
How Can Sport-Based Interventions Improve Health among Women and Girls? A Scoping Review

Abstract
:1. Introduction
2. Materials and Methods
- What health-related outcomes have been evaluated within sport-based intervention research focused on gender equity among women and girls?
- How have participatory research approaches been applied within sport-based intervention research focused on gender equity to enhance relevance and impacts among women and girls?
2.1. Inclusion and Exclusion Criteria
2.2. Search Strategy
2.3. Evidence Screening and Selection
2.4. Data Extraction and Analysis
3. Results
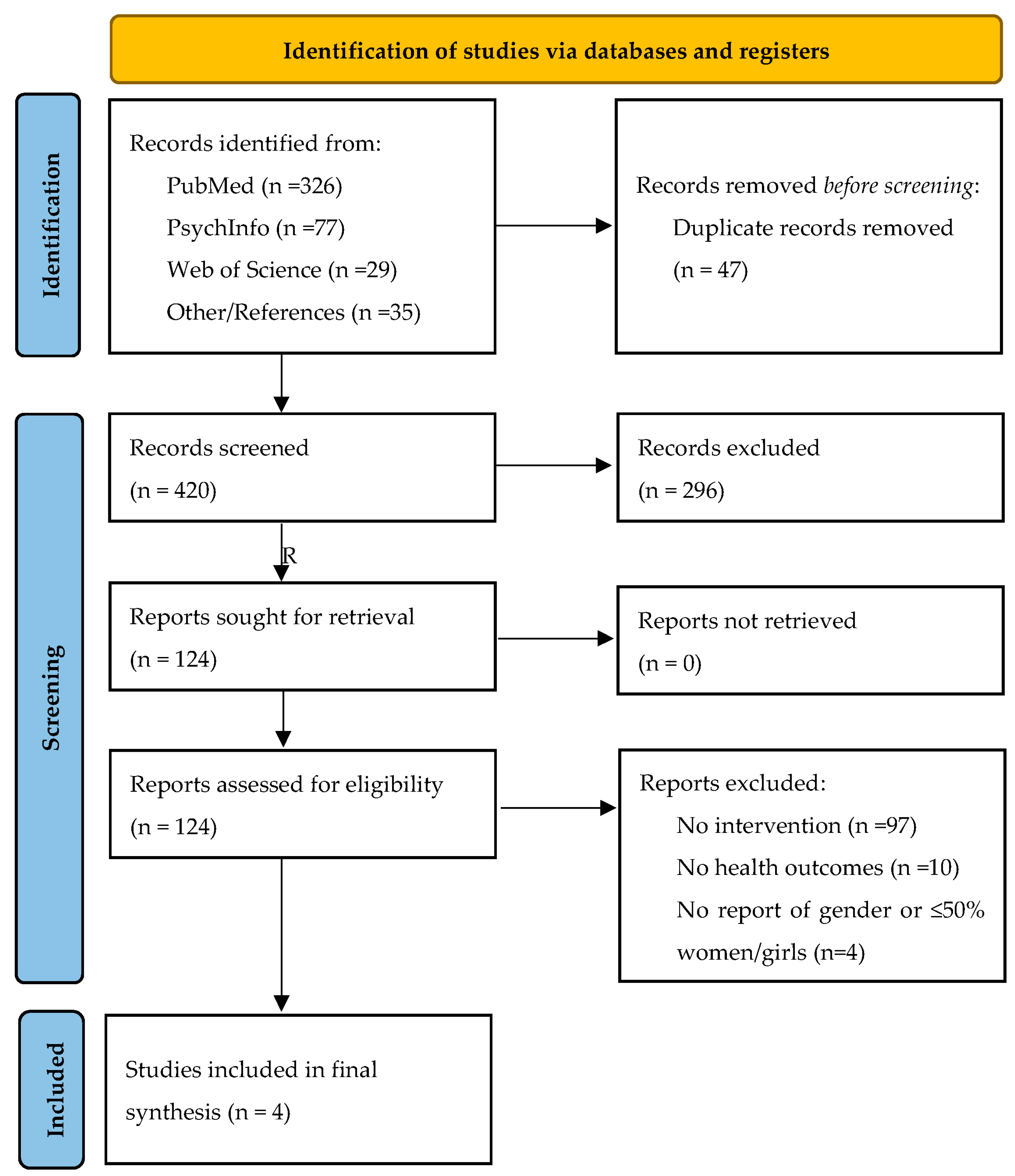
3.1. Selection of Evidence
3.2. Characteristics of the Evidence
3.2.1. Participants
3.2.2. Concept
3.2.3. Context
3.2.4. Evaluation and Results
3.2.5. Participatory and Community-Engaged Approaches
4. Discussion
4.1. Implications for Research and Practice
4.1.1. Develop the Field’s Focus to Include Additional Health and Physical Activity Outcomes
4.1.2. Incorporate Multilevel Approaches and Inclusive Practices to Uncover Structural Barriers and Supports to Sport Participation across the Life Course
4.1.3. Expand Community-Engaged and Participatory Research Approaches
4.1.4. Leverage Emerging Digital Technologies to Collect Data Relevant to Individual, Social, and Environmental Factors
4.2. Promising Directions: An Example Using the Our Voice Participatory Action Citizen Science Method
4.3. Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| NCDs | Non-communicable diseases |
| NGO | Non-governmental organization |
| PA | Physical activity |
| SFD | Sport for development |
| SMS | Short message service |
| UN | United Nations |
| UNESCO | United Nations Educational, Scientific, and Cultural Organization |
| WHO | World Health Organization |
References
- World Health Organization. Global Action Plan on Physical Activity 2018–2030: More Active People for a Healthier World; World Health Organization: Geneva, Switzerland, 2018. Available online: http://apps.who.int/iris/bitstream/handle/10665/272722/9789241514187-eng.pdf (accessed on 18 June 2022).
- Physical Activity Guidelines Advisory Committee. 2018 Physical Activity Guidelines Advisory Committee Scientific Report. 2018. Available online: https://health.gov/sites/default/files/2019-09/PAG_Advisory_Committee_Report.pdf (accessed on 14 April 2020).
- Althoff, T.; Sosič, R.; Hicks, J.L.; King, A.C.; Delp, S.L.; Leskovec, J. Large-scale physical activity data reveal worldwide activity inequality. Nature 2017, 547, 336–339. [Google Scholar] [CrossRef]
- World Health Organization. Global Status Report on Physical Activity 2022; World Health Organization: Geneva, Switzerland, 2022.
- Guthold, R.; Stevens, G.A.; Riley, L.M.; Bull, F.C. Global trends in insufficient physical activity among adolescents: A pooled analysis of 298 population-based surveys with 1·6 million participants. Lancet Child Adolesc. Health 2020, 4, 23–35. [Google Scholar] [CrossRef] [PubMed]
- Khan, K.M.; Thompson, A.M.; Blair, S.N.; Sallis, J.F.; Powell, K.E.; Bull, F.C.; Bauman, A.E. Sport and exercise as contributors to the health of nations. Lancet 2012, 380, 59–64. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Elsborg, P.; Nielsen, G.; Klinker, C.D.; Melby, P.S.; Christensen, J.H.; Bentsen, P. Sports-based recreation as a means to address social inequity in health: Why, when, where, who, what, and how. BMC Public Health 2019, 19, 1084. [Google Scholar] [CrossRef] [Green Version]
- United States President’s Council on Sports, Fitness and Nutrition Benefits of Youth Sports. United States President’s Council on Sports, Fitness and Nutrition; U.S. Department of Health and Human Service: Washington, DC, USA, 2020.
- Eime, R.M.; Young, J.A.; Harvey, J.T.; Charity, M.J.; Payne, W.R. A systematic review of the psychological and social benefits of participation in sport for children and adolescents: Informing development of a conceptual model of health through sport. Int. J. Behav. Nutr. Phys. Act. 2013, 10, 98. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Telama, R.; Yang, X.; Hirvensalo, M.; Raitakari, O. Participation in Organized Youth Sport as a Predictor of Adult Physical Activity: A 21-Year Longitudinal Study. Pediatr. Exerc. Sci. 2006, 18, 76–88. [Google Scholar] [CrossRef]
- Logan, K.; Lloyd, R.S.; Schafer-Kalkhoff, T.; Khoury, J.C.; Ehrlich, S.; Dolan, L.M.; Shah, A.S.; Myer, G.D. Youth sports participation and health status in early adulthood: A 12-year follow-up. Prev. Med. Rep. 2020, 19, 101107. [Google Scholar] [CrossRef]
- Krustrup, P.; Dvorak, J.; Junge, A.; Bangsbo, J. Executive summary: The health and fitness benefits of regular participation in small-sided football games. Scand. J. Med. Sci. Sports 2010, 20, 132–135. [Google Scholar] [CrossRef]
- Helge, E.W.; Aagaard, P.; Jakobsen, M.D.; Sundstrup, E.; Randers, M.B.; Karlsson, M.K.; Krustrup, P. Recreational football training decreases risk factors for bone fractures in untrained premenopausal women. Scand. J. Med. Sci. Sports 2010, 20, 31–39. [Google Scholar] [CrossRef] [PubMed]
- Krustrup, P.; Nielsen, J.J.; Krustrup, B.R.; Christensen, J.F.; Pedersen, H.; Randers, M.B.; Aagaard, P.; Petersen, A.-M.; Nybo, L.; Bangsbo, J. Recreational soccer is an effective health-promoting activity for untrained men. Br. J. Sports Med. 2008, 43, 825–831. [Google Scholar] [CrossRef]
- UNESCO International Charter of Physical Education, Physical Activity and Sport. UNESCO 2015. Available online: https://unesdoc.unesco.org/ark:/48223/pf0000235409_eng (accessed on 14 September 2022).
- Sport for Generation Equality: Advancing Gender Equality in and through Sport. United Nations. United Nations 2020. Available online: https://www.unwomen.org/sites/default/files/Headquarters/Attachments/Sections/News%20and%20events/Stories/2020/Sport-GenerationEquality.pdf (accessed on 14 February 2022).
- UNESCO Fit for Life. UNESCO 2022. Available online: https://www.unesco.org/en/sport-and-anti-doping/fit4life (accessed on 14 September 2022).
- Kidd, B. A new social movement: Sport for development and peace. Sport Soc. 2008, 11, 370–380. [Google Scholar] [CrossRef]
- Schulenkorf, N.; Sherry, E.; Rowe, K. Sport for Development: An Integrated Literature Review. J. Sport Manag. 2016, 30, 22–39. [Google Scholar] [CrossRef] [Green Version]
- United Nations United Nations Charter. United Nations 1945. Available online: https://www.un.org/en/about-us/un-charter (accessed on 14 February 2022).
- Mashale, R.; Kelly, K.; Motuba, T.; Myers, L. TESTING TIMES: A Review of HIV Counselling and Testing within Sports for Development Programmes for Young People in Southern Africa; Centre for AIDS Development, Research and Evaluation (CADRE): Johannesburg, South Africa, 2012. [Google Scholar]
- Hayhurst, L.M.C. Girls as the ‘New’ Agents of Social Change? Exploring the ‘Girl Effect’ through Sport, Gender and Development Programs in Uganda. Sociol. Res. Online 2013, 18, 192–203. [Google Scholar] [CrossRef] [Green Version]
- Richards, J.; Foster, C. Sport-for-Development Interventions: Whom Do They Reach and What Is Their Potential for Impact on Physical and Mental Health in Low-Income Countries? J. Phys. Act. Health 2013, 10, 929–931. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lebel, K.; Mumcu, C.; Pegoraro, A.; LaVoi, N.M.; Lough, N.; Antunovic, D. Re-thinking Women’s Sport Research: Looking in the Mirror and Reflecting Forward. Front. Sports Act. Living 2021, 3, 929–931. [Google Scholar] [CrossRef]
- McDonald, M.G. Imagining neoliberal feminisms? Thinking critically about the US diplomacy campaign, ‘Empowering Women and Girls Through Sports’. Sport Soc. 2015, 18, 909–922. [Google Scholar] [CrossRef]
- Darnell, S.C.; Hayhurst, L.M.C. Sport for decolonization. Prog. Dev. Stud. 2011, 11, 183–196. [Google Scholar] [CrossRef]
- Baum, F. Participatory action research. J. Epidemiol. Community Health 2006, 60, 854–857. [Google Scholar] [CrossRef] [Green Version]
- Wallerstein, N.B.; Duran, B. Using Community-Based Participatory Research to Address Health Disparities. Health Promot. Pract. 2006, 7, 312–323. [Google Scholar] [CrossRef] [PubMed]
- King, A.C.; Odunitan-Wayas, F.A.; Chaudhury, M.; Rubio, M.A.; Baiocchi, M.; Kolbe-Alexander, T.; Montes, F.; Banchoff, A.; Sarmiento, O.; Bälter, K.; et al. Community-Based Approaches to Reducing Health Inequities and Fostering Environmental Justice through Global Youth-Engaged Citizen Science. Int. J. Environ. Res. Public Health 2021, 18, 892. [Google Scholar] [CrossRef]
- King, A.C.; Winter, S.J.; Sheats, J.L.; Rosas, L.G.; Buman, M.P.; Salvo, D.; Rodriguez, N.M.; Seguin, R.A.; Moran, M.; Garber, R.; et al. Leveraging Citizen Science and Information Technology for Population Physical Activity Promotion. Transl. J. Am. Coll. Sports Med. 2016, 1, 30–44. [Google Scholar] [CrossRef]
- González, S.A.; Rubio, M.A.; Triana, C.A.; King, A.C.; Banchoff, A.W.; Sarmiento, O.L. Building healthy schools through technology-enabled citizen science: The case of the our voice participatory action model in schools from Bogotá, Colombia. Glob. Public Health 2021, 17, 403–419. [Google Scholar] [CrossRef]
- Rosas, L.G.; Salvo, D.; Winter, S.J.; Cortes, D.; Rivera, J.; Rodriguez, N.M.; King, A.C. Harnessing Technology and Citizen Science to Support Neighborhoods that Promote Active Living in Mexico. J. Urban Health 2016, 93, 953–973. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Spaaij, R.; Oxford, S.; Jeanes, R. Transforming communities through sport? critical pedagogy and sport for development. Sport Educ. Soc. 2016, 21, 570–587. [Google Scholar] [CrossRef] [Green Version]
- Sherry, E.; Schulenkorf, N. League Bilong Laif: Rugby, education and sport-for-development partnerships in Papua New Guinea. Sport Educ. Soc. 2016, 21, 513–530. [Google Scholar] [CrossRef]
- Peters, M.D.; Marnie, C.; Tricco, A.C.; Pollock, D.; Munn, Z.; Alexander, L.; McInerney, P.; Godfrey, C.M.; Khalil, H. Updated methodological guidance for the conduct of scoping reviews. JBI Database Syst. Rev. Implement. Rep. 2020, 18, 2119–2126. [Google Scholar] [CrossRef] [PubMed]
- Munn, Z.; Peters, M.D.J.; Stern, C.; Tufanaru, C.; McArthur, A.; Aromataris, E. Systematic Review or Scoping Review? Guidance for Authors When Choosing between a Systematic or Scoping Review Approach. BMC Med. Res. Methodol. 2018, 18, 143. [Google Scholar] [CrossRef]
- Tricco, A.C.; Lillie, E.; Zarin, W.; O’Brien, K.K.; Colquhoun, H.; Levac, D.; Moher, D.; Peters, M.D.J.; Horsley, T.; Weeks, L.; et al. PRISMA Extension for Scoping Reviews (PRISMA-ScR): Checklist and Explanation. Ann. Intern. Med. 2018, 169, 467–473. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cislaghi, B.; Bankar, S.; Verma, R.K.; Heise, L.; Collumbien, M. Widening cracks in patriarchy: Mothers and daughters navigating gender norms in a Mumbai slum. Cult. Health Sex. 2019, 22, 166–183. [Google Scholar] [CrossRef] [Green Version]
- Collumbien, M.; Das, M.; Bankar, S.; Cislaghi, B.; Heise, L.; Verma, R.K. Practice-based insights in developing and implementing a sport-based programme for girls. Dev. Pract. 2019, 29, 5–64. [Google Scholar] [CrossRef]
- Hershow, R.B.; Gannett, K.; Merrill, J.; Kaufman, E.B.; Barkley, C.; DeCelles, J.; Harrison, A. Using soccer to build confidence and increase HCT uptake among adolescent girls: A mixed-methods study of an HIV prevention programme in South Africa. Sport Soc. 2015, 18, 1009–1022. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Merrill, K.G.; Merrill, J.C.; Hershow, R.B.; Barkley, C.; Rakosa, B.; DeCelles, J.; Harrison, A. Linking at-risk South African girls to sexual violence and reproductive health services: A mixed-methods assessment of a soccer-based HIV prevention program and pilot SMS campaign. Eval. Program Plan. 2018, 70, 12–24. [Google Scholar] [CrossRef]
- Sallis, J.; Owen, N.; Fisher, E. Ecological Models of Health Behavior. In Health Behavior and Health Education: Theory, Research, and Practice, 4th ed.; Glanz, K., Rimer, B.K., Viswanath, K., Eds.; Jossey-Bass: San Francisco, CA, USA, 2008; pp. 465–485. [Google Scholar]
- Fetters, M.D.; Curry, L.A.; Creswell, J.W. Achieving Integration in Mixed Methods Designs-Principles and Practices. Health Serv. Res. 2013, 48, 2134–2156. [Google Scholar] [CrossRef] [Green Version]
- Alvidrez, J.; Castille, D.; Laude-Sharp, M.; Rosario, A.; Tabor, D. The National Institute on Minority Health and Health Disparities Research Framework. Am. J. Public Health 2019, 109, S16–S20. [Google Scholar] [CrossRef]
- Hopkins, C.S.; Hopkins, C.; Kanny, S.; Watson, A. A Systematic Review of Factors Associated with Sport Participation among Adolescent Females. Int. J. Environ. Res. Public Health 2022, 19, 3353. [Google Scholar] [CrossRef]
- Westerbeek, H.; Eime, R. The Physical Activity and Sport Participation Framework—A Policy Model Toward Being Physically Active Across the Lifespan. Front. Sports Act. Living 2021, 3, 608593. [Google Scholar] [CrossRef] [PubMed]
- UN Women Intersectional Feminism: What it Means and Why it Matters Right Now. UN Women 2020. Available online: https://www.unwomen.org/en/news/stories/2020/6/explainer-intersectional-feminism-what-it-means-and-why-it-matters (accessed on 1 September 2022).
- Válková, E. ‘You’re going to teach my son to be viado’: From ‘girling’ to queering sport for development? Int. Rev. Sociol. Sport 2020, 56, 97–113. [Google Scholar] [CrossRef]
- Murray, K. Sport Across Cultures: Applications of the Human Capital Model in Refugee Communities. J. Phys. Act. Health 2014, 11, 681–682. [Google Scholar] [CrossRef] [Green Version]
- Hirvensalo, M.; Lintunen, T. Life-course perspective for physical activity and sports participation. Eur. Rev. Aging Phys. Act. 2011, 8, 13–22. [Google Scholar] [CrossRef] [Green Version]
- Hightow-Weidman, L.B.; Horvath, K.J.; Scott, H.; Hill-Rorie, J.; Bauermeister, J.A. Engaging youth in mHealth: What works and how can we be sure? mHealth 2021, 7, 23. [Google Scholar] [CrossRef] [PubMed]
- Gibbs, L.; Kornbluh, M.; Marinkovic, K.; Bell, S.; Ozer, E.J. Using Technology to Scale up Youth-Led Participatory Action Research: A Systematic Review. J. Adolesc. Health 2020, 67, S14–S23. [Google Scholar] [CrossRef]
- McCool, J.; Dobson, R.; Whittaker, R.; Paton, C. Mobile Health (mHealth) in Low- and Middle-Income Countries. Annu. Rev. Public Health 2022, 43, 525–539. [Google Scholar] [CrossRef]
- Gunasekeran, D.V.; Tseng, R.M.W.W.; Tham, Y.-C.; Wong, T.Y. Applications of digital health for public health responses to COVID-19: A systematic scoping review of artificial intelligence, telehealth and related technologies. NPJ Digit. Med. 2021, 4, 40. [Google Scholar] [CrossRef]
- Figueroa, C.A.; Luo, T.; Aguilera, A.; Lyles, C.R. The need for feminist intersectionality in digital health. Lancet Digit. Health 2021, 3, e526–e533. [Google Scholar] [CrossRef]
- Graham, S.C.; Zha, C.C.; King, A.W.; Banchoff, A.; Sarnquist, C.; Dauber, M.; Baiocchi, M. A Novel Model for Generating Creative, Community-Responsive Interventions to Reduce Gender-Based Violence on College Campuses. Int. J. Environ. Res. Public Health 2021, 18, 7933. [Google Scholar] [CrossRef] [PubMed]
- King, A.C.; King, D.K.; Banchoff, A.; Solomonov, S.; Ben Natan, O.; Hua, J.; Gardiner, P.; Rosas, L.G.; Espinosa, P.R.; Winter, S.J.; et al. Employing Participatory Citizen Science Methods to Promote Age-Friendly Environments Worldwide. Int. J. Environ. Res. Public Health 2020, 17, 1541. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- King, A.C.; Winter, S.J.; Chrisinger, B.W.; Hua, J.; Banchoff, A.W. Maximizing the promise of citizen science to advance health and prevent disease. Prev. Med. 2018, 119, 44–47. [Google Scholar] [CrossRef]
- Pedersen, M.; Wood, G.E.R.; Fernes, P.K.; Rosas, L.G.; Banchoff, A.; King, A.C. The “Our Voice” Method: Participatory Action Citizen Science Research to Advance Behavioral Health and Health Equity Outcomes. Int. J. Environ. Res. Public Health 2022, 19, 14773. [Google Scholar] [CrossRef] [PubMed]
- Nienhuis, C.P.; Lesser, I.A. The Impact of COVID-19 on Women’s Physical Activity Behavior and Mental Well-Being. Int. J. Environ. Res. Public Health 2020, 17, 9036. [Google Scholar] [CrossRef]


{kind=link}
| Domain | Inclusion Criteria | Exclusion Criteria |
|---|---|---|
| Participants |
|
|
| Concept |
|
|
| Context |
|
|
| Type of studies |
|
|
| Author, Year | Country | Health-Related Focus of Study | Participants | Intervention | Design, Method of Data Collection |
|---|---|---|---|---|---|
| Cislaghi (2020) [38] | India | Impact of kabaddi-based intervention (Parivartan for Girls) on gender-related social norms to prevent child marriage | Girls ages 12–16 years old (n = 15) | Duration of 15-months; Group-based, outside of school; facilitated by local, trained near-peer female mentors (20–24 years old); 2 sessions per week, 1.5 h each, including one session of life skills and gender training 1 session for playing kabaddi; Plus 2 public tournaments | Prospective qualitative research design, semi-structured interviews with participants only at two time points: 6 and 12 months; Field notes and observations |
| Collumbien (2019) [39] | India | Practice-based learnings and impact from the development and implementation of Parivartan for Girls | Same as above | Same as above | Longitudinal design, semi-structured interviews with participants (n = 15) and intervention mentors (n = 10) at three timepoints: 6 & 12 months, 1-year post-intervention; Field notes and observations |
| Hershow (2015) [40] | South Africa | Impact of soccer-based intervention (SKILLZ Street) to address three aims: (1) Increase self-efficacy to avoid risky sexual behavior; (2) Increase belief in gender equitable norms; (3) Facilitate access and uptake of HIV counseling and testing services | Girls ages 11–14 years old (n = 4260) | Duration of 6-weeks; Group-based, after school; facilitated by local, trained near-peer female coaches; 2 sessions per week, 2 h each, including a life skills activity, a non-competitive soccer match, and informal ‘team time’ facilitated by coaches | Mixed methods design. Quantitative data: program attendance, HIV testing rate, pre/post questionnaire (n = 514) on HIV-related knowledge, attitudes, and communication. Qualitative data: focus groups with participants (n = 11 groups) and coaches (n = 5 groups) |
| Merrill (2018) [41] | South Africa | Same as above, plus evaluation of SMS-based component and implementation factors | Girls ages 11–16 years old (n = 394) | Same as above, but delivered across 5-weeks, with intervention content revise to add focus on gender-based violence, and addition of a two-way SMS-campaign | Convergent parallel mixed-methods design. Quantitative data: program attendance, SMS campaign platform usage, pre/post questionnaire. Qualitative: focus groups with participants (n = 3 groups), parents of participants (n = 2 groups), coaches (n = 1 group); individual interviews (n = 4) with parents of participants and a social worker engaged in project. Structured observation and fidelity checks |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pedersen, M.; King, A.C. How Can Sport-Based Interventions Improve Health among Women and Girls? A Scoping Review. Int. J. Environ. Res. Public Health 2023, 20, 4818. https://doi.org/10.3390/ijerph20064818
Pedersen M, King AC. How Can Sport-Based Interventions Improve Health among Women and Girls? A Scoping Review. International Journal of Environmental Research and Public Health. 2023; 20(6):4818. https://doi.org/10.3390/ijerph20064818
Chicago/Turabian StylePedersen, Maja, and Abby C. King. 2023. "How Can Sport-Based Interventions Improve Health among Women and Girls? A Scoping Review" International Journal of Environmental Research and Public Health 20, no. 6: 4818. https://doi.org/10.3390/ijerph20064818