
A Systematic Review of Joint Spatial and Spatiotemporal Models in Health Research

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Source and Search Strategy
2.2. Inclusion and Exclusion Criteria
2.3. Data Extraction
2.4. Risk of Bias Assessment
2.5. Data Synthesis and Analysis
3. Results
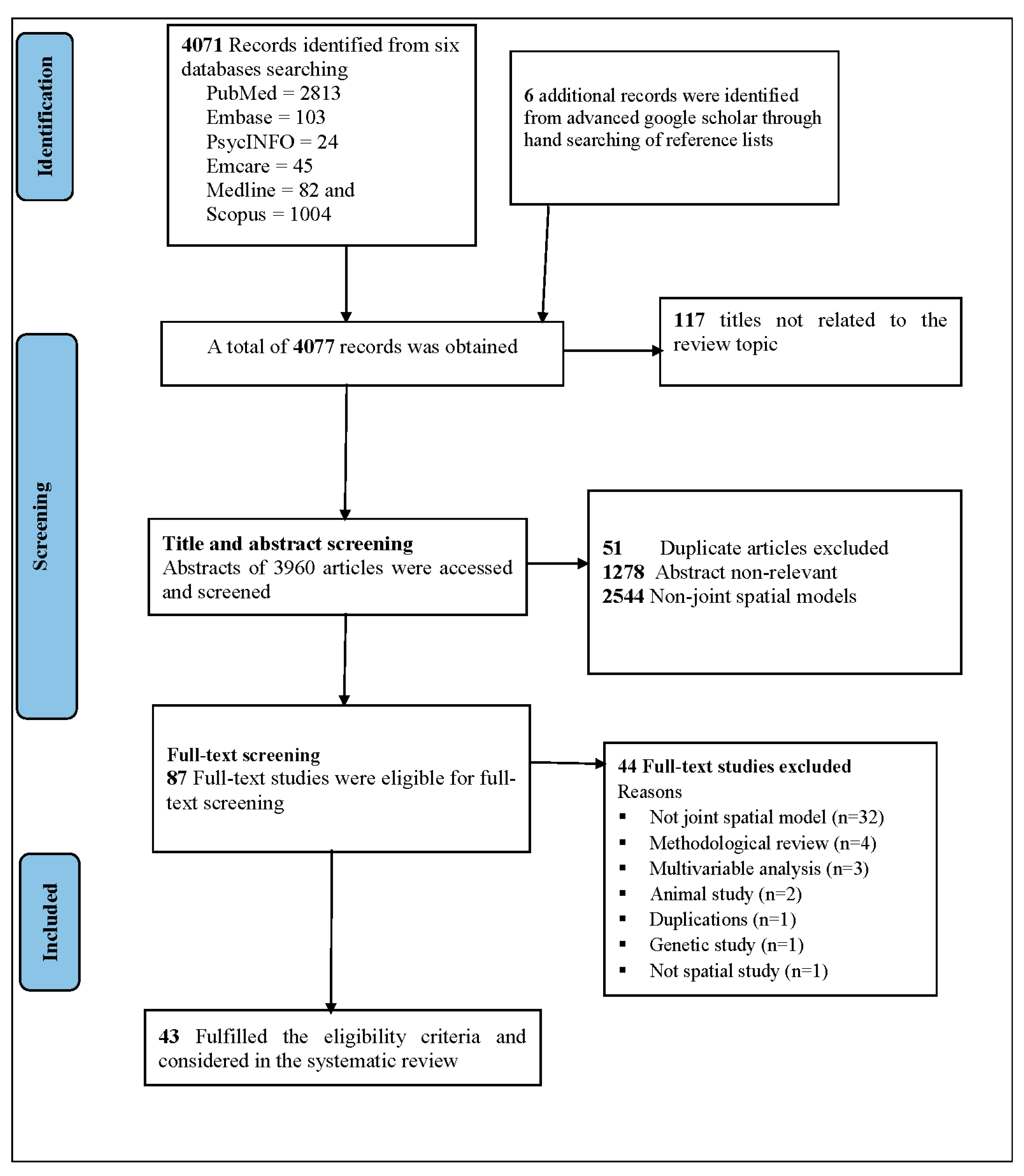
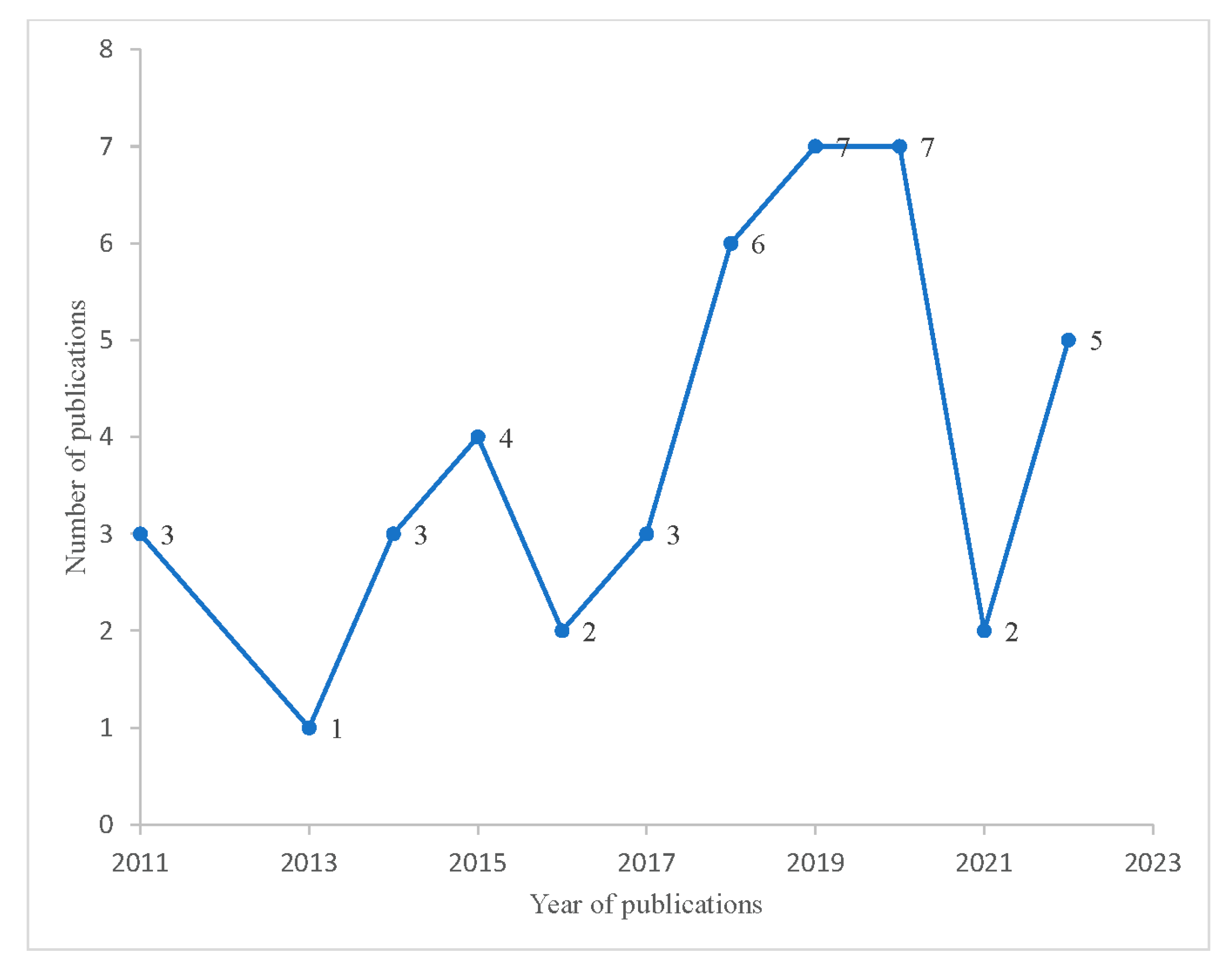
3.1. Search Results and Characteristics of Included Studies
3.2. Data Source, Study Design, and Unit of Analysis
3.3. Spatial Data and Modelling Techniques
3.4. Covariates, Model Validation, and Goodness of Fit Assessment
3.5. Key Implications of Applying Joint Spatial Modelling, Findings, and Methodological Gaps
3.6. Assessment of Quality
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Krieger, N. Place, space, and health: GIS and epidemiology. Epidemiology 2003, 14, 384–385. [Google Scholar] [CrossRef]
- Best, N.; Hansell, A.L. Geographic variations in risk: Adjusting for unmeasured confounders through joint modeling of multiple diseases. Epidemiology 2009, 20, 400. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Werneck, G.L. Georeferenced data in epidemiologic research. Ciência Saúde Coletiva 2008, 13, 1753–1766. [Google Scholar] [CrossRef]
- Sui, D.Z. Tobler’s first law of geography: A big idea for a small world? Ann. Assoc. Am. Geogr. 2004, 94, 269–277. [Google Scholar] [CrossRef]
- Leitner, M.; Glasner, P.; Kounadi, O. Laws of geography. In Oxford Research Encyclopedia of Criminology and Criminal Justice; Oxford University Press: New York, NY, USA, 2018. [Google Scholar]
- Andrienko, G.; Andrienko, N.; Demsar, U.; Dransch, D.; Dykes, J.; Fabrikant, S.I.; Jern, M.; Kraak, M.-J.; Schumann, H.; Tominski, C. Space, time and visual analytics. Int. J. Geogr. Inf. Sci. 2010, 24, 1577–1600. [Google Scholar] [CrossRef] [Green Version]
- Pfeiffer, D.U.; Robinson, T.P.; Stevenson, M.; Stevens, K.B.; Rogers, D.J.; Clements, A.C. Spatial Analysis in Epidemiology; OUP: Oxford, UK, 2008. [Google Scholar]
- Waller, L.A.; Carlin, B.P.; Xia, H.; Gelfand, A.E. Hierarchical spatio-temporal mapping of disease rates. J. Am. Stat. Assoc. 1997, 92, 607–617. [Google Scholar] [CrossRef]
- Lawson, A.B. Hierarchical modeling in spatial epidemiology. Wiley Interdiscip. Rev. Comput. Stat. 2014, 6, 405–417. [Google Scholar] [CrossRef]
- Beale, L.; Abellan, J.J.; Hodgson, S.; Jarup, L. Methodologic issues and approaches to spatial epidemiology. Environ. Health Perspect. 2008, 116, 1105–1110. [Google Scholar] [CrossRef] [Green Version]
- Lindgren, F.; Rue, H. Bayesian spatial modelling with R-INLA. J. Stat. Softw. 2015, 63, 1–25. [Google Scholar] [CrossRef] [Green Version]
- Louzada, F.; do Nascimento, D.C.; Egbon, O.A. Spatial statistical models: An overview under the Bayesian approach. Axioms 2021, 10, 307. [Google Scholar] [CrossRef]
- Lee, D. A comparison of conditional autoregressive models used in Bayesian disease mapping. Spat. Spatio-Temporal Epidemiol. 2011, 2, 79–89. [Google Scholar] [CrossRef]
- Fix, M.J.; Cooley, D.S.; Thibaud, E. Simultaneous autoregressive models for spatial extremes. Environmetrics 2021, 32, e2656. [Google Scholar] [CrossRef]
- De Oliveira, V. Bayesian analysis of conditional autoregressive models. Ann. Inst. Stat. Math. 2012, 64, 107–133. [Google Scholar] [CrossRef]
- Besag, J.; York, J.; Mollié, A. Bayesian image restoration, with two applications in spatial statistics. Ann. Inst. Stat. Math. 1991, 43, 1–20. [Google Scholar] [CrossRef]
- Leroux, B.G.; Lei, X.; Breslow, N. Estimation of disease rates in small areas: A new mixed model for spatial dependence. In Statistical Models in Epidemiology, the Environment, and Clinical Trials; Springer: Berlin/Heidelberg, Germany, 2000; pp. 179–191. [Google Scholar]
- Goodchild, M.F.; Longley, P.A. Geographic information science. In Handbook of Regional Science; Springer: Berlin/Heidelberg, Germany, 2021; pp. 1597–1614. [Google Scholar]
- Ancelet, S.; Abellan, J.J.; Del Rio Vilas, V.J.; Birch, C.; Richardson, S. Bayesian shared spatial-component models to combine and borrow strength across sparse disease surveillance sources. Biom. J. 2012, 54, 385–404. [Google Scholar] [CrossRef]
- Dabney, A.R.; Wakefield, J.C. Issues in the mapping of two diseases. Stat. Methods Med. Res. 2005, 14, 83–112. [Google Scholar] [CrossRef]
- Botella-Rocamora, P.; Martinez-Beneito, M.A.; Banerjee, S. A unifying modeling framework for highly multivariate disease mapping. Stat. Med. 2015, 34, 1548–1559. [Google Scholar] [CrossRef]
- Corberán-Vallet, A. Prospective surveillance of multivariate spatial disease data. Stat. Methods Med. Res. 2012, 21, 457–477. [Google Scholar] [CrossRef] [Green Version]
- Finley, A.O.; Banerjee, S.; Gelfand, A.E. spBayes for large univariate and multivariate point-referenced spatio-temporal data models. arXiv 2013, arXiv:1310.8192. [Google Scholar]
- Knorr-Held, L.; Best, N.G. A shared component model for detecting joint and selective clustering of two diseases. J. R. Stat. Soc. Ser. A 2001, 164, 73–85. [Google Scholar] [CrossRef]
- Blangiardo, M.; Cameletti, M. Spatial and Spatio-Temporal Bayesian Models with R-INLA; John Wiley & Sons: Hoboken, NJ, USA, 2015. [Google Scholar]
- Chang, C.-D.; Wang, C.-C.; Jiang, B.C. Using data mining techniques for multi-diseases prediction modeling of hypertension and hyperlipidemia by common risk factors. Expert Syst. Appl. 2011, 38, 5507–5513. [Google Scholar] [CrossRef]
- Wong, C.W.; Wong, T.Y.; Cheng, C.-Y.; Sabanayagam, C. Kidney and eye diseases: Common risk factors, etiological mechanisms, and pathways. Kidney Int. 2014, 85, 1290–1302. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Meijers, W.C.; de Boer, R.A. Common risk factors for heart failure and cancer. Cardiovasc. Res. 2019, 115, 844–853. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Held, L.; Natário, I.; Fenton, S.E.; Rue, H.; Becker, N. Towards joint disease mapping. Stat. Methods Med. Res. 2005, 14, 61–82. [Google Scholar] [CrossRef] [Green Version]
- Cressie, N.; Wikle, C.K. Statistics for Spatio-Temporal Data; John Wiley & Sons: Hoboken, NJ, USA, 2015. [Google Scholar]
- Gómez-Rubio, V.; Palmí-Perales, F.; López-Abente, G.; Ramis-Prieto, R.; Fernández-Navarro, P. Bayesian joint spatio-temporal analysis of multiple diseases. SORT-Stat. Oper. Res. Trans. 2019, 43, 51–74. [Google Scholar]
- Mahaki, B.; Mehrabi, Y.; Kavousi, A.; Schmid, V.J. Joint spatio-temporal shared component model with an application in Iran Cancer Data. Asian Pac. J. Cancer Prev. APJCP 2018, 19, 1553. [Google Scholar]
- Ahmadipanahmehrabadi, V.; Hassanzadeh, A.; Mahaki, B. Bivariate spatio-temporal shared component modeling: Mapping of relative death risk due to colorectal and stomach cancers in Iran provinces. Int. J. Prev. Med. 2019, 10, 39. [Google Scholar]
- Bermudi, P.M.M.; Pellini, A.C.G.; Rebolledo, E.A.S.; Diniz, C.S.G.; Aguiar, B.S.d.; Ribeiro, A.G.; Failla, M.A.; Baquero, O.S.; Chiaravalloti-Neto, F. Spatial pattern of mortality from breast and cervical cancer in the city of São Paulo. Rev. De Saúde Pública 2020, 54, 142. [Google Scholar] [CrossRef]
- Carroll, R.; Lawson, A.B.; Faes, C.; Kirby, R.S.; Aregay, M.; Watjou, K. Extensions to multivariate space time mixture modeling of small area cancer data. Int. J. Environ. Res. Public Health 2017, 14, 503. [Google Scholar] [CrossRef] [Green Version]
- Chamanpara, P.; Moghimbeigi, A.; Faradmal, J.; Poorolajal, J. Joint disease mapping of two digestive cancers in Golestan Province, Iran using a shared component model. Osong Public Health Res. Perspect. 2015, 6, 205–210. [Google Scholar] [CrossRef] [Green Version]
- Cramb, S.M.; Baade, P.D.; White, N.M.; Ryan, L.M.; Mengersen, K.L. Inferring lung cancer risk factor patterns through joint Bayesian spatio-temporal analysis. Cancer Epidemiol. 2015, 39, 430–439. [Google Scholar] [CrossRef] [Green Version]
- Mahaki, B.; Mehrabi, Y.; Kavousi, A.; Akbari, M.E.; Waldhoer, T.; Schmid, V.J.; Yaseri, M. Multivariate disease mapping of seven prevalent cancers in Iran using a shared component model. Asian. Pac. J. Cancer Prev. 2011, 12, 2353–2358. [Google Scholar]
- Nasrazadani, M.; Maracy, M.R.; Dreassi, E.; Mahaki, B. Mapping of stomach, colorectal, and bladder cancers in Iran, 2004–2009: Applying Bayesian polytomous logit model. Int. J. Prev. Med. 2018, 9, 104. [Google Scholar]
- Stoppa, G.; Mensi, C.; Fazzo, L.; Minelli, G.; Manno, V.; Consonni, D.; Biggeri, A.; Catelan, D. Spatial analysis of shared risk factors between pleural and ovarian cancer mortality in Lombardy (Italy). Int. J. Environ. Res. Public Health 2022, 19, 3467. [Google Scholar] [CrossRef]
- Raei, M.; Schmid, V.J.; Mahaki, B. Bivariate spatiotemporal disease mapping of cancer of the breast and cervix uteri among Iranian women. Geospat. Health 2018, 13, 645. [Google Scholar] [CrossRef]
- Asmarian, N.; Ayatollahi, S.M.T.; Sharafi, Z.; Zare, N. Bayesian spatial joint model for disease mapping of zero-inflated data with R-INLA: A simulation study and an application to male breast cancer in Iran. Int. J. Environ. Res. Public Health 2019, 16, 4460. [Google Scholar] [CrossRef] [Green Version]
- Adeyemi, R.A.; Zewotir, T.; Ramroop, S. Joint spatial mapping of childhood anemia and malnutrition in sub-Saharan Africa: A cross-sectional study of small-scale geographical disparities. Afr. Health Sci. 2019, 19, 2692–2712. [Google Scholar] [CrossRef]
- Baker, J.; White, N.; Mengersen, K.; Rolfe, M.; Morgan, G.G. Joint modelling of potentially avoidable hospitalisation for five diseases accounting for spatiotemporal effects: A case study in New South Wales, Australia. PLoS ONE 2017, 12, e0183653. [Google Scholar] [CrossRef] [Green Version]
- Besharati, M.M.; Kashani, A.T.; Li, Z.; Washington, S.; Prato, C.G. A bivariate random effects spatial model of traffic fatalities and injuries across Provinces of Iran. Accid. Anal. Prev. 2020, 136, 105394. [Google Scholar] [CrossRef]
- Kazembe, L.N.; Kandala, N.-B. Estimating areas of common risk in low birth weight and infant mortality in Namibia: A joint spatial analysis at sub-regional level. Spat. Spatio-Temporal Epidemiol. 2015, 12, 27–37. [Google Scholar] [CrossRef]
- Kline, D.; Hepler, S.; Bonny, A.; McKnight, E. A joint spatial model of opioid-associated deaths and treatment admissions in Ohio. Ann. Epidemiol 2019, 33, 19–23. [Google Scholar] [CrossRef] [PubMed]
- Kramer, M.R.; Williamson, R. Multivariate Bayesian spatial model of preterm birth and cardiovascular disease among Georgia women: Evidence for life course social determinants of health. Spat. Spatio-Temporal Epidemiol. 2013, 6, 25–35. [Google Scholar] [CrossRef] [PubMed]
- Law, J.; Perlman, C. Exploring geographic variation of mental health risk and service utilization of doctors and hospitals in Toronto: A shared component spatial modeling approach. Int. J. Environ. Res. Public Health 2018, 15, 593. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Law, J.; Quick, M.; Jadavji, A. A Bayesian spatial shared component model for identifying crime-general and crime-specific hotspots. Ann. GIS 2020, 26, 65–79. [Google Scholar] [CrossRef] [Green Version]
- Lawson, A.; Schritz, A.; Villarroel, L.; Aguayo, G.A. Multi-Scale Multivariate Models for Small Area Health Survey Data: A Chilean Example. Int. J. Environ. Res. Public Health 2020, 17, 1682. [Google Scholar] [CrossRef] [Green Version]
- Neelon, B.; Anthopolos, R.; Miranda, M.L. A spatial bivariate probit model for correlated binary data with application to adverse birth outcomes. Stat. Methods Med. Res. 2014, 23, 119–133. [Google Scholar] [CrossRef]
- Odhiambo, J.N.; Sartorius, B. Joint spatio-temporal modelling of adverse pregnancy outcomes sharing common risk factors at sub-county level in Kenya, 2016–2019. BMC Public Health 2021, 21, 1–13. [Google Scholar] [CrossRef]
- Okango, E.; Mwambi, H.; Ngesa, O.; Achia, T. Semi-parametric spatial joint modeling of HIV and HSV-2 among women in Kenya. PLoS ONE 2015, 10, e0135212. [Google Scholar] [CrossRef]
- Ransome, Y.; Subramanian, S.V.; Duncan, D.T.; Vlahov, D.; Warren, J. Multivariate spatiotemporal modeling of drug- and alcohol-poisoning deaths in New York City, 2009–2014. Spat. Spatio-Temporal Epidemiol. 2020, 32, 100306. [Google Scholar] [CrossRef]
- Norwood, T.A.; Encisa, C.; Wang, X.; Seliske, L.; Cunningham, J.; De, P. A Bayesian shared components modeling approach to develop small area indicators of social determinants of health with measures of uncertainty. Can. J. Public Health 2020, 111, 342–357. [Google Scholar] [CrossRef]
- Adebayo, S.B.; Gayawan, E.; Heumann, C.; Seiler, C. Joint modeling of Anaemia and Malaria in children under five in Nigeria. Spat. Spatio-Temporal Epidemiol. 2016, 17, 105–115. [Google Scholar] [CrossRef]
- Huang, G.; Lee, D.; Scott, E.M. Multivariate space-time modelling of multiple air pollutants and their health effects accounting for exposure uncertainty. Stat. Med. 2018, 37, 1134–1148. [Google Scholar] [CrossRef] [Green Version]
- Kang, J.; Zhang, N.; Shi, R. A Bayesian nonparametric model for spatially distributed multivariate binary data with application to a multidrug-resistant tuberculosis (MDR-TB) study. Biometrics 2014, 70, 981–992. [Google Scholar] [CrossRef] [Green Version]
- Roberts, D.J.; Zewotir, T. Shared component modelling of early childhood anaemia and malaria in Kenya, Malawi, Tanzania and Uganda. BMC Pediatr. 2022, 22, 1–11. [Google Scholar] [CrossRef]
- Carabali, M.; Schmidt, A.M.; Restrepo, B.N.; Kaufman, J.S. A joint spatial marked point process model for dengue and severe dengue in Medellin, Colombia. Spat. Spatio-Temporal Epidemiol. 2022, 41, 100495. [Google Scholar] [CrossRef]
- Kinyoki, D.K.; Manda, S.O.; Moloney, G.M.; Odundo, E.O.; Berkley, J.A.; Noor, A.M.; Kandala, N.B. Modelling the ecological comorbidity of acute respiratory infection, diarrhoea and stunting among children under the age of 5 years in Somalia. Int. Stat. Rev. 2017, 85, 164–176. [Google Scholar] [CrossRef] [Green Version]
- Lawson, A.B.; Carroll, R.; Castro, M. Joint spatial Bayesian modeling for studies combining longitudinal and cross-sectional data. Stat. Methods Med. Res. 2014, 23, 611–624. [Google Scholar] [CrossRef] [Green Version]
- Orunmoluyi, O.S.; Gayawan, E.; Manda, S. Spatial Co-Morbidity of Childhood Acute Respiratory Infection, Diarrhoea and Stunting in Nigeria. Int. J. Environ. Res. Public Health 2022, 19, 1838. [Google Scholar] [CrossRef]
- Otiende, V.A.; Achia, T.N.; Mwambi, H.G. Bayesian hierarchical modeling of joint spatiotemporal risk patterns for Human Immunodeficiency Virus (HIV) and Tuberculosis (TB) in Kenya. PLoS ONE 2020, 15, e0234456. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. Syst. Rev. 2021, 10, 1–11. [Google Scholar] [CrossRef]
- Lawson, A.B. Statistical Methods in Spatial Epidemiology; John Wiley & Sons: Hoboken, NJ, USA, 2013. [Google Scholar]
- Elliot, P.; Wakefield, J.C.; Best, N.G.; Briggs, D.J. Spatial Epidemiology: Methods and Applications; Oxford University Press: Oxford, UK, 2000. [Google Scholar]
- Rezaeian, M.; Dunn, G.; St Leger, S.; Appleby, L. Geographical epidemiology, spatial analysis and geographical information systems: A multidisciplinary glossary. J. Epidemiol. Community Health 2007, 61, 98–102. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fone, D.; Hollinghurst, S.; Temple, M.; Round, A.; Lester, N.; Weightman, A.; Roberts, K.; Coyle, E.; Bevan, G.; Palmer, S. Systematic review of the use and value of computer simulation modelling in population health and health care delivery. J. Public Health 2003, 25, 325–335. [Google Scholar] [CrossRef] [PubMed]
- Harris, R.C.; Sumner, T.; Knight, G.M.; White, R.G. Systematic review of mathematical models exploring the epidemiological impact of future TB vaccines. Hum. Vaccines Immunother. 2016, 12, 2813–2832. [Google Scholar] [CrossRef] [PubMed]
- Darikwa, T.B.; Manda, S.O. Spatial co-clustering of cardiovascular diseases and select risk factors among adults in South Africa. Int. J. Environ. Res. Public Health 2020, 17, 3583. [Google Scholar] [CrossRef] [PubMed]
- Roberts, D.J.; Zewotir, T. Copula geoadditive modelling of anaemia and malaria in young children in Kenya, Malawi, Tanzania and Uganda. J. Health Popul. Nutr. 2020, 39, 8. [Google Scholar] [CrossRef]
- Desjardins, M.; Whiteman, A.; Casas, I.; Delmelle, E. Space-time clusters and co-occurrence of chikungunya and dengue fever in Colombia from 2015 to 2016. Acta Trop. 2018, 185, 77–85. [Google Scholar] [CrossRef]
- Freitas, L.P.; Carabali, M.; Yuan, M.; Jaramillo-Ramirez, G.I.; Balaguera, C.G.; Restrepo, B.N.; Zinszer, K. Spatio-temporal clusters and patterns of spread of dengue, chikungunya, and Zika in Colombia. medRxiv 2022, 16, e0010334. [Google Scholar] [CrossRef]
- Schur, N.; Gosoniu, L.; Raso, G.; Utzinger, J.; Vounatsou, P. Modelling the geographical distribution of co-infection risk from single-disease surveys. Stat. Med. 2011, 30, 1761–1776. [Google Scholar] [CrossRef]
- Stensgaard, A.-S.; Vounatsou, P.; Onapa, A.W.; Simonsen, P.E.; Pedersen, E.M.; Rahbek, C.; Kristensen, T.K. Bayesian geostatistical modelling of malaria and lymphatic filariasis infections in Uganda: Predictors of risk and geographical patterns of co-endemicity. Malar. J. 2011, 10, 298. [Google Scholar] [CrossRef] [Green Version]
- Chidumwa, G.; Maposa, I.; Kowal, P.; Micklesfield, L.K.; Ware, L.J. Bivariate joint spatial modeling to identify shared risk patterns of hypertension and diabetes in south africa: Evidence from WHO SAGE South Africa Wave 2. Int. J. Environ. Res. Public Health 2021, 18, 359. [Google Scholar] [CrossRef]
- Adegboye, O.; Al-Saghir, M.; LEUNG, D.H. Joint spatial time-series epidemiological analysis of malaria and cutaneous leishmaniasis infection. Epidemiol. Infect. 2017, 145, 685–700. [Google Scholar] [CrossRef] [Green Version]
- Darikwa, T.B.; Manda, S.; Lesaoana, M. Assessing joint spatial autocorrelations between mortality rates due to cardiovascular conditions in South Africa. Geospat. Health 2019, 14. [Google Scholar] [CrossRef]
- Bhutta, Z.A.; Sommerfeld, J.; Lassi, Z.S.; Salam, R.A.; Das, J.K. Global burden, distribution, and interventions for infectious diseases of poverty. Infect. Dis. Poverty 2014, 3, 21. [Google Scholar] [CrossRef] [Green Version]
- Murray, C.J.; Lopez, A.D. Measuring the global burden of disease. N. Engl. J. Med. 2013, 369, 448–457. [Google Scholar] [CrossRef] [Green Version]
- Bruchfeld, J.; Correia-Neves, M.; Källenius, G. Tuberculosis and HIV coinfection. Cold Spring Harb. Perspect. Med. 2015, 5, a017871. [Google Scholar] [CrossRef]
- Richardson, S.; Abellan, J.J.; Best, N. Bayesian spatio-temporal analysis of joint patterns of male and female lung cancer risks in Yorkshire (UK). Stat. Methods Med. Res. 2006, 15, 385–407. [Google Scholar] [CrossRef]
- Lewandowska, A.M.; Rudzki, M.; Rudzki, S.; Lewandowski, T.; Laskowska, B. Environmental risk factors for cancer-review paper. Ann. Agric. Environ. Med. 2018, 26, 1–7. [Google Scholar] [CrossRef]
- Stein, C.; Colditz, G. Modifiable risk factors for cancer. Br. J. Cancer 2004, 90, 299–303. [Google Scholar] [CrossRef] [Green Version]
- De Pergola, G.; Silvestris, F. Obesity as a major risk factor for cancer. J. Obes. 2013, 2013, 291546. [Google Scholar] [CrossRef] [Green Version]
- Morens, D.M.; Breman, J.G.; Calisher, C.H.; Doherty, P.C.; Hahn, B.H.; Keusch, G.T.; Kramer, L.D.; LeDuc, J.W.; Monath, T.P.; Taubenberger, J.K. The origin of COVID-19 and why it matters. Am. J. Trop. Med. Hyg. 2020, 103, 955. [Google Scholar] [CrossRef]
- Best, N.; Richardson, S.; Thomson, A. A comparison of Bayesian spatial models for disease mapping. Stat. Methods Med. Res. 2005, 14, 35–59. [Google Scholar] [CrossRef] [PubMed]
- Rutstein, S.O.; Rojas, G. Guide to DHS statistics. Calverton MD ORC Macro 2006, 38, 78. [Google Scholar]
- Kulldorff, M.; Mostashari, F.; Duczmal, L.; Katherine Yih, W.; Kleinman, K.; Platt, R. Multivariate scan statistics for disease surveillance. Stat. Med. 2007, 26, 1824–1833. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Scrucca, L. Clustering multivariate spatial data based on local measures of spatial autocorrelation. Quad. Del Dip. Di Econ. Finanz. E Stat. 2005, 20, 11. [Google Scholar]
- Vicente, G.; Goicoa, T.; Ugarte, M. Bayesian inference in multivariate spatio-temporal areal models using INLA: Analysis of gender-based violence in small areas. Stoch. Environ. Res. Risk Assess. 2020, 34, 1421–1440. [Google Scholar] [CrossRef]
- Besag, J. Spatial interaction and the statistical analysis of lattice systems. J. R. Stat. Soc. Ser. B 1974, 36, 192–225. [Google Scholar] [CrossRef]
- Mossel, E.; Vigoda, E. Limitations of Markov chain Monte Carlo algorithms for Bayesian inference of phylogeny. Ann. Appl. Probab. 2006, 16, 2215–2234. [Google Scholar] [CrossRef] [Green Version]
- Gómez-Rubio, V. Bayesian Inference with INLA; CRC Press: Boca Raton, FL, USA, 2020. [Google Scholar]
- Held, L.; Schrödle, B.; Rue, H. Posterior and cross-validatory predictive checks: A comparison of MCMC and INLA. In Statistical Modelling and Regression Structures; Springer: Berlin/Heidelberg, Germany, 2010; pp. 91–110. [Google Scholar]
- Carroll, R.; Lawson, A.; Faes, C.; Kirby, R.S.; Aregay, M.; Watjou, K. Comparing INLA and OpenBUGS for hierarchical Poisson modeling in disease mapping. Spat. Spatio-Temporal Epidemiol. 2015, 14, 45–54. [Google Scholar] [CrossRef] [Green Version]
- Lawson, A.B.; Biggeri, A.; Böhning, D.; Lesaffre, E.; Viel, J.-F.; Clark, A.; Schlattmann, P.; Divino, F. Disease mapping models: An empirical evaluation. Disease Mapping Collaborative Group. Stat. Med. 2000, 19, 2217–2241. [Google Scholar]
- Li, J. Application of Copulas as a New Geostatistical Tool; Universität Stuttgart: Stuttgart, Germany, 2010. [Google Scholar]
- Morris, M.; Wheeler-Martin, K.; Simpson, D.; Mooney, S.J.; Gelman, A.; DiMaggio, C. Bayesian hierarchical spatial models: Implementing the Besag York Mollié model in stan. Spat. Spatio-Temporal Epidemiol. 2019, 31, 100301. [Google Scholar] [CrossRef]
- Duncan, E.W.; Mengersen, K.L. Comparing Bayesian spatial models: Goodness-of-smoothing criteria for assessing under-and over-smoothing. PLoS ONE 2020, 15, e0233019. [Google Scholar] [CrossRef]
- Spiegelhalter, D.J.; Best, N.G.; Carlin, B.P.; Van der Linde, A. The deviance information criterion: 12 years on. J. R. Stat. Soc. Ser. B 2014, 76, 485–493. [Google Scholar] [CrossRef]
- Aregay, M.; Lawson, A.B.; Faes, C.; Kirby, R. Bayesian multiscale modeling for aggregated disease mapping data. In Proceedings of the Third ACM SIGSPATIAL International Workshop on the Use of GIS in Public Health, Dallas, TX, USA, 4 November 2014; pp. 45–48. [Google Scholar]




{kind=link}
{kind=link}
{kind=link}
| Characteristics | Frequency | Percentage (%) | References |
|---|---|---|---|
| Study category | |||
| Cancer | 11 | 25.58 | [32,33,34,35,36,37,38,39,40,41,42] |
| Chronic diseases | 7 | 16.28 | [44,48,51,58,72,73,74] |
| Infectious diseases | 15 | 34.88 | [54,57,59,60,61,62,63,64,65,75,76,77,78,79,80] |
| Health service utilisation | 1 | 2.33 | [49] |
| Maternal and child health outcomes | 3 | 6.98 | [46,52,53] |
| Others * | 6 | 13.95 | [43,45,47,50,55,56] |
| Publication journal | |||
| International Journal of Environmental Research and Public Health | 7 | 16.67 | [35,40,49,51,64,72,73] |
| Spatial and Spatio-temporal Epidemiology | 5 | 11.63 | [46,48,55,57,61] |
| PLOS ONE | 3 | 6.98 | [44,54,65] |
| Statistics in Medicine | 2 | 6.65 | [58,78] |
| Statistical Methods in Medical Research | 2 | 4.65 | [52,63] |
| BMC Public Health | 1 | 2.32 | [53] |
| Malaria journal | 1 | 2.32 | [79] |
| Epidemiology and infection | 1 | 2.32 | [80] |
| Annuals of GIS | 1 | 2.32 | [50] |
| Geospatial Health | 1 | 2.32 | [74] |
| International Journal of Preventive Medicine | 2 | 4.65 | [33,39] |
| International Statistical Review | 1 | 2.32 | [62] |
| African Health Sciences | 1 | 2.32 | [43] |
| Journal of Health, Population, and Nutrition | 1 | 2.32 | [75] |
| Others ** | 12 | 27.91 | [32,34,36,37,38,45,47,56,59,60,76,77] |
| Item | Category | Number | Percentage (%) | References |
|---|---|---|---|---|
| Data source(s) | DHS or National health survey | 7 | 16.28 | [43,46,51,60,64,72,75] |
| Malaria indicator survey | 3 | 6.98 | [57,63,75] | |
| HMIS/DHIS | 2 | 4.65 | [53,80] | |
| Death and cause of death registration system | 1 | 2.33 | [33] | |
| Multiple surveys | 5 | 11.63 | [37,38,47,65,80] | |
| Hospital records | 2 | 4.65 | [44,59] | |
| AIDS indicator survey | 1 | 2.33 | [54] | |
| Cancer registry | 7 | 16.28 | [35,36,37,38,39,41,42] | |
| Others * | 23 | 53.49 | [32,40,46,47,48,49,50,51,52,53,54,55,56,58,61,62,63,73,74,76,77,78,79] | |
| Study design (More than one design was applied in some of the studies) | Ecological | 18 | 41.86 | [32,33,34,38,39,40,47,48,49,52,55,58,61,73,74,76,77,79] |
| Cross-sectional | 14 | 32.56 | [43,46,51,54,56,57,60,62,63,64,72,75,78,80] | |
| Retrospective | 9 | 20.93 | [35,36,37,41,42,44,45,59,65] | |
| Longitudinal | 2 | 4.65 | [51,53] | |
| Others ** | 2 | 4.65 | [49,50] | |
| Number of outcomes of the study | 2 | 24 | 55.81 | [33,34,36,37,40,41,45,46,48,49,50,52,54,55,58,60,61,65,72,73,75,76,78,79,80] |
| 3 | 7 | 16.28 | [35,39,43,62,64,74,77] | |
| 4 | 2 | 4.65 | [51,53] | |
| 5 | 2 | 4.65 | [44,56] | |
| 6 | 0 | 0 | ---- | |
| 7 | 2 | 4.65 | [32,38] | |
| Prevalence of outcomes of the study | All less than 10% | 11 | 25.58 | [33,34,35,36,37,41,42,46,52,53,61] |
| Either of them is less than 10% | 4 | 9.30 | [48,51,79,80] | |
| All greater than 10% | 6 | 13.95 | [43,45,60,62,73,75] | |
| Not reported | 22 | 51.16 | [32,38,39,40,44,47,49,50,54,55,56,57,58,59,63,65,72,74,76,77,78] | |
| Spatial unit | Provinces | 11 | 25.58 | [32,33,35,36,38,39,41,43,45,51,80] |
| County | 7 | 16.28 | [42,47,48,52,53,54,65] | |
| Municipalities | 4 | 9.30 | [40,74,76,77] | |
| Districts | 3 | 6.98 | [60,72,73,75] | |
| Schools/Health facility | 3 | 6.98 | [34,78,79] | |
| SLAs | 1 | 2.33 | [37] | |
| Not reported | 1 | 2.33 | [59] | |
| Others *** | 12 | 27.91 | [44,46,49,50,55,56,57,58,61,62,63,64] | |
| Temporal units (n = 17) | Year | 15 | 88.23 | [32,33,34,35,37,41,44,45,53,58,62,65,74,76] |
| Month | 1 | 5.88 | [80] | |
| Weeks | 1 | 5.88 | [77] |
| Items | Number | Percentage (%) | References |
|---|---|---|---|
| Types of spatial data | |||
| Point | 7 | 16.38 | [59,61,62,76,77,78,79] |
| Area | 36 | 83.72 | [32,33,34,35,36,37,38,39,40,41,42,43,44,45,46,47,48,49,50,51,52,53,54,55,56,58,60,63,64,65,72,73,74,75] |
| Methods of inference | |||
| Frequentist | 8 | 18.60 | [34,72,74,75,76,77,78,80] |
| Bayesian | 35 | 81.40 | [32,33,35,36,37,38,39,40,41,42,43,44,45,46,47,48,49,50,51,52,53,54,55,56,57,58,59,60,61,62,63,64,65,73,79] |
| Estimation techniques (n = 36) | |||
| ML | 2 | 4.65 | [75,80] |
| MCMC | 27 | 62.79 | [32,33,35,36,37,38,39,40,41,43,44,45,46,47,48,49,50,51,52,53,54,55,56,57,58,59,60] |
| INLA | 7 | 16.28 | [42,43,61,62,63,64,65] |
| Joint spatial analysis techniques | |||
| Joint spatial autocorrelation analysis | 7 | 16.28 | [34,72,74,76,77,78,79] |
| Joint spatial models | 24 | 55.81 | [36,38,39,40,42,43,45,46,47,48,49,50,51,52,54,56,57,59,60,61,62,64,73,75] |
| Joint Spatio-temporal models | 12 | 27.91 | [32,33,35,37,41,44,55,58,63,65,80] |
| Spatial structure (n = 36) | |||
| MCAR/BCAR/ ICAR/CAR | 26 | 72.22 | [32,33,35,36,37,38,39,40,41,43,44,46,47,48,49,50,51,52,53,55,58,60,61,63,64,65] |
| SAR | 1 | 2.78 | [45] |
| GMRF | 3 | 8.33 | [42,54,57] |
| Not reported | 6 | 16.67 | [56,59,62,73,75,80] |
| Temporal structure (n = 12) | |||
| Prior first-order random walk | 7 | 58.33 | [32,33,35,41,53,58,65] |
| log-linear structure | 1 | 8.33 | [44] |
| Prior first-order autoregressive | 2 | 16.66 | [37,55] |
| Second-order random walk | 1 | 8.33 | [63] |
| Not reported | 1 | 8.33 | [80] |
| Spatio-temporal term (n = 12) | |||
| Uncorrelated ST interaction term | 1 | 8.33 | [35] |
| Simple exchangeable hierarchical Structure | 5 | 41.67 | [32,33,41,53,65] |
| First order autoregressive | 1 | 8.33 | [58] |
| Not reported | 5 | 41.67 | [37,44,55,63,80] |
| The software’s used | |||
| R/R-studio/R2WinBUGS/R-INLA | 26 | 60.47 | [34,35,36,42,43,44,45,48,51,52,54,55,56,57,58,59,60,61,62,63,64,65,75,77,79,80] |
| ArcGIS/QGIS | 7 | 16.28 | [38,41,50,53,60,75,77] |
| WinBUGS/OpenBUGS/GeoBUGS | 21 | 48.84 | [32,33,36,37,38,39,40,41,43,44,46,49,50,51,53,54,56,63,73,78,79] |
| GeoDA | 4 | 9.30 | [34,45,72,74] |
| SaTScan | 3 | 6.98 | [76,77,80] |
| Fortran/MATLAB | 2 | 4.65 | [47,78] |
| Spatial models used (n = 36) | |||
| A multivariate negative binomial model with CAR random effects | 2 | 5.56 | [43,80] |
| Multivariate Bayesian Spatio-temporal shared component model with Poisson distribution | 2 | 5.56 | [33,37] |
| Poisson generalised linear mixed model (GLMM) with a shared spatial component with the log-linear temporal trend | 1 | 2.78 | [44] |
| Multivariate spatial autocorrelation and hotspot analysis | 7 | 19.44 | [34,48,72,74,76,77,80] |
| Joint spatial marked point processes model with Poisson distribution | 1 | 2.78 | [61] |
| Bayesian multivariate ST mixture model | 1 | 2.78 | [35] |
| Bivariate bayesian logit spatial model | 4 | 11.11 | [46,51,63,64] |
| Bayesian hierarchical geostatistical shared component model/ Bivariate bayesian geostatistical logistic model | 2 | 5.56 | [62,78] |
| A bayesian multivariate conditional auto-regressive model with Poisson distribution | 1 | 2.78 | [48] |
| Bayesian spatial Polytomous Logit Model | 1 | 2.78 | [39] |
| Bayesian spatial biprobit model | 1 | 2.78 | [52] |
| Joint bayesian Spatio-temporal shared component binomial model/Bayesian joint hierarchical Spatio-temporal Log-linear model/Bayesian shared component model | 4 | 11.11 | [42,53,60,65] |
| Bayesian semi-parametric spatial joint model/Bayesian nonparametric model using Gaussian processes for the analysis of spatially distributed multivariate binary outcome | 2 | 5.56 | [54,59] |
| Geoadditive mixed model | 2 | 5.56 | [57,75] |
| Bayesian geostatistical shared component multinomial modelling | 1 | 2.78 | [78] |
| Bayesian ANOVA | 1 | 2.78 | [56] |
| Model validation (n = 36) | |||
| No | 31 | 86.11 | [32,33,35,36,37,38,39,40,41,43,44,45,46,47,48,49,50,51,52,53,54,55,56,57,60,61,62,64,65,73,75] |
| Yes | 5 | 13.89 | [42,58,59,63,80] |
| Model comparison metrics (n = 36) | |||
| DIC | 22 | 51.16 | [32,33,37,38,39,41,43,44,46,47,48,49,52,53,54,60,61,62,63,64,73,78] |
| WAIC | 4 | 9.30 | [35,40,55,62] |
| CPO | 2 | 4.65 | [37,62] |
| PIT | 1 | 2.33 | [62] |
| RMSPE/Mean absolute error | 6 | 13.95 | [35,37,44,58,59,78] |
| KL | 1 | 2.33 | [40] |
| Credible interval plot | 1 | 2.33 | [78] |
| Bayesian p-value and L-criterion | 1 | 2.33 | [37] |
| Others * (AIC, BIC) | 2 | 4.65 | [75,79] |
| Effect measure reported (n = 36) | |||
| OR | 9 | 25.00 | [43,46,60,61,62,63,64,73,79] |
| RR | 17 | 47.22 | [32,33,36,37,38,39,40,41,42,47,48,49,50,53,54,55,65] |
| Coefficient | 8 | 22.22 | [35,44,45,51,52,57,58,59,80] |
| Covariates (n = 36) | |||
| Demographic | 14 | 38.89 | [43,46,47,51,52,54,57,59,60,61,64,73,75,79] |
| Socio-economical | 16 | 44.44 | [34,37,38,43,46,47,48,52,54,55,57,59,60,64,73,75] |
| Environmental | 6 | 16.67 | [37,45,60,75,79,80] |
| Clinical, health service, and behavioral related | 6 | 16.67 | [32,43,46,53,57,73] |
| Standardisation (n = 36) | |||
| No | 31 | 86.11 | [32,33,35,36,37,39,41,42,43,44,45,46,47,49,50,51,52,53,54,56,57,58,59,60,62,63,64,65,73,75,80] |
| Yes | 5 | 13.89 | [38,40,48,55,61] |
| Method to define spatial neighbourhood structure | |||
| Distance-based neighbourhood matrix | 1 | 2.33 | [34] |
| Queen contiguity | 10 | 23.26 | [45,48,50,53,54,55,60,65,72,75] |
| Rook contiguity | 2 | 4.65 | [46,52] |
| Non-specified adjacency based | 3 | 6.98 | [33,44,49] |
| Not reported | 27 | 62.79 | [32,35,36,37,38,39,40,41,42,43,47,51,56,57,58,59,61,62,63,64,73,74,76,77,78,79,80] |
| Map reported | |||
| No | 3 | 6.98 | [34,44,77] |
| Yes | 40 | 93.02 | [32,33,35,36,37,38,39,40,41,42,43,45,46,47,48,49,50,51,52,53,54,55,56,57,58,59,60,61,62,63,64,65,72,73,74,75,76,78,79,80] |
| Script provided (n = 36) | |||
| No | 31 | 86.11 | [32,33,36,37,38,39,40,41,42,43,44,45,46,47,48,49,50,51,52,55,56,57,58,59,60,61,62,64,73,75,80] |
| Yes | 5 | 13.89 | [35,53,54,63,65] |
| Items | Number | Percentage (%) | References |
|---|---|---|---|
| Reasons for using joint modelling (n = 36) | |||
| To borrow strength between diseases and to incorporate data from a more common and related disease when interest is in a relatively rare disease strengthens the relevant results of the rare disease | 9 | 25.00 | [36,37,42,44,49,53,55,60,61] |
| For ease of interpretation, and to improve the precision of estimation | 12 | 33.33 | [38,39,43,44,49,53,54,55,57,60,65,76] |
| To consider the spatial dependence of interrelated outcome variables and to better understand the overlapping epidemiology | 14 | 38.89 | [43,44,47,52,57,58,60,61,62,65,72,73,75,78] |
| To account for such unmeasured exposures that may be common among the diseases | 2 | 5.56 | [37,44] |
| For estimating the relative weight of each shared component for all related disease | 6 | 16.67 | [38,41,50,53,65,73] |
| Key findings | |||
| The joint spatial model yields more precise and efficient estimates especially when the number of desired observed cases is low | 6 | 13.95 | [33,43,60,62,73,78] |
| Found reasonable patterns in the co-occurrence in geographic prevalence across areas | 31 | 72.09 | [32,34,35,38,40,41,42,45,46,47,48,49,50,51,52,54,55,56,57,58,59,61,64,65,72,74,75,76,77,79,80] |
| They had shared risk factors. | 7 | 16.28 | [37,39,44,53,60,72,80] |
| The shared component joint spatial model had a better model fit relative to a joint spatial model without the shared component | 5 | 11.63 | [36,46,53,62,73] |
| Methodological gaps (n = 36) | |||
| A meaningful time period is required to detect the temporal effects | 4 | 11.11 | [38,41,44,80] |
| Assuming the shared and specific components as independent ignores the possibility of interactions between the true covariates | 4 | 11.11 | [38,44,62,73] |
| Edge effects | 3 | 8.33 | [36,38,77] |
| The results are biased by the Modifiable Areal Unit Problem (MAUP) | 2 | 5.56 | [48,55] |
| Aggregation of the data has the effect of introducing ecological fallacy and large geographical units of analysis may mask some information of interest. Results and efficiency may be improved by having smaller units of analysis | 7 | 19.44 | [40,47,48,49,53,65,80] |
| MCMC has a computational problems, model fitting, and convergence issues | 3 | 8.33 | [42,43,56] |
| ID | Author | Year | AaO | SaP | MS | MM | PRD | QoD | PoR | IDOR | Sum | Rating |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | Freitas et al., 2022 [75] | 2022 | 2 | 2 | 1 | 1 | 2 | 2 | 1 | 2 | 13 | High |
| 2 | Kazembe et al., 2015 [46] | 2015 | 2 | 2 | 1 | 2 | 2 | 2 | 2 | 2 | 15 | Very high |
| 3 | Kinyoki et al., 2017 [62] | 2017 | 2 | 2 | 1 | 1 | 2 | 1 | 1 | 2 | 12 | High |
| 4 | Besharati et al., 2020 [45] | 2020 | 2 | 2 | 1 | 2 | 2 | 1 | 1 | 2 | 13 | High |
| 5 | Kramer et al., 2013 [48] | 2013 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 2 | 9 | Medium |
| 6 | Law et al., 2018 [49] | 2018 | 2 | 2 | 1 | 1 | 2 | 1 | 1 | 2 | 12 | High |
| 7 | Lawson et al., 2014 [63] | 2014 | 2 | 2 | 2 | 1 | 2 | 0 | 2 | 1 | 12 | High |
| 8 | Lawson et al., 2020 [51] | 2020 | 1 | 1 | 1 | 1 | 2 | 2 | 1 | 0 | 9 | Medium |
| 9 | Mahaki et al., 2011 [38] | 2011 | 2 | 2 | 2 | 1 | 2 | 2 | 2 | 1 | 14 | Very high |
| 10 | Mahaki et al., 2018 [32] | 2018 | 2 | 2 | 1 | 1 | 2 | 1 | 2 | 1 | 12 | High |
| 11 | Nasrazadani et al., 2018 [39] | 2018 | 2 | 2 | 2 | 1 | 2 | 2 | 2 | 2 | 15 | Very high |
| 12 | Desjardins et al., 2014 [76] | 2018 | 2 | 2 | 1 | 1 | 2 | 1 | 2 | 1 | 12 | High |
| 13 | Odhiambo et al., 2021 [53] | 2021 | 2 | 2 | 2 | 2 | 2 | 1 | 2 | 2 | 15 | Very high |
| 14 | Okango et al., 2015 [54] | 2015 | 2 | 2 | 1 | 1 | 2 | 2 | 1 | 2 | 13 | High |
| 15 | Orunmoluyi et al., 2022 [64] | 2022 | 2 | 2 | 1 | 1 | 2 | 2 | 1 | 2 | 13 | High |
| 16 | Otiende et al., 2020 [65] | 2020 | 2 | 2 | 2 | 2 | 2 | 2 | 2 | 2 | 16 | Very high |
| 17 | Raei et al., 2018 [41] | 2018 | 2 | 2 | 1 | 1 | 1 | 1 | 1 | 1 | 10 | Medium |
| 18 | Ransome et al., 2019 [55] | 2019 | 2 | 2 | 1 | 1 | 1 | 2 | 1 | 1 | 11 | High |
| 19 | Roberts et al., 2020 [75] | 2020 | 2 | 2 | 2 | 2 | 2 | 2 | 2 | 2 | 16 | Very high |
| 20 | Schur et al., 2011 [78] | 2011 | 2 | 2 | 1 | 2 | 2 | 2 | 1 | 1 | 13 | High |
| 21 | Stensgaard et al., 2011 [79] | 2011 | 1 | 2 | 2 | 1 | 1 | 1 | 1 | 1 | 10 | Medium |
| 22 | Stoppa et al., 2022 [40] | 2022 | 1 | 2 | 2 | 2 | 1 | 2 | 1 | 1 | 12 | High |
| 23 | Norwood et al., 2020 [56] | 2020 | 2 | 2 | 2 | 2 | 2 | 2 | 1 | 1 | 14 | Very high |
| 24 | Adebayo et al., 2016 [57] | 2016 | 2 | 2 | 2 | 2 | 2 | 2 | 2 | 1 | 15 | Very high |
| 25 | Asmarian et al., 2019 [42] | 2019 | 2 | 2 | 1 | 2 | 2 | 1 | 1 | 1 | 12 | High |
| 26 | Huang et al., 2018 [58] | 2018 | 2 | 1 | 1 | 2 | 2 | 2 | 2 | 1 | 13 | High |
| 27 | Kang et al., 2014 [59] | 2014 | 2 | 2 | 2 | 2 | 2 | 2 | 2 | 1 | 15 | Very high |
| 28 | Law et al., 2020 [50] | 2020 | 2 | 2 | 2 | 2 | 2 | 2 | 2 | 1 | 15 | Very high |
| 29 | Roberts et al., 2022 [60] | 2022 | 2 | 2 | 1 | 2 | 2 | 1 | 1 | 1 | 12 | High |
| 30 | Carabali et al., 2022 [61] | 2022 | 2 | 2 | 2 | 2 | 1 | 2 | 1 | 1 | 13 | High |
| 31 | Cramb et al., 2015 [37] | 2015 | 2 | 2 | 2 | 2 | 2 | 2 | 1 | 1 | 14 | Very high |
| 32 | Kinyoki et al., 2017 [62] | 2017 | 2 | 2 | 1 | 1 | 2 | 1 | 1 | 1 | 11 | High |
| 33 | Kline et al., 2019 [47] | 2019 | 2 | 2 | 1 | 1 | 2 | 2 | 1 | 1 | 12 | High |
| 34 | Chidumwa et al., 2021 [73] | 2021 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 8 | Medium |
| 35 | Adeyemi et al., 2019 [43] | 2019 | 2 | 2 | 1 | 1 | 2 | 2 | 1 | 1 | 12 | High |
| 36 | Darikwa et al., 2019 [74] | 2019 | 2 | 2 | 1 | 1 | 2 | 2 | 1 | 1 | 12 | High |
| 37 | Darikwa et al., 2020 [51] | 2020 | 1 | 2 | 1 | 1 | 1 | 1 | 1 | 1 | 9 | Medium |
| 38 | Chamanpara et al., 2015 [36] | 2015 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 8 | Medium |
| 39 | Carroll et al., 2017 [35] | 2017 | 2 | 2 | 1 | 1 | 1 | 1 | 1 | 1 | 10 | Medium |
| 40 | Adegboye et al., 2017 [80] | 2017 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 8 | Medium |
| 41 | Neelon et al., 2014 [52] | 2014 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 8 | Medium |
| 42 | Ahmadipanahmehrabadi et al., 2019 [33] | 2019 | 2 | 2 | 1 | 2 | 2 | 2 | 1 | 1 | 13 | High |
| 43 | Bermudi et al., 2020 [34] | 2020 | 2 | 2 | 2 | 2 | 2 | 2 | 2 | 2 | 16 | Very high |
| Range | 1–2 | 1–2 | 1–2 | 1–2 | 1–2 | 0–2 | 1–2 | 0–2 | 8–16 | |||
| Median score | 2 | 2 | 1 | 1 | 2 | 2 | 1 | 1 | 12 | High | ||
| Mean score | 1.79 | 1.84 | 1.35 | 1.42 | 1.72 | 1.53 | 1.33 | 1.28 | 12.26 | |||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tesema, G.A.; Tessema, Z.T.; Heritier, S.; Stirling, R.G.; Earnest, A. A Systematic Review of Joint Spatial and Spatiotemporal Models in Health Research. Int. J. Environ. Res. Public Health 2023, 20, 5295. https://doi.org/10.3390/ijerph20075295
Tesema GA, Tessema ZT, Heritier S, Stirling RG, Earnest A. A Systematic Review of Joint Spatial and Spatiotemporal Models in Health Research. International Journal of Environmental Research and Public Health. 2023; 20(7):5295. https://doi.org/10.3390/ijerph20075295
Chicago/Turabian StyleTesema, Getayeneh Antehunegn, Zemenu Tadesse Tessema, Stephane Heritier, Rob G. Stirling, and Arul Earnest. 2023. "A Systematic Review of Joint Spatial and Spatiotemporal Models in Health Research" International Journal of Environmental Research and Public Health 20, no. 7: 5295. https://doi.org/10.3390/ijerph20075295