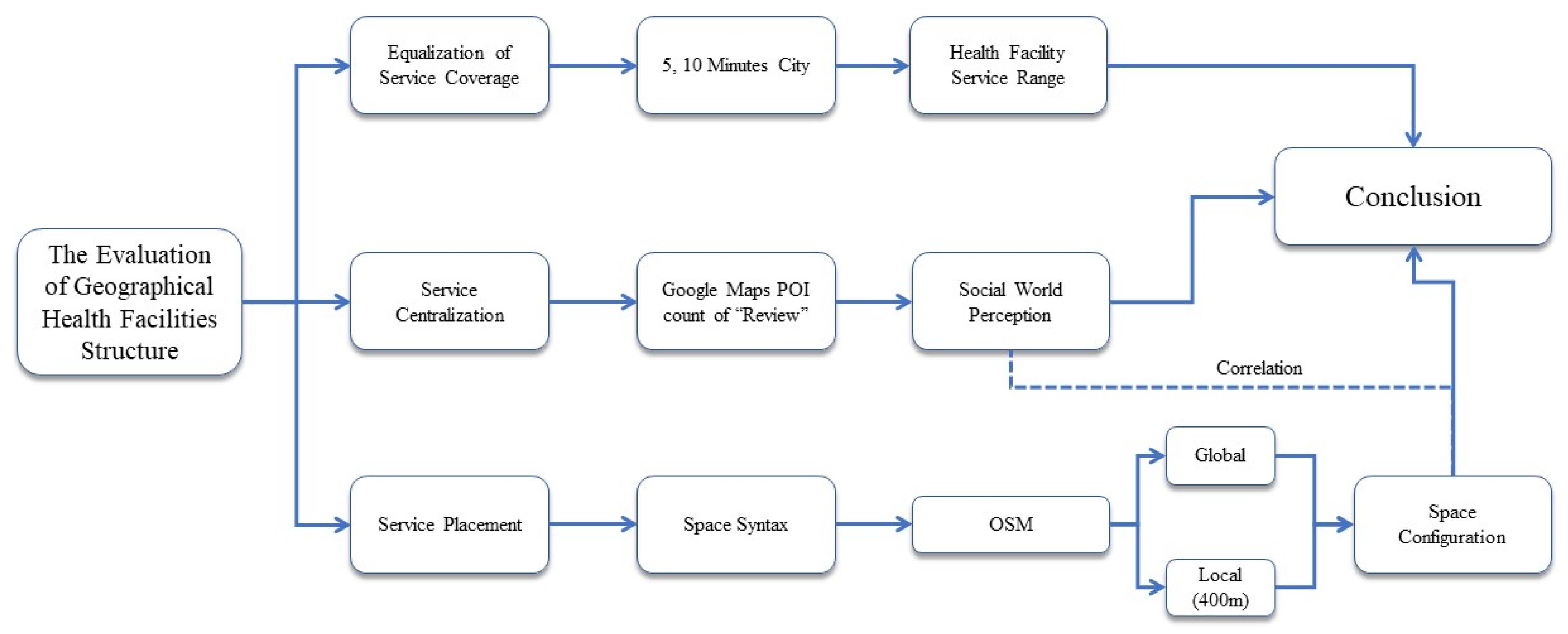
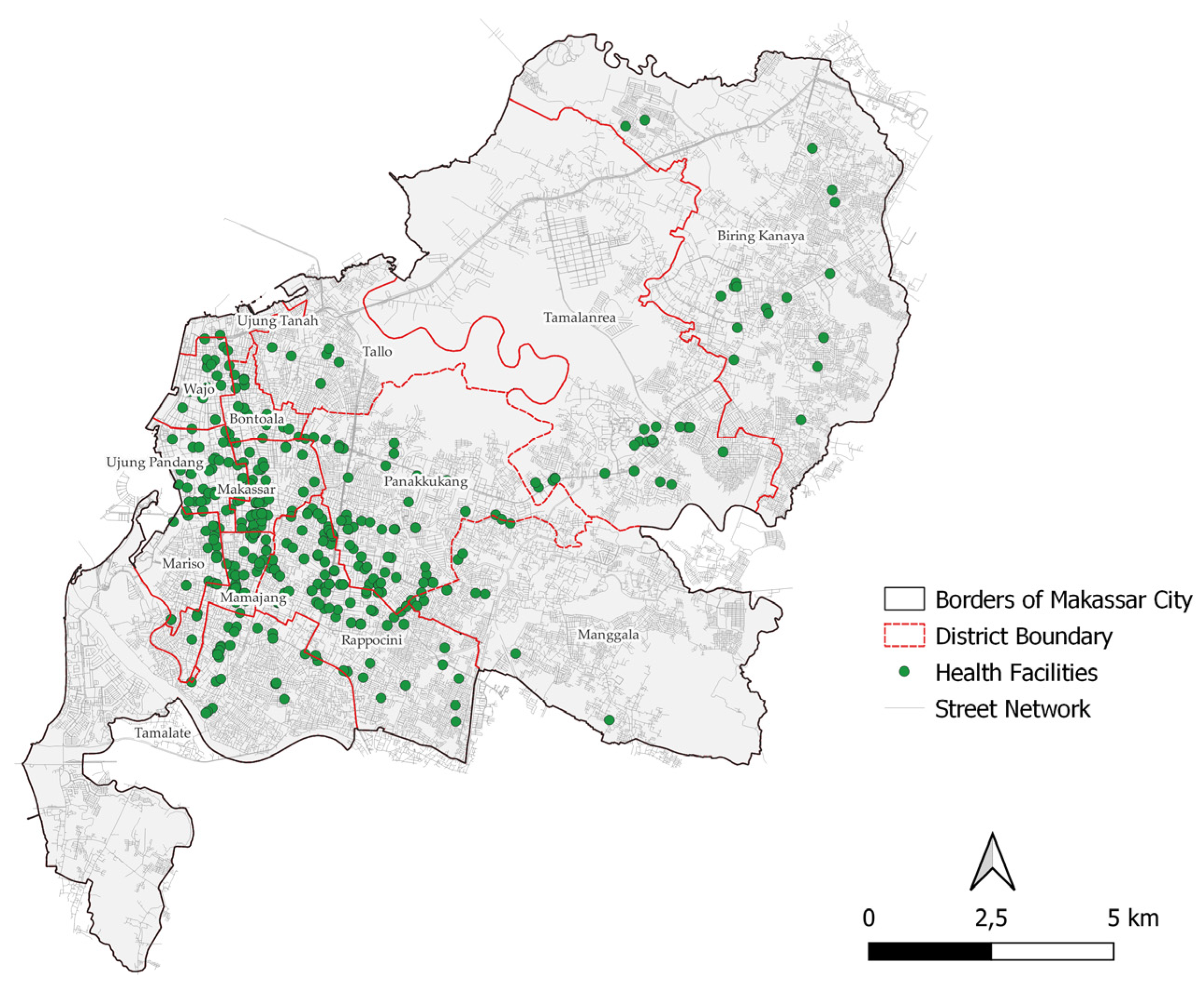
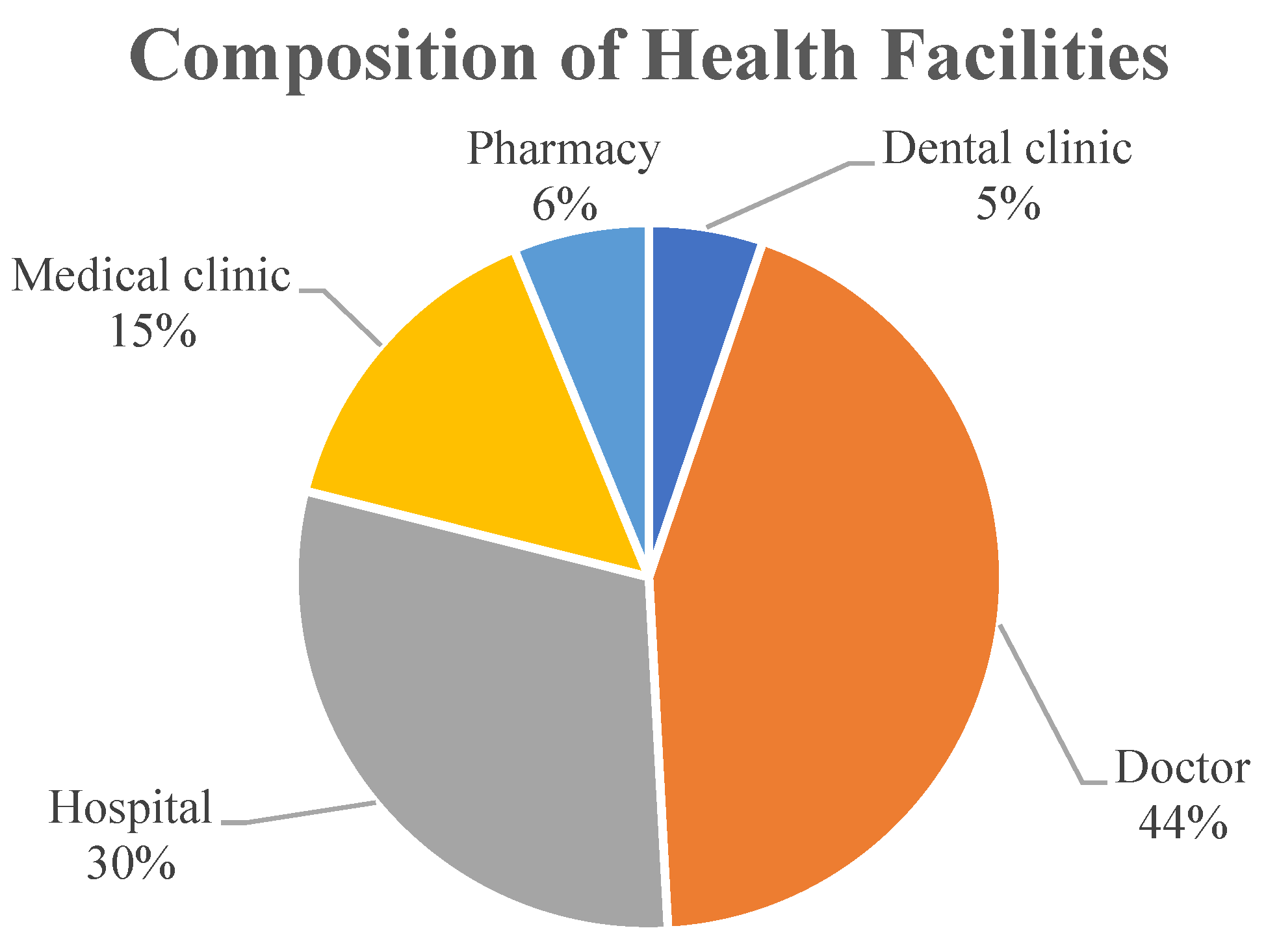
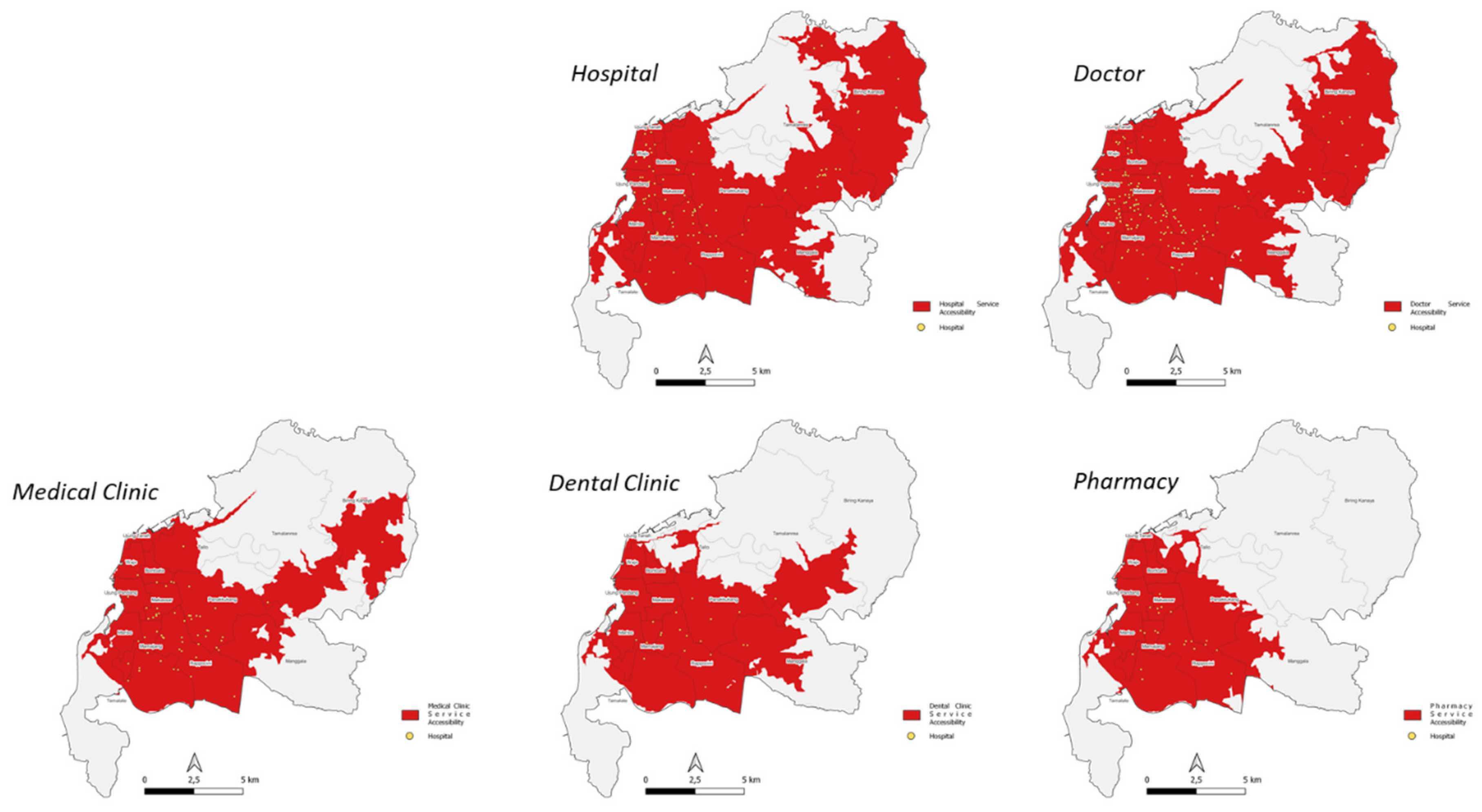
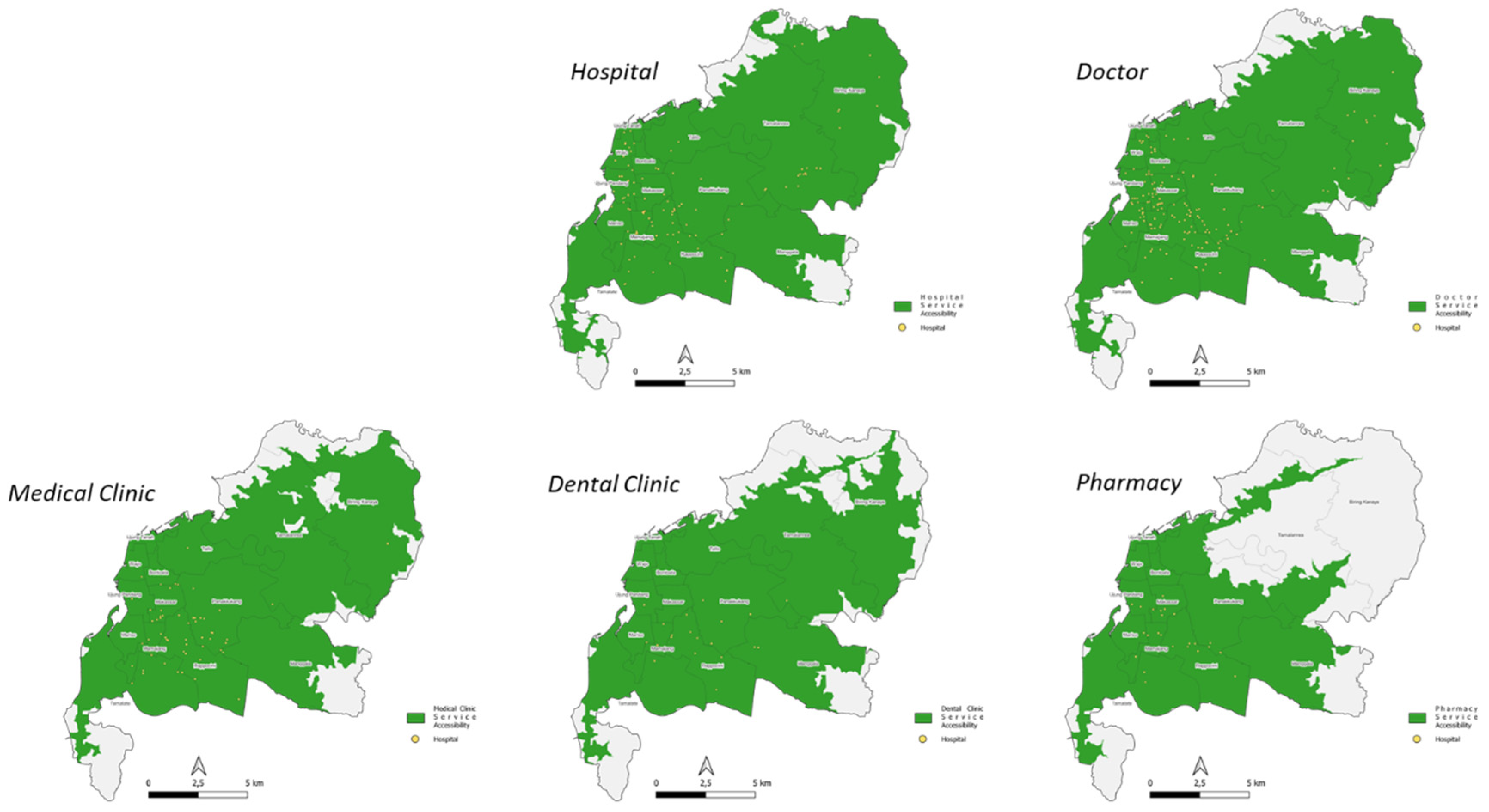
Data preparation was done first, before proceeding to the next process. As discussed in the previous chapter, this study focuses on the geographic evaluation of a healthcare facility, where we will look at the Equalization of Service Coverage, Service Centralization, and Service Placement of healthcare facilities in a region. The administrative district area of kecamatan in Makassar City was obtained from GADM.org data. This administrative area was used to assess the level of equity. To obtain healthcare facilities according to the kecamatan administrative boundary, a zonal statistic process was conducted in QGIS. Healthcare facilities in Makassar city were obtained from Google POI using the keyword “health facility”. The results of this collection were then sorted by facility type and grouped into five major categories: Dental Clinic, Doctor, Hospital, Medical Clinic, and Pharmacy. User-generated review data were not removed and used as the basis for digital world perception of the facilities in question. Road network data, used as the basis for network analysis and spatial configuration analysis, were obtained from OSM. After all the data were obtained and processed, an analysis process was carried out, which will be explained in the following sub-chapter.
4.3. Centralized Facility Services
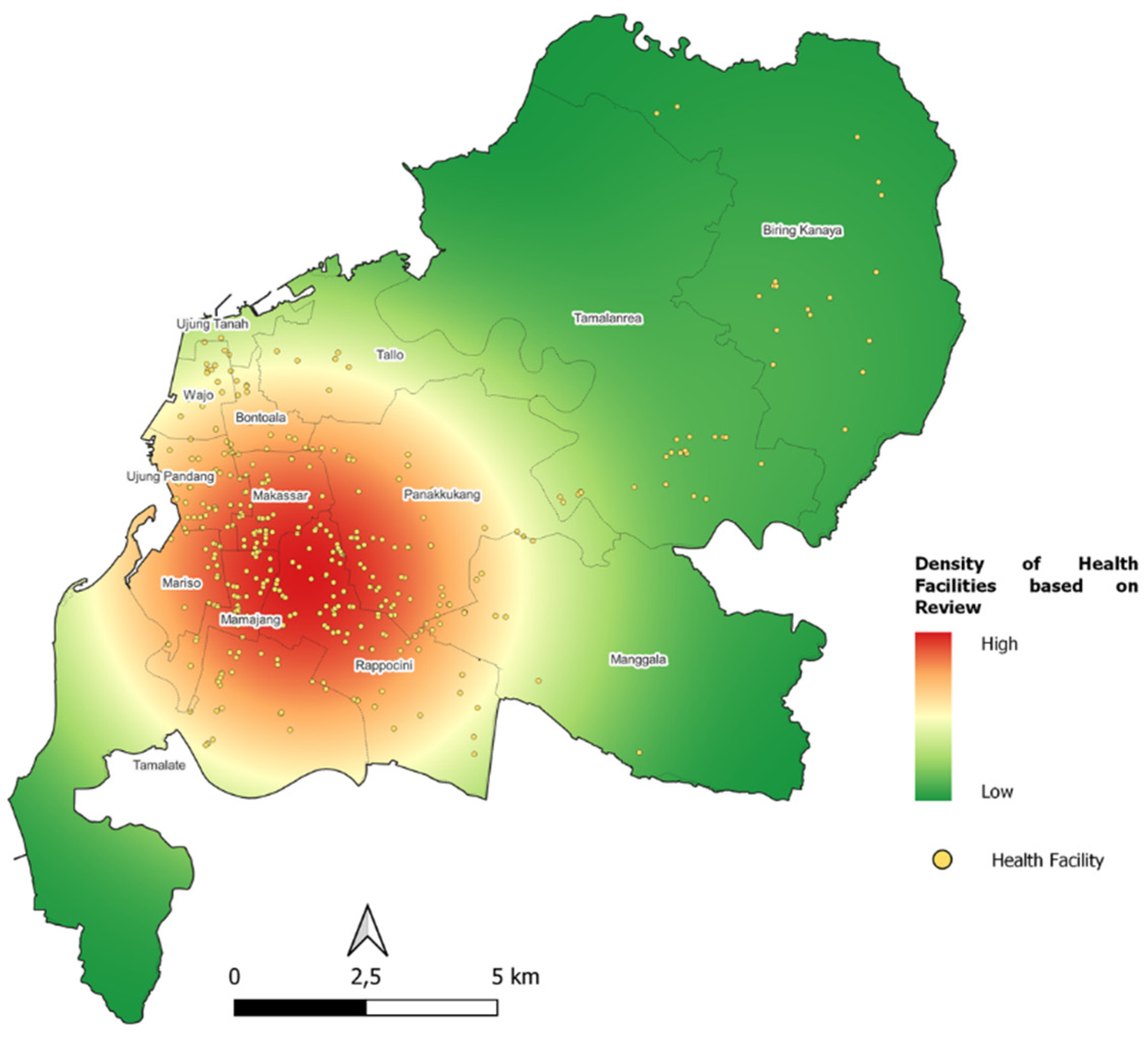
To obtain an evaluation of Service Centralization, the analysis used is the point density analysis with the weight of “reviews” from Google Maps POI. Unlike the geographic analysis commonly used by researchers, which uses point density without any weight of whether a facility is attractive and visited frequently, the method of using “reviews” weight from Google Maps POI can provide a more realistic picture and can solve the difficulty of obtaining service data in a region.
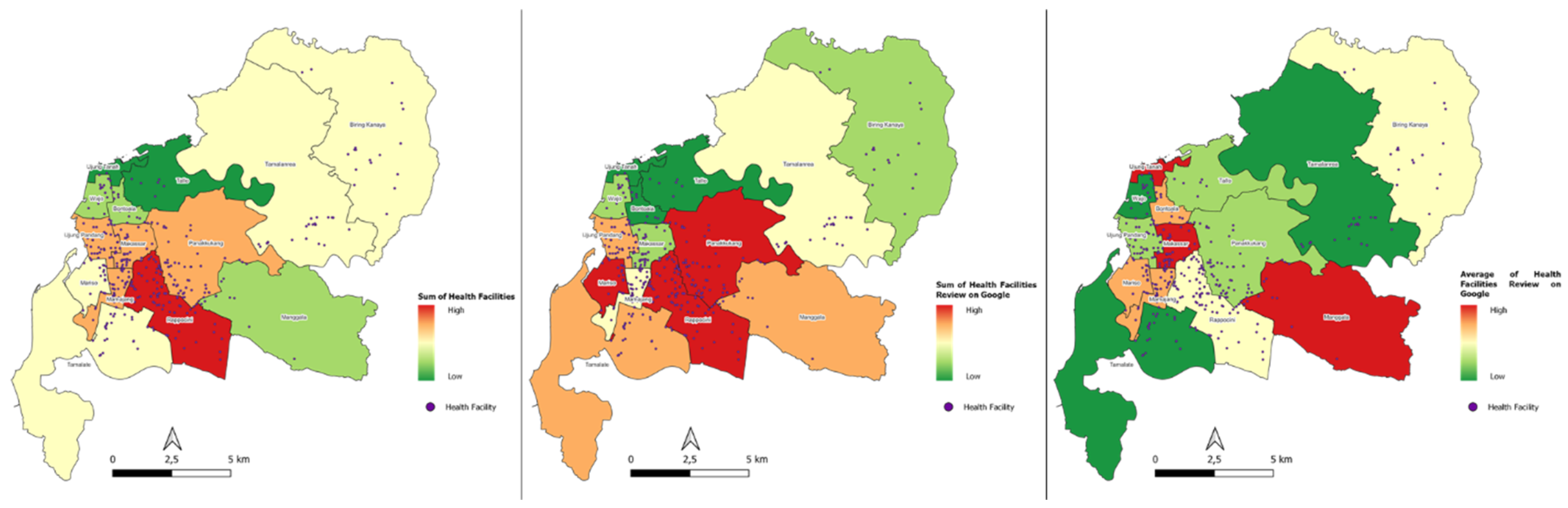
The first step was to find where the centralization is according to the kecamatan in Makassar City. This method was done by conducting zonal statistics of the number of healthcare facilities into kecamatan/districts. The division according to natural breaks (jenk) is carried out to obtain a visualization of high to low.
Centralization of the highest health facilities is in
kecamatan Rappocini. Google’s highest POI review in aggregate is in
kecamatan Panakkukang,
kecamatan Rappocini, and
kecamatan Mariso. Meanwhile the average Google POI rating is the highest in aggregate in
kecamatan Manggala,
kecamatan Makassar, and
kecamatan Ujung Tanah (
Figure 7).
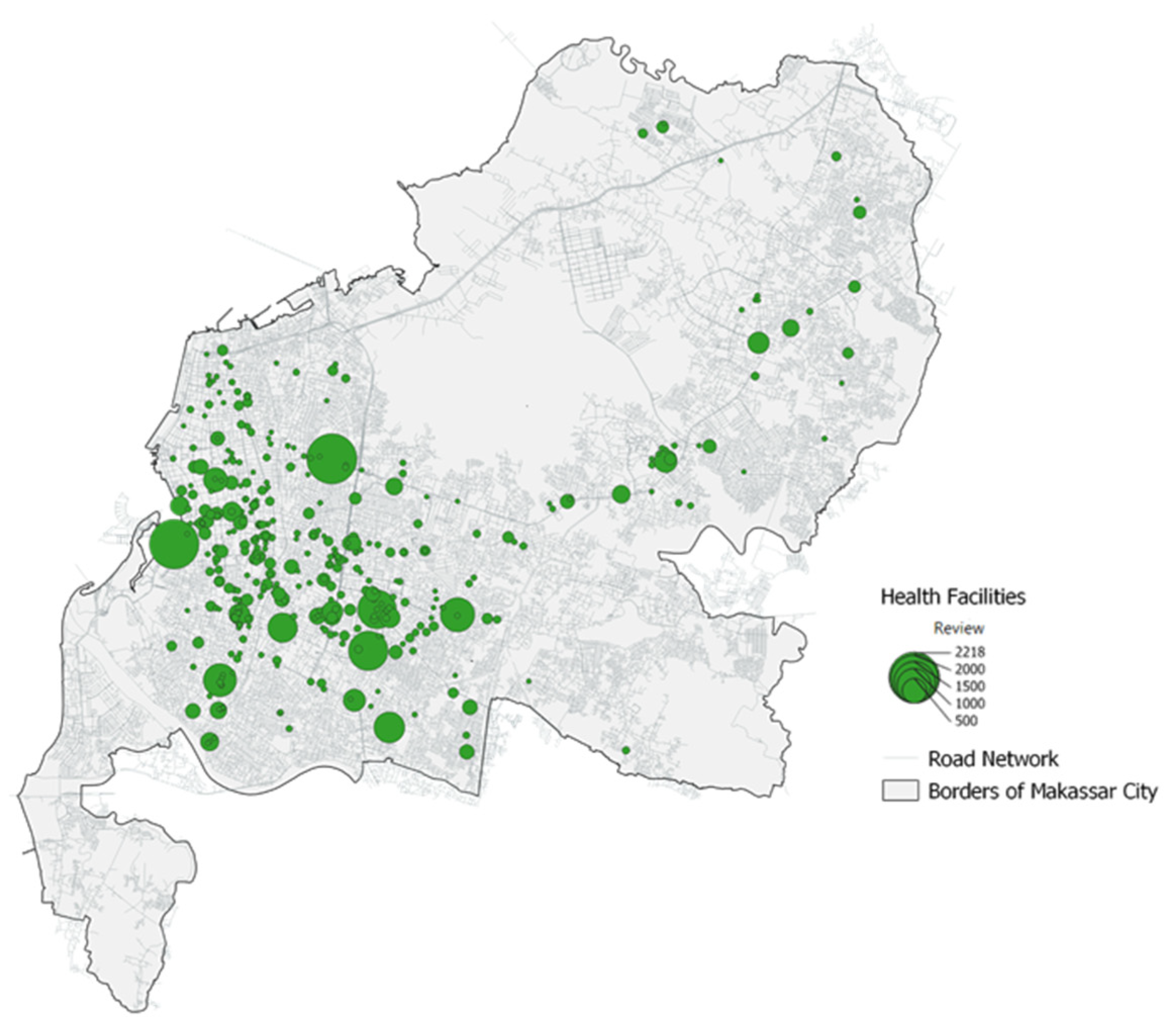
The second step was to calculate how centralization is according to its “reviews” weight through kernel density analysis. The result of this analysis is the area (raster) where the centralization of healthcare facilities is located. This visualization can be used as a basis for future planning to determine whether a new healthcare facility needs to be built on the suburb of the city or in other settlement centres. Another advantage that can be gained is that we can evaluate how people rate each facility, where it is conveyed in the range of 0–5 on Google Maps POI.
Social media perception of the highest number of Google POI reviews is hospital by 60% and the lowest is pharmacy by 2%. Meanwhile, from the average Google POI rating, the highest is a dental clinic at 23% and the lowest is a hospital at 17% (
Table 7,
Figure 8 and
Figure 9).
4.4. Facility Placement Evaluation
Space configuration is the arrangement of space and its components, including buildings, roads, and public spaces. It is an important aspect of urban planning and design that can impact how people interact with their environment.
One method for analyzing space configuration is space syntax. Space syntax is a technique used to analyze the spatial properties of urban environments by measuring the accessibility, connectivity, and visibility of different spaces. It uses graph theory to model the spatial relationships between different spaces and identify the underlying patterns of movement and interaction. The space syntax approach involves mapping the urban environment into a graph-based representation of the street network. This representation is then analyzed using a set of metrics that capture different aspects of spatial configuration, such as the degree of connectivity, the level of integration, and the centrality of different spaces. These metrics can be used to identify areas of the urban environment that are more or less accessible, connected, or visible, and to determine how these properties affect pedestrian movement, social interaction, and other urban phenomena. By using space syntax, planners and designers can gain insights into the spatial properties of urban environments and develop strategies for improving accessibility, connectivity, and visibility. This can include interventions such as reconfiguring street networks, enhancing pedestrian routes, and creating more open and visible public spaces. Ultimately, the goal of space syntax is to create more livable, sustainable, and equitable urban environments that support the needs and aspirations of all residents.
Space syntax analysis can be used to identify the most central and accessible locations for healthcare facilities, based on factors such as the degree of connectivity to surrounding streets and the level of integration with other urban spaces. This analysis can also help identify areas of the city that are underserved by healthcare facilities and need new facilities to be established. In addition, space syntax can be used to evaluate the impact of health facility placement on urban mobility and accessibility. For instance, it can help identify pedestrian routes that are obstructed or poorly connected to healthcare facilities, and suggest interventions such as creating new pedestrian paths or improving existing ones to enhance mobility and accessibility. Overall, space syntax analysis is a useful tool for evaluating health facility placement and improving access to healthcare services in urban areas.
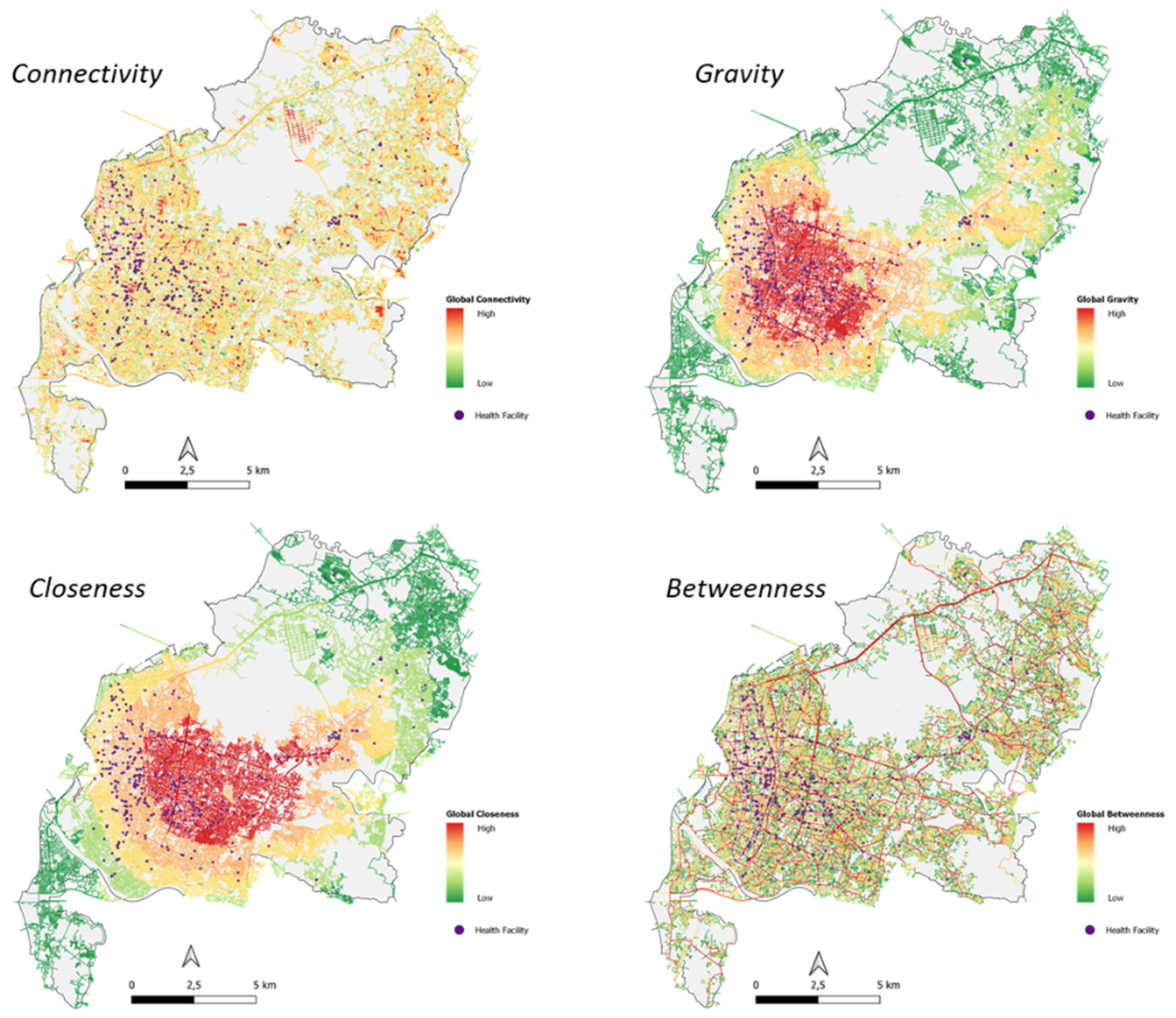
The algorithm produced by space syntax is a mathematical model that uses graph theory to analyze spatial configurations and their impact on urban mobility and accessibility. The algorithm calculates a set of metrics that capture different aspects of spatial configuration, such as the degree of connectivity, the level of integration, and the centrality of different spaces. The main concept behind the space syntax algorithm is that spatial configurations influence the way people move and interact in urban environments. By analyzing the spatial relationships between different spaces, the algorithm can identify patterns of movement and interaction and evaluate how these patterns are affected by changes in the spatial configuration. The algorithm produces a range of metrics, each of which provides insights into different aspects of spatial configuration. These metrics include:
Closeness: This measures the extent to which a space is connected to other spaces in the urban network.
Betweenness: This measures the number of alternative paths that can be taken to reach a particular space.
Gravity: This measures the degree to which a space is strategically located within the urban network.
Connectivity: This measures the importance of a space in terms of its position within the network.
By analyzing these metrics, the space syntax algorithm can identify the most important spaces in the urban network, such as central locations that are well-connected and highly visible. It can also identify areas that are underserved by urban amenities, such as health facilities, and suggest interventions to improve access and mobility.
In space syntax analysis, global configuration refers to the overall spatial structure and organization of an urban environment, while local configuration refers to the immediate surroundings of a specific location or space. The global configuration of an urban environment is analyzed using metrics such as the degree of connectivity, the level of integration, and the centrality of different spaces. These metrics capture the overall structure and organization of the urban network and can help identify important spatial features such as the most central locations or the most well-connected areas of the city.
On the other hand, local configuration refers to the immediate surroundings of a particular location or space, typically within a radius of 400 m. The analysis of local configuration can help identify how a specific location is connected to its immediate surroundings and how this affects movement and accessibility. For example, local configuration analysis can help identify pedestrian paths that are obstructed or poorly connected to surrounding areas, as well as areas that are underserved by urban amenities such as health facilities. This information can be used to suggest interventions such as creating new pedestrian paths, improving existing ones, or establishing new health facilities in underserved areas.
Overall, the analysis of both global and local configuration is important for understanding the spatial properties of urban environments and their impact on mobility and accessibility. by using metrics such as connectivity, integration, and centrality, space syntax analysis can help identify areas of the city that need improvement and suggest interventions to enhance mobility and accessibility for all residents. Global Spatial Configuration
4.4.1. Global Spatial Configuration
In a global spatial review, the highest connectivity value was identified in medical clinics and the lowest in hospitals. The highest closeness value was identified in dental clinics and the lowest at hospitals. The highest gravity value was identified in pharmacies and the lowest in hospitals. The highest value of betweenness was identified at dental clinics and the lowest at the hospitals (
Table 8,
Figure 10).
The highest correlation between the number of reviews and global spatial configuration is in the gravity algorithm, which shows that the closer the facility to the centre of the city road network, the higher the number of reviews (public perception).
The highest correlation between the average rating and global spatial configuration is in the closeness algorithm, which shows that the closer the facility to the centre of the city road network, the higher the rating given (
Table 9).
4.4.2. 400-m Radius Area Configuration
In a review of the 400-m radius, the highest connectivity value was identified in medical clinics and the lowest in hospitals. The highest closeness value was identified in hospitals and the lowest in doctors. The highest gravity value was identified in pharmacies and the lowest in dental clinics. The highest value of betweenness was identified in medical clinics and the lowest in hospitals (
Table 10,
Figure 11).
The highest correlation between the number of reviews and the configuration of the 400-m radius area is in the connectivity and betweenness algorithm, which shows that the closer the facility to the centre of the local network and those on the local main network, the higher the number of reviews (public perception).
The highest correlation between the average rating and the configuration of the 400-m radius area is in the betweenness algorithm, which shows that if the facility is on the local main network, the higher the rating is given (
Table 11).















{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}