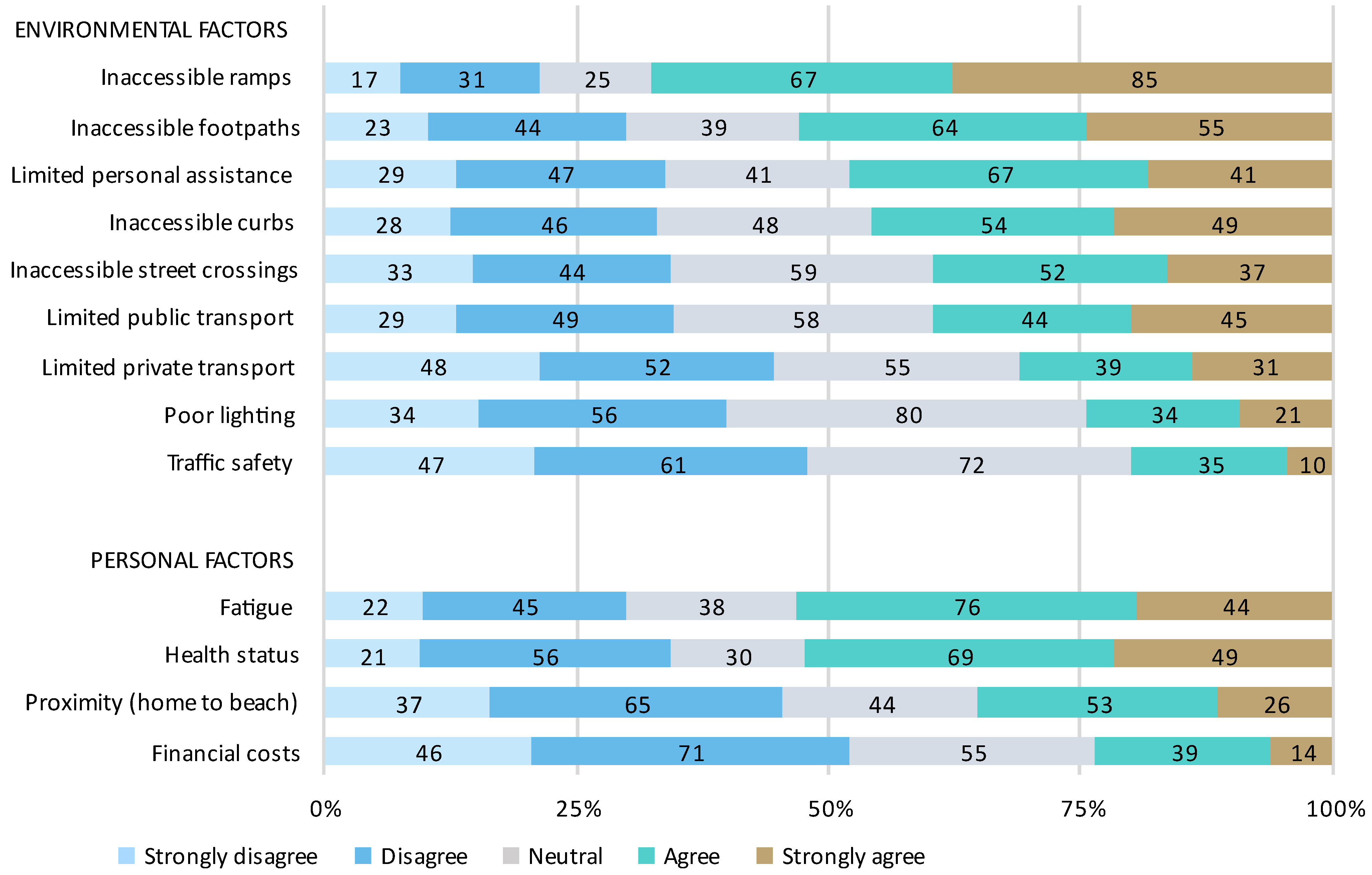
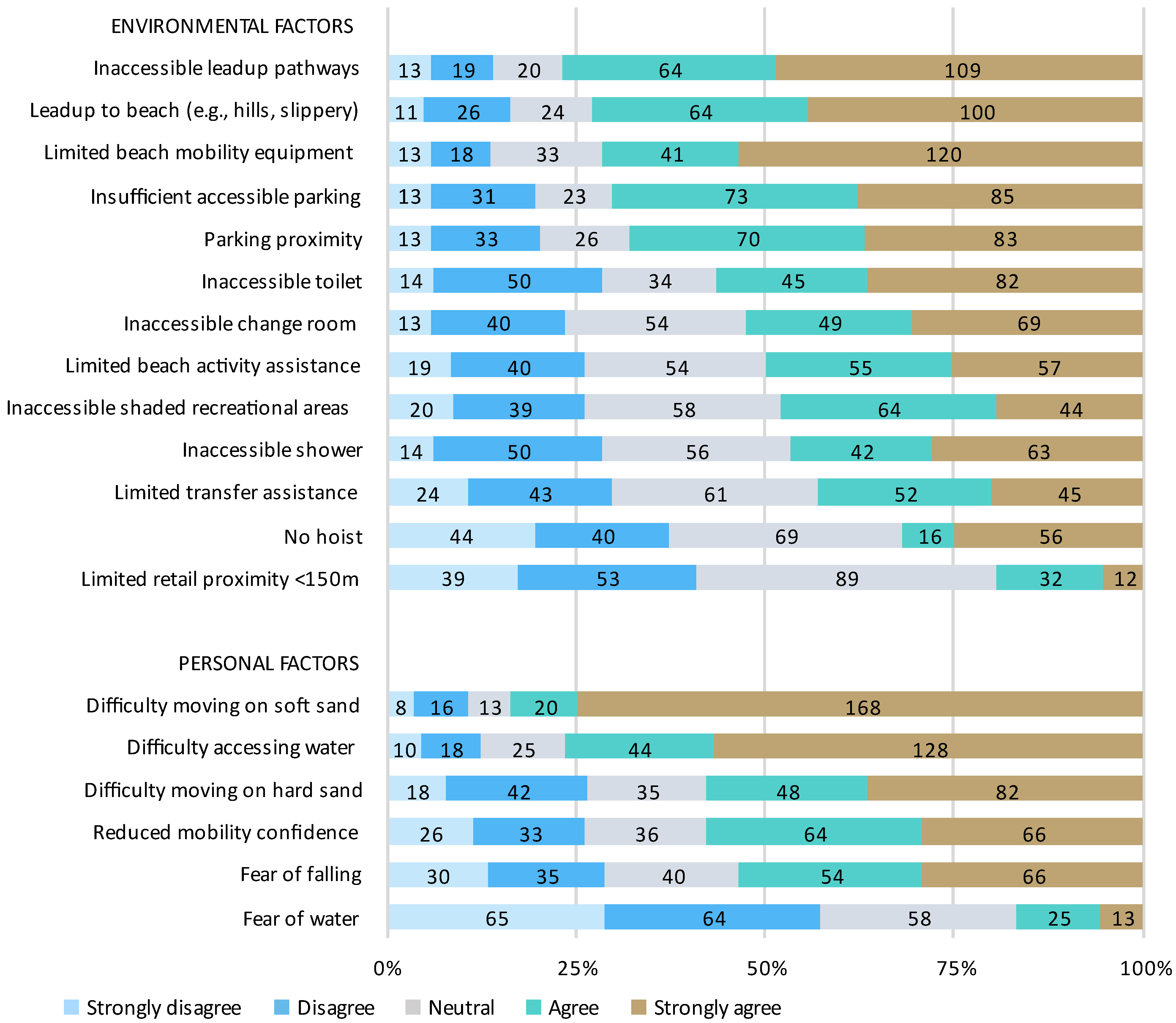
3.2. Barriers to Beach Access
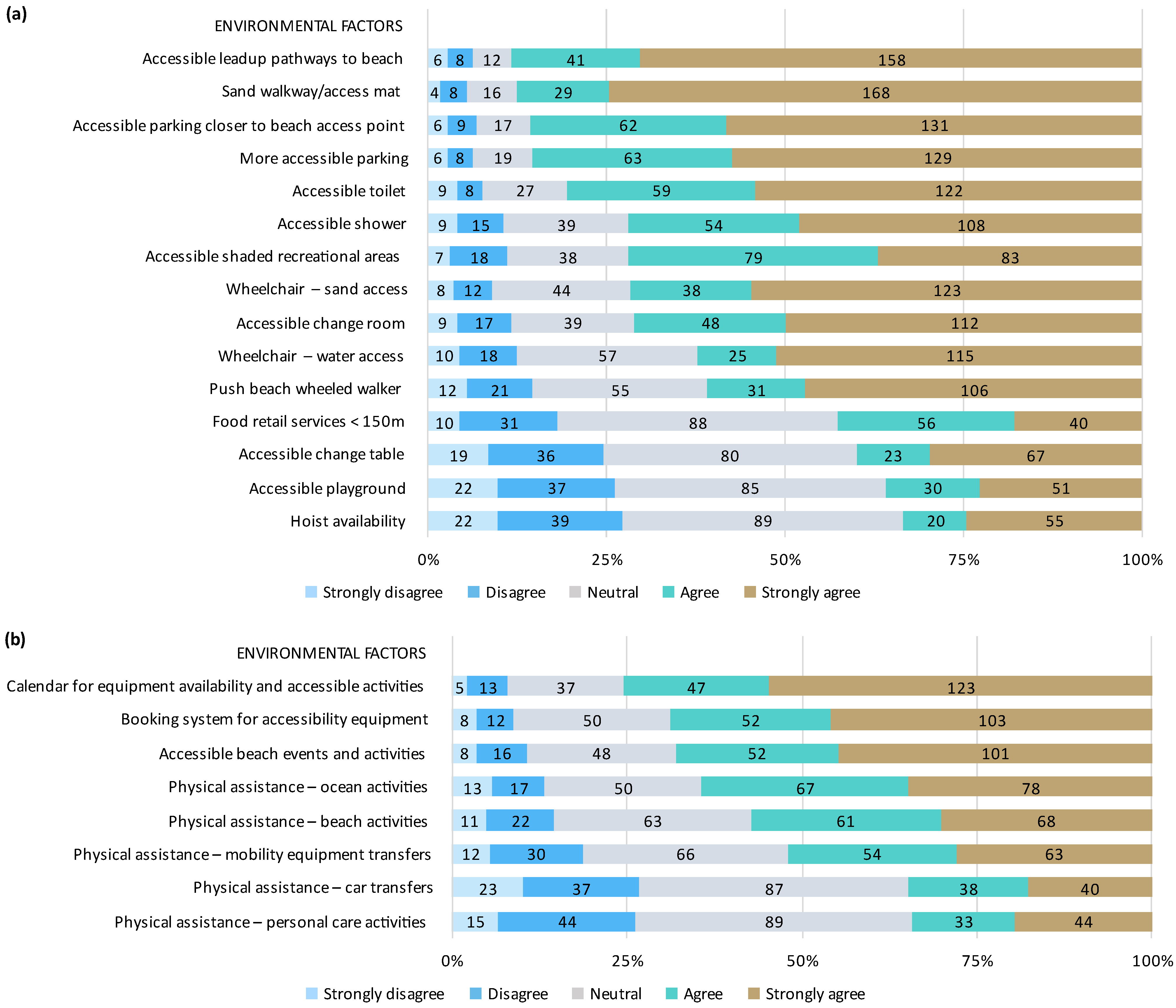
3.3. Facilitators to Beach Access
4. Discussion
4.1. Barriers and Facilitators to Travelling to the Beach
4.2. Barriers and Facilitators to Accessing the Beach and Surrounds
4.3. Beach Access for Older People and People with Disability (Mobility and Non-Mobility)
4.4. Limitations and Future Directions
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Australian Insitute of Health and Welfare. Disability and Ageing Australian Population Patterns and Implications; The Australian Institute of Health and Welfare: Canberra, Australia, 2020. [Google Scholar]
- World Health Organisation. WHO Global Disability Action Plan 2014–2021. Better Health for all People with Disability; World Health Organisation: Geneva, Switzerland, 2015. [Google Scholar]
- Australian Institute of Health and Welfare. People with Disability in Australia. 2020. Available online: https://www.aihw.gov.au/reports/disability/people-with-disability-in-australia/contents/health/health-risk-factors-and-behaviours (accessed on 25 November 2022).
- World Health Organisation. World Disability Report; World Health Organisation: Geneva, Switzerland, 2011; Available online: https://www.who.int/teams/noncommunicable-diseases/sensory-functions-disability-and-rehabilitation/world-report-on-disability (accessed on 25 November 2020).
- Australian Institute of Health and Welfare. Older Australia at a Glance; Australian Institute of Health and Welfare: Canberra, Australia, 2018. Available online: https://www.aihw.gov.au/reports/older-people/older-australia-at-a-glance/contents/demographics-of-older-australians/australia-s-changing-age-and-gender-profile (accessed on 25 November 2022).
- United Nations. Convention on the Rights of Persons with Disabilities (CRPD). 2007. Available online: https://www.un.org/development/desa/disabilities/convention-on-the-rights-of-persons-with-disabilities.html (accessed on 6 March 2023).
- Nieuwenhuijsen, M.J.; Kruize, H.; Gidlow, C.; Andrusaityte, S.; Antó, J.M.; Basagaña, X.; Cirach, M.; Dadvand, P.; Danileviciute, A.; Donaire-Gonzalez, D.; et al. Positive health effects of the natural outdoor environment in typical populations in different regions in Europe (PHENOTYPE): A study programme protocol. BMJ Open 2014, 4, e004951. [Google Scholar] [CrossRef] [PubMed]
- Wheeler, B.W.; White, M.; Stahl-Timmins, W.; Depledge, M.H. Does living by the coast improve health and wellbeing? Health Place 2012, 18, 1198–1201. [Google Scholar] [CrossRef] [PubMed]
- White, M.; Bell, S.; Elliot, L.R.; Jenkin, R. Green exercise: Linking nature, health and well-being. In The Health Benefits of Blue Exercise in the UK; Barton, J., Bragg, R., Wood, C., Eds.; Routledge: Abingdon, UK, 2016. [Google Scholar]
- Völker, S.; Kistemann, T. Reprint of: “I’m always entirely happy when I’m here!” Urban blue enhancing human health and well-being in Cologne and Düsseldorf, Germany. Soc. Sci. Med. 2013, 91, 141–152. [Google Scholar] [CrossRef] [PubMed]
- White, M.P.; Wheeler, B.W.; Herbert, S.; Alcock, I.; Depledge, M.H. Coastal proximity and physical activity: Is the coast an under-appreciated public health resource? Prev. Med. 2014, 69, 135–140. [Google Scholar] [CrossRef] [PubMed]
- Ashbullby, K.J.; Pahl, S.; Webley, P.; White, M.P. The beach as a setting for families’ health promotion: A qualitative study with parents and children living in coastal regions in Southwest England. Health Place 2013, 23, 138–147. [Google Scholar] [CrossRef]
- White, M.P.; Pahl, S.; Ashbullby, K.; Herbert, S.; Depledge, M.H. Feelings of restoration from recent nature visits. J. Environ. Psychol. 2013, 35, 40–51. [Google Scholar] [CrossRef]
- Gascon, M.; Zijlema, W.; Vert, C.; White, M.P.; Nieuwenhuijsen, M.J. Outdoor blue spaces, human health and well-being: A systematic review of quantitative studies. Int. J. Hyg. Environ. Health 2017, 220, 1207–1221. [Google Scholar] [CrossRef]
- Britton, E.; Kindermann, G.; Domegan, C.; Carlin, C. Blue care: A systematic review of blue space interventions for health and wellbeing. Health Promot. Int. 2018, 35, 50–69. [Google Scholar] [CrossRef]
- Job, S.; Heales, L.; Obst, S. Oceans of opportunity for universal beach accessibility: An integrated model for health and wellbeing in people with disability. Aust. New Zealand J. Public Health 2022, 46, 252–254. [Google Scholar] [CrossRef]
- World Health Organisation. Towards a Common Language for Functioning Disability and Health: ICF; World Health Organisation: Geneva, Switzerland, 2002. [Google Scholar]
- Ploeg, H.; Beek, A.; Woude, L.; Mechelen, W. Physical activity for people with a disability: A conceptual model. Sports Med. 2004, 34, 639–649. [Google Scholar] [CrossRef]
- White, M.P.; Elliott, L.R.; Gascon, M.; Roberts, B.; Fleming, L.E. Blue space, health and well-being: A narrative overview and synthesis of potential benefits. Environ. Res. 2020, 191, 110169. [Google Scholar] [CrossRef] [PubMed]
- Monforte, J.; Úbeda-Colomer, J.; Pans, M.; Pérez-Samaniego, V.; Devís-Devís, J. Environmental Barriers and Facilitators to Physical Activity among University Students with Physical Disability—A Qualitative Study in Spain. Int. J. Environ. Res. Public Health 2021, 18, 464. [Google Scholar] [CrossRef] [PubMed]
- Maguire, G.S.; Miller, K.K.; Weston, M.A.; Young, K. Being beside the seaside: Beach use and preferences among coastal residents of south-eastern Australia. Ocean Coast. Manag. 2011, 54, 781–788. [Google Scholar] [CrossRef]
- Schlacher, T.A.; Schoeman, D.S.; Dugan, J.; Lastra, M.; Jones, A.; Scapini, F.; McLachlan, A. Sandy beach ecosystems: Key features, sampling issues, management challenges and climate change impacts. Mar. Ecol. 2008, 29, 70–90. [Google Scholar] [CrossRef]
- Australian Department of Climate Change(DCC). Climate Change Risks to Australia’s Coast: A First Pass National Assessment; ACT, Department of Climate Change: Canberra, Australia, 2009. [Google Scholar]
- Aliyas, Z. Physical, mental, and physiological health benefits of green and blue outdoor spaces among elderly people. Int. J. Environ. Health Res. 2019, 31, 703–714. [Google Scholar] [CrossRef]
- Finlay, J.; Franke, T.; McKay, H.; Sims-Gould, J. Therapeutic landscapes and wellbeing in later life: Impacts of blue and green spaces for older adults. Health Place 2015, 34, 97–106. [Google Scholar] [CrossRef]
- Chu, K.S.; Eng, J.J.; Dawson, A.S.; Harris, J.E.; Ozkaplan, A.; Gylfadóttir, S. Water-based exercise for cardiovascular fitness in people with chronic stroke: A randomized controlled trial. Arch. Phys. Med. Rehabil. 2004, 85, 870–874. [Google Scholar] [CrossRef]
- Taylor, L.P.S.; McGruder, J.E. The Meaning of Sea Kayaking for Persons With Spinal Cord Injuries. Am. J. Occup. Ther. 1996, 50, 39–46. [Google Scholar] [CrossRef]
- Freudenberg, P.; Arlinghaus, R. Benefits and constraints of outdoor recreation for people with physical disabilities: Inferences from recreational fishing. Leis. Sci. 2009, 32, 55–71. [Google Scholar] [CrossRef]
- Lee, D.; Kim, J.; Thapa, B.; Stein, T. Measuring Beach Accessibility for People with Ambulatory Difficulty. J. Park Recreat. Adm. 2020, 38, 106–126. [Google Scholar] [CrossRef]
- Darcy, S.; Maxwell, H.; Edwards, M.; Almond, B. Disability inclusion in beach precincts: Beach for all abilities—A community development approach through a social relational model of disability lens. Sport Manag. Rev. 2022, 26, 1–23. [Google Scholar] [CrossRef]
- Disability, Ageing and Carers, Australia: Summary of Findings. 2019. Available online: https://www.abs.gov.au/statistics/health/disability/disability-ageing-and-carers-australia-summary-findings/latest-release (accessed on 6 March 2023).
- Keysor, J.J.; Jette, A.M.; LaValley, M.P.; Lewis, C.E.; Torner, J.C.; Nevitt, M.C.; Felson, D.T.; the Multicenter Osteoarthritis (MOST) Group. Community Environmental Factors Are Associated With Disability in Older Adults With Functional Limitations: The MOST Study. J. Gerontol. Ser. A 2009, 65, 393–399. [Google Scholar] [CrossRef] [PubMed]
- Walsh, K.; Gannon, B. Perceived neighbourhood context, disability onset and old age. J. Socio-Econ. 2011, 40, 631–636. [Google Scholar] [CrossRef]
- Freedman, V.A.; Grafova, I.; Schoeni, R.F.; Rogowski, J. Neighborhoods and disability in later life. Soc. Sci. Med. 2008, 66, 2253–2267. [Google Scholar] [CrossRef] [PubMed]
- Mayordomo-Martínez, D.; Sánchez-Aarnoutse, J.-C.; Carrillo-de-Gea, J.M.; García-Berná, J.A.; Fernández-Alemán, J.L.; García-Mateos, G. Design and development of a mobile app for accessible beach tourism information for people with disabilities. Int. J. Environ. Res. Public Health 2019, 16, 2131. [Google Scholar] [CrossRef] [PubMed]
- Noblet, T.; Marriot, J.; Jones, T.; Dean, C.; Rushton, A. Views and perceptions of Australian physiotherapists and physiotherapy students about the potential implementation of physiotherapist prescribing in Australia: A survey protocol. BioMed Cent. Health Serv. Res. 2018, 18, 472. [Google Scholar] [CrossRef]
- Noblet, T.D.; Marriott, J.F.; Jones, T.; Dean, C.; Rushton, A.B. Perceptions about the implementation of physiotherapist prescribing in Australia: A national survey of Australian physiotherapists. BMJ Open 2019, 9, e024991. [Google Scholar] [CrossRef]
- Bennell, K.L.; Lawford, B.J.; Metcalf, B.; Mackenzie, D.; Russell, T.; Berg, M.V.D.; Finnin, K.; Crowther, S.; Aiken, J.; Fleming, J.; et al. Physiotherapists and patients report positive experiences overall with telehealth during the COVID-19 pandemic: A mixed-methods study. J. Physiother. 2021, 67, 201–209. [Google Scholar] [CrossRef]
- Freene, N.; Cools, S.; Bissett, B. Are we missing opportunities? Physiotherapy and physical activity promotion: A cross-sectional survey. BMC Sports Sci. Med. Rehabil. 2017, 9, 19. [Google Scholar] [CrossRef]
- Oliveira, J.S.; Sherrington, C.; Paul, S.S.; Ramsay, E.; Chamberlain, K.; Kirkham, C.; O’Rourke, S.D.; Hassett, L.; Tiedemann, A. A combined physical activity and fall prevention intervention improved mobility-related goal attainment but not physical activity in older adults: A randomised trial. J. Physiother. 2018, 65, 16–22. [Google Scholar] [CrossRef]
- Bennett, C.; Khangura, S.; Brehaut, J.C.; Graham, I.D.; Moher, D.; Potter, B.K.; Grimshaw, J. Reporting Guidelines for Survey Research: An Analysis of Published Guidance and Reporting Practices. PLOS Med. 2011, 8, e1001069. [Google Scholar] [CrossRef] [PubMed]
- Hicks, C.M. Research Methods for Clinical Therapists: Applied Project Design and Analysis; Elsevier Health Sciences: Amsterdam, The Netherlands, 2009. [Google Scholar]
- Abu Hassan, Z.; Schattner, P.; Mazza, D. Doing A Pilot Study: Why Is It Essential? Malays. Fam. Physician 2006, 1, 70–73. [Google Scholar]
- Storozuk, A.; Ashley, M.; Delage, V.; Maloney, E.A. Got Bots? Practical Recommendations to Protect Online Survey Data from Bot Attacks. Quant. Methods Psychol. 2020, 16, 472–481. [Google Scholar] [CrossRef]
- Australian Bureau of Statistics. Sample Size Calculator. Available online: https://www.abs.gov.au/websitedbs/d3310114.nsf/home/sample+size+calculator (accessed on 3 March 2021).
- DATAtab. Mann-Whitney U-Test. Available online: https://datatab.net (accessed on 30 January 2023).
- Accessible Beaches Australia. Accessible Beaches. Available online: https://accessiblebeaches.com/ (accessed on 25 November 2022).
- Rimmer, J.H.; Riley, B.; Wang, E.; Rauworth, A.; Jurkowski, J. Physical activity participation among persons with disabilities: Barriers and facilitators. Am. J. Prev. Med. 2004, 26, 419–425. [Google Scholar] [CrossRef]
- Twohig-Bennett, C.; Jones, A. The health benefits of the great outdoors: A systematic review and meta-analysis of greenspace exposure and health outcomes. Environ. Res. 2018, 166, 628–637. [Google Scholar] [CrossRef]
- Hästbacka, E.; Nygård, M.; Nyqvist, F. Barriers and facilitators to societal participation of people with disabilities: A scoping review of studies concerning European countries. Alter 2016, 10, 201–220. [Google Scholar] [CrossRef]
- Deslippe, A.L.; Soanes, A.; Bouchaud, C.C.; Beckenstein, H.; Slim, M.; Plourde, H.; Cohen, T.R. Barriers and facilitators to diet, physical activity and lifestyle behavior intervention adherence: A qualitative systematic review of the literature. Int. J. Behav. Nutr. Phys. Act. 2023, 20, 14. [Google Scholar] [CrossRef]
- Park, K.; Esfahani, H.N.; Novack, V.L.; Sheen, J.; Hadayeghi, H.; Song, Z.; Christensen, K. Impacts of disability on daily travel behaviour: A systematic review. Transp. Rev. 2022, 43, 178–203. [Google Scholar] [CrossRef]
- Ewing, R.; Cervero, R. Travel and the built environment: A meta-analysis. J. Am. Plan. Assoc. 2010, 76, 265–294. [Google Scholar] [CrossRef]
- Santana-Santana, S.B.; Peña-Alonso, C.; Espino, E.P.-C. Assessing universal accessibility in Spanish beaches. Ocean Coast. Manag. 2021, 201, 105486. [Google Scholar] [CrossRef]
- Australia’s Coasts and Estuaries. 2022. Available online: https://www.ga.gov.au/scientific-topics/marine/coasts-estuaries#heading-1 (accessed on 25 November 2022).
- Web Content Accessibility Guidelines 2.0, Web Accessibility Initiative. 2008. Available online: http://www.w3.org/TR/WCAG/ (accessed on 25 November 2022).
- Shanahan, D.F.; Bush, R.; Gaston, K.J.; Lin, B.B.; Dean, J.; Barber, E.; Fuller, R.A. Health Benefits from Nature Experiences Depend on Dose. Sci. Rep. 2016, 6, 28551. [Google Scholar] [CrossRef] [PubMed]
- Cox, D.T.C.; Shanahan, D.F.; Hudson, H.L.; Fuller, R.A.; Anderson, K.; Hancock, S.; Gaston, K.J. Doses of Nearby Nature Simultaneously Associated with Multiple Health Benefits. Int. J. Environ. Res. Public Health 2017, 14, 172. [Google Scholar] [CrossRef] [PubMed]
- Mitchell, R.J.; Richardson, E.A.; Shortt, N.K.; Pearce, J.R. Neighborhood Environments and Socioeconomic Inequalities in Mental Well-Being. Am. J. Prev. Med. 2015, 49, 80–84. [Google Scholar] [CrossRef] [PubMed]
- Allen, J.; Balfour, R. Natural Solutions for Tackling Health Inequalities; UCL Institute of Health Equity: London, UK, 2014; Available online: https://www.instituteofhealthequity.org/resources-reports/natural-solutions-to-tackling-health-inequalities (accessed on 3 March 2021).
- Burt, J.; Stewart, D.; Preston, S.; Costley, T. Monitor of Engagement with the Natural Environment Survey (2009–2012): Difference in access to the natural environment between social groups within the adult English population. Nat. Engl. 2013. Available online: https://publications.naturalengland.org.uk/publication/4646400 (accessed on 3 March 2021).
- Cumming, R.G.; Salkeld, G.; Thomas, M.; Szonyi, G. Prospective study of the impact of fear of falling on activities of daily living, SF-36 scores, and nursing home admission. J. Gerontol. Ser. A Biol. Sci. Med. Sci. 2000, 55, M299–M305. [Google Scholar] [CrossRef]
- Maxwell, H.; Edwards, M.; Stronach, M.; Brown, V. A ‘fair go’on Australian beaches. Ann. Leis. Res. 2014, 4, 476–494. [Google Scholar] [CrossRef]
- Small, J. Women’s “beach body” in Australian women’s magazines. Ann. Tour. Res. 2017, 63, 23–33. [Google Scholar] [CrossRef]
- Frawley, P.; Bigby, C. Inclusion in political and public life: The experiences of people with intellectual disability on government disability advisory bodies in Australia. J. Intellect. Dev. Disabil. 2011, 36, 27–38. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristic | Category | Data |
|---|---|---|
| Age (years) mean (SD) | 52.0 (19.7) (range 2–90) | |
| Gender | Female | 239 (68.3%) |
| Male | 103 (29.4%) | |
| Non-binary | 4 (1.1%) | |
| Prefer not to say | 4 (1.1%) | |
| Disability status * | Disability | 185 (65.4%) |
| Disability with mobility limitation | 103 (29.4%) | |
| Older person (≥65 years) | 112 (32.0%) | |
| Older person (≥65 years) with disability | 66 (18.9%) | |
| Carer or service provider of person with disability | 94 (26.9%) | |
| Assistance required * | Self-care physical assistance | 166 (49.1%) |
| Mobility physical assistance | 182 (53.8%) | |
| Home mobility aid | 226 (66.9%) | |
| Community mobility aid | 260 (76.9%) | |
| Mobility aid * | Walking stick | 78 (23.1%) |
| Crutches | 24 (7.1%) | |
| Walking frame—pickup | 3 (0.9%) | |
| Walking frame—wheeled | 104 (30.8%) | |
| Wheelchair—manual | 133 (39.3%) | |
| Wheelchair—power | 80 (23.7%) | |
| Scooter | 31 (9.2%) | |
| Other | 21 (6.2%) | |
| Self-reported health | Excellent | 30 (8.6%) |
| Very Good | 85 (24.3%) | |
| Good | 112 (32.0%) | |
| Fair | 88 (25.1%) | |
| Poor | 35 (10.0%) |
| Barrier | Kruskal–Wallis H | Mann–Whitney U | |||||
|---|---|---|---|---|---|---|---|
| Group 1 vs. Group 2 | Group 1 vs. Group 3 | Group 1 vs. Group 4 | Group 2 vs. Group 3 | Group 2 vs. Group 4 | Group 3 vs. Group 4 | ||
| Limited accessible parking | 11.727 p = 0.008 | 1071.500; p = 0.506 MR Group 1 = 69.03 MR Group 2 = 75.82 r = −0.08 | 432.000; p = 0.893 MR Group 1 34.50 MR Group 3 33.82 r = −0.02 | 157.500; p = 0.040 MR Group 1 27.75 MR Group 4 19.83 r = −0.31 | 2889.500; p = 0.277 MR Group 2 92.94 MR Group 3 83.97 r = −0.08 | 1080.000; p =< 0.001 MR Group 2 84.76 MR Group 4 54.00 r = −0.27 | 459.500; p = 0.023 MR Group 3 42.62 MR Group 4 31.02 r = −0.26 |
| Parking proximity to beach access point | 22.590 p =< 0.001 | 843.500; p = 0.038 MR Group 1=56.36 MR Group 2=77.56 r = −0.17 | 416.000; p = 0.715 MR Group 1 32.61 MR Group 3 34.51 r = −0.04 | 167.500; p = 0.074 MR Group 1 27.19 MR Group 4 20.20 r = −0.27 | 2453.500; p = 0.023 MR Group 2 95.58 MR Group 3 76.91 r = −0.17 | 868.500; p =< 0.001 MR Group 2 86.37 MR Group 4 46.17 r = −0.35 | 457.000; p = 0.022 MR Group 3 42.67 MR Group 4 30.93 r = −0.26 |
| Physically challenging geography leading to beach | 33.196 p =< 0.001 | 1121.000; p = 0.711 MR Group 1 = 71.78 MR Group 2 = 75.44 r = −0.05 | 385.000; p = 0.402 MR Group 1 37.11 MR Group 3 32.86 r = −0.10 | 92.500; p =< 0.001 MR Group 1 31.36 MR Group 4 17.43 r = −0.53 | 2701.500; p = 0.077 MR Group 2 94.38 MR Group 3 80.13 r = −0.13 | 630.500; p =< 0.001 MR Group 2 88.19 MR Group 4 37.33 r = −0.45 | 304.000; p =< 0.001 MR Group 3 45.80 MR Group 4 25.26 r = −0.46 |
| Inaccessible lead-up pathways to beach | 25.514 p =< 0.001 | 1155.000; p = 0.877 MR Group 1 76.33 MR Group 2 74.82 r = −0.02 | 386.500; p = 0.404 MR Group 1 37.08 MR Group 3 32.89 r = −0.10 | 108.500; p = 0.001 MR Group 1 30.47 MR Group 4 18.02 r = −0.48 | 2862.000; p = 0.220 MR Group 2 93.15 MR Group 3 83.41 r = −0.09 | 767.000; p =< 0.001 MR Group 2 87.15 MR Group 4 42.41 r = −0.40 | 355.000; p =< 0.001 MR Group 3 44.76 MR Group 4 27.15 r = −0.40 |
| Inaccessible toilet | 15.134 p = 0.002 | 1139.000; p = 0.807 MR Group 1 77.22 MR Group 2 74.69 r = −0.03 | 340.000; p = 0.137 MR Group 1 39.61 MR Group 3 31.94 r = −0.18 | 137.000; p = 0.011 MR Group 1 28.89 MR Group 4 19.07 r = −0.38 | 2559.500; p = 0.030 MR Group 2 95.46 MR Group 3 77.23 r = −0.16 | 1039.000; p =< 0.001 MR Group 2 85.07 MR Group 4 52.48 r = −0.28 | 529.500; p = 0.139 MR Group 3 41.19 MR Group 4 33.19 r = −0.17 |
| Inaccessible shower | 14.308 p = 0.003 | 932.000; p = 0.136 MR Group 1 88.72 MR Group 2 73.11 r = −0.18 | 300.500; p = 0.041 MR Group 1 41.81 MR Group 3 31.13 r = −0.25 | 101.000; p =< 0.001 MR Group 1 30.89 MR Group 4 17.74 r = −0.50 | 2792.000; p = 0.167 MR Group 2 93.69 MR Group 3 81.98 r = −0.01 | 1110.500; p = 0.002 MR Group 2 84.52 MR Group 4 55.13 r = −0.25 | 518.000; p = 0.109 MR Group 3 41.43 MR Group 4 33.19 r = −0.18 |
| Inaccessible change room | 22.282 p =< 0.001 | 784.500; p = 0.017 MR Group 1 96.92 MR Group 2 71.99 r = −0.20 | 225.500; p = 0.002 MR Group 1 45.97 MR Group 3 29.60 r = −0.39 | 71.000; p =< 0.001 MR Group 1 32.56 MR Group 4 16.63 r = −0.61 | 2561.500; p = 0.032 MR Group 2 95.45 MR Group 3 77.28 r = −0.16 | 1062.500; p =< 0.001 MR Group 2 84.89 MR Group 4 53.35 r = −0.27 | 548.500; p = 0.207 MR Group 3 40.81 MR Group 4 34.31 r = −0.14 |
| Difficulty moving—soft sand | 65.742 p = 0.011 | 1032.000; p = 0.181 MR Group 1 83.17 MR Group 2 73.89 r = −0.16 | 364.000; p = 0.103 MR Group 1 38.28 MR Group 3 32.43 r = −0.20 | 48.000; p =< 0.001 MR Group 1 33.83 MR Group 4 15.78 r = −0.72 | 3062.500; p = 0.489 MR Group 2 91.62 MR Group 3 87.50 r = −0.05 | 501.500; p =< 0.001 MR Group 2 89.17 MR Group 4 32.57 r = −0.59 | 186.500; p =< 0.001 MR Group 3 48.19 MR Group 4 20.91 r = −0.66 |
| Difficulty moving—hard sand | 22.891 p =< 0.001 | 1043.000; p = 0.408 MR Group 1 82.56 MR Group 2 73.96 r = −0.10 | 412.000; p = 0.665 MR Group 1 35.61 MR Group 3 33.41 r = −0.05 | 91.000; p =< 0.001 MR Group 1 31.44 MR Group 4 17.37 r = −0.54 | 3071.500; p = 0.643 MR Group 2 89.45 MR Group 3 93.32 r = −0.03 | 833.00; p =< 0.001 MR Group 2 86.64 MR Group 4 44.85 r = −0.35 | 307.000; p =< 0.001 MR Group 3 45.73 MR Group 4 25.37 r = −0.45 |
| Difficult to access water | 45.199 p =< 0.001 | 1062.000; p = 0.430 MR Group 1 81.50 MR Group 2 74.11 r = −0.10 | 411.000; p = 0.610 MR Group 1 35.67 MR Group 3 33.39 r = −0.06 | 73.000; p =< 0.001 MR Group 1 32.44 MR Group 4 16.70 r = −0.61 | 3138.500; p = 0.792 MR Group 2 89.96 MR Group 3 91.95 r = −0.02 | 494.500; p =< 0.001 MR Group 2 89.23 MR Group 4 32.31 r = −0.51 | 198.500; p =< 0.001 MR Group 3 47.95 MR Group 4 21.35 r = −0.61 |
| Limited specialised beach mobility equipment | 649.238 p =< 0.001 | 742.000; p = 0.004 MR Group 1 99.28 MR Group 2 71.66 r = −0.23 | 315.000; p = 0.027 MR Group 1 41.00 MR Group 3 31.43 r = −0.27 | 22.000; p =< 0.001 MR Group 1 35.28 MR Group 4 14.81 r = −0.80 | 3056.500; p = 0.584 MR Group 2 89.33 MR Group 3 93.62 r = −0.04 | 535.000; p =< 0.001 MR Group 2 88.92 MR Group 4 33.81 r = −0.48 | 220.000; p =< 0.001 MR Group 3 47.51 MR Group 4 22.15 r = −0.58 |
| No hoist availability | 12.507 p = 0.006 | 880.000; p = 0.072 MR Group 1 91.61 MR Group 2 72.72 r = −0.22 | 284.500; p = 0.023 MR Group 1 42.69 MR Group 3 30.81 r = −0.28 | 113.500; p = 0.002 MR Group 1 30.19 MR Group 4 18.20 r = −0.46 | 2793.000; p = 0.167 MR Group 2 93.68 MR Group 3 82.00 r = −0.10 | 2453.500; p = 0.023 MR Group 2 83.69 MR Group 4 59.15 r = −0.21 | 549.000; p = 0.208 MR Group 3 40.80 MR Group 4 34.33 r = −0.14 |
| Limited retail services within 150 m | 7.176 p = 0.066 | ||||||
| Inaccessible shaded recreational areas | 14.786 p = 0.002 | 1144.500; p = 0.835 MR Group 1 73.08 MR Group 2 75.26 r = −0.03 | 345.500; p = 0.166 MR Group 1 39.31 MR Group 3 32.05 r = −0.17 | 148.000; p = 0.023 MR Group 1 28.28 MR Group 4 19.48 r = −0.34 | 2471.000; p = 0.015 MR Group 2 96.14 MR Group 3 75.43 r = −0.18 | 1066.000; p =< 0.001 MR Group 2 84.86 MR Group 4 53.48 r = −0.27 | 548.00; p = 0.206 MR Group 3 40.82 MR Group 4 34.30 r = −0.15 |
| Lack of physical assistance for transfers | 13.523 p = 0.004 | 1094.500; p = 0.613 MR Group 1 79.69 MR Group 2 74.35 r = −0.06 | 396.000; p = 0.514 MR Group 1 36.50 MR Group 3 33.08 r = −0.08 | 128.500; p = 0.006 MR Group 1 29.36 MR Group 4 18.76 r = −0.41 | 3085.500; p = 0.683 MR Group 2 91.45 MR Group 3 87.97 r = −0.03 | 997.500; p =< 0.001 MR Group 2 85.39 MR Group 4 76.91 r = −0.29 | 431.000; p = 0.010 MR Group 3 43.20 MR Group 4 29.96 r = −0.29 |
| Lack of physical assistance available for beach activities | 18.937 p =< 0.001 | 1137.000; p = 0.801 MR Group 1 77.33 MR Group 2 74.68 r = −0.03 | 405.000; p = 0.600 MR Group 1 36.00 MR Group 3 33.08 r = −0.06 | 125.500; p = 0.005 MR Group 1 29.53 MR Group 4 18.65 r = −0.42 | 3057.000; p = 0.614 MR Group 2 91.66 MR Group 3 87.39 r = −0.04 | 840.500; p =< 0.001 MR Group 2 95.58 MR Group 4 50.94 r = −0.35 | 376.000; p = 0.002 MR Group 3 44.33 MR Group 4 27.93 r = −0.39 |
| Personal safety—fear of falling | 16.063 p = 0.001 | 1007.000; p = 0.302 MR Group 1 65.44 MR Group 2 76.31 r = −0.13 | 365.000; p = 0.217 MR Group 1 39.31 MR Group 3 35.72 r = −0.15 | 173.500; p = 0.099 MR Group 1 26.86 MR Group 4 20.43 r = −0.25 | 3046.000; p = 0.588 MR Group 2 89.25 MR Group 3 93.84 r = −0.04 | 964.500; p =< 0.001 MR Group 2 85.64 MR Group 4 49.72 r = −0.30 | 357.000; p =< 0.001 MR Group 3 44.71 MR Group 4 27.22 r = −0.39 |
| Personal safety—reduced confidence outdoor mobility | 17.423 p =< 0.001 | 927.000; p = 0.128 MR Group 1 61.00 MR Group 2 76.92 r = −0.19 | 351.000; p = 0.190 MR Group 1 29.00 MR Group 3 35.84 r = −0.16 | 189.500; p = 0.204 MR Group 1 25.97 MR Group 4 21.02 r = −0.19 | 3145.500; p = 0.831 MR Group 2 90.99 MR Group 3 89.19 r = −0.02 | 936.000; p =< 0.001 MR Group 2 85.85 MR Group 4 48.67 r = −0.31 | 355.000; p =< 0.001 MR Group 3 44.76 MR Group 4 27.15 r = −0.39 |
| Personal safety—fear of water | 3.813 p = 0.282 | ||||||
| Facilitator | Kruskal−Wallis H | Mann–Whitney U | |||||
|---|---|---|---|---|---|---|---|
| Group 1 vs. Group 2 | Group 1 vs. Group 3 | Group 1 vs. Group 4 | Group 2 vs. Group 3 | Group 2 vs. Group 4 | Group 3 vs. Group 4 | ||
| More accessible parking | 11.953 p =< 0.008 | 1030.000; p = < 0.316 MR Group 1 66.72 MR Group 2 76.14 r = −0.08 | 416.000; p = 0.692 MR Group 1 32.61 MR Group 3 34.51 r = −0.05 | 165.00; p = 0.056 MR Group 1 27.33 MR Group 4 20.11 r = −0.28 | 3026.000; p = 0.495 MR Group 2 91.90 MR Group 3 86.76 r = −0.05 | 1118.000; p = <0.001 MR Group 2 84.47 MR Group 4 55.41 r = −0.27 | 460.000; p = 0.018 MR Group 3 42.61 MR Group 4 31.04 r = −0.27 |
| Accessible parking closer to beach access point | 13.094 p =< 0.004 | 1043.500; p =< 0.356 MR Group 1 82.53 MR Group 2 73.97 r = −0.08 | 362.500; p = 0.201 MR Group 1 38.36 MR Group 3 32.40 r = −0.16 | 133.000; p = 0.006 MR Group 1 29.11 MR Group 4 18.93 r = −0.41 | 2986.500; p = 0.411 MR Group 2 92.20 MR Group 3 85.95 r = −0.06 | 1122.000; p =< 0.001 MR Group 2 84.44 MR Group 4 55.56 r = −0.27 | 472.000; p = 0.027 MR Group 3 42.37 MR Group 4 31.48 r = −0.25 |
| Accessible lead-up pathways to beach | 30.086 p =< 0.001 | 924.500; p =< 0.047 MR Group 1 89.14 MR Group 2 73.06 r = −0.16 | 347.000; p = 0.060 MR Group 1 39.22 MR Group 3 32.08 r = −0.23 | 88.000; p =< 0.001 MR Group 1 31.61 MR Group 4 17.26 r = −0.60 | 3194.000; p = 0.949 MR Group 2 90.38 MR Group 3 90.82 r = −0.00 | 921.500; p =< 0.001 MR Group 2 85.97 MR Group 4 48.13 r = −0.37 | 341.500; p = <0.001 MR Group 3 45.03 MR Group 4 26.65 r = −0.45 |
| Sand walkway/access mat | 56.402 p < 0.001 | 936.000; p =< 0.035 MR Group 1 88.50 MR Group 2 73.15 r = −0.17 | 360.000; p = 0.053 MR Group 1 38.50 MR Group 3 32.35 r = −0.24 | 54.000; p =< 0.001 MR Group 1 33.50 MR Group 4 16.00 r = −0.72 | 3152.500; p = 0.793 MR Group 2 90.06 MR Group 3 91.66 r = −0.02 | 624.000; p =< 0.001 MR Group 2 88.24 MR Group 4 37.11 r = −0.52 | 229.500; p =< 0.001 MR Group 3 47.32 MR Group 4 22.50 r = −0.61 |
| Push beach wheeled walker | 21.686 p < 0.001 | 898.500; p =< 0.081 MR Group 1 59.42 MR Group 2 77.14 r = −0.14 | 278.500; p = 0.011 MR Group 1 24.97 MR Group 3 37.32 r = −0.31 | 214.000; p = 0.481 MR Group 1 24.61 MR Group 4 21.93 r = −0.11 | 2712.500; p = 0.080 MR Group 2 86.71 MR Group 3 100.64 r = −0.13 | 1034.500; p =< 0.001 MR Group 2 85.10 MR Group 4 52.31 r = −0.28 | 292.500; p =< 0.001 MR Group 3 46.03 MR Group 4 24.83 r = −0.49 |
| Wheelchair—sand access | 35.981 p < 0.001 | 822.000; p =< 0.015 MR Group 1 94.83 MR Group 2 72.27 r = −0.20 | 248.000; p = 0.002 MR Group 1 44.72 MR Group 3 30.06 r = −0.38 | 36.000; p =< 0.001 MR Group 1 34.50 MR Group 4 15.33 r = −0.75 | 2767.000; p = 0.111 MR Group 2 93.88 MR Group 3 81.47 r = −0.12 | 769.500; p =< 0.001 MR Group 2 87.13 MR Group 4 42.50 r = −0.40 | 376.500; p = 0.001 MR Group 3 44.32 MR Group 4 27.94 r = −0.37 |
| Wheelchair–water access | 26.900 p < 0.001 | 1083.500; p =< 0.528 MR Group 1 80.31 MR Group 2 74.27 r = −0.05 | 330.500; p = 0.091 MR Group 1 40.14 MR Group 3 31.74 r = −0.21 | 72.000; p = <0.001 MR Group 1 32.50 MR Group 4 16.67 r = −0.62 | 2725.500; p = 0.084 MR Group 2 94.19 MR Group 3 80.62 r = −0.13 | 798.500; p = <0.001 MR Group 2 86.90 MR Group 4 43.57 r = −0.39 | 404.500; p = 0.004 MR Group 3 43.74 MR Group 4 28.98 r = −0.33 |
| Accessible toilet | 22.042 p < 0.001 | 1022.500; p =< 0.290 MR Group 1 83.69 MR Group 2 73.81 r = −0.09 | 307.500; p = 0.038 MR Group 1 41.42 MR Group 3 31.28 r = −0.25 | 101.500; p = <0.001 MR Group 1 30.86 MR Group 4 17.76 r = −0.52 | 2693.500; p = 0.063 MR Group 2 94.44 MR Group 3 79.97 r = −0.14 | 953.000; p =< 0.001 MR Group 2 85.73 MR Group 4 49.30 r = −0.33 | 431.500; p = 0.009 MR Group 3 43.19 MR Group 4 29.98 r = −0.30 |
| Accessible shower | 27.454 p < 0.001 | 837.000; p =< 0.028 MR Group 1 94.00 MR Group 2 72.39 r = −0.18 | 281.000; p = 0.013 MR Group 1 42.89 MR Group 3 30.73 r = −0.30 | 62.500; p =< 0.001 MR Group 1 33.03 MR Group 4 16.31 r = −0.65 | 2986.500; p = 0.438 MR Group 2 92.20 MR Group 3 85.95 r = −0.06 | 868.000; p =< 0.001 MR Group 2 86.37 MR Group 4 46.15 r = −0.35 | 362.500; p =< 0.001 MR Group 3 44.60 MR Group 4 27.43 r = −0.39 |
| Accessible change room | 31.637 p < 0.001 | 738.000; p =< 0.004 MR Group 1 99.50 MR Group 2 71.63 r = −0.24 | 222.000; p = <0.001 MR Group 1 46.17 MR Group 3 29.53 r = −0.42 | 46.000; p = <0.001 MR Group 1 33.94 MR Group 4 15.70 r = −0.72 | 2771.500; p = 0.127 MR Group 2 93.84 MR Group 3 81.56 r = −0.11 | 888.000; p = <0.001 MR Group 2 86.22 MR Group 4 46.89 r = −0.35 | 422.000; p = 0.007 MR Group 3 43.38 MR Group 4 29.63 r = −0.31 |
| Accessible change table | 39.115 p < 0.001 | 378.000; p = <0.001 MR Group 1 119.50 MR Group 2 68.89 r = −0.40 | 924.500; p = 0.047 MR Group 1 54.17 MR Group 3 26.59 r = −0.65 | 30.000; p = <0.001 MR Group 1 34.83 MR Group 4 15.11 r = −0.78 | 2398.500; p = 0.007 MR Group 2 96.69 MR Group 3 73.95 r = −0.20 | 1290.500; p = 0.021 MR Group 2 83.15 MR Group 4 61.80 r = −0.18 | 661.500; p = 1.000 MR Group 3 38.50 MR Group 4 38.50 r = −0.00 |
| Hoist availability | 12.556 p =< 0.006 | 907.500; p =< 0.099 MR Group 1 90.08 MR Group 2 72.93 r = −0.14 | 78.000; p = 0.007 MR Group 1 44.22 MR Group 3 30.24 r = −0.33 | 134.000; p = 0.007 MR Group 1 29.06 MR Group 4 18.96 r = −0.40 | 2512.500; p = 0.020 MR Group 2 95.82 MR Group 3 76.28 r = −0.17 | 1359.500; p = 0.048 MR Group 2 82.62 MR Group 4 64.35 r = −0.16 | 643.000; p = 0.832 MR Group 3 38.12 MR Group 4 39.19 r = −0.02 |
| Food retail services within 150 m | 5.117 p =< 0.163 | ||||||
| Accessible shaded recreational areas | 16.395 p < 0.001 | 1165.500; p =< 0.918 MR Group 1 75.92 MR Group 2 74.87 r = −0.01 | 369.000; p = 0.285 MR Group 1 38.00 MR Group 3 32.53 r = −0.13 | 130.000; p = 0.007 MR Group 1 29.28 MR Group 4 18.81 r = −0.40 | 2716.000; p = 0.092 MR Group 2 94.27 MR Group 3 80.43 r = −0.13 | 969.500; p = <0.001 MR Group 2 85.60 MR Group 4 49.91 r = −0.31 | 470.500; p = 0.032 MR Group 3 42.40 MR Group 4 31.43 r = −0.25 |
| Accessible playground | 44.201 p < 0.001 | 470.500; p = <0.001 MR Group 1 114.36 MR Group 2 69.59 r = −0.35 | 79.500; p = <0.001 MR Group 1 54.08 MR Group 3 26.62 r = −0.64 | 57.000; p = <0.001 MR Group 1 33.33 MR Group 4 16.11 r = −0.67 | 1901.000; p = <0.001 MR Group 2 100.49 MR Group 3 63.80 r = −0.33 | 1269.000; p = 0.016 MR Group 2 83.31 MR Group 4 61.00 r = −0.19 | 559.000; p = 0.238 MR Group 3 36.41 MR Group 4 42.30 r = −0.14 |
| Physical assistance—car transfers | 6.680 p =< 0.083 | ||||||
| Physical assistance—transfers to beach mobility equipment | 11.264 p =< 0.010 | 1047.000; p =< 0.426 MR Group 1 82.33 MR Group 2 73.99 r = −0.07 | 351.000; p = 0.188 MR Group 1 39.00 MR Group 3 32.16 r = −0.16 | 144.000; p = 0.017 MR Group 1 28.50 MR Group 4 19.33 r = −0.36 | 2848.500; p = 0.230 MR Group 2 93.26 MR Group 3 83.13 r = −0.09 | 1126.000; p = 0.002 MR Group 2 84.40 MR Group 4 55.70 r = −0.24 | 477.500; p = 0.037 MR Group 3 42.26 MR Group 4 31.69 r = −0.24 |
| Physical assistance—personal care activities | 6.691 p =< 0.082 | ||||||
| Physical assistance—beach activities | 16.452 p < 0.001 | 1122.500; p =< 0.731 MR Group 1 78.14 MR Group 2 74.57 r = −0.03 | 372.000; p = 0.309 MR Group 1 37.83 MR Group 3 32.59 r = −0.12 | 122.000; p = 0.004 MR Group 1 29.72 MR Group 4 18.52 r = −0.43 | 2853.500; p = 0.234 MR Group 2 93.22 MR Group 3 83.23 r = −0.09 | 962.500; p =< 0.001 MR Group 2 85.65 MR Group 4 49.65 r = −0.31 | 409.500; p = 0.004 MR Group 3 43.64 MR Group 4 29.17 r = −0.33 |
| Physical assistance—ocean activities | 22.133 p < 0.001 | 1141.500; p =< 0.817 MR Group 1 77.08 MR Group 2 74.71 r = −0.02 | 372.500; p = 0.313 MR Group 1 37.81 MR Group 3 32.60 r = −0.12 | 110.500; p = 0.002 MR Group 1 30.36 MR Group 4 18.09 r = −0.47 | 2793.500; p = 0.160 MR Group 2 93.68 MR Group 3 82.01 r = −0.10 | 809.500; p = <0.001 MR Group 2 86.82 MR Group 4 43.98 r = −0.37 | 392.500; p = 0.003 MR Group 3 43.99 MR Group 4 28.54 r = −0.34 |
| Accessible beach events and activities | 36.814 p < 0.001 | 928.000; p =< 0.109 MR Group 1 88.94 MR Group 2 73.08 r = −0.13 | 287.000; p = 0.020 MR Group 1 42.56 MR Group 3 30.86 r = −0.29 | 41.000; p =< 0.001 MR Group 1 34.22 MR Group 4 15.52 r = −0.72 | 2749.000; p = 0.112 MR Group 2 94.02 MR Group 3 81.10 r = −0.12 | 632.000; p =< 0.001 MR Group 2 88.18 MR Group 4 37.41 r = −0.44 | 337.500; p =< 0.001 MR Group 3 45.11 MR Group 4 26.50 r = −0.42 |
| Booking system for accessibility equipment | 35.851 p < 0.001 | 10155.500; p=< 0.283 MR Group 1 84.08 MR Group 2 73.75 r = −0.09 | 298.500; p = 0.031 MR Group 1 41.92 MR Group 3 31.09 r = −0.26 | 44.500; p = <0.001 MR Group 1 34.03 MR Group 4 15.65 r = −0.71 | 2712.500; p = 0.084 MR Group 2 94.29 MR Group 3 80.36 r = −0.13 | 657.500; p = <0.001 MR Group 2 87.98 MR Group 4 38.35 r = −0.43 | 311.500; p = <0.001 MR Group 3 45.64 MR Group 4 25.54 r = −0.46 |
| Calendar of equipment availability and accessible events/activities | 41.084 p < 0.001 | 1080.000; p =< 0.504 MR Group 1 80.50 MR Group 2 74.24 r = −0.05 | 369.500; p = 0.250 MR Group 1 37.97 MR Group 3 32.54 r = −0.14 | 47.500; p = <0.001 MR Group 1 33.86 MR Group 4 15.76 r = −0.70 | 2987.500; p = 0.415 MR Group 2 92.19 MR Group 3 85.97 r = −0.06 | 560.500; p = <0.001 MR Group 2 88.72 MR Group 4 34.76 r = −0.48 | 250.000; p = <0.001 MR Group 3 46.90 MR Group 4 23.26 r = −0.54 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Job, S.; Heales, L.; Obst, S. Tides of Change—Barriers and Facilitators to Beach Accessibility for Older People and People with Disability: An Australian Community Survey. Int. J. Environ. Res. Public Health 2023, 20, 5651. https://doi.org/10.3390/ijerph20095651
Job S, Heales L, Obst S. Tides of Change—Barriers and Facilitators to Beach Accessibility for Older People and People with Disability: An Australian Community Survey. International Journal of Environmental Research and Public Health. 2023; 20(9):5651. https://doi.org/10.3390/ijerph20095651
Chicago/Turabian StyleJob, Sasha, Luke Heales, and Steven Obst. 2023. "Tides of Change—Barriers and Facilitators to Beach Accessibility for Older People and People with Disability: An Australian Community Survey" International Journal of Environmental Research and Public Health 20, no. 9: 5651. https://doi.org/10.3390/ijerph20095651