
A Case of Autoimmune Small Fiber Neuropathy as Possible Post COVID Sequelae
 , , ,
, , , {kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Case Presentation
3. Materials and Methods
3.1. Medical History
3.2. Laboratory Testing
3.2.1. Routine and Rheumatologic Parameters
3.2.2. SCN9A Gene
3.2.3. SARS-CoV-2 Testing
3.3. Noninvasive Diagnostics
3.4. Dermatologic and Neurologic Testing
3.4.1. Nerve Conduction Studies
3.4.2. Nerve Biopsy
4. Results
4.1. General Clinical Findings
4.2. Laboratory Findings
4.2.1. Routine and Rheumatologic Parameters
4.2.2. Genetic Testing
4.2.3. SARS-CoV-2 Testing
4.3. Noninvasive Diagnostics
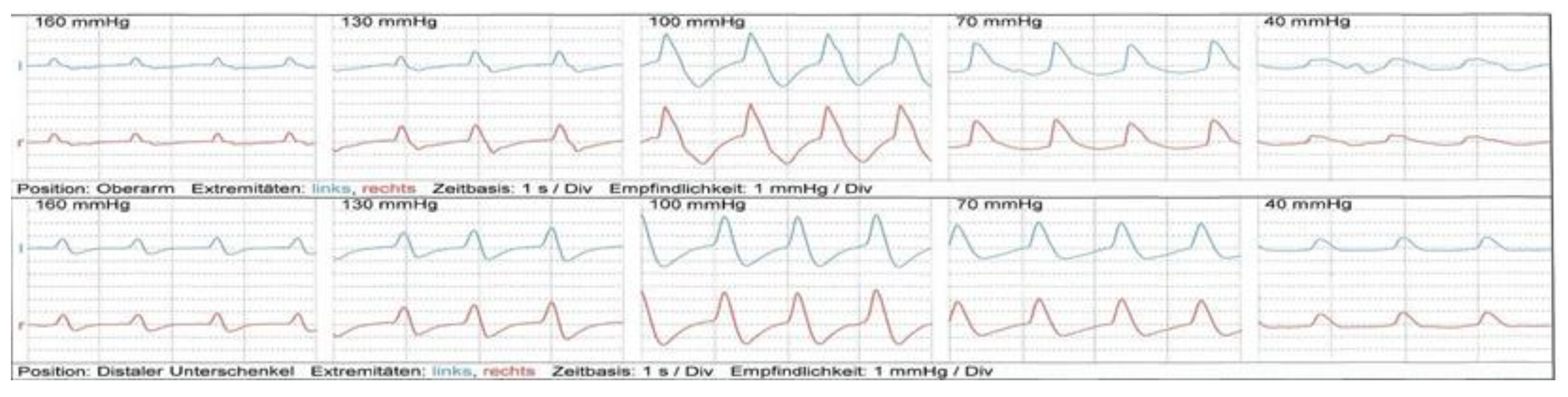
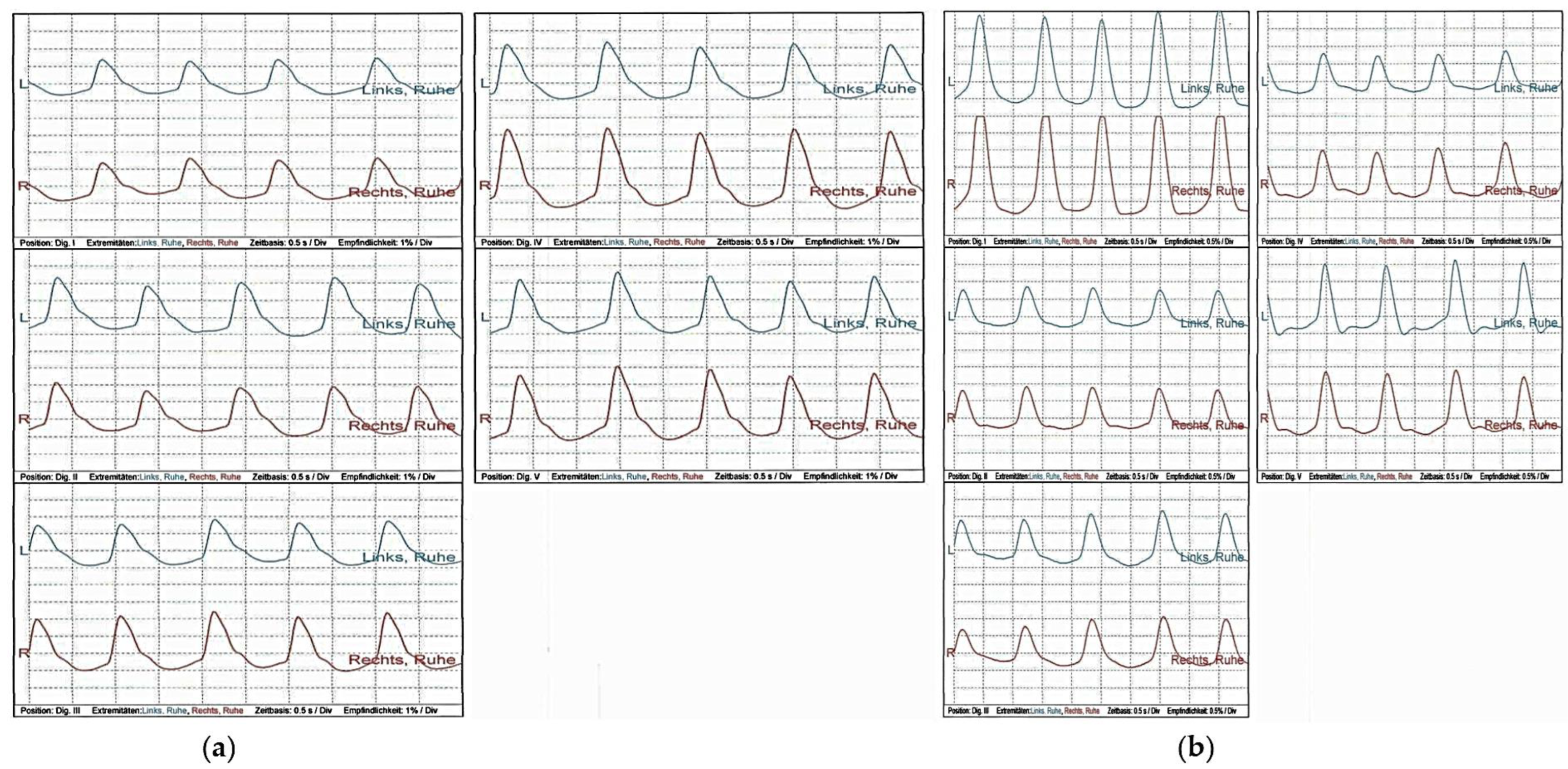
4.3.1. Sonography and Oscillography
4.3.2. Capillary Microscopy
4.4. Dermatologic and Neurologic Testing
4.4.1. Skin Biopsy
4.4.2. Nerve Conduction Studies
4.4.3. Nerve Biopsy
5. Therapeutic Measures and Outcomes
6. Discussion
7. Conclusions
Author Contributions
Funding
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Hovaguimian, A.; Gibbons, C.H. Diagnosis and treatment of pain in small-fiber neuropathy. Curr. Pain Headache Rep. 2011, 15, 193–200. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brouwer, B.A.; de Greef, B.T.A.; Hoeijmakers, J.G.J.; Geerts, M.; van Kleef, M.; Merkies, I.S.J.; Faber, C.G. Neuropathic Pain due to Small Fiber Neuropathy in Aging: Current Management and Future Prospects. Drugs Aging 2015, 32, 611–621. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Levine, T.D. Small Fiber Neuropathy: Disease Classification Beyond Pain and Burning. J. Cent. Nerv. Syst. Dis. 2018, 10, 1179573518771703. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tavee, J.; Zhou, L. Small fiber neuropathy: A burning problem. Clevel. Clin. J. Med. 2009, 76, 297–305. [Google Scholar] [CrossRef]
- Samuelsson, K.; Kostulas, K.; Vrethem, M.; Rolfs, A.; Press, R. Idiopathic small fiber neuropathy: Phenotype, etiologies, and the search for fabry disease. J. Clin. Neurol. 2014, 10, 108–118. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Terkelsen, A.J.; Karlsson, P.; Lauria, G.; Freeman, R.; Finnerup, N.B.; Jensen, T.S. The diagnostic challenge of small fibre neuropathy: Clinical presentations, evaluations, and causes. Lancet Neurol. 2017, 16, 934–944. [Google Scholar] [CrossRef]
- Planté-Bordeneuve, V.; Said, G. Familial amyloid polyneuropathy. Lancet Neurol. 2011, 10, 1086–1097. [Google Scholar] [CrossRef]
- Baker, M.D.; Nassar, M.A. Painful and painless mutations of SCN9A and SCN11A voltage-gated sodium channels. Pflugers Arch. 2020, 472, 865–880. [Google Scholar] [CrossRef]
- Fertleman, C.R.; Baker, M.D.; Parker, K.A.; Moffatt, S.; Elmslie, F.V.; Abrahamsen, B.; Ostman, J.; Klugbauer, N.; Wood, J.N.; Gardiner, R.M.; et al. SCN9A mutations in paroxysmal extreme pain disorder: Allelic variants underlie distinct channel defects and phenotypes. Neuron 2006, 52, 767–774. [Google Scholar] [CrossRef] [Green Version]
- Tang, Z.; Chen, Z.; Tang, B.; Jiang, H. Primary erythromelalgia: A review. Orphanet J. Rare Dis. 2015, 10, 127. [Google Scholar] [CrossRef] [Green Version]
- Jin, Y.; Wang, W.; Chen, W.; Guo, S.; Li, C.; Zhu, D.; Bi, Y. Corneal confocal microscopy: A useful tool for diagnosis of small fiber neuropathy in type 2 diabetes. J. Diabetes Investig. 2021, 12, 2183–2189. [Google Scholar] [CrossRef] [PubMed]
- Binder, A.; Baron, R. The Pharmacological Therapy of Chronic Neuropathic Pain. Dtsch. Arztebl. Int. 2016, 113, 616–625. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Finnerup, N.B.; Attal, N.; Haroutounian, S.; McNicol, E.; Baron, R.; Dworkin, R.H.; Gilron, I.; Haanpää, M.; Hansson, P.; Jensen, T.S.; et al. Pharmacotherapy for neuropathic pain in adults: A systematic review and meta-analysis. Lancet Neurol. 2015, 14, 162–173. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wadowski, P.P.; Piechota-Polańczyk, A.; Andreas, M.; Kopp, C.W. Cardiovascular Disease Management in the Context of Global Crisis. Int. J. Environ. Res. Public Health 2022, 20, 689. [Google Scholar] [CrossRef] [PubMed]
- Siripanthong, B.; Asatryan, B.; Hanff, T.C.; Chatha, S.R.; Khanji, M.Y.; Ricci, F.; Muser, D.; Ferrari, V.A.; Nazarian, S.; Santangeli, P.; et al. The Pathogenesis and Long-Term Consequences of COVID-19 Cardiac Injury. JACC Basic Transl. Sci. 2022, 7, 294–308. [Google Scholar] [CrossRef] [PubMed]
- Wadowski, P.P.; Jilma, B.; Kopp, C.W.; Ertl, S.; Gremmel, T.; Koppensteiner, R. Glycocalyx as Possible Limiting Factor in COVID-19. Front. Immunol. 2021, 12, 607306. [Google Scholar] [CrossRef] [PubMed]
- Ackermann, M.; Verleden, S.E.; Kuehnel, M.; Haverich, A.; Welte, T.; Laenger, F.; Vanstapel, A.; Werlein, C.; Stark, H.; Tzankov, A.; et al. Pulmonary Vascular Endothelialitis, Thrombosis, and Angiogenesis in Covid-19. N. Engl. J. Med. 2020, 383, 120–128. [Google Scholar] [CrossRef]
- Varga, Z.; Flammer, A.J.; Steiger, P.; Haberecker, M.; Andermatt, R.; Zinkernagel, A.S.; Mehra, M.R.; Schuepbach, R.A.; Ruschitzka, F.; Moch, H. Endothelial cell infection and endotheliitis in COVID-19. Lancet 2020, 395, 1417–1418. [Google Scholar] [CrossRef]
- Wadowski, P.P.; Panzer, B.; Józkowicz, A.; Kopp, C.W.; Gremmel, T.; Panzer, S.; Koppensteiner, R. Microvascular Thrombosis as a Critical Factor in Severe COVID-19. Int. J. Mol. Sci. 2023, 24, 2492. [Google Scholar] [CrossRef]
- Gracia-Ramos, A.E.; Martin-Nares, E.; Hernández-Molina, G. New Onset of Autoimmune Diseases Following COVID-19 Diagnosis. Cells 2021, 10, 3592. [Google Scholar] [CrossRef]
- Seeliger, T.; Prenzler, N.K.; Gingele, S.; Seeliger, B.; Körner, S.; Thiele, T.; Bönig, L.; Sühs, K.-W.; Witte, T.; Stangel, M.; et al. Neuro-Sjögren: Peripheral Neuropathy With Limb Weakness in Sjögren’s Syndrome. Front. Immunol. 2019, 10, 1600. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liu, Z.; Chu, A. Sjögren’s Syndrome and Viral Infections. Rheumatol. Ther. 2021, 8, 1051–1059. [Google Scholar] [CrossRef] [PubMed]
- Utomo, S.W.; Putri, J.F. Infections as Risk Factor of Sjögren’s Syndrome. Open Access Rheumatol. Res. Rev. 2020, 12, 257–266. [Google Scholar] [CrossRef] [PubMed]
- Aiyegbusi, O.L.; Hughes, S.E.; Turner, G.; Rivera, S.C.; McMullan, C.; Chandan, J.S.; Haroon, S.; Price, G.; Davies, E.H.; Nirantharakumar, K.; et al. Symptoms, complications and management of long COVID: A review. J. R. Soc. Med. 2021, 114, 428–442. [Google Scholar] [CrossRef]
- Banda, J.M.; Gurdas, V.; Singh, S.R.; Alser, O.H.; Prieto-Alhambra, D. Long-term patient-reported symptoms of COVID-19: An analysis of social media data. medRxiv, 2020; preprint. [Google Scholar] [CrossRef]
- Cirulli, E.T.; Barrett, K.M.S.; Riffle, S.; Bolze, A.; Neveux, I.; Dabe, S.; Grzymski, J.J.; Lu, J.T.; Washington, N.L. Long-term COVID-19 symptoms in a large unselected population. medRxiv, 2020; preprint. [Google Scholar] [CrossRef]
- Davis, H.E.; Assaf, G.S.; McCorkell, L.; Wei, H.; Low, R.J.; Re'Em, Y.; Redfield, S.; Austin, J.P.; Akrami, A. Characterizing Long COVID in an International Cohort: 7 Months of Symptoms and Their Impact. EClinicalMedicine 2021, 38, 101019. [Google Scholar] [CrossRef]
- Lu, Y.; Li, X.; Geng, D.; Mei, N.; Wu, P.-Y.; Huang, C.-C.; Jia, T.; Zhao, Y.; Wang, D.; Xiao, A.; et al. Cerebral Micro-Structural Changes in COVID-19 Patients—An MRI-based 3-month Follow-up Study. EClinicalMedicine 2020, 25, 100484. [Google Scholar] [CrossRef]
- Stavem, K.; Ghanima, W.; Olsen, M.K.; Gilboe, H.M.; Einvik, G. Persistent symptoms 1.5–6 months after COVID-19 in non-hospitalised subjects: A population-based cohort study. Thorax 2021, 76, 405. [Google Scholar] [CrossRef]
- Sudre, C.H.; Murray, B.; Varsavsky, T.; Graham, M.S.; Penfold, R.S.; Bowyer, R.C.; Pujol, J.C.; Klaser, K.; Antonelli, M.; Canas, L.S. Attributes and predictors of Long-COVID: Analysis of COVID cases and their symptoms collected by the Covid Symptoms Study App. medRxiv 2020, 10, 20214494. [Google Scholar] [CrossRef]
- Daher, A.; Balfanz, P.; Cornelissen, C.; Müller, A.; Bergs, I.; Marx, N.; Müller-Wieland, D.; Hartmann, B.; Dreher, M.; Müller, T. Follow up of patients with severe coronavirus disease 2019 (COVID-19): Pulmonary and extrapulmonary disease sequelae. Respir. Med. 2020, 174, 106197. [Google Scholar] [CrossRef]
- Shouman, K.; Vanichkachorn, G.; Cheshire, W.P.; Suarez, M.D.; Shelly, S.; Lamotte, G.J.; Sandroni, P.; Benarroch, E.E.; Berini, S.E.; Cutsforth-Gregory, J.K.; et al. Autonomic dysfunction following COVID-19 infection: An early experience. Clin. Auton. Res. 2021, 31, 385–394. [Google Scholar] [CrossRef] [PubMed]
- Gemignani, F. Small Fiber Neuropathy and SARS-CoV-2 Infection. Another piece in the long COVID puzzle? Muscle Nerve 2022, 65, 369–370. [Google Scholar] [CrossRef] [PubMed]
- Bocci, T.; Bertini, A.; Campiglio, L.; Botta, S.; Libelli, G.; Guidetti, M.; Priori, A. Not myopathic, but autonomic changes in patients with long-COVID syndrome: A case series. Neurol. Sci. 2023, 1, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Oke, V.; Wahren-Herlenius, M. The immunobiology of Ro52 (TRIM21) in autoimmunity: A critical review. J. Autoimmun. 2012, 39, 77–82. [Google Scholar] [CrossRef] [PubMed]
- Invernizzi, P.; Bossuyt, X.; Bogdanos, D.P. Serum autoantibodies: From identification to clinical relevance. Clin. Dev. Immunol. 2013, 2013, 382069. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hervier, B.; Rimbert, M.; Colonna, F.; Hamidou, M.A.; Audrain, M. Clinical significance of anti-Ro/SSA-52 kDa antibodies: A retrospective monocentric study. Rheumatology 2009, 48, 964–967. [Google Scholar] [CrossRef] [Green Version]
- Cox, J.J.; Reimann, F.; Nicholas, A.K.; Thornton, G.; Roberts, E.; Springell, K.; Karbani, G.; Jafri, H.; Mannan, J.; Raashid, Y.; et al. An SCN9A channelopathy causes congenital inability to experience pain. Nature 2006, 444, 894–898. [Google Scholar] [CrossRef]
- Dib-Hajj, S.D.; Cummins, T.R.; Black, J.A.; Waxman, S.G. From genes to pain: Na v 1.7 and human pain disorders. Trends Neurosci. 2007, 30, 555–563. [Google Scholar] [CrossRef]
- Elecsys® Anti-SARS-CoV-2 S. Available online: https://diagnostics.roche.com/global/en/products/params/elecsys-anti-sars-cov-2-s.html (accessed on 4 March 2023).
- Elecsys® Anti-SARS-CoV-2. Available online: https://diagnostics.roche.com/global/en/products/params/elecsys-anti-sars-cov-2.html (accessed on 4 March 2023).
- Taffertshofer, K.; Walter, M.; Mackeben, P.; Kraemer, J.; Potapov, S.; Jochum, S. Design and performance characteristics of the Elecsys anti-SARS-CoV-2 S assay. Front. Immunol. 2022, 13, 1002576. [Google Scholar] [CrossRef]
- Aboyans, V.; Ricco, J.-B.; Bartelink, M.-L.E.L.; Björck, M.; Brodmann, M.; Cohnert, T.; Collet, J.-P.; Czerny, M.; De Carlo, M.; Debus, S.; et al. 2017 ESC Guidelines on the Diagnosis and Treatment of Peripheral Arterial Diseases, in collaboration with the European Society for Vascular Surgery (ESVS): Document covering atherosclerotic disease of extracranial carotid and vertebral, mesenteric, renal. Eur. Heart J. 2018, 39, 763–816. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wadowski, P.P.; Giurgea, G.-A.; Schlager, O.; Luf, A.; Gremmel, T.; Hobl, E.-L.; Unterhumer, S.; Löffler-Stastka, H.; Koppensteiner, R. Acute Limb Ischemia after Intake of the Phenylethylamine Derivate NBOMe. Int. J. Environ. Res. Public Health 2019, 16, 5071. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- AbuRahma, A.F. Overview of Noninvasive Vascular Techniques in Peripheral Arterial Disease. In Noninvasive Peripheral Arterial Diagnosis; AbuRahma, A.F., Bergan, J.J., Eds.; Springer: London, UK, 2010. [Google Scholar] [CrossRef]
- Tavee, J. Nerve conduction studies: Basic concepts. Handb. Clin. Neurol. 2019, 160, 217–224. [Google Scholar] [CrossRef] [PubMed]
- Weis, J.; Katona, I.; Nikolin, S.; Nobbio, L.; Prada, V.; Grandis, M.; Schenone, A. Techniques for the standard histological and ultrastructural assessment of nerve biopsies. J. Peripher. Nerv. Syst. 2021, 26 (Suppl. S2), S3–S10. [Google Scholar] [CrossRef]
- Shiboski, C.H.; Shiboski, S.C.; Seror, R.; Criswell, L.A.; Labetoulle, M.; Lietman, T.M.; Rasmussen, A.; Scofield, H.; Vitali, C.; Bowman, S.J.; et al. 2016 American College of Rheumatology/European League Against Rheumatism Classification Criteria for Primary Sjögren’s Syndrome: A Consensus and Data-Driven Methodology Involving Three International Patient Cohorts. Arthritis Rheumatol. 2017, 69, 35–45. [Google Scholar] [CrossRef] [PubMed]
- Ørstavik, K.; Norheim, I.; Jørum, E. Pain and small-fiber neuropathy in patients with hypothyroidism. Neurology 2006, 67, 786–791. [Google Scholar] [CrossRef]
- Sumner, C.J.; Sheth, S.; Griffin, J.W.; Cornblath, D.R.; Polydefkis, M. The spectrum of neuropathy in diabetes and impaired glucose tolerance. Neurology 2003, 60, 108–111. [Google Scholar] [CrossRef]
- Stein, S.R.; Ramelli, S.C.; Grazioli, A.; Chung, J.-Y.; Singh, M.; Yinda, C.K.; Winkler, C.W.; Sun, J.; Dickey, J.M.; Ylaya, K.; et al. SARS-CoV-2 infection and persistence in the human body and brain at autopsy. Nature 2022, 612, 758–763. [Google Scholar] [CrossRef]
- Abrams, R.M.C.; Simpson, D.M.; Navis, A.; Jette, N.; Zhou, L.; Shin, S.C. Small fiber neuropathy associated with SARS-CoV-2 infection. Muscle Nerve 2022, 65, 440–443. [Google Scholar] [CrossRef]
- Oaklander, A.L.; Mills, A.J.; Kelley, M.; Toran, L.S.; Smith, B.; Dalakas, M.C.; Nath, A. Peripheral Neuropathy Evaluations of Patients With Prolonged Long COVID. Neurol. Neuroimmunol. Neuroinflamm. 2022, 9, e1146. [Google Scholar] [CrossRef]
- Milena Luisa, S.; Letícia Caroline, B.; Marcus Vinícius Magno, G. Small Fiber Neuropathy Associated COVID-19: A Common or Uncommon Complication? Int. J. Neurol. Neurother. 2021, 8, 113. [Google Scholar] [CrossRef]
- Burakgazi, A.Z. Small-Fiber Neuropathy Possibly Associated with COVID-19. Case Rep. Neurol. 2022, 14, 208–212. [Google Scholar] [CrossRef] [PubMed]
- Shiers, S.; Ray, P.R.; Wangzhou, A.; Sankaranarayanan, I.; Tatsui, C.E.; Rhines, L.D.; Li, Y.; Uhelski, M.L.; Dougherty, P.M.; Price, T.J. ACE2 and SCARF expression in human dorsal root ganglion nociceptors: Implications for SARS-CoV-2 virus neurological effects. Pain 2020, 161, 2494–2501. [Google Scholar] [CrossRef]
- Shiers, S.; Ray, P.R.; Wangzhou, A.; Tatsui, C.E.; Rhines, L.; Li, Y.; Uhelski, M.; Dougherty, P.M.; Price, T. ACE2 expression in human dorsal root ganglion sensory neurons: Implications for SARS-CoV-2 virus-induced neurological effects. bioRxiv, 2020; preprint. [Google Scholar] [CrossRef]
- Martínez-Lavín, M.; Martínez-Martínez, L.A.; Reyes-Loyola, P. HPV vaccination syndrome. A questionnaire-based study. Clin. Rheumatol. 2015, 34, 1981–1983. [Google Scholar] [CrossRef] [PubMed]
- Ryabkova, V.A.; Churilov, L.P.; Shoenfeld, Y. Neuroimmunology: What Role for Autoimmunity, Neuroinflammation, and Small Fiber Neuropathy in Fibromyalgia, Chronic Fatigue Syndrome, and Adverse Events after Human Papillomavirus Vaccination? Int. J. Mol. Sci. 2019, 20, 5164. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Martínez-Lavín, M. Hypothesis: Human papillomavirus vaccination syndrome--small fiber neuropathy and dysautonomia could be its underlying pathogenesis. Clin. Rheumatol. 2015, 34, 1165–1169. [Google Scholar] [CrossRef]
- Kang, L.W.; Crawford, N.; Tang, M.L.K.; Buttery, J.; Royle, J.; Gold, M.; Ziegler, C.; Quinn, P.; Elia, S.; Choo, S. Hypersensitivity reactions to human papillomavirus vaccine inAustralian schoolgirls: Retrospective cohort study. BMJ 2008, 337, 1392–1396. [Google Scholar] [CrossRef] [Green Version]
- Chaudhari, P.; Bruckner, A.; Kim, J.; Benjamin, L.; Zaba, L. Urticarial vasculitis secondary to HPV vaccination in a 13-year-old girl. J. Am. Acad. Dermatol. 2012, 66, AB169. [Google Scholar] [CrossRef]
- Gold, M.; Goodwin, H.; Botham, S.; Burgess, M.; Nash, M.; Kempe, A. Re-vaccination of 421 children with a past history of an adversevaccine reaction in a special immunisation service. Arch. Dis. Child. 2000, 83, 128. [Google Scholar] [CrossRef] [Green Version]
- Löffler-Stastka, H.; Pietrzak-Franger, M. COVID-19 survivors: Multi-disciplinary efforts in psychiatry and medical humanities for long-term realignment. World J. Psychiatry 2022, 12, 995–998. [Google Scholar] [CrossRef] [PubMed]
- Löffler-Stastka, H.; Steinmair, D. Future of processing and facilitating change and learning. World J. Psychiatry 2021, 11, 507–516. [Google Scholar] [CrossRef] [PubMed]
- Steinmair, D.; Löffler-Stastka, H. Personalized treatment-which interaction ingredients should be focused to capture the unconscious. World J. Clin. Cases 2022, 10, 2053–2062. [Google Scholar] [CrossRef] [PubMed]
- Tretter, F.; Löffler-Stastka, H. The Human Ecological Perspective and Biopsychosocial Medicine. Int. J. Environ. Res. Public Health 2019, 16, 4230. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Löffler-Stastka, H.; Bednar, K.; Pleschberger, I.; Prevendar, T.; Pietrabissa, G. How to Include Patients’ Perspectives in the Study of the Mind: A Review of Studies on Depression. Front. Psychol. 2021, 12, 651423. [Google Scholar] [CrossRef]
- Romero, C.; Díez, J.M.; Gajardo, R. Anti-SARS-CoV-2 antibodies in healthy donor plasma pools and IVIG products—An update. Lancet Infect. Dis. 2022, 22, 19. [Google Scholar] [CrossRef]
- Stinca, S.; Barnes, T.W.; Vogel, P.; Meyers, W.; Schulte-Pelkum, J.; Filchtinski, D.; Steller, L.; Hauser, T.; Manni, S.; Gardiner, D.F.; et al. Modelling the concentration of anti-SARS-CoV-2 immunoglobulin G in intravenous immunoglobulin product batches. PLoS ONE 2021, 16, e0259731. [Google Scholar] [CrossRef] [PubMed]
- Lindahl, H.; Klingström, J.; Rodrigues, R.D.S.; Christ, W.; Chen, P.; Ljunggren, H.-G.; Buggert, M.; Aleman, S.; Smith, C.I.E.; Bergman, P. Neutralizing SARS-CoV-2 Antibodies in Commercial Immunoglobulin Products Give Patients with X-Linked Agammaglobulinemia Limited Passive Immunity to the Omicron Variant. J. Clin. Immunol. 2022, 42, 1130. [Google Scholar] [CrossRef]




Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Panagiotides, N.G.; Zimprich, F.; Machold, K.; Schlager, O.; Müller, M.; Ertl, S.; Löffler-Stastka, H.; Koppensteiner, R.; Wadowski, P.P. A Case of Autoimmune Small Fiber Neuropathy as Possible Post COVID Sequelae. Int. J. Environ. Res. Public Health 2023, 20, 4918. https://doi.org/10.3390/ijerph20064918
Panagiotides NG, Zimprich F, Machold K, Schlager O, Müller M, Ertl S, Löffler-Stastka H, Koppensteiner R, Wadowski PP. A Case of Autoimmune Small Fiber Neuropathy as Possible Post COVID Sequelae. International Journal of Environmental Research and Public Health. 2023; 20(6):4918. https://doi.org/10.3390/ijerph20064918
Chicago/Turabian StylePanagiotides, Noel G., Fritz Zimprich, Klaus Machold, Oliver Schlager, Markus Müller, Sebastian Ertl, Henriette Löffler-Stastka, Renate Koppensteiner, and Patricia P. Wadowski. 2023. "A Case of Autoimmune Small Fiber Neuropathy as Possible Post COVID Sequelae" International Journal of Environmental Research and Public Health 20, no. 6: 4918. https://doi.org/10.3390/ijerph20064918