
Use of Wearable Activity-Monitoring Technologies to Promote Physical Activity in Cancer Survivors: Challenges and Opportunities for Improved Cancer Care
 , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Identification of the Research Question
- What is the scope and acceptability of the use of wearable activity monitors for individuals with cancer?
- Does the use of a wearable activity monitor motivate gains in PA behaviors in cancer survivors?
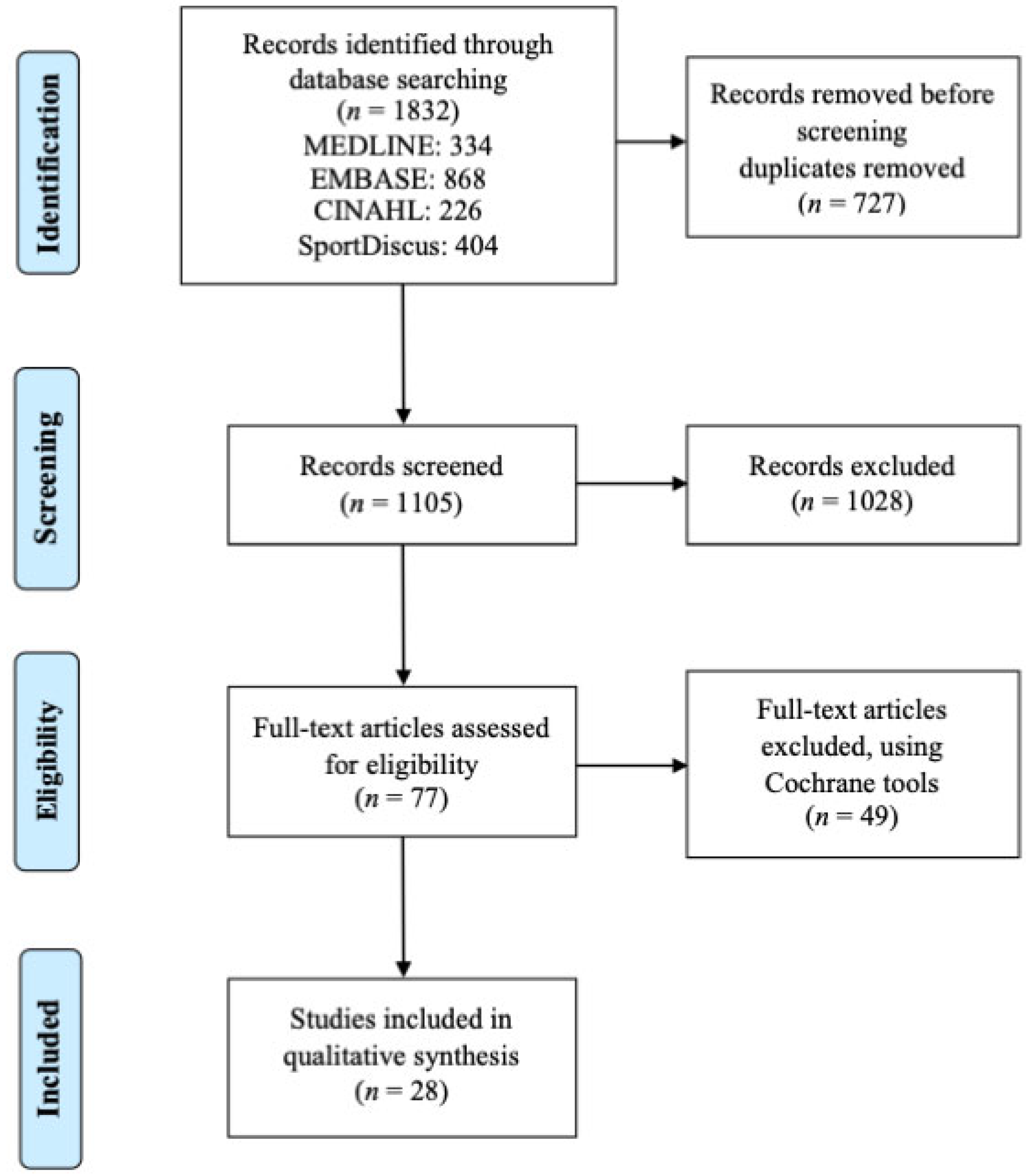
2.3. Identification of Relevant Articles
2.4. Selection of Relevant Articles for Review
2.5. Charting the Data
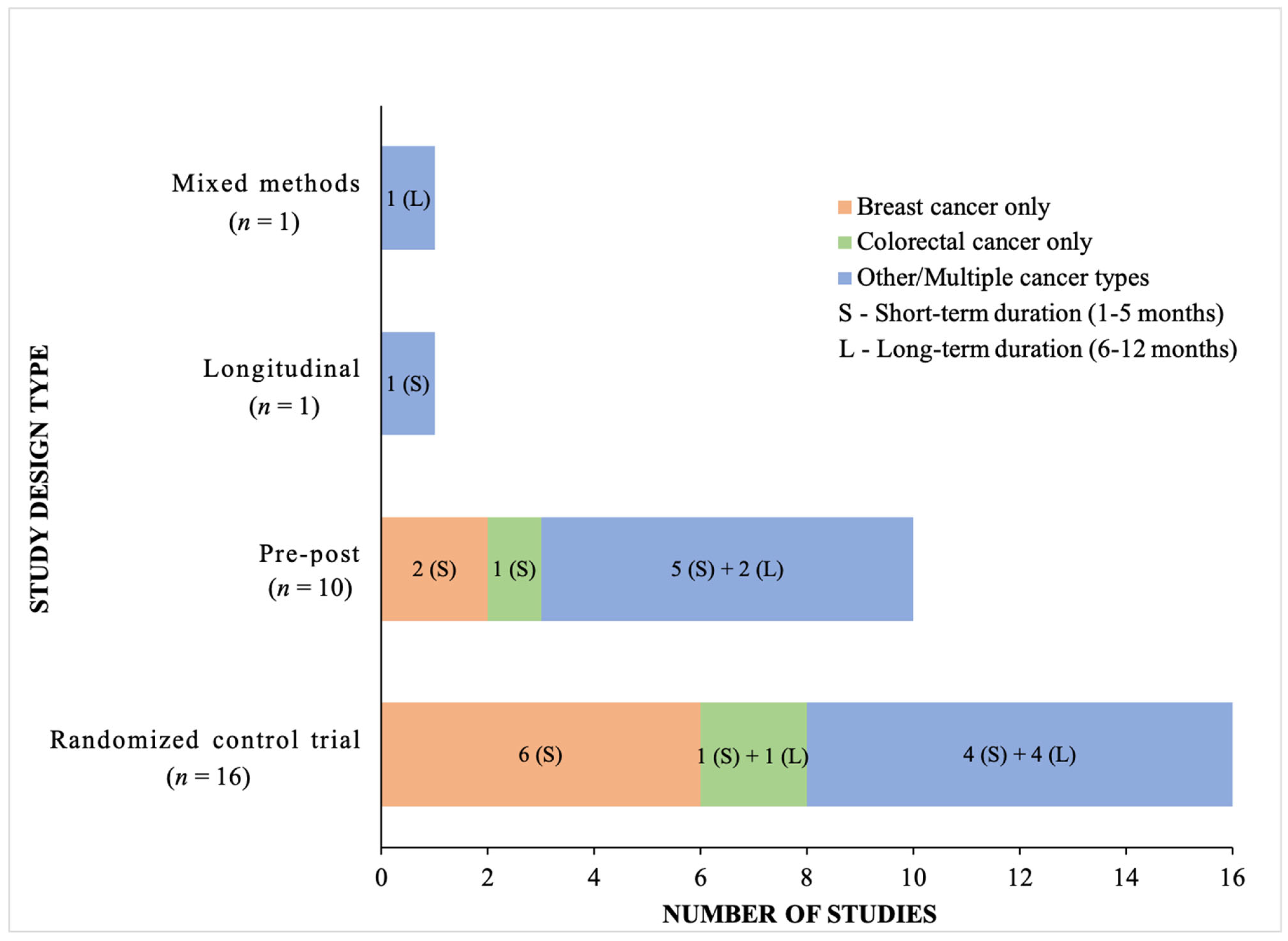
3. Results
4. Discussion
5. Conclusions and Future Directions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Miller, K.D.; Siegel, R.L.; Lin, C.C.; Mariotto, A.B.; Kramer, J.L.; Rowland, J.H.; Stein, K.D.; Alteri, R.; Jemal, A. Cancer Treatment and Survivorship Statistics, 2016. CA Cancer J. Clin. 2016, 66, 271–289. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- World Cancer Report 2014; Stewart, B.W.; Wild, C.; International Agency for Research on Cancer; World Health Organization (Eds.) International Agency for Research on Cancer: Lyon, France, 2014; ISBN 978-92-832-0429-9. [Google Scholar]
- Rowland, J.H.; Bellizzi, K.M. Cancer Survivorship Issues: Life After Treatment and Implications for an Aging Population. JCO 2014, 32, 2662–2668. [Google Scholar] [CrossRef] [Green Version]
- Weaver, K.E.; Forsythe, L.P.; Reeve, B.B.; Alfano, C.M.; Rodriguez, J.L.; Sabatino, S.A.; Hawkins, N.A.; Rowland, J.H. Mental and Physical Health–Related Quality of Life among U.S. Cancer Survivors: Population Estimates from the 2010 National Health Interview Survey. Cancer Epidemiol. Biomark. Prev. 2012, 21, 2108–2117. [Google Scholar] [CrossRef] [Green Version]
- Rock, C.L.; Thomson, C.A.; Sullivan, K.R.; Howe, C.L.; Kushi, L.H.; Caan, B.J.; Neuhouser, M.L.; Bandera, E.V.; Wang, Y.; Robien, K.; et al. American Cancer Society Nutrition and Physical Activity Guideline for Cancer Survivors. CA Cancer J. Clin. 2022, 72, 230–262. [Google Scholar] [CrossRef]
- Ferioli, M.; Zauli, G.; Martelli, A.M.; Vitale, M.; McCubrey, J.A.; Ultimo, S.; Capitani, S.; Neri, L.M. Impact of Physical Exercise in Cancer Survivors during and after Antineoplastic Treatments. Oncotarget 2018, 9, 14005–14034. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, Y.; Song, H.; Yin, Y.; Feng, L. Cancer Survivors Could Get Survival Benefits from Postdiagnosis Physical Activity: A Meta-Analysis. Evid. Based Complement. Altern. Med. 2019, 2019, 1940903. [Google Scholar] [CrossRef]
- Hayes, S.C.; Newton, R.U.; Spence, R.R.; Galvão, D.A. The Exercise and Sports Science Australia Position Statement: Exercise Medicine in Cancer Management. J. Sci. Med. Sport 2019, 22, 1175–1199. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cormie, P.; Atkinson, M.; Bucci, L.; Cust, A.; Eakin, E.; Hayes, S.; McCarthy, A.L.; Murnane, A.; Patchell, S.; Adams, D. Clinical Oncology Society of Australia Position Statement on Exercise in Cancer Care. Med. J. Aust. 2018, 209, 184–187. [Google Scholar] [CrossRef] [Green Version]
- Choy, K.T.; Lam, K.; Kong, J.C. Exercise and Colorectal Cancer Survival: An Updated Systematic Review and Meta-Analysis. Int. J. Color. Dis. 2022, 37, 1751–1758. [Google Scholar] [CrossRef]
- Ashcraft, K.A.; Warner, A.B.; Jones, L.W.; Dewhirst, M.W. Exercise as Adjunct Therapy in Cancer. Semin. Radiat. Oncol. 2019, 29, 16–24. [Google Scholar] [CrossRef]
- Campbell, K.L.; Winters-Stone, K.M.; Wiskemann, J.; May, A.M.; Schwartz, A.L.; Courneya, K.S.; Zucker, D.S.; Matthews, C.E.; Ligibel, J.A.; Gerber, L.H.; et al. Exercise Guidelines for Cancer Survivors: Consensus Statement from International Multidisciplinary Roundtable. Med. Sci. Sport. Exerc. 2019, 51, 2375–2390. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Courneya, K.S.; Friedenreich, C.M. Physical Activity and Cancer: An Introduction. In Physical Activity and Cancer; Courneya, K.S., Friedenreich, C.M., Eds.; Recent Results in Cancer Research; Springer: Berlin/Heidelberg, Germany, 2010; Volume 186, pp. 1–10. ISBN 978-3-642-04230-0. [Google Scholar]
- Pinto, B.M.; Ciccolo, J.T. Physical Activity Motivation and Cancer Survivorship. In Physical Activity and Cancer; Courneya, K.S., Friedenreich, C.M., Eds.; Recent Results in Cancer Research; Springer: Berlin/Heidelberg, Germany, 2010; Volume 186, pp. 367–387. ISBN 978-3-642-04230-0. [Google Scholar]
- LeMasters, T.J.; Madhavan, S.S.; Sambamoorthi, U.; Kurian, S. Health Behaviors among Breast, Prostate, and Colorectal Cancer Survivors: A US Population-Based Case-Control Study, with Comparisons by Cancer Type and Gender. J. Cancer Surviv. 2014, 8, 336–348. [Google Scholar] [CrossRef] [PubMed]
- Mowls, D.S.; Brame, L.S.; Martinez, S.A.; Beebe, L.A. Lifestyle Behaviors among US Cancer Survivors. J. Cancer Surviv. 2016, 10, 692–698. [Google Scholar] [CrossRef] [PubMed]
- Neil, S.E.; Gotay, C.C.; Campbell, K.L. Physical Activity Levels of Cancer Survivors in Canada: Findings from the Canadian Community Health Survey. J. Cancer Surviv. 2014, 8, 143–149. [Google Scholar] [CrossRef]
- Husebø, A.M.L.; Dyrstad, S.M.; Søreide, J.A.; Bru, E. Predicting Exercise Adherence in Cancer Patients and Survivors: A Systematic Review and Meta-Analysis of Motivational and Behavioural Factors. J. Clin. Nurs. 2013, 22, 4–21. [Google Scholar] [CrossRef]
- Courneya, K.S.; Stevinson, C.; Mcneely, M.L.; Sellar, C.M.; Friedenreich, C.M.; Peddle-Mcintyre, C.J.; Chua, N.; Reiman, T. Effects of Supervised Exercise on Motivational Outcomes and Longer-Term Behavior. Med. Sci. Sport. Exerc. 2012, 44, 542–549. [Google Scholar] [CrossRef] [PubMed]
- Trinh, L.; Plotnikoff, R.C.; Rhodes, R.E.; North, S.; Courneya, K.S. Feasibility and Preliminary Efficacy of Adding Behavioral Counseling to Supervised Physical Activity in Kidney Cancer Survivors: A Randomized Controlled Trial. Cancer Nurs. 2014, 37, E8–E22. [Google Scholar] [CrossRef]
- Bluethmann, S.M.; Vernon, S.W.; Gabriel, K.P.; Murphy, C.C.; Bartholomew, L.K. Taking the next Step: A Systematic Review and Meta-Analysis of Physical Activity and Behavior Change Interventions in Recent Post-Treatment Breast Cancer Survivors. Breast Cancer Res. Treat. 2015, 149, 331–342. [Google Scholar] [CrossRef] [Green Version]
- Stacey, F.G.; James, E.L.; Chapman, K.; Courneya, K.S.; Lubans, D.R. A Systematic Review and Meta-Analysis of Social Cognitive Theory-Based Physical Activity and/or Nutrition Behavior Change Interventions for Cancer Survivors. J. Cancer Surviv. 2015, 9, 305–338. [Google Scholar] [CrossRef] [Green Version]
- Connelly, J.; Kirk, A.; Masthoff, J.; MacRury, S. The Use of Technology to Promote Physical Activity in Type 2 Diabetes Management: A Systematic Review. Diabet. Med. 2013, 30, 1420–1432. [Google Scholar] [CrossRef]
- Davies, C.A.; Spence, J.C.; Vandelanotte, C.; Caperchione, C.M.; Mummery, W. Meta-Analysis of Internet-Delivered Interventions to Increase Physical Activity Levels. Int. J. Behav. Nutr. Phys. Act. 2012, 9, 52. [Google Scholar] [CrossRef] [Green Version]
- Kuijpers, W.; Groen, W.G.; Aaronson, N.K.; van Harten, W.H. A Systematic Review of Web-Based Interventions for Patient Empowerment and Physical Activity in Chronic Diseases: Relevance for Cancer Survivors. J. Med. Internet Res. 2013, 15, e37. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vandelanotte, C.; Kirwan, M.; Rebar, A.; Alley, S.; Short, C.; Fallon, L.; Buzza, G.; Schoeppe, S.; Maher, C.; Duncan, M.J. Examining the Use of Evidence-Based and Social Media Supported Tools in Freely Accessible Physical Activity Intervention Websites. Int. J. Behav. Nutr. Phys. Act. 2014, 11, 105. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vandelanotte, C.; Spathonis, K.M.; Eakin, E.G.; Owen, N. Website-Delivered Physical Activity Interventions. Am. J. Prev. Med. 2007, 33, 54–64. [Google Scholar] [CrossRef]
- Jennings, C.A.; Vandelanotte, C.; Caperchione, C.M.; Mummery, W.K. Effectiveness of a Web-Based Physical Activity Intervention for Adults with Type 2 Diabetes—A Randomised Controlled Trial. Prev. Med. 2014, 60, 33–40. [Google Scholar] [CrossRef]
- Kohl, L.F.; Crutzen, R.; de Vries, N.K. Online Prevention Aimed at Lifestyle Behaviors: A Systematic Review of Reviews. J. Med. Internet Res. 2013, 15, e146. [Google Scholar] [CrossRef] [Green Version]
- Singleton, A.C.; Raeside, R.; Hyun, K.K.; Partridge, S.R.; Di Tanna, G.L.; Hafiz, N.; Tu, Q.; Tat-Ko, J.; Sum, S.C.M.; Sherman, K.A.; et al. Electronic Health Interventions for Patients with Breast Cancer: Systematic Review and Meta-Analyses. JCO 2022, 40, 2257–2270. [Google Scholar] [CrossRef]
- Alley, S.; Schoeppe, S.; Guertler, D.; Jennings, C.; Duncan, M.J.; Vandelanotte, C. Interest and Preferences for Using Advanced Physical Activity Tracking Devices: Results of a National Cross-Sectional Survey. BMJ Open 2016, 6, e011243. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lewis, Z.H.; Lyons, E.J.; Jarvis, J.M.; Baillargeon, J. Using an Electronic Activity Monitor System as an Intervention Modality: A Systematic Review. BMC Public Health 2015, 15, 585. [Google Scholar] [CrossRef] [Green Version]
- Healthcare—Apple Watch. Available online: https://www.apple.com/ca/healthcare/apple-watch/ (accessed on 1 March 2023).
- Fitbit Official Site for Activity Trackers & More. Available online: https://www.fitbit.com/global/en-ca/home (accessed on 1 March 2023).
- Garmin|Canada. Available online: https://www.garmin.com/en-CA/ (accessed on 1 March 2023).
- Mercer, K.; Li, M.; Giangregorio, L.; Burns, C.; Grindrod, K. Behavior Change Techniques Present in Wearable Activity Trackers: A Critical Analysis. JMIR mHealth uHealth 2016, 4, e40. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lyons, E.J.; Lewis, Z.H.; Mayrsohn, B.G.; Rowland, J.L. Behavior Change Techniques Implemented in Electronic Lifestyle Activity Monitors: A Systematic Content Analysis. J. Med. Internet Res. 2014, 16, e192. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Singh, B.; Zopf, E.M.; Howden, E.J. Effect and Feasibility of Wearable Physical Activity Trackers and Pedometers for Increasing Physical Activity and Improving Health Outcomes in Cancer Survivors: A Systematic Review and Meta-Analysis. J. Sport Health Sci. 2022, 11, 184–193. [Google Scholar] [CrossRef] [PubMed]
- Arksey, H.; O’Malley, L. Scoping Studies: Towards a Methodological Framework. Int. J. Soc. Res. Methodol. 2005, 8, 19–32. [Google Scholar] [CrossRef] [Green Version]
- Levac, D.; Colquhoun, H.; O’Brien, K.K. Scoping Studies: Advancing the Methodology. Implement. Sci. 2010, 5, 69. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Higgins, J.P.T.; Altman, D.G.; Gotzsche, P.C.; Juni, P.; Moher, D.; Oxman, A.D.; Savovic, J.; Schulz, K.F.; Weeks, L.; Sterne, J.A.C.; et al. The Cochrane Collaboration’s Tool for Assessing Risk of Bias in Randomised Trials. BMJ 2011, 343, d5928. [Google Scholar] [CrossRef] [Green Version]
- Blount, D.S.; McDonough, D.J.; Gao, Z. Effect of Wearable Technology-Based Physical Activity Interventions on Breast Cancer Survivors’ Physiological, Cognitive, and Emotional Outcomes: A Systematic Review. J. Clin. Med. 2021, 10, 2015. [Google Scholar] [CrossRef]
- Tang, M.S.S.; Moore, K.; McGavigan, A.; Clark, R.A.; Ganesan, A.N. Effectiveness of Wearable Trackers on Physical Activity in Healthy Adults: Systematic Review and Meta-Analysis of Randomized Controlled Trials. JMIR mHealth uHealth 2020, 8, e15576. [Google Scholar] [CrossRef]
- Brown, J.C.; Rhim, A.D.; Manning, S.L.; Brennan, L.; Mansour, A.I.; Rustgi, A.K.; Damjanov, N.; Troxel, A.B.; Rickels, M.R.; Ky, B.; et al. Effects of Exercise on Circulating Tumor Cells among Patients with Resected Stage I-III Colon Cancer. PLoS ONE 2018, 13, e0204875. [Google Scholar] [CrossRef] [Green Version]
- Cadmus-Bertram, L.; Tevaarwerk, A.J.; Sesto, M.E.; Gangnon, R.; Van Remortel, B.; Date, P. Building a Physical Activity Intervention into Clinical Care for Breast and Colorectal Cancer Survivors in Wisconsin: A Randomized Controlled Pilot Trial. J. Cancer Surviv. 2019, 13, 593–602. [Google Scholar] [CrossRef] [PubMed]
- Chan, J.M.; Van Blarigan, E.L.; Langlais, C.S.; Zhao, S.; Ramsdill, J.W.; Daniel, K.; Macaire, G.; Wang, E.; Paich, K.; Kessler, E.R.; et al. Feasibility and Acceptability of a Remotely Delivered, Web-Based Behavioral Intervention for Men with Prostate Cancer: Four-Arm Randomized Controlled Pilot Trial. J. Med. Internet Res. 2020, 22, e19238. [Google Scholar] [CrossRef]
- Cheong, I.Y.; An, S.Y.; Cha, W.C.; Rha, M.Y.; Kim, S.T.; Chang, D.K.; Hwang, J.H. Efficacy of Mobile Health Care Application and Wearable Device in Improvement of Physical Performance in Colorectal Cancer Patients Undergoing Chemotherapy. Clin. Color. Cancer 2018, 17, e353–e362. [Google Scholar] [CrossRef] [PubMed]
- Ferrante, J.M.; Lulla, A.; Williamson, J.D.; Devine, K.A.; Ohman-Strickland, P.; Bandera, E.V. Patterns of Fitbit Use and Activity Levels Among African American Breast Cancer Survivors During an EHealth Weight Loss Randomized Controlled Trial. Am. J. Health Promot. 2022, 36, 94–105. [Google Scholar] [CrossRef]
- Finley, D.J.; Fay, K.A.; Batsis, J.A.; Stevens, C.J.; Sacks, O.A.; Darabos, C.; Cook, S.B.; Lyons, K.D. A Feasibility Study of an Unsupervised, Pre-operative Exercise Program for Adults with Lung Cancer. Eur. J. Cancer Care 2020, 29, e13254. [Google Scholar] [CrossRef] [PubMed]
- Gehring, K.; Kloek, C.J.; Aaronson, N.K.; Janssen, K.W.; Jones, L.W.; Sitskoorn, M.M.; Stuiver, M.M. Feasibility of a Home-Based Exercise Intervention with Remote Guidance for Patients with Stable Grade II and III Gliomas: A Pilot Randomized Controlled Trial. Clin. Rehabil. 2018, 32, 352–366. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gell, N.M.; Grover, K.W.; Humble, M.; Sexton, M.; Dittus, K. Efficacy, Feasibility, and Acceptability of a Novel Technology-Based Intervention to Support Physical Activity in Cancer Survivors. Support. Care Cancer 2017, 25, 1291–1300. [Google Scholar] [CrossRef] [PubMed]
- Granger, C.L.; Irving, L.; Antippa, P.; Edbrooke, L.; Parry, S.M.; Krishnasamy, M.; Denehy, L. CAPACITY: A Physical Activity Self-Management Program for Patients Undergoing Surgery for Lung Cancer, a Phase I Feasibility Study. Lung Cancer 2018, 124, 102–109. [Google Scholar] [CrossRef]
- Groarke, J.M.; Richmond, J.; Mc Sharry, J.; Groarke, A.; Harney, O.M.; Kelly, M.G.; Walsh, J.C. Acceptability of a Mobile Health Behavior Change Intervention for Cancer Survivors with Obesity or Overweight: Nested Mixed Methods Study within a Randomized Controlled Trial. JMIR mHealth uHealth 2021, 9, e18288. [Google Scholar] [CrossRef]
- Hardcastle, S.J.; Jiménez-Castuera, R.; Maxwell-Smith, C.; Bulsara, M.K.; Hince, D. Fitbit Wear-Time and Patterns of Activity in Cancer Survivors throughout a Physical Activity Intervention and Follow-up: Exploratory Analysis from a Randomised Controlled Trial. PLoS ONE 2020, 15, e0240967. [Google Scholar] [CrossRef]
- Hartman, S.J.; Nelson, S.H.; Weiner, L.S. Patterns of Fitbit Use and Activity Levels Throughout a Physical Activity Intervention: Exploratory Analysis from a Randomized Controlled Trial. JMIR mHealth uHealth 2018, 6, e29. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kanzawa-Lee, G.A.; Ploutz-Snyder, R.J.; Larson, J.L.; Krauss, J.C.; Resnicow, K.; Lavoie Smith, E.M. Efficacy of the Motivational Interviewing-Walk Intervention for Chemotherapy-Induced Peripheral Neuropathy and Quality of Life During Oxaliplatin Treatment: A Pilot Randomized Controlled Trial. Cancer Nurs. 2022, 45, E531–E544. [Google Scholar] [CrossRef]
- Kenfield, S.A.; Van Blarigan, E.L.; Ameli, N.; Lavaki, E.; Cedars, B.; Paciorek, A.T.; Monroy, C.; Tantum, L.K.; Newton, R.U.; Signorell, C.; et al. Feasibility, Acceptability, and Behavioral Outcomes from a Technology-Enhanced Behavioral Change Intervention (Prostate 8): A Pilot Randomized Controlled Trial in Men with Prostate Cancer. Eur. Urol. 2019, 75, 950–958. [Google Scholar] [CrossRef] [PubMed]
- Kim, Y.; Seo, J.; An, S.-Y.; Sinn, D.H.; Hwang, J.H. Efficacy and Safety of an MHealth App and Wearable Device in Physical Performance for Patients with Hepatocellular Carcinoma: Development and Usability Study. JMIR mHealth uHealth 2020, 8, e14435. [Google Scholar] [CrossRef]
- Low, C.A.; Danko, M.; Durica, K.C.; Kunta, A.R.; Mulukutla, R.; Ren, Y.; Bartlett, D.L.; Bovbjerg, D.H.; Dey, A.K.; Jakicic, J.M. A Real-Time Mobile Intervention to Reduce Sedentary Behavior Before and After Cancer Surgery: Usability and Feasibility Study. JMIR Perioper Med. 2020, 3, e17292. [Google Scholar] [CrossRef] [PubMed]
- Lynch, B.M.; Nguyen, N.H.; Moore, M.M.; Reeves, M.M.; Rosenberg, D.E.; Boyle, T.; Vallance, J.K.; Milton, S.; Friedenreich, C.M.; English, D.R. A Randomized Controlled Trial of a Wearable Technology-based Intervention for Increasing Moderate to Vigorous Physical Activity and Reducing Sedentary Behavior in Breast Cancer Survivors: The ACTIVATE Trial. Cancer 2019, 125, 2846–2855. [Google Scholar] [CrossRef] [PubMed]
- Lynch, B.M.; Nguyen, N.H.; Moore, M.M.; Reeves, M.M.; Rosenberg, D.E.; Boyle, T.; Milton, S.; Friedenreich, C.M.; Vallance, J.K.; English, D.R. Maintenance of Physical Activity and Sedentary Behavior Change, and Physical Activity and Sedentary Behavior Change after an Abridged Intervention: Secondary Outcomes from the ACTIVATE Trial. Cancer 2019, 125, 2856–2860. [Google Scholar] [CrossRef] [PubMed]
- Marthick, M.; Dhillon, H.M.; Alison, J.A.; Cheema, B.S.; Shaw, T. An Interactive Web Portal for Tracking Oncology Patient Physical Activity and Symptoms: Prospective Cohort Study. JMIR Cancer 2018, 4, e11978. [Google Scholar] [CrossRef]
- Maxwell-Smith, C.; Hince, D.; Cohen, P.A.; Bulsara, M.K.; Boyle, T.; Platell, C.; Tan, P.; Levitt, M.; Salama, P.; Tan, J.; et al. A Randomized Controlled Trial of WATAAP to Promote Physical Activity in Colorectal and Endometrial Cancer Survivors. Psycho Oncol. 2019, 28, 1420–1429. [Google Scholar] [CrossRef]
- Rastogi, S.; Tevaarwerk, A.J.; Sesto, M.; Van Remortel, B.; Date, P.; Gangnon, R.; Thraen-Borowski, K.; Cadmus-Bertram, L. Effect of a Technology-supported Physical Activity Intervention on Health-related Quality of Life, Sleep, and Processes of Behavior Change in Cancer Survivors: A Randomized Controlled Trial. Psycho Oncol. 2020, 29, 1917–1926. [Google Scholar] [CrossRef] [PubMed]
- Schrier, E.; Xiong, N.; Thompson, E.; Poort, H.; Schumer, S.; Liu, J.F.; Krasner, C.; Campos, S.M.; Horowitz, N.S.; Feltmate, C.; et al. Stepping into Survivorship Pilot Study: Harnessing Mobile Health and Principles of Behavioral Economics to Increase Physical Activity in Ovarian Cancer Survivors. Gynecol. Oncol. 2021, 161, 581–586. [Google Scholar] [CrossRef]
- Singh, B.; Spence, R.R.; Sandler, C.X.; Tanner, J.; Hayes, S.C. Feasibility and Effect of a Physical Activity Counselling Session with or without Provision of an Activity Tracker on Maintenance of Physical Activity in Women with Breast Cancer—A Randomised Controlled Trial. J. Sci. Med. Sport 2020, 23, 283–290. [Google Scholar] [CrossRef] [Green Version]
- Uhm, K.E.; Yoo, J.S.; Chung, S.H.; Lee, J.D.; Lee, I.; Kim, J.I.; Lee, S.K.; Nam, S.J.; Park, Y.H.; Lee, J.Y.; et al. Effects of Exercise Intervention in Breast Cancer Patients: Is Mobile Health (MHealth) with Pedometer More Effective than Conventional Program Using Brochure? Breast Cancer Res. Treat. 2017, 161, 443–452. [Google Scholar] [CrossRef] [PubMed]
- Van Blarigan, E.L.; Chan, H.; Van Loon, K.; Kenfield, S.A.; Chan, J.M.; Mitchell, E.; Zhang, L.; Paciorek, A.; Joseph, G.; Laffan, A.; et al. Self-Monitoring and Reminder Text Messages to Increase Physical Activity in Colorectal Cancer Survivors (Smart Pace): A Pilot Randomized Controlled Trial. BMC Cancer 2019, 19, 218. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, Y.-J.; Boehmke, M.; Wu, Y.-W.B.; Dickerson, S.S.; Fisher, N. Effects of a 6-Week Walking Program on Taiwanese Women Newly Diagnosed with Early-Stage Breast Cancer. Cancer Nurs. 2011, 34, E1–E13. [Google Scholar] [CrossRef]
- Zeng, N.; Liao, N.; Han, C.; Liu, W.; Gao, Z. Leveraging Fitness Tracker and Personalized Exercise Prescription to Promote Breast Cancer Survivors’ Health Outcomes: A Feasibility Study. JCM 2020, 9, 1775. [Google Scholar] [CrossRef] [PubMed]
- Zhang, X.; McClean, D.; Ko, E.; Morgan, M.; Schmitz, K. Exercise Among Women with Ovarian Cancer: A Feasibility and Pre-/Post-Test Exploratory Pilot Study. ONF 2017, 44, 366–374. [Google Scholar] [CrossRef] [Green Version]
- Vallance, J.; Spark, L.; Eakin, E. Exercise Behavior, Motivation, and Maintenance Among Cancer Survivors. In Exercise, Energy Balance, and Cancer; Ulrich, C.M., Steindorf, K., Berger, N.A., Eds.; Springer: New York, NY, USA, 2013; pp. 215–231. ISBN 978-1-4614-4492-3. [Google Scholar]
- Michie, S.; Abraham, C.; Whittington, C.; McAteer, J.; Gupta, S. Effective Techniques in Healthy Eating and Physical Activity Interventions: A Meta-Regression. Health Psychol. 2009, 28, 690–701. [Google Scholar] [CrossRef] [Green Version]
- Michie, S.; Richardson, M.; Johnston, M.; Abraham, C.; Francis, J.; Hardeman, W.; Eccles, M.P.; Cane, J.; Wood, C.E. The Behavior Change Technique Taxonomy (v1) of 93 Hierarchically Clustered Techniques: Building an International Consensus for the Reporting of Behavior Change Interventions. Ann. Behav. Med. 2013, 46, 81–95. [Google Scholar] [CrossRef]
- Bravata, D.M.; Smith-Spangler, C.; Sundaram, V.; Gienger, A.L.; Lin, N.; Lewis, R.; Stave, C.D.; Olkin, I.; Sirard, J.R. Using Pedometers to Increase Physical Activity and Improve Health: A Systematic Review. JAMA 2007, 298, 2296. [Google Scholar] [CrossRef]
- Tudor-Locke, C.; Lutes, L. Why Do Pedometers Work? A Reflection upon the Factors Related to Successfully Increasing Physical Activity. Sport. Med. 2009, 39, 981–993. [Google Scholar] [CrossRef]
- Buffart, L.M.; Galvão, D.A.; Brug, J.; Chinapaw, M.J.M.; Newton, R.U. Evidence-Based Physical Activity Guidelines for Cancer Survivors: Current Guidelines, Knowledge Gaps and Future Research Directions. Cancer Treat. Rev. 2014, 40, 327–340. [Google Scholar] [CrossRef]
- Årsand, E.; Muzny, M.; Bradway, M.; Muzik, J.; Hartvigsen, G. Performance of the First Combined Smartwatch and Smartphone Diabetes Diary Application Study. J. Diabetes Sci. Technol. 2015, 9, 556–563. [Google Scholar] [CrossRef] [Green Version]
- Mercer, K.; Giangregorio, L.; Schneider, E.; Chilana, P.; Li, M.; Grindrod, K. Acceptance of Commercially Available Wearable Activity Trackers Among Adults Aged Over 50 and with Chronic Illness: A Mixed-Methods Evaluation. JMIR mHealth uHealth 2016, 4, e7. [Google Scholar] [CrossRef]
- Sanders, J.P.; Loveday, A.; Pearson, N.; Edwardson, C.; Yates, T.; Biddle, S.J.; Esliger, D.W. Devices for Self-Monitoring Sedentary Time or Physical Activity: A Scoping Review. J. Med. Internet. Res. 2016, 18, e90. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nauman, J.; Nes, B.M.; Gutvik, C.; Wisløff, U. Personal Activity Intelligence (PAI) for Promotion of Physical Activity and Prevention of CVD. Eur. Heart J. 2016, 37, 815. [Google Scholar]
- Funk, M.; Taylor, E. Pedometer-Based Walking Interventions for Free-Living Adults with Type 2 Diabetes: A Systematic Review. CDR 2013, 9, 462–471. [Google Scholar] [CrossRef]
- McMillan, K.A.; Kirk, A.; Hewitt, A.; MacRury, S. A Systematic and Integrated Review of Mobile-Based Technology to Promote Active Lifestyles in People with Type 2 Diabetes. J. Diabetes Sci. Technol. 2017, 11, 299–307. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Qiu, S.; Cai, X.; Chen, X.; Yang, B.; Sun, Z. Step Counter Use in Type 2 Diabetes: A Meta-Analysis of Randomized Controlled Trials. BMC Med. 2014, 12, 36. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chiauzzi, E.; Rodarte, C.; DasMahapatra, P. Patient-Centered Activity Monitoring in the Self-Management of Chronic Health Conditions. BMC Med. 2015, 13, 77. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Årsand, E.; Frøisland, D.H.; Skrøvseth, S.O.; Chomutare, T.; Tatara, N.; Hartvigsen, G.; Tufano, J.T. Mobile Health Applications to Assist Patients with Diabetes: Lessons Learned and Design Implications. J. Diabetes Sci. Technol. 2012, 6, 1197–1206. [Google Scholar] [CrossRef] [Green Version]
- Lobelo, F.; Kelli, H.M.; Tejedor, S.C.; Pratt, M.; McConnell, M.V.; Martin, S.S.; Welk, G.J. The Wild Wild West: A Framework to Integrate MHealth Software Applications and Wearables to Support Physical Activity Assessment, Counseling and Interventions for Cardiovascular Disease Risk Reduction. Prog. Cardiovasc. Dis. 2016, 58, 584–594. [Google Scholar] [CrossRef] [Green Version]



{kind=link}
{kind=link}
| Search | Review Component | Query Terms |
|---|---|---|
| 1 | Population | cancer OR tumor OR malignancy OR neoplasm |
| 2 | Wearable technology | monitor OR wearable technology OR wearable device OR Fitbit OR Garmin OR Apple OR Polar OR Huawei OR Samsung |
| 3 | Behavior | physical activity OR exercise OR fitness OR physical exercise OR sedentary OR sitting |
| 4 | All | #1 and #2 and #3 |
| Author | Objective | Study Design/Methods | Activity Monitor/Intervention | Key Outcome Measures † | Key Findings † | Risk of Bias Score |
|---|---|---|---|---|---|---|
| Brown et al. (2018) [44] | Characterize changes in circulating tumor cells after exercise training | RCT. Participants (n = 23) were randomized to either low-dose (n = 11), high-dose (n = 7) or usual care (n = 5). Baseline and 6-month assessments. | Control: usual care; Intervention: low-dose (141 min/wk), or high-dose exercise (247 min/wk). Activity monitor: in-home treadmill, and heart rate monitor. | Adherence rate was used to measure the feasibility. | Over six months, the low-dose group had an adherence of 93%, and the high-dose group had an adherence rate of 95%. | 0/7 |
| Cadmus-Bertram et al. (2019) [45] | Test the feasibility of augmenting care planning with a multi-level PA intervention | RCT. Participants (n = 50) were randomized to intervention (n = 26) or comparison (n = 24). Baseline and 12-weeks assessments. | Control: dietary guidelines + standardized email contact; Intervention: care plan + Fitbit-based PA module + in-persona session with goal-setting + email-based coaching + Fitbit review. Activity monitor: ActiGraph GT3X+ accelerometer. | PA was accelerometer-measured by MVPA, and daily step. Clinicians and support partners reviewed web-based surveys within EHR that track frequency and usefulness of exercise process. | Participants and their support partners experienced substantial increases in accelerometer-measured PA after completing the intervention session. In terms of EHR online feedback, half (50.0%) rated the procedure as “very easy”, 18.2% as “very easy”, 13.6% as “neither easy nor difficult”, and 18.2% as “somewhat difficult”. | 2/7 |
| Chan et al. (2020) [46] | Determine the feasibility and acceptability of a remotely delivered web-based behavioral intervention among men with prostate cancer. | RCT. Participants (n = 202) were randomized to either level 1 (n = 49), level 2 (n = 51), level 3 (n = 50), or level 4 (n = 52). Baseline, 3- and 6-mon assessments. | Control: L1 = general educational information, resource directory, and study-specific guidelines. Intervention: L2 = L1 + personalized diet and exercise prescriptions. L3 = L2 + Fitbit Alta. L4 = L3 + 2 optional calls from either exercise trainer or registered dietician. Activity monitor: Physical activity reported by Fitbit | The effect of intervention was evaluated by self-reported diet and PA. The accrual time and retention were used to determine feasibility. Personal surveys were used to assess acceptability with general satisfaction. | The follow-up rate at 3 months was 82.7%, whereas it was 77.2% after 6 months. The intervention was well received by the vast majority of responders. The highest percentage of Level 4 participants were highly satisfied. Level 1 expressed the most dissatisfaction. At 3 months, there was a minor difference in diet and PA between males in level 4 and those in level 1. | 2/7 |
| Cheong et al. (2018) [47] | Evaluate the efficacy and feasibility of comprehensive mobile health care of colorectal cancer patients during active chemotherapy | Pre-post design. Assessments were conducted in baseline (n = 102), 6-week (n = 92), and 12-week (n = 75). | Intervention: smartphone aftercare program + wearable device (Internet of Things) + rehabilitation exercise. Activity monitor: Self-reported questionnaire and wearable device. | Subjective measurement: Questionnaires track the amount of time spent exercising MVPA and walking. Objective measurement (wearable device): number of steps, walking distance, and heart rate. The feasibility was determined by the compliance rate. | Although the quantity of PA dropped from 6 to 12 weeks, the overall amount of weekly PA improved after 12 weeks. The participants’ compliance rate was 83.8%, while the rate of dizziness and dyspnea during exercise was 15%. | 6/7 |
| Ferrante et al. (2022) [48] | Examined adherence with a physical activity tracker and patterns of activity among different subgroups of African American/Black breast cancer survivors | This is a follow-up (n = 44) to an RCT consists of control (n = 17), intervention (n = 17), an additional intervention (n = 10). Baseline, 3-, 6-, 9-, and 12-month follow-up visits. | Control: Fitbit only; Intervention: SparkPeople + Fitbit; Additional intervention: SparkPeople Premium + Fitbit; Physical monitor: Fitbit Alta. Self-reported questionaries on self-regulation and self-efficacy | Fitbit devices calculate active minutes for activities lasting at least 10 min at or above 3 METs. Insufficient Fitbit wear or data capture (fewer than 1000 steps) were deemed non-adherent. | Adherence was shown to be significantly related to steps and active minutes. Activity levels were significantly correlated to self-monitoring, goal setting, and self-efficacy. Some subgroups, such as those over 60, retired, with a BMI more than 40, a greater number of comorbidities, or more household members, may demand further assistance. | 2/7 |
| Finley et al. (2020) [49] | Explore the feasibility, acceptability and perceived utility of a wearable fitness device and an exercise prescription from a surgeon | Pre-post design. Assessments were conducted in baseline (n = 30), and post-study (n = 17). Day of surgery, 2- and 16- weeks after surgery, and two semi-structured interviews. | Intervention: prescription for 150 min/wk MVPA exercise. Activity monitor: Garmin Vivoactive HR device. Alternatively, they can use their own. | Acceptance is defined as (a) the number of days that any form of information from the device was received and (b) the number of days that heart rate data was specifically received. Semi-structured phone interview on the acceptability of the device and exercise prescription. Participants may self-motivate by viewing their heart rate time series every 15 s, number of steps taken, floors climbed, minutes spent exercising, and near real-time GPS locations. | Acceptance: During the pre-operative phase, 71% of registered participants successfully synced their device. During the post-operative period, 75% were active. Perceived utility: Ten individuals (36%) expressed satisfaction with the device. They enjoyed how the device provided them feedback on their activity level (n = 6) or progress over time (n = 2), and how it reminded them to move through alert system (n = 2). | 5/7 |
| Gehring et al. (2018) [50] | Investigates the feasibility of a home-based, remotely guided exercise intervention for patients with gliomas. | Randomized controlled trial. 34 (n = 202) were randomized to either control (n = 11) or intervention (n = 23). Baseline and 6 months assessments. | Intervention package: individualized exercise prescription + weekly personal feedback by e-mail + last call on the feedback on program. Control: motivational brochures + bi-monthly phone calls on general health questions. Activity monitor: Objective measurement by heart rate monitors. Self-reported PA by the International Physical Activity Questionnaire | Adherence was measured as the proportion of physical exercise sessions performed throughout the time out of the specified sessions. The average heart rate of all training sessions as a percentage of the maximal heart rate as determined during the first exercise test showed average intensity. Two physiotherapists independently rated overall exercise performance for each participant. | The average adherence to scheduled sessions was 79%. Patients had positive experiences. There were no negative events. The physical exercise program was rated as satisfactory or good by 84% of participants. The exercise group improved more than the control group in maximal cardiopulmonary exercise testing (+158.9 mL/min; 95% CI: 44.8 to 362.5) and BMI (0.3 kg/m2; 95% CI: 0.9 to 0.2). | 0/7 |
| Gell et al. (2017) [51] | Examine the efficacy, feasibility, and acceptability of a technology-based intervention to promote maintenance of PA | Pre-post design. Baseline (n = 38); post study (n = 24). Participants meet weekly to download/review weekly PA by step data for Fitbit step counts and minutes. | Intervention package: tailored text message + Fitbit self-monitoring, and brief health coaching sessions. Physical Monitor: Fitbit and Actigraph GT3X+ accelerometer. Fitbit was used to support self-monitoring and text message content. Locations were assessed by QStarz BT-Q1000XT GPS. | MVPA were estimated by total weekly minutes and average daily step counts. Acceptability was determined by the percentage cancer survivors who agreed to participate in the study, intervention attrition and post-intervention questions on satisfaction. | The intervention was well-received by the majority of participants, with 87% satisfied with the health coach and Fitbit and 91% satisfied with the text message content. The majority of participants reported that text messages and Fitbit improved their motivation and the quantity of PA they performed. There was no attrition among those who began the intervention. There was no significant difference in PA levels measured with an accelerometer before and after the intervention, suggesting that PA levels were maintained 4 weeks after completing exercise-based cancer rehabilitation. | 3/7 |
| Granger et al. (2018) [52] | Determine the: (1) feasibility and (2) exploratory effectiveness of a PA self-management program aiming to increase PA levels | Pre-post design. Baseline (n = 42) and 8-weeks follow-up (n = 37) assessments. Followed-up with weekly telephone consultations. | Intervention package: unsupervised home aerobic exercise program + written information manual + Fitbit for self-monitor and personalized program/goals. Activity monitor: The Fitbit was used to self-monitoring behavior, but PA was self-reported by questionnaire. | The feasibility was determined by the rate of consent and the number of consultations provided. As a result, a 70% consent rate determined viability. The secondary assessment focused on the start date of the intervention, the number of intervention consultations provided, and the location of the initial consultations. | Participants undergoing lung cancer surgery may be interested in such an intervention (89% consent rate), are able to participate when it is delivered in the post-surgical setting (100%) and may not have declines in PA levels as a result. There were no statistically significant changes in self-efficacy for PA. | 6/7 |
| Groarke et al. (2021) [53] | Examine the acceptability of a behavior change intervention using mHealth for cancer survivors with a BMI of 25 or more. | RCT-based mixed method: 13 participants were interviewed, and 36 participants completed the quantitative survey. At the 24-week follow-up. | Intervention: 8-week PA goal setting: Fitbit activity monitor + SMS contact. Activity monitor: Fitbit. | Qualitative: Semi-structured interviews were used to assess retrospective acceptance. Quantitative: Response rates and retention rates were also used as measures of the acceptability of the intervention. | The majority of survey respondents (35/36, 97%) were satisfied with the intervention. Many of the intervention components were liked in qualitative reports, with the mHealth components receiving particularly positive ratings. The burden of participation in the intervention was rated as either high (6/36, 17%) or low (5/36, 14%). The majority of respondents (35/36, 97%) reported they understood how the intervention worked, and qualitative data show that participants’ understanding of the intervention’s goal was broader than weight control and focused more on moving on psychologically after cancer. | 5/7 |
| Hardcastle et al. (2020) [54] | explore patterns of Fitbit-measured PA and wear-time over 24-weeks and their relationship to changes in Actigraph-derived moderate-to-vigorous PA (MVPA). | This is a follow-up to an RCT. Pre-post design. Baseline (n = 29) and post-study (n = 28). Baseline, intervention (12-weeks) and end of follow-up (24-weeks) assessment. | Intervention: Fitbit Alta + two-hour group sessions + action-planning and goal-setting + phone-call feedback. Daily steps and active minutes were recorded. Activity monitor: The Actigraph GT9X research grade accelerometer provided minutes/week of MVPA. The Fitbit Alta was used for self-monitoring and explore patterns of PA. | Fitbit wear-time adherence rates (percentage of valid wear days). As a result, a valid wear-day was defined as a step count of =>1000 steps each day. Participants performed daily accelerometer diaries to allow for data cross-checking. For uniaxial and triaxial cut point definitions, MVPA was defined as =>1952 and =>2690 counts per minute, respectively. | The median adherence score for all 24 weeks examined separately was 100%. Fitbit wear-time was also high during the follow-up period (13 to 24 weeks), with an adherence score of 98%. (IQR 75 to 100). | 2/7 |
| Hartman et al. (2018) [55] | Examine patterns of Fitbit use and activity and their relationships with success in the intervention based on ActiGraph-measured MVPA. | Pre-post study to follow an RCT. Baseline (n = 43) and post-study (n = 42) assessment. | Intervention package: Fitbit for self-monitoring PA + phone calls (2-week and 6-week time points and automatic emails every 3 days throughout the 12-week intervention, which included reminders to sync and wear their Fitbit). Activity monitor: Fitbit. ActiGraph GT3X+ accelerometer. | Active Minutes and daily adherence were measured by Fibit tracker. Accelerometers were used to determine frequency, duration, and intensity. Self-report questionnaires were utilized to measure how frequently individuals glanced at their Fitbit tracker activity data. | Adherence to wearing the Fitbit was robust and consistent, with a mean of 88.13% of valid days (SD 14.49%) for 12 weeks. Greater adherence to Fitbit use was related to higher increases in MVPA. The highest minutes of MVPA occurred at week 3, immediately after the intervention call, which generally occurred towards the end of week 2, and at week 9, which was approximately when participants were contacted to confirm their final visit at 12 weeks. | 2/7 |
| Kanzawa-Lee et al. (2022) [56] | Explore the effect of an 8-week home-based brisk walking (the “MI-Walk”) intervention compared with PA education alone. | RCT. Participants (n = 57) were randomized to control (n = 28) or intervention (n = 29). Baseline and 8-month assessments. | Control: PA education and phone assessments. Intervention: control + MI-WALK motivational supports (Fitbit + enhancement therapy session). Activity monitor: Fitbit. | A 0–793 scaled questionnaire was used to assess self-reported PA. Questionaries were used to assess self-reported motivational interviewing fidelity and PA. | The intervention and control groups had the same self-reported PA scores at baseline (n = 51) and 8 weeks (n = 48). Among the MI-Walk intervention participants, no baseline Fitbit data (only post-intervention initiation) were gathered. As a result, there was no analyses on the change in PA. | 2/7 |
| Kenfield et al. (2019) [57] | Determine the feasibility and acceptability of a digital lifestyle intervention among men with prostate cancer. | Randomized controlled trial. Participants (n = 76) were assigned to either intervention (n = 37) or control (n = 39). Baseline, first 12-week, and second 12-week assessments. | Control: only usual standard of care; Intervention: personalized recommendations on website + Fitbit One + and text messaging. Activity monitor: Self-reported questionaries on PA and accelerometers. | The rates of recruitment and the utilization of study components were used to determine feasibility. Adherence was determined each week as responding to a text message. Online questionnaires with closed and open-ended questions were used to measure acceptability. After 12 weeks, Fitbit activity data was used to examine responses on the text messaging platform, and website login and page visit data were used to quantify study component consumption. | The intervention arm self-reported change was 1.1 h per week (IQR: −0.3, 3.6), while the control arm was 0 h per week (IQR: −1.1, 1.7). There were no statistically significant differences between the groups. Accelerometer: There were no differences in step counts, moderate, or MPVA between the two arms. Participants in the intervention wore their Fitbits for an average of 82 days (IQR: 72–83), with 98% of the days falling within the 12-week period, responded to an average of 71% of text messages (IQR: 57–89%), and saw the website for an average of 3 days (IQR: 2–5). Acceptability: 60.7% of participants rated the website as high or very high in quality, 87.1% rated Fitbits as good to excellent, 68.8% rated SMS messaging as good to exceptional, and 78.1% rated the baseline personalized suggestion report as good to excellent. Participant satisfaction (defined as “pleased” or “very satisfied”) for the website was 60%, 90.6% for Fitbits, and 73.3% for text messaging. | 2/7 |
| Kim et al. (2020) [58] | Evaluate the efficacy and safety of rehabilitation exercises among hepatocellular carcinoma patients. | Pre-post design. Baseline (n = 37); post study (n = 31). Baseline, and 6- and 12- week assessments. | Intervention: Neofit (wearable wristband) + mHealth app + prescribed rehabilitation exercise. Activity monitor: Neofit. | Neofit assessed the number of steps taken, calorie expenditure, activity time, and heart rate using wearable sensors. Self-reported MVPA minutes per day or days per week, as well as time spent walking or sitting in the previous 7 days. Physical fitness was carefully assessed using clinical equipment. | The completion rate for this trial was 84% (31/37). According to a satisfaction survey, after 12 weeks of mHealth program for patients, 84% of participants rated medium-to-high satisfaction with the program. After the trial, 87% of participants stated a wish to continue utilizing the program. Both the 30-s chair stand test and the 6 min walk test significantly improved from 0 to 6 weeks, 0 to 12 weeks, and 6 to 12 weeks. Muscle mass and the IPAQ-SF score increased considerably after 12 weeks of therapy, with no biochemical deterioration. | 4/7 |
| Low et al. (2020) [59] | To develop and test a mobile technology-supported intervention to reduce Sedentary behavior before and after cancer surgery, and to evaluate the usability and feasibility of the intervention. | Pre-post design. Baseline (n = 15); post study (n = 14). Participants were called once per week to complete semi-structured interviews during the 30 days after hospital discharge | Intervention: Fitbit + a smartphone app (i.e., Detecting Activity to Support Healing) + weekly call + semi-structured interviews. Activity Monitor. Participants were asked to respond to the activity prompt. The prompt was calculated by their Fitbit PA data. | (1) Weekly ratings on how easy it was to use each app’s interface in terms of appearance design, and usability; and how satisfied the participant was overall with the DASH intervention program. (2) A ten-item questionnaire based on the Usability Scale. The semi-structured interviews’ notes were examined and organized into recognized themes. Accrual and retention rates, as well as compliance with reporting symptoms, were used to determine feasibility. A questionnaire about the usability of the apps. Semi-structured interviews were used to assess the intervention. | Low (1/15, 7%) attrition was due to poor health and extended hospitalization. Fitbit compliance was 70% (653/927 days) overall, however it decreased from before surgery (330/364, 91%) to inpatient (51/143, 36%) and post discharge (272/420, 65%). Fitbit wear time compliance is also dropping, which is consistent with research in healthy individuals, which found that 40% of participants abandoned the Fitbit after six months. Overall system satisfaction was 89.9, while the mean System Usability Scale score was 83.8 out of 100. | 4/7 |
| Lynch et al. (2019) [60] | Determine the efficacy of a 12-week intervention for increasing MVPA and reducing sedentary behavior for postmenopausal breast cancer survivors. | RCT. Participants (n = 83) were assigned to either intervention (n = 43) or control (n = 40). Baseline, first 12-week, and second 12-week assessments. | Control: Behavioral feedback and goal-setting session + telephone-delivered behavioral counseling. Intervention: control + Garmin Vivofit 2 (activity monitor). Activity monitor: Actigraph GT3X+ accelerometer, Garmin Vivofit 2, and activPAL. | The retention rate was used to measure acceptance. Accelerometer data is used to count movement. MVPA was computed by adding together the average weekly time spent and time spent in “bouts” of 10 min or more. The activPAL counts the number of posture changes as well as the length of time spent in each posture. | The experiment had a high retention rate, with 80 (96%) of patients completing T2 data collection. At T2, there was a statistically significant difference in MVPA across groups (69 min/wk; 95% CI = 22–116; p 0.01), favoring the intervention arm. Overall sitting time (37 min/d; 95% CI: 72 to 2; p = 0.01) and protracted episodes of at least 20 min length (42 min/d; 95% CI: 83 to 2; p = 0.04) were statistically different in the intervention arm. | 2/7 |
| Lynch et al. (2019) [61] | (1) to examine the maintenance of MVPA and sitting time changes in the primary intervention group approximately 12 weeks after intervention (T3) (2) to determine the efficacy of an abridged intervention (Garmin Vivofit 2 only). | This is follow-up analysis (T3) after the intervention (T2) for the Lynch-1. For aim 1 (maintenance): Baseline (n = 43); post study (36 for maintenance, 30 for sitting). For aim 2: baseline (n = 40), post study (n = 37). Assessments were T3 after the Lynch-1 (T2). | Intervention and control are the same from above. Activity Monitor: MVPA was measured by the Actigraph GT3X+ accelerometer, calibrated by the Garmin Vivofit 2. Sitting time was assessed by the activPAL. Garmin Vivofit 2 was used to assess the MVPA in Aim 2. | The retention rate was considered to assess the acceptability. MVPA was quantified using the Sasaki vector magnitude cut point (using tri-axial data) of 2690 counts per minute (we also used the Freedson and Matthews cut points); sitting time was measured using the activPAL, which participants were instructed to wear 24 h a day. | The retention rate was 87%. The study had a good retention rate, with 80 (96%) of individuals completing T2 data collection. (95% CI = 18 to 46; p = 0.37); the mean change between T2 and T3 was 8 min per week (95% CI = 17 to 33; p = 0.52). At T3, the MVPA of participants in the primary intervention arm was 86 min per week (95% CI = 47–125; p 0.01) greater than at T1. At T3, participants had increased their MVPA by 33 min per week (95% CI = 3–64; p = 0.03). The average increase in MVPA from T1 was much larger (38 min/week, 95% CI = 4–73; p = 0.03). In the waitlist control arm, average sitting time was decreased by 38 min per day (95% CI = 69 to 7; p = 0.02), but sitting time at T3 was only 23 min less than at T1 (95% CI = 54 to 8; p = 0.15). Between T2 and T3, the abbreviated intervention reduced prolonged sitting by 28 min per day (95% CI = 60 to 5; p = 0.09). | 5/7 |
| Marthick et al. (2018) [62] | Evaluate the feasibility, usability, and acceptability of an interactive Web portal developed to support patients with cancer to increase daily PA levels. | longitudinal cohort design. All participants (n = 49) were allocated to 3 cohorts: 1. Web portal (n = 17) 2. Web portal + summative messaging (n = 17) 3. Web portal personalized coaching messaging (n = 15). | Intervention: Interactive web portal, included integration of real-time wearable activity device data, collection of PROs and symptom information, the provision of educational material, and individualized coaching messaging to support behavior change by encouraging patient engagement in PA. Activity monitor: Misfit Shine activity monitor or Fitbit was used to measure feasibility. | To measure feasibility, the number of log-ins and completed surveys were employed. Semi-structured qualitative interviews were used to assess acceptability, which included participant satisfaction, acceptability of the intervention, self-efficacy linked to changes in lifestyle determinants, median daily step count, and weekly email involvement. | The number of individuals satisfying the two feasibility criteria grew over the cohorts, with cohort 1 having the fewest (7/17, 35%) and cohort 3 having the highest (12/14, 86%). Only cohort 3 satisfied the feasibility criterion. The activity tracker distributed to participants was generally well received, with individuals indicating that they enjoyed it and found it straightforward to use. Participants were extremely or somewhat happy with the intervention, with 83% (33/40) of responders extremely or moderately satisfied. Satisfaction with the Misfit Shine activity tracker was high, with 77% (31/40) of respondents extremely or fairly satisfied. | 5/7 |
| Maxwell-Smith et al. (2019) [63] | Ascertain whether activity monitor coupled with action planning was effective in increasing PA in colorectal and endometrial cancer survivors at cardiovascular risk. | RCT. All participants (n = 68) were randomized to intervention (n = 34) or control (n = 34). 30 min assessments at baseline and 12 weeks. | Control: PA guidelines. Intervention: Fitbit Alta + group session + support phone call. Activity monitor: Fitbit and ActiGraph Link GT9X accelerometer. | The ActiGraph was also used to calculate the number of minutes per day of MVPA accumulated in bouts of at least 10 min. The wristworn Fitbit Alta tracker was utilized as an experiment to capture daily steps. The ActiGraph GT9X accelerometer was used to calculate MVPA minutes each week. MVPA is accumulated in 10 min increments) and distance, and it gives automated alerts pushing participants to collect 250 steps each hour. | With 94% attendance across group sessions, intervention adherence was excellent. The majority of intervention group participants (88%, n = 29) accepted the Fitbit friend invitation. Fitbit involvement was high, with 86% (SD = 29) of valid weardays recorded throughout the 12-week period (n = 28). A legitimate wearday was defined as a step count of 1000 steps each day. The intervention group raised MVPA by 45 min per week, whereas the control group decreased by 21 min per week. On both triaxial (29 vs. 8 min/wk) and uniaxial (31 vs. 7 min/wk) measurements of MVPA accumulated in bouts of at least 10 min, the observed mean increases in MV10 were higher in the intervention group compared to controls one. | 1/7 |
| Rastogi et al. (2020) [64] | Determine whether the PA module improved lasting behavior change. | RCT. Participants (n = 50) were randomized to intervention (n = 26) or control (n = 24). Baseline and 12-weeks. | Control: Dietary guidelines + standardized emails. Intervention: Fitbit tracker + customized email feedback. Activity monitor: ActiGraph GT3X+. | The scale runs from 1 to 5, with higher scores suggesting that the person is working to improve their PA-related thoughts and behavior. Decision- making balancing was used to investigate the perceived benefits and barriers of PA. | A total of 94% of survivors retained in the study after 12 weeks. The intervention was associated with moderate-to-large improvements in physical health (effect size: d = 0.39, 95% CI = 0.0, 0.78), mental health (d = 0.59, 95% CI = 0.19, 0.99), sleep impairment (d = 0.62, 95% CI = 1.02, 0.22), and exercise self-efficacy (d = 0.60, 95% CI = 0.20, 1.0) compared to the controls. | 2/7 |
| Schrier et al. (2021) [65] | (1) assess the feasibility and acceptability of the intervention. (2) assess the change in mean daily step counts. | Pre-post design. Baseline (n = 29) and post-study (n = 24). Baseline 2-week intervention; 12-week follow-up. | Intervention: two Fitbit Charge 2 s (one for the participant and one for the teammate). Fitbits + increased step goal + collaborative game integrates wireless devices, clinical trial randomization and enrollment processes, self-administered surveys, automatic transfers of financial incentives, and secure data capture for research purposes. Activity monitor: Fitbit. | Daily steps were assessed by feasibility (defined a priori as a 60% approach-to-consent ratio and 70% Fitbit adherence), acceptance (defined by 20% of participants expressing burden or regret for participation), and preliminary effectiveness (defined by 70% reporting greater motivation). At the end, there was a debriefing interview. | Tracker adherence was 94%. At the 24-week follow-up, 1/24 (5%) of participants reported burden, 0/24 (0%) expressed regret for participating in the study, and 22/24 (>90%) agreed/strongly agreed that “the study pushed me to raise exercise levels”. Participants’ mean daily steps increased from 6210.7 (3328.1) at baseline to 7643 (3610.9) steps (p 0.001) during the 12-week intervention. During the 12-week intervention period, participants raised their mean daily steps by 1432 steps and met their step objectives 61.1% of the time. However, twelve weeks after the intervention ended, participants’ mean daily steps dropped to 6435.1 (+3551), which was not significantly higher than their baseline step count (6210 (3328) vs. 6435 (3551), p > 0.05). Only 33.9% of individuals met their step objectives during this time period. Working with a teammate was pleasurable for the majority of participants. | 6/7 |
| Singh et al. (2020) [66] | Evaluate the effect and acceptability of a PAC session, plus provision of a Fitbit, on maintenance of PA levels 12 weeks following participation in exercise intervention. | RCT. Participants (n = 60) were randomized to intervention (n = 30) or control (n = 30). Baseline and 12- weeks follow up assessments. | Control: PAC. Intervention: PAC + Fibit. Activity Monitor: Self-report questionnaire and Actigraph® GT3X+ accelerometers. | The fulfillment of the following requirements indicates feasibility: 1 Participants wore the Fitbit for at least 10 h per day on at least five out of seven days in a regular week (group mean); 2 More than 80% of participants said the Fitbit was straightforward to use; 3 More than 80% of participants said the Fitbit was comfortable to wear; 4. More than 80% of people were satisfied with the Fitbit as a method of assistance with PA maintenance; 5. Over 80% of participants stated they would keep using the Fitbit in the future. | At 12-week follow-up, the PAC + F group had higher self-reported MVPA and self-reported total activity than the PAC group (between-group mean difference: 78.2 [95% CI = 8.3, 164.9] min/week, p 0.01, and 171.9 [95% CI = 46.1, 297.8] min/week, p 0.01, respectively). At 12-week follow-up, the PAC + F group had higher objectively-assessed MVPA (p = 0.03) and steps/day (p = 0.07) than the PAC group. The majority (>80%) of the PAC + F group reported high levels of Fitbit use, indicating the device was useful for PA maintenance. The Fitbit was easy to use (n = 24, 92%) and comfortable to wear (n = 22, 84%), according to the majority of participants. | 5/7 |
| Uhm et al. (2017) [67] | Compare the effects of mobile health (mHealth) and pedometer with conventional exercise program using a brochure on physical function and quality of life. | Randomized clinical trial. Participants (n = 356) were randomized to either mHealth with pedometer (n = 179) or conventional program (n = 177). Baseline and 12- weeks follow up examined the self-reported PA. | Control: exercise brochure. Intervention: home-based prescribed aerobic exercise and resistance exercises + physical therapists + smartphone exercise application (Smart After Care). Activity Monitor: pedometer, and self-reported questionnaire. | Weekly physical activity as indicated by the pedometer user satisfaction questionnaire survey, with responses ranked from 1 (“strongly disagree”) to 5 (“strongly agree”). | Weekly PA increased significantly in both groups, with the increase being greater in the mHealth group but not statistically significant. In the mHealth group, the mean Likert scale response for overall satisfaction with the service was 4.27/5. | 2/7 |
| Van Blarigan et al. (2019) [68] | Determine the feasibility and acceptability of the intervention and explore the potential effect of the intervention on accelerometer-measured PA. | Randomized clinical trial. Participants (n = 42) were randomized to intervention (n = 21) or control (n = 21). Baseline and 12- weeks follow up assessments. | Control: usual care. Intervention package: Fitbit Flex™ + daily text message. Activity monitor: Actigraph GTX3+ accelerometers. | Adherence and attrition were used to determine feasibility. Acceptability was measured using a 14-item questionnaire in which participants were asked to rate their level of agreement with four claims regarding text messages and one statement about the Fitbit. | The majority (88%) of the 16 intervention participants who completed the feedback survey reported that the intervention motivated them to exercise and that they were satisfied with their experience. The intervention arm increased their MVPA by 13 min per day more than the control arm (mean difference: 13.1 min per day; 95% confidence interval: −13.5, 39.7). There was no statistically significant difference in MVPA change among arms from baseline to 12 weeks. | 2/7 |
| Wang et al. (2011) [69] | Examine the effects of a walking program on Taiwanese women newly diagnosed with early-stage breast cancer. | RCT. Participants (n = 72) were randomized to the either exercise group (n = 35) or usual care group (n = 37). Assessment: (1) 24 h prior to the surgery, (2) 2–3 weeks after surgery, (3) 7–10 days after chemotherapy, (4) the end of the 6-week intervention. | Control: usual care. Intervention package: 6-week walking program + plan to boost exercise self-efficacy (the HR ring monitor + pedometer + weekly phone call + weekly exercise diary + weekly meeting + role model store). Activity monitor: The exercise intensity was measured by HR rings and pedometer. | The retention rate was considered to assess the feasibility. MVPA was defined as a heart rate maximum (HRmax) of 40% to 60% or a modified Borg Scale of 0.5 to 2, 3 to 5 sessions per week, and at least 30 min each session or the accumulation of 10 min sessions to achieve 30 min. Exercise capacity was measured using a 6 min walk distance. During exercise, self-monitoring using the heart rate ring and pedometer. The appropriate exercise intensity was determined using the heart rate. | The retention rate for this study was 86.1%. The exercise group significantly outperformed the usual-care group in terms of exercise behavior following the intervention (F1,60 =13.55, p = 0.001). | 1/7 |
| Zeng et al. (2020) [70] | Investigates whether a year-long combined fitness wristband-based and personalized exercise prescription intervention improves Chinese breast cancer survivors’ health outcomes. | Pre-post design. baseline (n = 95) and post-study (n = 33). Baseline and 12-month assessments. | Intervention package: Xiao mi wristband + exercise prescriptionActivity monitor: Xiaomi wristband | In the hospital, health outcomes were assessed. Blood samples were used to measure lipid profile and blood glucose, electrochemiluminescence immunoassay and chemiluminescence enzyme immunoassay were used to examine breast cancer biomarkers, and the Senior Fitness Test (SFT) was used to assess functional fitness. The Xiaomi bracelet measured PA, including steps taken, heart rate, calories expended, and so forth. | The percentage of retention was 35%. Remarkable shifts in functional fitness: agility and balance (MD: −0.47, 95% CI: −0.68–−0.26, t = −4.336, p < 0.001), aerobic endurance (MD: 89.25, 95% CI: 73.82–104.68, t = 11.336, p < 0.001), lower-body flexibility (left) (MD: 4.58, 95% CI: −4.4–13.56, t = 4.653, p < 0.001), and low-er-body flexibility (right) (MD: 4.84, 95% CI: −4.65–14.33, t = 4.092, p < 0.001). | 4/7 |
| Zhang et al. (2017) [71] | Establish the feasibility and acceptability of completing a higher dose of the planned PA volume among women with ovarian cancer. | Pre-post design. Baseline (n = 10); post study (n = 10). A total of 10 of 17 were enrolled in a first-contacted, first-served manner. Participants met weekly to download/review weekly PA by step count data. | Intervention package: exercise DVDs + self-reported logs + objective PA monitor (Fitbit). Activity monitor: ActiGraph GT3X triaxial accelerometer. | The adherence rate was used to assess acceptability. Participants were asked for feedback and if they were satisfied with the exercise intervention during the 26-week phone follow-ups. To objectively measure and track adherence to the exercise intervention, participants were requested to wear an activity tracker (Fitbit Zip) for the whole 26-week period. PA is measured as follows: (a) minutes of MVPA (METs), (b) minutes of light-intensity physical activity (1–3 METs), (c) average minutes of MVPA (3 METs or greater), and (d) ambulatory steps using validated cut-points appropriate for adults. | Participants received 83% of in-person sessions with the trainer. The intervention was rated as “very helpful” by all eight research participants. The majority of respondents reported improved function, as evidenced by remarks such as “feeling better” or “more active”. The amount of moderate-intensity movement per day increased by 15 min per day (p = 0.05). The number of steps taken per day rose by 1593 (p = 0.041). On average, MVPA increased by 10.02 min per day (p = 0.078). The amount of time spent on personal activities rose by 15.5 min (p = 0.009). | 4/7 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Keats, M.R.; Yu, X.; Sweeney Magee, M.; Forbes, C.C.; Grandy, S.A.; Sweeney, E.; Dummer, T.J.B. Use of Wearable Activity-Monitoring Technologies to Promote Physical Activity in Cancer Survivors: Challenges and Opportunities for Improved Cancer Care. Int. J. Environ. Res. Public Health 2023, 20, 4784. https://doi.org/10.3390/ijerph20064784
Keats MR, Yu X, Sweeney Magee M, Forbes CC, Grandy SA, Sweeney E, Dummer TJB. Use of Wearable Activity-Monitoring Technologies to Promote Physical Activity in Cancer Survivors: Challenges and Opportunities for Improved Cancer Care. International Journal of Environmental Research and Public Health. 2023; 20(6):4784. https://doi.org/10.3390/ijerph20064784
Chicago/Turabian StyleKeats, Melanie R., Xing Yu, Molly Sweeney Magee, Cynthia C. Forbes, Scott A. Grandy, Ellen Sweeney, and Trevor J. B. Dummer. 2023. "Use of Wearable Activity-Monitoring Technologies to Promote Physical Activity in Cancer Survivors: Challenges and Opportunities for Improved Cancer Care" International Journal of Environmental Research and Public Health 20, no. 6: 4784. https://doi.org/10.3390/ijerph20064784