
A Middle-Range Theory of Social Isolation in Chronic Illness

Abstract
:1. Background
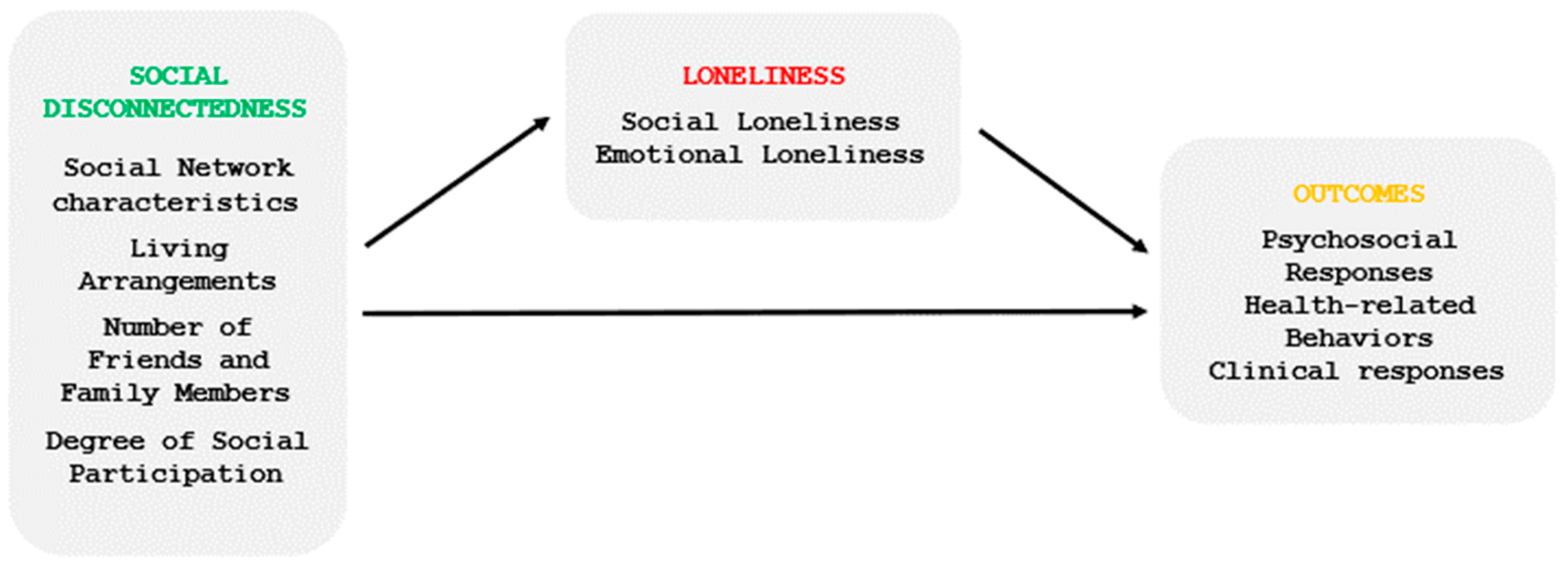
2. Operational Definition of Concepts
2.1. Social Disconnectedness
2.2. Loneliness
2.3. Chronic Illness
3. Antecedents of Social Isolation
3.1. Predisposing Factors
3.2. Precipitating Factors
4. Outcomes of Social Isolation
4.1. Psychosocial Responses
4.2. Health-Related Behaviors
4.3. Clinical Responses
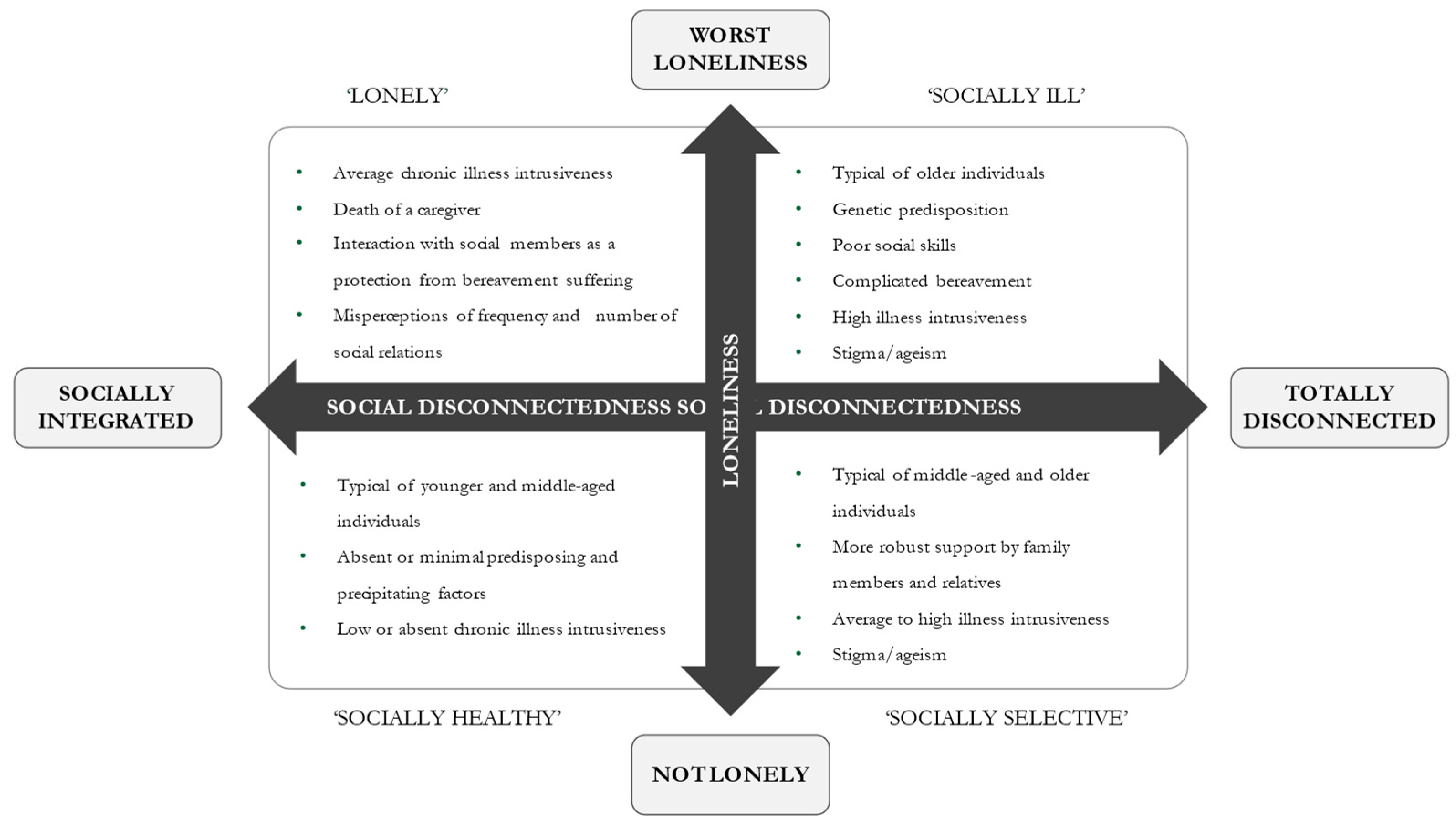
5. Patterns of Social Isolation in Chronic Illness
5.1. Low or Absent Social Disconnectedness and Loneliness
5.2. Increased Social Disconnectedness and Low or Absent Loneliness
5.3. Increased Social Disconnectedness and High Loneliness
5.4. Low/Absent Social Disconnectedness and Increased Loneliness
6. Assumptions
- (1)
- (2)
- Loneliness is a traumatic and detrimental form of social isolation, given the psychological pain and distressing state resulting from the experience [67].
- (3)
- Loneliness is an experience that people do not seek voluntarily. This assumption is in contrast to objective isolation, which can be manipulated to regulate social adjustment, for example, using social network selectivity [60].
7. Propositions
- (1)
- Higher levels of chronic illness intrusiveness impede social participation and reduce the size of social networks.
- (2)
- Social isolation decreases self-care behaviors in people with chronic illnesses.
- (3)
- Stigma related to the chronic illness undermines social interactions and predisposes people to loneliness.
- (4)
- Social disconnectedness and loneliness in chronic illness patients significantly increase health service use.
- (5)
- In chronic illness, the precipitating factors act as triggers to generate social isolation, especially when they occur in clusters.
- (6)
- Social network selectivity in chronically ill people protects against loneliness.
- (7)
- When an illness is not intrusive and predisposing, and the precipitating factors are absent or minimal, individuals are likely to be socially healthy.
8. Clinical and Research Implications
9. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Elovainio, M.; Hakulinen, C.; Pulkki-Råback, L.; Virtanen, M.; Josefsson, K.; Jokela, M.; Vahtera, J.; Kivimäki, M. Contribution of risk factors to excess mortality in isolated and lonely individuals: An analysis of data from the UK Biobank cohort study. Lancet Public Health 2017, 2, e260–e266. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rico-Uribe, L.A.; Caballero, F.F.; Martín-María, N.; Cabello, M.; Ayuso-Mateos, J.L.; Miret, M. Association of loneliness with all-cause mortality: A meta-analysis. PLoS ONE 2018, 13, e0190033. [Google Scholar] [CrossRef] [PubMed]
- Röhr, S.; Wittmann, F.; Engel, C.; Enzenbach, C.; Witte, A.V.; Villringer, A.; Löffler, M.; Riedel-Heller, S.G. Social factors and the prevalence of social isolation in a population-based adult cohort. Soc. Psychiatry Psychiatr. Epidemiol. 2021, 57, 1959–1968. [Google Scholar] [CrossRef] [PubMed]
- Christiansen, J.; Lund, R.; Qualter, P.; Andersen, C.M.; Pedersen, S.S.; Lasgaard, M. Loneliness, social isolation, and chronic disease outcomes. Ann. Behav. Med. 2021, 55, 203–215. [Google Scholar] [CrossRef]
- Petitte, T.; Mallow, J.; Barnes, E.; Petrone, A.; Barr, T.; Theeke, L. A Systematic Review of Loneliness and Common Chronic Physical Conditions in Adults. Open Psychol. J. 2015, 8 (Suppl. S2), 113–132. [Google Scholar] [CrossRef]
- Van Wilder, L.; Pype, P.; Mertens, F.; Rammant, E.; Clays, E.; Devleesschauwer, B.; Boeckxstaens, P.; De Smedt, D. Living with a chronic disease: Insights from patients with a low socioeconomic status. BMC Fam. Pract. 2021, 22, 233. [Google Scholar] [CrossRef]
- Polenick, C.A.; Perbix, E.A.; Salwi, S.M.; Maust, D.T.; Birditt, K.S.; Brooks, J.M. Loneliness During the COVID-19 Pandemic Among Older Adults With Chronic Conditions. J. Appl. Gerontol. 2021, 40, 804–813. [Google Scholar] [CrossRef]
- Stachteas, P.; Symvoulakis, M.; Tsapas, A.; Smyrnakis, E. The impact of the COVID-19 pandemic on the management of patients with chronic diseases in Primary Health Care. Popul. Med. 2022, 4, 1–13. [Google Scholar] [CrossRef]
- Holt-Lunstad, J. A pandemic of social isolation? World Psychiatry 2021, 20, 55. [Google Scholar] [CrossRef]
- Smith, M.J.; Liehr, P.R. Middle Range Theory for Nursing; Springer Publishing Company: Berlin/Heidelberg, Germany, 2018. [Google Scholar]
- Holt-Lunstad, J.; Robles, T.F.; Sbarra, D.A. Advancing social connection as a public health priority in the United States. Am. Psychol. 2017, 72, 517–530. [Google Scholar] [CrossRef]
- Cornwell, E.Y.; Waite, L.J. Measuring Social Isolation Among Older Adults Using Multiple Indicators From the NSHAP Study. J. Gerontol. Ser. B 2009, 64 (Suppl. S1), i38–i46. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Whitehead, L.; Jacob, E.; Towell, A.; Abu-qamar, M.E.; Cole-Heath, A. The role of the family in supporting the self-management of chronic conditions: A qualitative systematic review. J. Clin. Nurs. 2018, 27, 22–30. [Google Scholar] [CrossRef] [PubMed]
- Yanguas, J.; Pinazo-Henandis, S.; Tarazona-Santabalbina, F.J. The complexity of loneliness. Acta Biomed. Atenei Parm. 2018, 89, 302–314. [Google Scholar]
- Weis, R. The Experience of Emotional and Social Isolation; The MIT Press: Cambridge, MA, USA, 1973. [Google Scholar]
- National Academies of Sciences Medicine. Social Isolation and Loneliness in Older Adults: Opportunities for the Health Care System; National Academies Press: Washington, DC, USA, 2020. [Google Scholar]
- Courtin, E.; Knapp, M. Social isolation, loneliness and health in old age: A scoping review. Health Soc. Care Community 2017, 25, 799–812. [Google Scholar] [CrossRef] [PubMed]
- Chatters, L.M.; Taylor, H.O.; Nicklett, E.J.; Taylor, R.J. Correlates of Objective Social Isolation from Family and Friends among Older Adults. Healthcare 2018, 6, 24. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Albert, I. Perceived loneliness and the role of cultural and intergenerational belonging: The case of Portuguese first-generation immigrants in Luxembourg. Eur. J. Ageing 2021, 18, 299–310. [Google Scholar] [CrossRef]
- Henssler, J.; Brandt, L.; Müller, M.; Liu, S.; Montag, C.; Sterzer, P.; Heinz, A. Migration and schizophrenia: Meta-analysis and explanatory framework. Eur. Arch. Psychiatry Clin. Neurosci. 2019, 270, 325–335. [Google Scholar] [CrossRef]
- Keum, B.T.; Waters, E.M.; Wong, M.J.; Salim-Eissa, R. Witnessing racism against racial minority individuals online and loneliness among White emerging adults: Anti-racism advocacy as a moderator. J. Community Psychol. 2022; early view. [Google Scholar] [CrossRef]
- Segel-Karpas, D.; Ayalon, L.; Lachman, M.E. Loneliness and depressive symptoms: The moderating role of the transition into retirement. Aging Ment. Health 2016, 22, 135–140. [Google Scholar] [CrossRef]
- Cohen-Mansfield, J.; Shmotkin, D.; Goldberg, S. Loneliness in old age: Longitudinal changes and their determinants in an Israeli sample. Int. Psychogeriatrics 2009, 21, 1160–1170. [Google Scholar] [CrossRef]
- Victor, C.R.; Pikhartova, J. Lonely places or lonely people? Investigating the relationship between loneliness and place of residence. BMC Public Health 2020, 20, 778. [Google Scholar] [CrossRef] [PubMed]
- Andrew, N.; Meeks, S. Fulfilled preferences, perceived control, life satisfaction, and loneliness in elderly long-term care residents. Aging Ment. Health 2018, 22, 183–189. [Google Scholar] [CrossRef]
- Iveniuk, J. Social networks, role-relationships, and personality in older adulthood. J. Gerontol. Ser. B 2019, 74, 815–826. [Google Scholar] [CrossRef] [PubMed]
- Litwin, H.; Levinsky, M. Does personality shape the personal social networks of older Europeans? Eur. J. Ageing 2022, 19, 717–727. [Google Scholar] [CrossRef] [PubMed]
- O’Donnell, A.T.; Habenicht, A.E. Stigma is associated with illness self-concept in individuals with concealable chronic illnesses. Br. J. Health Psychol. 2021, 27, 136–158. [Google Scholar] [CrossRef]
- O’Donnell, A.T.; O’Carroll, T.; Toole, N. Internalized stigma and stigma-related isolation predict women’s psychological distress and physical health symptoms post-abortion. Psychol. Women Q. 2018, 42, 220–234. [Google Scholar] [CrossRef]
- Palant, A.; Himmel, W. Are there also negative effects of social support? A qualitative study of patients with inflammatory bowel disease. BMJ Open 2019, 9, e022642. [Google Scholar] [CrossRef] [Green Version]
- Ayalon, L.; Tesch-Römer, C. Contemporary Perspectives on Ageism; Springer Nature: Berlin, Germany, 2018. [Google Scholar]
- Richman, S. Grief and Chronic Disease; Cinahl Information Systems: Glendale, CA, USA, 2022. [Google Scholar]
- Liu, S.Y.; Wrosch, C.; Morin, A.J.; Quesnel-Vallée, A.; Pruessner, J.C. Changes in self-esteem and chronic disease across adulthood: A 16-year longitudinal analysis. Soc. Sci. Med. 2019, 242, 112600. [Google Scholar] [CrossRef]
- Filej, B.; Žvanut, B.; Kaučič, B.M. The connection between chronic diseases and self-image and self-esteem. J. Health Sci. 2018, 8, 54–61. [Google Scholar] [CrossRef] [Green Version]
- Michalski, C.A.; Diemert, L.M.; Helliwell, J.F.; Goel, V.; Rosella, L.C. Relationship between sense of community belonging and self-rated health across life stages. SSM Popul. Health 2020, 12, 100676. [Google Scholar] [CrossRef]
- Lian, O.S.; Lorem, G.F. “I Do Not Really Belong Out There Anymore” Sense of Being and Belonging Among People With Medically Unexplained Long-Term Fatigue. Qual. Health Res. 2017, 27, 474–486. [Google Scholar] [CrossRef] [PubMed]
- Antonovsky, A. How People Manage Stress and Stay Well. In Unraveling the Mystery of Health; Jossey-Bass: San Francisco, CA, USA, 1987. [Google Scholar]
- Czaja, S.J.; Moxley, J.H.; Rogers, W.A. Social Support, Isolation, Loneliness, and Health Among Older Adults in the PRISM Randomized Controlled Trial. Front. Psychol. 2021, 12, 4307. [Google Scholar] [CrossRef] [PubMed]
- Elmer, T.; Stadtfeld, C. Depressive symptoms are associated with social isolation in face-to-face interaction networks. Sci. Rep. 2020, 10, 1444. [Google Scholar] [CrossRef] [Green Version]
- Santini, Z.I.; Koyanagi, A.; Tyrovolas, S.; Mason, C.; Haro, J.M. The association between social relationships and depression: A systematic review. J. Affect. Disord. 2015, 175, 53–65. [Google Scholar] [CrossRef] [PubMed]
- Domènech-Abella, J.; Lara, E.; Rubio-Valera, M.; Olaya, B.; Moneta, M.V.; Rico-Uribe, L.A.; Ayuso-Mateos, J.L.; Mundó, J.; Haro, J.M. Loneliness and depression in the elderly: The role of social network. Soc. Psychiatry Psychiatr. Epidemiol. 2017, 52, 381–390. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jeuring, H.W.; Stek, M.L.; Huisman, M.; Voshaar, R.C.O.; Naarding, P.; Collard, R.M.; Beekman, A.T.; Comijs, H.C. A six-year prospective study of the prognosis and predictors in patients with late-life depression. Am. J. Geriatr. Psychiatry 2018, 26, 985–997. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Matthews, T.; Danese, A.; Wertz, J.; Odgers, C.L.; Ambler, A.; Moffitt, T.E.; Arseneault, L. Social isolation, loneliness and depression in young adulthood: A behavioural genetic analysis. Soc. Psychiatry Psychiatr. Epidemiol. 2016, 51, 339–348. [Google Scholar] [CrossRef] [Green Version]
- Beridze, G.; Ayala, A.; Ribeiro, O.; Fernández-Mayoralas, G.; Rodríguez-Blázquez, C.; Rodríguez-Rodríguez, V.; Calderón-Larrañaga, A. Are loneliness and social isolation associated with quality of life in older adults? Insights from Northern and Southern Europe. Int. J. Environ. Res. Public Health 2020, 17, 8637. [Google Scholar] [CrossRef]
- Moreno-Tamayo, K.; Manrique-Espinoza, B.; Ramírez-García, E.; Sánchez-García, S. Social isolation undermines quality of life in older adults. Int. Psychogeriatr. 2019, 32, 1283–1292. [Google Scholar] [CrossRef]
- Riegel, B.; Jaarsma, T.; Strömberg, A. A Middle-Range Theory of Self-Care of Chronic Illness. Adv. Nurs. Sci. 2012, 35, 194–204. [Google Scholar] [CrossRef] [Green Version]
- Lee, C.S.; Westland, H.; Faulkner, K.M.; Iovino, P.; Thompson, J.H.; Sexton, J.; Farry, E.; Jaarsma, T.; Riegel, B. The effectiveness of self-care interventions in chronic illness: A meta-analysis of randomized controlled trials. Int. J. Nurs. Stud. 2022, 134, 104322. [Google Scholar] [CrossRef] [PubMed]
- Kobayashi, L.C.; Steptoe, A. Social Isolation, Loneliness, and Health Behaviors at Older Ages: Longitudinal Cohort Study. Ann. Behav. Med. 2018, 52, 582–593. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Welch, L.; Sadler, E.; Austin, A.; Rogers, A. Social network participation towards enactment of self-care in people with chronic obstructive pulmonary disease: A qualitative meta-ethnography. Health Expect. 2021, 24, 1995–2012. [Google Scholar] [CrossRef] [PubMed]
- Ribeiro, T.C.S.; Barros, M.B.D.A.; Lima, M.G. Smoking and loneliness in older adults: A population-based study in Campinas, São Paulo State, Brazil. Cad. Saúde Pública 2022, 38, e00093621. [Google Scholar] [CrossRef]
- Avci, D.K. Evaluation of the relationship between loneliness and medication adherence in patients with diabetes mellitus: A cross-sectional study. J. Int. Med. Res. 2018, 46, 3149–3161. [Google Scholar] [CrossRef] [Green Version]
- Hawkley, L.C.; Cacioppo, J.T. Loneliness matters: A theoretical and empirical review of consequences and mechanisms. Ann. Behav. Med. 2010, 40, 218–227. [Google Scholar] [CrossRef] [Green Version]
- Evans, I.E.; Martyr, A.; Collins, R.; Brayne, C.; Clare, L. Social isolation and cognitive function in later life: A systematic review and meta-analysis. J. Alzheimer’s Dis. 2019, 70, S119–S144. [Google Scholar] [CrossRef] [Green Version]
- Lara, E.; Caballero, F.F.; Rico-Uribe, L.A.; Olaya, B.; Haro, J.M.; Ayuso-Mateos, J.L.; Miret, M. Are loneliness and social isolation associated with cognitive decline? Int. J. Geriatr. Psychiatry 2019, 34, 1613–1622. [Google Scholar] [CrossRef]
- Hultsch, D.F.; Hertzog, C.; Small, B.J.; Dixon, R.A. Use it or lose it: Engaged lifestyle as a buffer of cognitive decline in aging? Psychol. Aging 1999, 14, 245. [Google Scholar] [CrossRef]
- Cacioppo, S.; Cacioppo, J.T. Why may allopregnanolone help alleviate loneliness? Med. Hypotheses 2015, 85, 947–952. [Google Scholar] [CrossRef] [Green Version]
- Cené, C.W.; Beckie, T.M.; Sims, M.; Suglia, S.F.; Aggarwal, B.; Moise, N.; Jiménez, M.C.; Gaye, B.; McCullough, L.D. Effects of Objective and Perceived Social Isolation on Cardiovascular and Brain Health: A Scientific Statement From the American Heart Association. J. Am. Heart Assoc. 2022, 11, e026493. [Google Scholar] [CrossRef] [PubMed]
- Mosen, D.M.; Banegas, M.P.; Tucker-Seeley, R.D.; Keast, E.; Hu, W.; Ertz-Berger, B.; Brooks, N. Social Isolation Associated with Future Health Care Utilization. Popul. Health Manag. 2021, 24, 333–337. [Google Scholar] [CrossRef] [PubMed]
- Carstensen, L.L.; Isaacowitz, D.M.; Charles, S.T. Taking time seriously: A theory of socioemotional selectivity. Am. Psychol. 1999, 54, 165. [Google Scholar] [CrossRef] [PubMed]
- Löckenhoff, C.E.; Carstensen, L.L. Socioemotional selectivity theory, aging, and health: The increasingly delicate balance between regulating emotions and making tough choices. J. Personal. 2004, 72, 1395–1424. [Google Scholar] [CrossRef]
- Cacioppo, J.T.; Cacioppo, S.; Boomsma, D.I. Evolutionary mechanisms for loneliness. Cogn. Emot. 2014, 28, 3–21. [Google Scholar] [CrossRef] [PubMed]
- Long, M.V.; Martin, P. Personality, relationship closeness, and loneliness of oldest old adults and their children. J. Gerontol. Ser. B Psychol. Sci. Soc. Sci. 2000, 55, P311–P319. [Google Scholar] [CrossRef] [Green Version]
- Ward, M.; Layte, R.; Kenny, R.A. Loneliness, Social Isolation, and Their Discordance among Older Adults; The Irish Longitudinal Study on Ageing: Dublin, Ireland, 2019. [Google Scholar]
- Peterson, S.J.; Bredow, T.S. (Eds.) Middle Range Theories: Application to Nursing Research; Lippincott Williams & Wilkins: Philadelphia, PA, USA, 2009. [Google Scholar]
- Fiske, S.T. Social Beings: Core Motives in Social Psychology; John Wiley Sons: Hoboken, NJ, USA, 2018. [Google Scholar]
- Halcomb, E.; Thompson, C.; Tillott, S.; Robinson, K.; Lucas, E. Exploring social connectedness in older Australians with chronic conditions: Results of a descriptive survey. Collegian 2022, 29, 860–866. [Google Scholar] [CrossRef]
- Roberts, T.; Krueger, J. Loneliness and the Emotional Experience of Absence. South. J. Philos. 2020, 59, 185–204. [Google Scholar] [CrossRef]
- Ellis, S.; Ali, S.S.; Ahmed, W. A review of the impact of hearing interventions on social isolation and loneliness in older people with hearing loss. Eur. Arch. Oto Rhino Laryngol. 2021, 278, 4653–4661. [Google Scholar] [CrossRef]
- Thomas, N.; McLeod, B.; Jones, N.; Abbott, J.-A. Developing Internet interventions to target the individual impact of stigma in health conditions. Internet Interv. 2015, 2, 351–358. [Google Scholar] [CrossRef] [Green Version]
- Kalik, D.; van Loon, A. Understanding transition in chronic illness. Aust. Nurs. Midwifery J. 2007, 15, 29. [Google Scholar]




{kind=link}
{kind=link}
{kind=link}
| Measure | Domain | Indicator/Description |
|---|---|---|
| Social disconnectedness | Social network characteristics | Social network size |
| Social network range | ||
| Amount of social network members | ||
| Average frequency of interaction with network members | ||
| Average closeness with network members | ||
| Living arrangements | Household size | |
| Living alone | ||
| Number of friends and family members | Spouse or current partner | |
| Number of friends | ||
| Number of children | ||
| Number of grandchildren | ||
| Social participation | Attending religious services | |
| Attending meetings of an organized group | ||
| Socializing with friends and relatives | ||
| Socializing with neighbors | ||
| Volunteering activities | ||
| Loneliness | Emotional loneliness | Lack of an attachment figure to rely on |
| Social loneliness | Lack of a larger social network |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Iovino, P.; Vellone, E.; Cedrone, N.; Riegel, B. A Middle-Range Theory of Social Isolation in Chronic Illness. Int. J. Environ. Res. Public Health 2023, 20, 4940. https://doi.org/10.3390/ijerph20064940
Iovino P, Vellone E, Cedrone N, Riegel B. A Middle-Range Theory of Social Isolation in Chronic Illness. International Journal of Environmental Research and Public Health. 2023; 20(6):4940. https://doi.org/10.3390/ijerph20064940
Chicago/Turabian StyleIovino, Paolo, Ercole Vellone, Nadia Cedrone, and Barbara Riegel. 2023. "A Middle-Range Theory of Social Isolation in Chronic Illness" International Journal of Environmental Research and Public Health 20, no. 6: 4940. https://doi.org/10.3390/ijerph20064940