
Fluorescent Marker as a Tool to Improve Strategies to Control Contaminated Surfaces and Decrease Danger of Cross-Contamination in Dental Clinics, during and beyond the COVID-19 Pandemic

Abstract
:1. Introduction
2. Materials and Methods
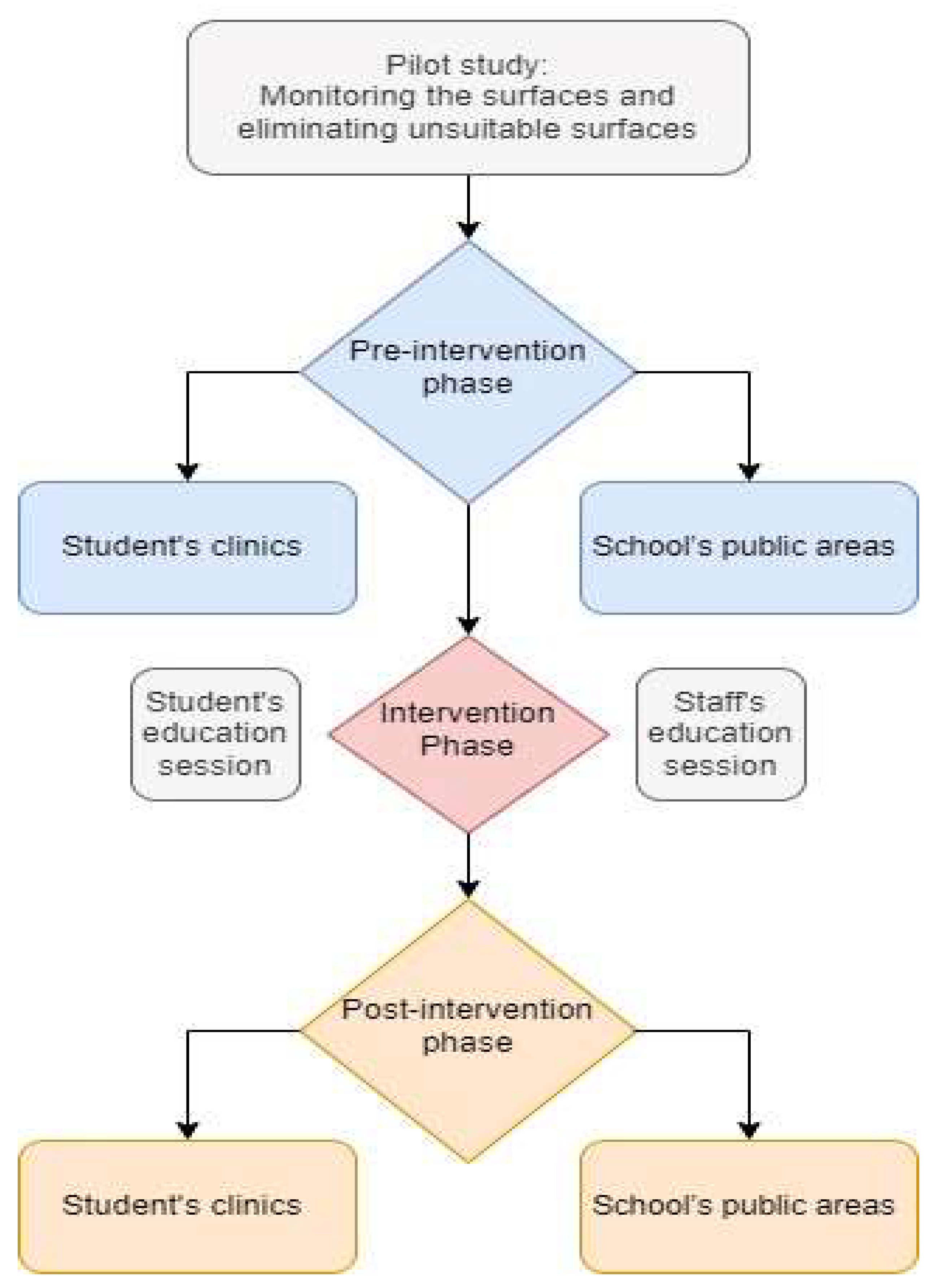
2.1. Study Design (Figure 1)

2.2. Evaluation of Surface Cleanliness
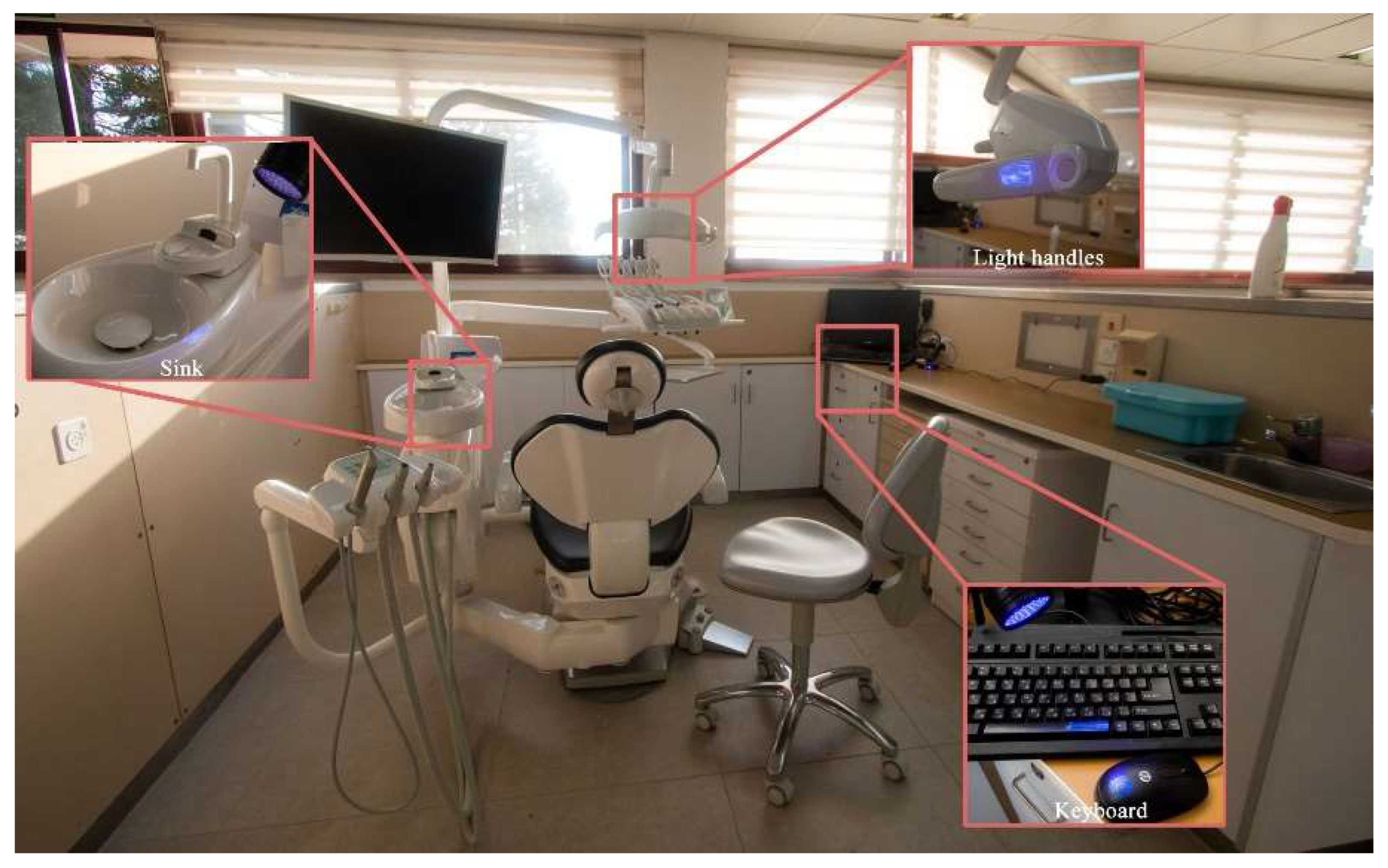
2.3. Surfaces Examined
2.3.1. Students’ Working Areas
2.3.2. Public Areas
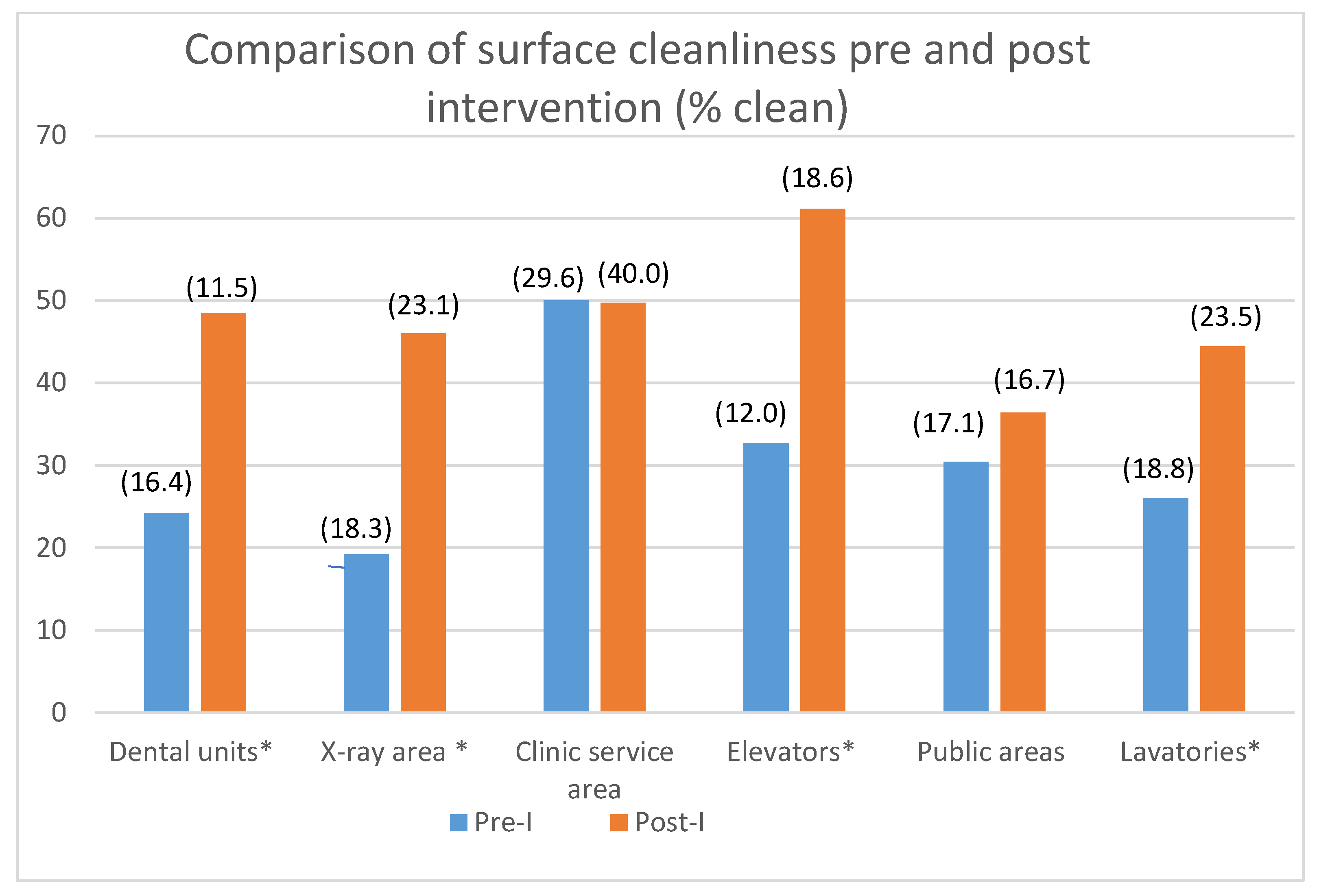
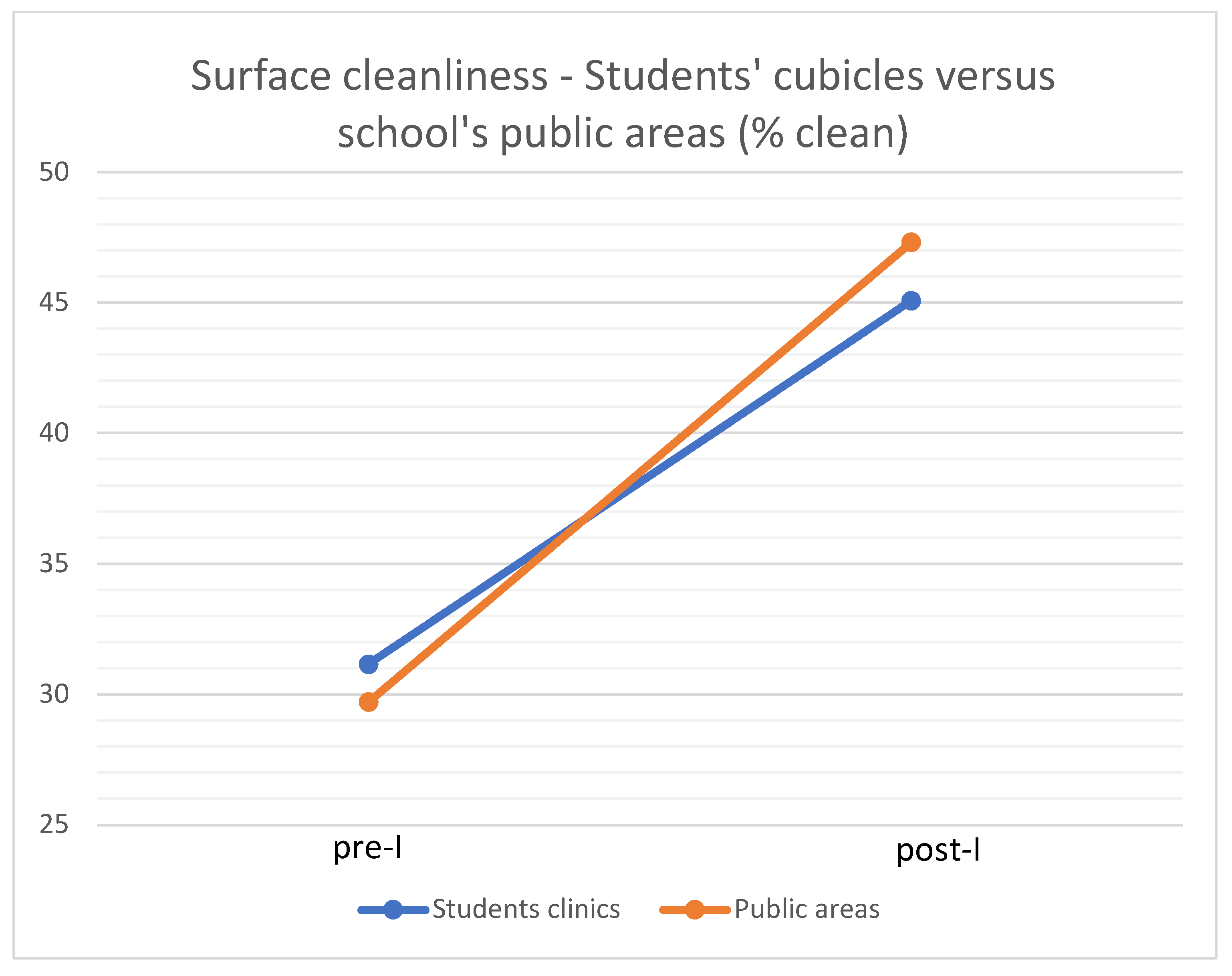
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Filip, R.; Gheorghita Puscaselu, R.; Anchidin-Norocel, L.; Dimian, M.; Savage, W.K. Global Challenges to Public Health Care Systems during the COVID-19 Pandemic: A Review of Pandemic Measures and Problems. J. Pers. Med. 2022, 12, 1295. [Google Scholar] [CrossRef] [PubMed]
- Mijiritsky, E.; Hamama-Raz, Y.; Liu, F.; Datarkar, A.N.; Mangani, L.; Caplan, J.; Shacham, A.; Kolerman, R.; Mijiritsky, O.; Ben-Ezra, M.; et al. Subjective Overload and Psychological Distress among Dentists during COVID-19. Int. J. Environ. Res. Public Health 2020, 17, 5074. [Google Scholar] [CrossRef] [PubMed]
- Meng, L.; Hua, F.; Bian, Z. Coronavirus Disease 2019 (COVID-19): Emerging and Future Challenges for Dental and Oral Medicine. J. Dent. Res. 2020, 99, 481–487. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Consolo, U.; Bellini, P.; Bencivenni, D.; Iani, C.; Checchi, V. Epidemiological Aspects and Psychological Reactions to COVID-19 of Dental Practitioners in the Northern Italy Districts of Modena and Reggio Emilia. Int. J. Environ. Res. Public Health 2020, 17, 3459. [Google Scholar] [CrossRef]
- Zhou, P.; Yang, X.L.; Wang, X.G.; Hu, B.; Zhang, L.; Zhang, W.; Si, H.R.; Zhu, Y.; Li, B.; Huang, C.L.; et al. A pneumonia outbreak associated with a new coronavirus of probable bat origin. Nature 2020, 579, 270–273. [Google Scholar] [CrossRef] [Green Version]
- Chen, Y.; Li, L. SARS-CoV-2: Virus dynamics and host response. Lancet Infect. Dis. 2020, 20, 515–516. [Google Scholar] [CrossRef] [Green Version]
- Wu, Y.; Ho, W.; Huang, Y.; Jin, D.Y.; Li, S.; Liu, S.L.; Liu, X.; Qiu, J.; Sang, Y.; Wang, Q.; et al. SARS-CoV-2 is an appropriate name for the new coronavirus. Lancet 2020, 395, 949–950. [Google Scholar] [CrossRef]
- Transmission of SARS-CoV-2: Implications for Infection Prevention Precautions. Available online: https://www.who.int/news-room/commentaries/detail/transmission-of-sars-cov-2-implications-for-infection-prevention-precautions (accessed on 4 March 2023).
- Asadi, S.; Wexler, A.S.; Cappa, C.D.; Barreda, S.; Bouvier, N.M.; Ristenpart, W.D. Aerosol emission and super emission during human speech increase with voice loudness. Sci. Rep. 2019, 9, 2348. [Google Scholar] [CrossRef] [Green Version]
- Uziel, N.; Gilon, E.; Meyerson, J.; Levin, L.; Khehra, A.; Emodi-Perlman, A.; Eli, I. Dental personnel in Israel, Canada, and France during the COVID-19 pandemic attitudes, worries, emotional responses, and posttraumatic growth. Quintessence Int. 2021, 52, 444–453. [Google Scholar] [CrossRef]
- Tang, J.W.; Tellier, R.; Li, Y. Hypothesis: All respiratory viruses (including SARS-CoV-2) are aerosol-transmitted. Indoor Air. 2022, 32, e12937. [Google Scholar] [CrossRef]
- Johnson, T.J.; Nishida, R.T.; Sonpar, A.P.; Lin, Y.J.; Watson, K.A.; Smith, S.W.; Conly, J.M.; Evans, D.H.; Olfert, J.S. Viral load of SARS-CoV-2 in droplets and bioaerosols directly captured during breathing, speaking and coughing. Sci. Rep. 2022, 12, 3484. [Google Scholar] [CrossRef] [PubMed]
- Gonçalves, J.; da Silva, P.G.; Reis, L.; Nascimento, M.S.J.; Koritnik, T.; Paragi, M.; Mesquita, J.R. Surface contamination with SARS-CoV-2: A systematic review. Sci. Total Environ. 2021, 798, 149231. [Google Scholar] [CrossRef] [PubMed]
- Weber, D.J.; Anderson, D.; Rutala, W.A. The role of the surface environment in healthcare-associated infections. Curr. Opin. Infect Dis. 2013, 26, 338–344. [Google Scholar] [CrossRef] [PubMed]
- The Australian Dental Association. ADA Environmental Cleaning and Disinfection Guidance for Dental Practitioners in the Context of COVID-19. Available online: https://www.ada.org.au/getdoc/933d1c88-fbe3-46b5-8ec1-0508b0757b4f/Card-Group-Selection.aspx (accessed on 21 January 2023).
- Sohrabi, C.; Alsafi, Z.; O’Neill, N.; Khan, M.; Kerwan, A.; Al-Jabir, A.; Iosifidis, C.; Agha, R. World Health Organization declares global emergency: A review of the 2019 novel coronavirus (COVID-19). Int. J. Surg. 2020, 76, 71–76. [Google Scholar] [CrossRef]
- Burki, T. Understanding variants of SARS-CoV-2. Lancet 2021, 397, 462. [Google Scholar] [CrossRef]
- Centers for Disease Control and Prevention. Summary of Infection Prevention Practices in Dental Settings: Basic Expectations for Safe Care. Available online: https://www.cdc.gov/oralhealth/infectioncontrol/pdf/safe-care2.pdf (accessed on 21 January 2023).
- Noura, A.A.; Manal, A.A. To what extent do dental students comply with infection control practices? Saudi J. Dent. Res. 2017, 8, 67–72. [Google Scholar] [CrossRef] [Green Version]
- Bracher, L.; Kulik, E.M.; Waltimo, T.; Turp, J.C. Surface microbial contamination in a dental department. A 10-year retrospective analysis. Swiss Dent. J. 2019, 129, 14–21. [Google Scholar]
- Kampf, G.; Todt, D.; Pfaender, S.; Steinmann, E. Persistence of coronaviruses on inanimate surfaces and their inactivation with biocidal agents. J. Hosp. Infect 2020, 104, 246–251. [Google Scholar] [CrossRef] [Green Version]
- Mathur, P. Infection Control in Operating Rooms: Sterilization and Disinfection Practices. In Textbook of Neuroanesthesia and Neurocritical Care; Prabhakar, H., Ali, Z., Eds.; Springer: Singapore, 2019; pp. 351–358. [Google Scholar] [CrossRef]
- Tan, H.; Wong, K.Y.; Nyakuma, B.B.; Kamar, H.M.; Chong, W.T.; Wong, S.L.; Kang, H.S. Systematic study on the relationship between particulate matter and microbial counts in hospital operating rooms. Environ. Sci. Pollut. Res. Int. 2022, 29, 6710–6721. [Google Scholar] [CrossRef]
- Carling, P. Methods for assessing the adequacy of practice and improving room disinfection. Am. J. Infect Control 2013, 41 (Suppl. Sl), S20–S25. [Google Scholar] [CrossRef]
- Drew, J.L.; Turner, J.; Mugele, J.; Hasty, G.; Duncan, T.; Zaiser, R.; Cooper, D. Beating the Spread: Developing a Simulation Analog for Contagious Body Fluids. Simul. Healthc. 2016, 11, 100–105. [Google Scholar] [CrossRef] [PubMed]
- Why Use a Fluorescent Marker? Available online: https://www.bio-rad-antibodies.com/flow-cytometry-why-use-a-fluorescent-probe.html (accessed on 1 March 2023).
- Flynn, T.G.; Dunaway, C.M.; LaRochelle, E.; Lyons, K.; Kennedy, L.S.; Romano, M.E.; Li, Z.; Spaller, M.R.; Cervinski, M.A.; Bejarano, S.; et al. Reducing dermal exposure to agrochemical carcinogens using a fluorescent dye-based intervention among subsistence farmers in rural Honduras. Int. J. Hyg. Environ. Health 2021, 234, 113734. [Google Scholar] [CrossRef] [PubMed]
- Maki, D.G.; Alvarado, C.J.; Hassemer, C.A.; Zilz, M.A. Relation of the inanimate hospital environment to endemic nosocomial infection. N. Engl. J. Med. 1982, 307, 1562–1566. [Google Scholar] [CrossRef] [PubMed]
- Gerba, C.P.; Lopez, G.U.; Ikner, L. A Distribution of Bacteria in Dental Offices and the Impact of Hydrogen Peroxide Disinfecting Wipes. J. Dent. Hyg. 2016, 90, 354–361. [Google Scholar]
- American Hospital Association. CDC Updates COVID-19 Infection Control Guidance for Health Care Settings. Available online: https://www.aha.org/news/headline/2022-09-26-cdc-updates-covid-19-infection-control-guidance-health-care-settings (accessed on 14 February 2023).
- Dewangan, A.; Gaikwad, U. Comparative evaluation of a novel fluorescent marker and environmental surface cultures to assess the efficacy of environmental cleaning practices at a tertiary care hospital. J. Hosp. Infect. 2020, 104, 261–268. [Google Scholar] [CrossRef]
- Trajtman, A.N.; Manickam, K.; Macrae, M.; Bruning, N.S.; Alfa, M.J. Continuing performance feedback and use of the ultraviolet visible marker to assess cleaning compliance in the healthcare environment. J. Hosp. Infect. 2013, 84, 166–172. [Google Scholar] [CrossRef]
- Rock, C.; Xie, A.; Andonian, J.; Hsu, Y.-J.; Osei, P.; Keller, S.C.; Gurses, A.P.; Trexler, P.; Maragakis, L.L.; Cosgrove, S.E.; et al. Evaluation of environmental cleaning of patient rooms: Impact of different fluorescent gel markers. Infect. Control Hosp. Epidemiol. 2019, 40, 100–102. [Google Scholar] [CrossRef]
- Ceriale, E.; Fattorini, M.; Lenzi, D.; Manzi, P.; Basagni, C.; Nante, N.; Messina, G. Use of a fluorescent marker for assessing hospital cleanliness. Eur. J. Public Health 2015, 25, ckv172.047. [Google Scholar] [CrossRef] [Green Version]
- Foss, C.R.; Allen, E.H.; Fenske, R.A.; Ramsay, C.A. Comparison of live skit and video delivery styles using presentations with and without fluorescent tracer dyes at pesticide applicator training for promotion of self-protection from dermal exposure. J. Pestic. Saf. Educ. 2002, 4, 1–9. [Google Scholar]
- Kohn, W.G.; Collins, A.S.; Cleveland, J.L.; Harte, J.A.; Eklund, K.J.; Malvitz, D.M. Centers for Disease, C. Prevention. Guidelines for infection control in dental health-care settings–2003. MMWR Recomm. Rep. 2003, 52, 1–61. [Google Scholar]
- Freire, D.N.; Pordeus, I.A.; Paixao, H.H. Observing the behavior of senior dental students in relation to infection control practices. J. Dent. Educ. 2000, 64, 352–356. [Google Scholar] [CrossRef] [PubMed]
- McCarthy, G.M.; Britton, J.E. A Survey of Final-Year Dental, Medical and Nursing Students: Occupational Injuries and Infection Control. J. Can Dent. Assoc. 2000, 66, 561. [Google Scholar] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Cleanliness (%) | Pre-I * | Post-I | ANOVA-F(1) | p *** | |
|---|---|---|---|---|---|
| Surface Category | |||||
| Students’ cubicles (n = 13) ** | 24.24 ± 16.14 | 48.48 ± 11.53 | 12.41 | 0.003 | |
| X-ray areas (n = 9) | 19.23 ± 18.33 | 46.03 ± 23.17 | 10.03 | 0.006 | |
| Clinic service areas (n = 3) | 50.00 ± 29.65 | 49.74 ± 40.06 | NS | NS | |
| Elevators (n = 4) | 32.69 ± 12.00 | 61.11 ± 18.16 | 19.192 | 0.000 | |
| Public areas (n = 10) | 30.42 ± 17.16 | 36.41 ± 16.76 | NS | NS | |
| Lavatories (n = 9) | 26.02 ± 18.87 | 44.44 ± 23.57 | 3.717 | 0.072 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dolev, E.; Eli, I.; Mashkit, E.; Grinberg, N.; Emodi-Perlman, A. Fluorescent Marker as a Tool to Improve Strategies to Control Contaminated Surfaces and Decrease Danger of Cross-Contamination in Dental Clinics, during and beyond the COVID-19 Pandemic. Int. J. Environ. Res. Public Health 2023, 20, 5229. https://doi.org/10.3390/ijerph20065229
Dolev E, Eli I, Mashkit E, Grinberg N, Emodi-Perlman A. Fluorescent Marker as a Tool to Improve Strategies to Control Contaminated Surfaces and Decrease Danger of Cross-Contamination in Dental Clinics, during and beyond the COVID-19 Pandemic. International Journal of Environmental Research and Public Health. 2023; 20(6):5229. https://doi.org/10.3390/ijerph20065229
Chicago/Turabian StyleDolev, Eran, Ilana Eli, Ester Mashkit, Naftali Grinberg, and Alona Emodi-Perlman. 2023. "Fluorescent Marker as a Tool to Improve Strategies to Control Contaminated Surfaces and Decrease Danger of Cross-Contamination in Dental Clinics, during and beyond the COVID-19 Pandemic" International Journal of Environmental Research and Public Health 20, no. 6: 5229. https://doi.org/10.3390/ijerph20065229