
Athletic Trainers’ Perceptions of and Experience with Social Determinants of Health
 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Design and Participants
2.2. Instrumentation
2.3. Procedures
2.4. Data Analysis
3. Results
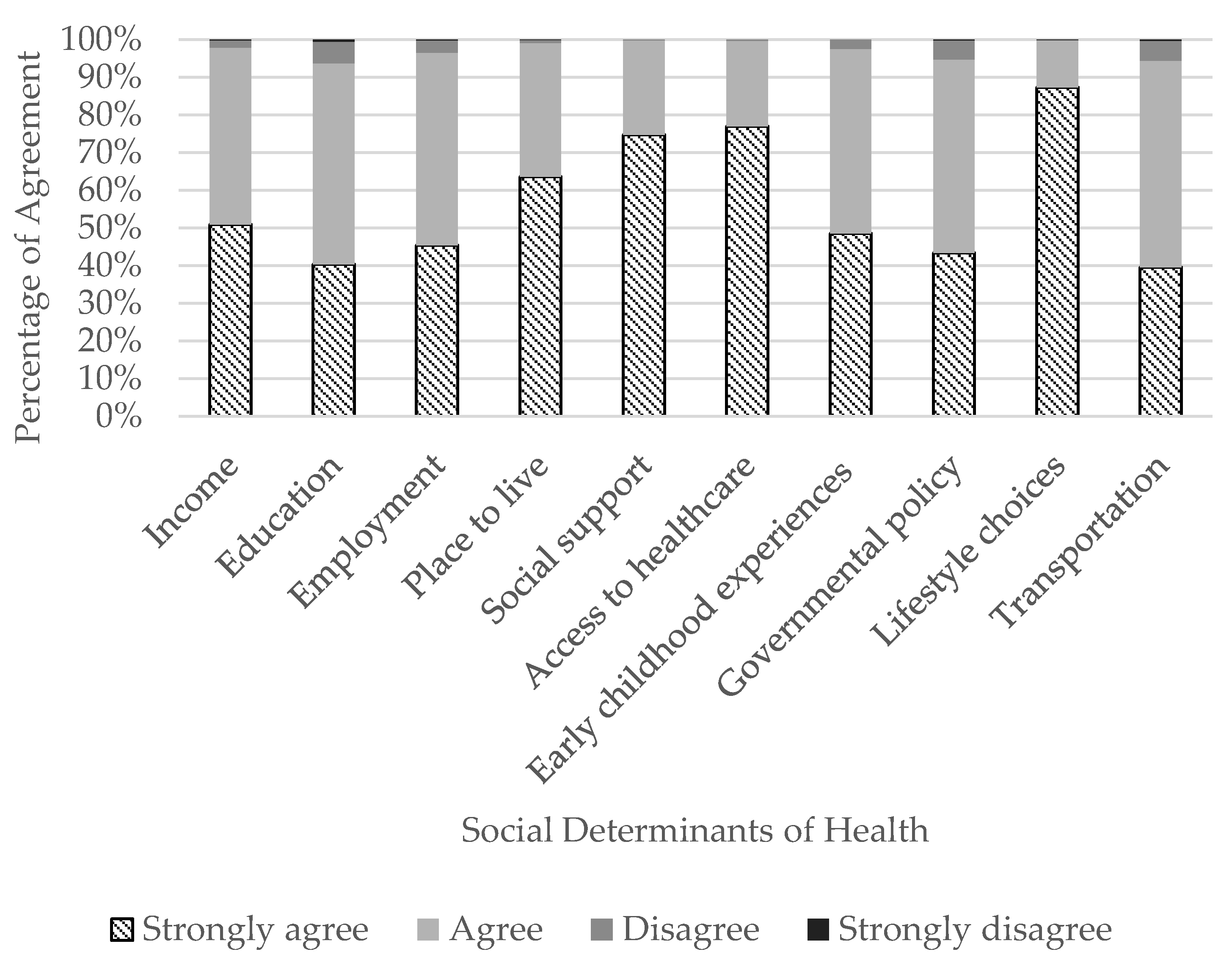
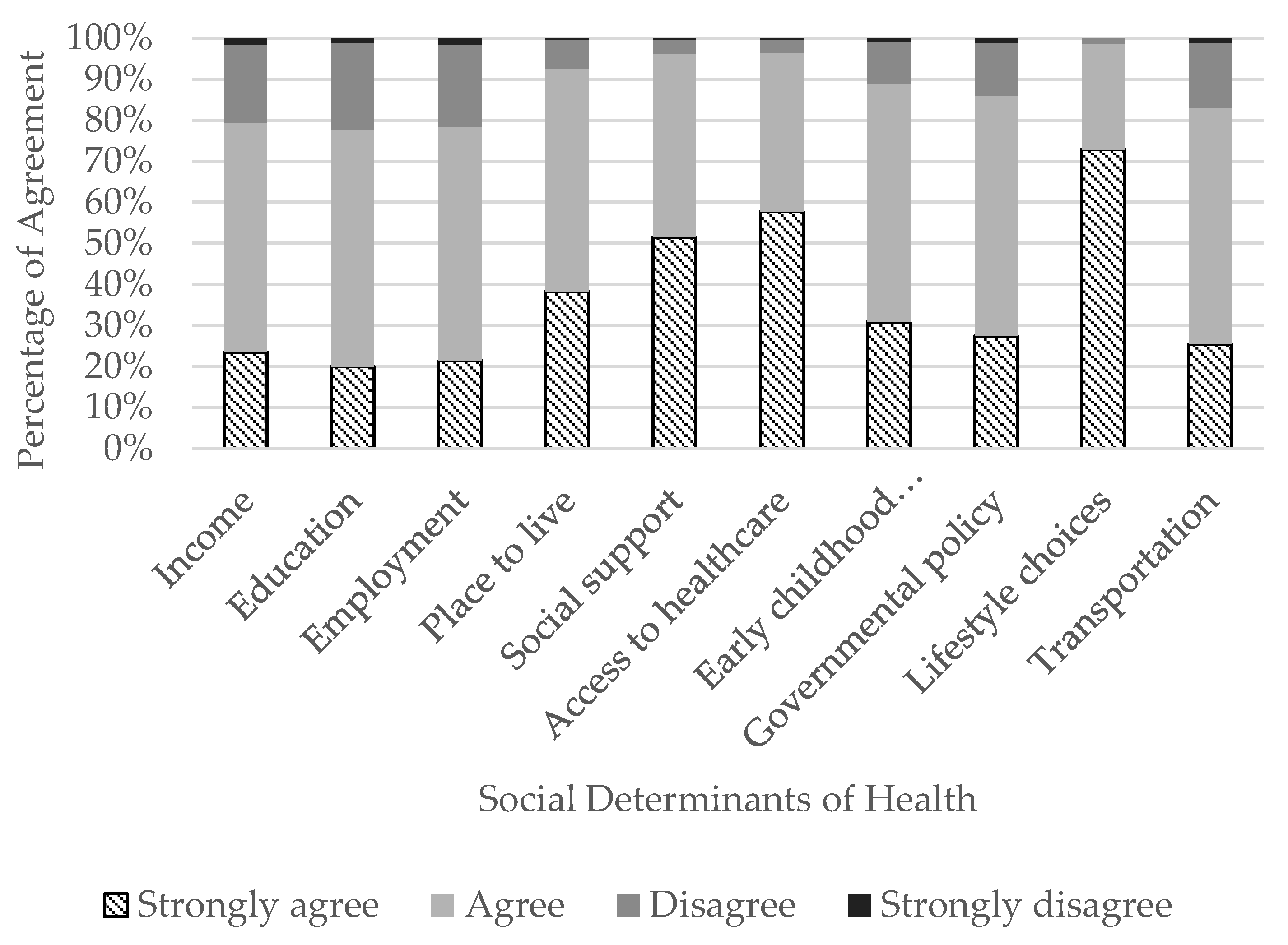
3.1. Perceptions of Social Determinants of Health
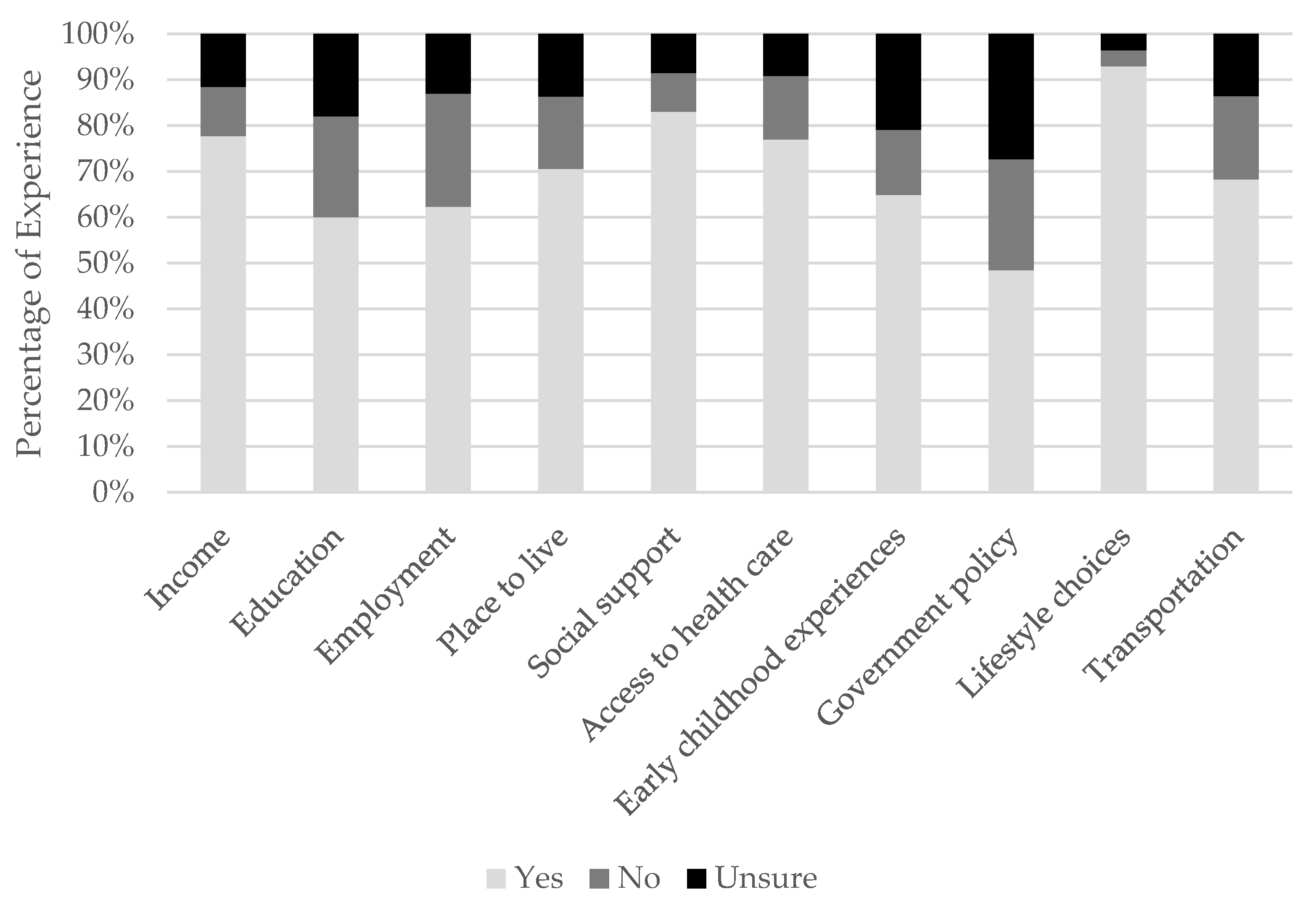
3.2. Experience with Social Determinants of Health
4. Discussion
Limitations and Future Research
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- National Academies of Science, Engineering, and Medicine. Social Determinants of Health (SDOH). Patient Engagement. Available online: https://catalyst.nejm.org/social-determinants-of-health/ (accessed on 17 April 2023).
- McGinnis, J.M.; Foege, W.H. Actual causes of death in the United States. JAMA 1993, 270, 2207–2212. [Google Scholar] [CrossRef] [PubMed]
- Wilkinson, R.; Marmot, M. Social Determinants of Health: The Solid Facts, 2nd ed.; World Health Organization: Copenhagen, Denmark, 2003. [Google Scholar]
- Marmot, M.; Allen, J.J. Social determinants of health equity. Am. J. Public. Health 2014, 104 (Suppl. 4), S517–S519. [Google Scholar] [CrossRef] [PubMed]
- Commission on Social Determinants of Health. Closing the Gap in a Generation: Health Equity through Action on the Social Determinants of Health. Final Report of the Commision on Social Determinants of Health; World Health Organization: Geneva, Switzerland, 2008; pp. 1–247. [Google Scholar]
- Centers for Disease Control and Prevention. About Social Determinants of Health (SDOH). Available online: https://www.cdc.gov/socialdeterminants/about.html (accessed on 11 May 2022).
- Robert Wood Johnson Foundation. Beyond Health Care: New Directions to a Healthier America; Robert Wood Johnson Foundation Commission to Build a Healthier America: Princeton, NJ, USA, 2009. [Google Scholar]
- Marmot, M.; Friel, S.; Bell, R.; Houweling, T.A.; Taylor, S. Closing the gap in a generation: Health equity through action on the social determinants of health. Lancet 2008, 372, 1661–1669. [Google Scholar] [CrossRef] [PubMed]
- Winfield, L.D.K.; Muhlestein, D. Social Determinants Matter, but Who is Responsible? 2017 Physician Survey on Social Determinants of Health; Leavitt Partners: Salt Lake City, UT, USA, 2018. [Google Scholar]
- Picha, K.J.; Welch Bacon, C.E.; Normore, C.; Snyder Valier, A.R. Social Determinants of Health: Considerations for Athletic Health Care. J. Athl. Train. 2021, 57, 521–531. [Google Scholar] [CrossRef] [PubMed]
- Freiburger, R.; Picha, K.J.; Welch Bacon, C.E.; Snyder Valier, A.R. Educational Technique: Incorporating Social Determinants of Health Into Athletic Training Education. Athl. Train. Educ. J. 2020, 15, 321–330. [Google Scholar] [CrossRef]
- Winkelmann, Z.K.; Games, K.E.; Rivera, M.J.; Neil, E.R.; Eberman, L.E. Athletic Trainers’ Knowledge and Practice Application of Public Health Topics. Athl. Train. Educ. J. 2020, 15, 308–320. [Google Scholar] [CrossRef]
- Lam, K.C.; Valier, A.R.; Anderson, B.E.; McLeod, T.C. Athletic Training Services During Daily Patient Encounters: A Report from the Athletic Training Practice-Based Research Network. J. Athl. Train. 2016, 51, 435–441. [Google Scholar] [CrossRef]
- Picha, K.J.; Welch Bacon, C.E.; Bay, C.; Lewis, J.; Snyder Valier, A.R. Athletic Trainers’ Familiarity, Comfort, Knowledge, and Recognition of Social Determinants of Health. J. Athl. Train. 2023, in press. [Google Scholar] [CrossRef]
- Lewis, J.H.; Whelihan, K.; Navarro, I.; Boyle, K.R.; Team, S.D.H.C.S.I. Community health center provider ability to identify, treat and account for the social determinants of health: A card study. BMC Fam. Prac. 2016, 17, 121. [Google Scholar] [CrossRef]
- Aubin, C. Attitudes and Beliefs about Social Determinants of Health; Halton Region Health Department: Burlington, NJ, USA, 2014. [Google Scholar]
- Gamble, T.K.; Gamble, M.W. The Interpersonal Communication Playbook; SAGE Publications: Washington, DC, USA, 2023. [Google Scholar]
- Berkman, L.F.; Kawachi, I.; Glymour, M.M. Social. Epidemiology; Oxford University Press: Oxford, UK, 2014. [Google Scholar]
- Viner, R.M.; Ozer, E.M.; Denny, S.; Marmot, M.; Resnick, M.; Fatusi, A.; Currie, C. Adolescence and the social determinants of health. Lancet 2012, 379, 1641–1652. [Google Scholar] [CrossRef]
- Mackenbach, J.P.; Stirbu, I.; Roskam, A.J.; Schaap, M.M.; Menvielle, G.; Leinsalu, M.; Kunst, A.E.; European Union Working Group on Socioeconomic Inequalities in Health. Socioeconomic inequalities in health in 22 European countries. N. Engl. J. Med. 2008, 358, 2468–2481. [Google Scholar] [CrossRef] [PubMed]
- Anderson, D.R.; Huston, A.C.; Schmitt, K.L.; Linebarger, D.L.; Wright, J.C. Early childhood television viewing and adolescent behavior: The recontact study. Monogr. Soc. Res. Child. Dev. 2001, 66, I–VIII, 1–147. [Google Scholar] [PubMed]
- Kucharczuk, A.J.; Oliver, T.L.; Dowdell, E.B. Social media’s influence on adolescents’ food choices: A mixed studies systematic literature review. Appetite 2022, 168, 105765. [Google Scholar] [CrossRef] [PubMed]
- Udry, E. Social support: Exploring its role in the context of athletic injuries. J. Sport Rehabil. 1996, 5, 151–163. [Google Scholar] [CrossRef]
- Lu, F.J.; Hsu, Y. Injured athletes’ rehabilitation beliefs and subjective well-being: The contribution of hope and social support. J. Athl. Train. 2013, 48, 92–98. [Google Scholar] [CrossRef]
- Clement, D.; Shannon, V.R. Injured athletes’ perceptions about social support. J. Sport. Rehabil. 2011, 20, 457–470. [Google Scholar] [CrossRef]
- Marshall, A.; Donovan-Hall, M.; Ryall, S. An exploration of athletes’ views on their adherence to physiotherapy rehabilitation after sport injury. J. Sport. Rehabil. 2012, 21, 18–25. [Google Scholar] [CrossRef]
- Cockerham, W.C.; Hamby, B.W.; Oates, G.R. The Social Determinants of Chronic Disease. Am. J. Prev. Med. 2017, 52, S5–S12. [Google Scholar] [CrossRef]
- Yang, J.; Schaefer, J.T.; Zhang, N.; Covassin, T.; Ding, K.; Heiden, E. Social support from the athletic trainer and symptoms of depression and anxiety at return to play. J. Athl. Train. 2014, 49, 773–779. [Google Scholar] [CrossRef]
- Prentice, W.E. Focusing the direction of our profession: Athletic trainers in America’s health care system. J. Athl. Train. 2013, 48, 7–8. [Google Scholar] [CrossRef]
- Hootman, J.M. 2008 Physical Activity Guidelines for Americans: An opportunity for athletic trainers. J. Athl. Train. 2009, 44, 5–6. [Google Scholar] [CrossRef]
- National Academies of Sciences, Engineering, and Medicine. Communities in Action: Pathways to Health Equity; The National Academies Press: Washington, DC, USA, 2017. [Google Scholar]
- Pryor, R.R.; Casa, D.J.; Vandermark, L.W.; Stearns, R.L.; Attanasio, S.M.; Fontaine, G.J.; Wafer, A.M. Athletic training services in public secondary schools: A benchmark study. J. Athl. Train. 2015, 50, 156–162. [Google Scholar] [CrossRef] [PubMed]
- Shanley, E.; Thigpen, C.A.; Chapman, C.G.; Thorpe, J.; Gilliland, R.G.; Sease, W.F. Athletic Trainers’ Effect on Population Health: Improving Access to and Quality of Care. J. Athl. Train. 2019, 54, 124–132. [Google Scholar] [CrossRef] [PubMed]
- Lucyk, K.; McLaren, L. Taking stock of the social determinants of health: A scoping review. PLoS ONE 2017, 12, e0177306. [Google Scholar] [CrossRef] [PubMed]
- Hughes, K.; Bellis, M.A.; Hardcastle, K.A.; Sethi, D.; Butchart, A.; Mikton, C.; Jones, L.; Dunne, M.P. The effect of multiple adverse childhood experiences on health: A systematic review and meta-analysis. Lancet Public. Health 2017, 2, e356–e366. [Google Scholar] [CrossRef]
- Anda, R.F.; Felitti, V.J.; Bremner, J.D.; Walker, J.D.; Whitfield, C.; Perry, B.D.; Dube, S.R.; Giles, W.H. The enduring effects of abuse and related adverse experiences in childhood. A convergence of evidence from neurobiology and epidemiology. Eur. Arch. Psychiatry Clin. Neurosci. 2006, 256, 174–186. [Google Scholar] [CrossRef]
- Bellis, M.A.; Hughes, K.; Leckenby, N.; Hardcastle, K.A.; Perkins, C.; Lowey, H. Measuring mortality and the burden of adult disease associated with adverse childhood experiences in England: A national survey. J. Public. Health 2015, 37, 445–454. [Google Scholar] [CrossRef]
- Berwick, D.M.; Nolan, T.W.; Whittington, J. The triple aim: Care, health, and cost. Health Aff. 2008, 27, 759–769. [Google Scholar] [CrossRef]
- Voelker, R. Decades of work to reduce disparities in health care produce limited success. JAMA 2008, 299, 1411–1413. [Google Scholar] [CrossRef]
- Chung, E.K.; Siegel, B.S.; Garg, A.; Conroy, K.; Gross, R.S.; Long, D.A.; Lewis, G.; Osman, C.J.; Jo Messito, M.; Wade, R., Jr.; et al. Screening for Social Determinants of Health Among Children and Families Living in Poverty: A Guide for Clinicians. Curr. Probl. Pediatr. Adolesc. Health Care 2016, 46, 135–153. [Google Scholar] [CrossRef]
- Finkelhor, D.; Shattuck, A.; Turner, H.; Hamby, S. A revised inventory of Adverse Childhood Experiences. Child Abuse Negl. 2015, 48, 13–21. [Google Scholar] [CrossRef] [PubMed]
- Nuruzzaman, N.; Broadwin, M.; Kourouma, K.; Olson, D.P. Making the social determinants of health a routine part of medical care. J. Health Care Poor Underserved 2015, 26, 321–327. [Google Scholar] [CrossRef] [PubMed]
- Billioux, A.; Verlander, K.; Anthony, S.; Alley, D. Standardized Screening for Health-Related Social Needs in Clinical Settings: The Accountable Health Communities Screening Tool. In NAM Perspectives; Discussion Paper; National Academy of Medicine: Washington, DC, USA, 2017. [Google Scholar] [CrossRef]
- Bleacher, H.; Lyon, C.; Mims, L.; Cebuhar, K.; Begum, A. The Feasibility of Screening for Social Determinants of Health: Seven Lessons Learned. Fam. Pr. Manag. 2019, 26, 13–19. [Google Scholar]
- Magnan, S. Social Determinants of Health 101 for Health Care: Five Plus Five; National Academy of Medicine: Washington, DC, USA, 2017. [Google Scholar]
- Eberman, L.E.; Winkelmann, Z.K.; Edler, J.R.; Neil, E.R. Athletic Trainers’ Knowledge Regarding Health Care Delivery Systems and Administration in the American Health Care System. Athl. Train. Educ. J. 2020, 15, 295–307. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| SDH | Questions Asked in the Survey |
|---|---|
| Access to quality and/or timely healthcare |
|
| Early childhood experiences |
|
| Education |
|
| Employment |
|
| Government policies and programs |
|
| Income |
|
| Lifestyle choices |
|
| Place to live |
|
| Social support |
|
| Transportation |
|
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Picha, K.J.; Welch Bacon, C.E.; Bay, R.C.; Lewis, J.H.; Snyder Valier, A.R. Athletic Trainers’ Perceptions of and Experience with Social Determinants of Health. Int. J. Environ. Res. Public Health 2023, 20, 5602. https://doi.org/10.3390/ijerph20085602
Picha KJ, Welch Bacon CE, Bay RC, Lewis JH, Snyder Valier AR. Athletic Trainers’ Perceptions of and Experience with Social Determinants of Health. International Journal of Environmental Research and Public Health. 2023; 20(8):5602. https://doi.org/10.3390/ijerph20085602
Chicago/Turabian StylePicha, Kelsey J., Cailee E. Welch Bacon, R. Curt Bay, Joy H. Lewis, and Alison R. Snyder Valier. 2023. "Athletic Trainers’ Perceptions of and Experience with Social Determinants of Health" International Journal of Environmental Research and Public Health 20, no. 8: 5602. https://doi.org/10.3390/ijerph20085602