

Child Tax Credit, Spending Patterns, and Mental Health: Mediation Analyses of Data from the U.S. Census Bureau’s Household Pulse Survey during COVID-19

Abstract
:1. Introduction
1.1. Expansion of the U.S. Child Tax Credit Amid the Crisis of Mental Health during COVID-19
1.2. Diverse Spending Patterns of the Child Tax Credit
2. Materials and Methods
2.1. U.S. Census Bureau’s HPS Data during COVID-19
2.2. Study Variables
2.2.1. Outcome: Mental Health Problems
2.2.2. Exposure: Receipt of the Child Tax Credit
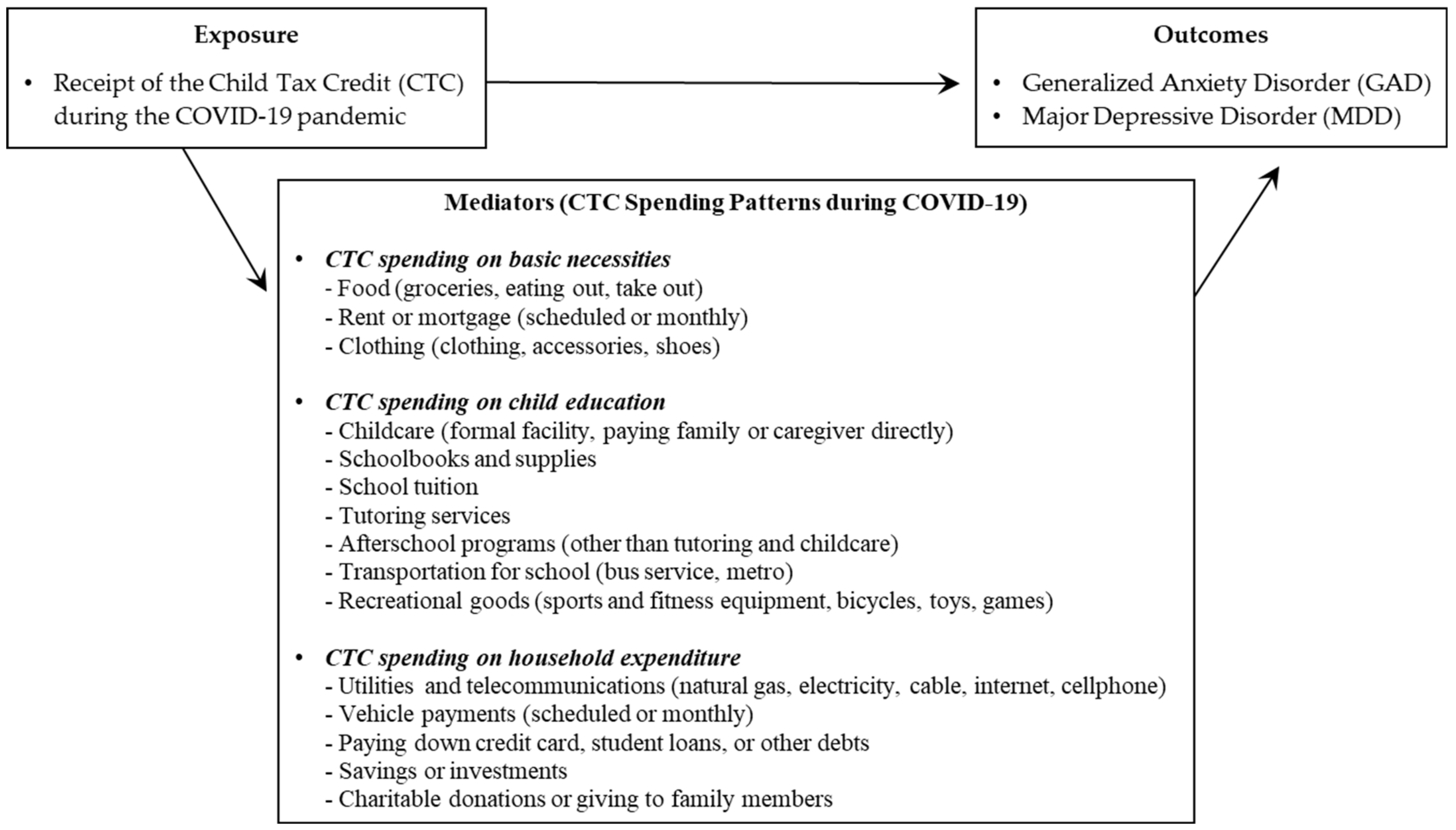
2.2.3. Mediator: Spending Patterns of the Child Tax Credit
2.2.4. Covariate: Characteristics of Survey Participants
2.3. Model Specification
3. Results
3.1. Spending Patterns of CTC and Anxiety
3.2. Spending Patterns of CTC and Depression
4. Discussion
4.1. Key Findings of Mediation Analyses
4.2. Limitations and Future Research
4.3. Policy Implications
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Hart, J.; Han, W.-J. COVID-19 Experiences and Parental Mental Health. J. Soc. Soc. Work Res. 2021, 12, 283–302. [Google Scholar] [CrossRef]
- Nelson, B.; Pettitt, A.; Flannery, J.; Allen, N. Psychological and Epidemiological Predictors of COVID-19 Concern and Health-Related Behaviors. Natl. Libr. Med. 2020, 15, 11. [Google Scholar]
- Rajkumar, R.P. COVID-19 and Mental Health: A Review of the Existing Literature. Asian J. Psychiatry 2020, 52, 102066. [Google Scholar] [CrossRef] [PubMed]
- Twenge, J.M.; Joiner, T.E. Mental Distress among U.S. Adults during the COVID-19 Pandemic. J. Clin. Psychol. 2020, 76, 2170–2182. [Google Scholar] [CrossRef]
- Cheng, Z.; Mendolia, S.; Paloyo, A.R.; Savage, D.A.; Tani, M. Working Parents, Financial Insecurity, and Childcare: Mental Health in the Time of COVID-19 in the UK. Rev. Econ. Househ. 2021, 19, 123–144. [Google Scholar] [CrossRef]
- OECD. Tackling the Mental Health Impact of the COVID-19 Crisis: An Integrated, Whole-of-Society Response; OECD: Paris, France, 2021. [Google Scholar]
- World Health Organization. Mental Health and COVID-19: Early Evidence of the Pandemic’s Impact: Scientific Brief. 2022. Available online: https://www.who.int/publications-detail-redirect/WHO-2019-nCoV-Sci_Brief-Mental_health-2022.1 (accessed on 30 January 2023).
- Chatterji, S.; McDougal, L.; Johns, N.; Ghule, M.; Rao, N.; Raj, A. COVID-19-Related Financial Hardship, Job Loss, and Mental Health Symptoms: Findings from a Cross-Sectional Study in a Rural Agrarian Community in India. Int. J. Environ. Res. Public Health 2021, 18, 8647. [Google Scholar] [CrossRef]
- Ikeda, T.; Igarashi, A.; Odani, S.; Murakami, M.; Tabuchi, T. Health-Related Quality of Life during COVID-19 Pandemic: Assessing Impacts of Job Loss and Financial Support Programs in Japan. Appl. Res. Qual. Life 2022, 17, 541–557. [Google Scholar] [CrossRef]
- Kiely, K.M.; Leach, L.S.; Olesen, S.C.; Butterworth, P. How Financial Hardship Is Associated with the Onset of Mental Health Problems over Time. Soc. Psychiatry Psychiatr. Epidemiol. 2015, 50, 909–918. [Google Scholar] [CrossRef]
- Bauer, A.; Garman, E.; McDaid, D.; Avendano, M.; Hessel, P.; Díaz, Y.; Araya, R.; Lund, C.; Malvasi, P.; Matijasevich, A.; et al. Integrating Youth Mental Health into Cash Transfer Programmes in Response to the COVID-19 Crisis in Low-Income and Middle-Income Countries. Lancet Psychiatry 2021, 8, 340–346. [Google Scholar] [CrossRef]
- Ohrnberger, J.; Anselmi, L.; Fichera, E.; Sutton, M. The Effect of Cash Transfers on Mental Health: Opening the Black Box—A Study from South Africa. Soc. Sci. Med. 2020, 260, 113181. [Google Scholar] [CrossRef]
- Shafer, P.R.; Gutiérrez, K.M.; Ettinger de Cuba, S.; Bovell-Ammon, A.; Raifman, J. Association of the Implementation of Child Tax Credit Advance Payments with Food Insufficiency in US Households. JAMA Netw. Open 2022, 5, e2143296. [Google Scholar] [CrossRef]
- Crandall-Hollick, M.L.; Carter, J.A.; Boyle, C.F. The Child Tax Credit: The Impact of the American Rescue Plan Act (ARPA P.L. 117-2) Expansion on Income and Poverty; Congressional Research Service: Washington, DC, USA, 2021. [Google Scholar]
- Ananat, E.; Glasner, B.; Hamilton, C.; Parolin, Z. Effects of the Expanded Child Tax Credit on Employment Outcomes: Evidence from Real-World Data from April to December 2021; Working Paper; National Bureau of Economic Research: Cambridge, MA, USA, 2022. [Google Scholar]
- Baker, M.; Messacar, D.; Stabile, M. The Effects of Child Tax Benefits on Poverty and Labor Supply: Evidence from the Canada Child Benefit and Universal Child Care Benefit; Working Paper; National Bureau of Economic Research: Cambridge, MA, USA, 2021. [Google Scholar]
- Chu, L.; Teng, L. Does Stimulus Check Payment Improve People’s Mental Health in the COVID-19 Pandemic? Evidence from U.S. Household Pulse Survey. J. Ment. Health Policy Econ. 2022, 25, 133–142. [Google Scholar]
- Tsai, J.; Huang, M.; Rajan, S.S.; Elbogen, E.B. Prospective Association between Receipt of the Economic Impact Payment and Mental Health Outcomes. J. Epidemiol. Commun. Health 2022, 76, 285–292. [Google Scholar] [CrossRef]
- Berkowitz, S.A.; Basu, S. Unemployment Insurance, Health-Related Social Needs, Health Care Access, and Mental Health During the COVID-19 Pandemic. JAMA Intern. Med. 2021, 181, 699–702. [Google Scholar] [CrossRef]
- Wolfson, J.A.; Garcia, T.; Leung, C.W. Food Insecurity Is Associated with Depression, Anxiety, and Stress: Evidence from the Early Days of the COVID-19 Pandemic in the United States. Health Equity 2021, 5, 64–71. [Google Scholar] [CrossRef]
- Smith, M.V.; Callinan, L.S.; Posner, C.S.; Holmes, S.C.; Ebling, R. Improving Maternal Mental Health as a Pathway to Economic Mobility in the TANF System. Psychiatr. Serv. 2021, 72, 1139–1144. [Google Scholar] [CrossRef]
- Dore, E.C.; Livingston, M.D., III; Shafer, P.R. Easing Cash Assistance Rules During COVID-19 Was Associated with Reduced Days of Poor Physical and Mental Health: Study Examines Impact of Easing Cash Assistance Rules during COVID-19 Had Participants’ Physical and Mental Health. Health Aff. 2022, 41, 1590–1597. [Google Scholar] [CrossRef]
- Sears, R. Cash Payments to Families Lead to Long Term Improvements in Child Mental Health. Mad in America, 11 October 2022. Available online: https://www.madinamerica.com/2022/10/cash-payments-families-leads-better-child-mental-health (accessed on 26 November 2022).
- Shevlin, M.; Redican, E.; Hyland, P.; Butter, S.; McBride, O.; Hartman, T.K.; Murphy, J.; Vallières, F.; Bentall, R.P. Perceived Manageability of Debt and Mental Health during the COVID-19 Pandemic: A UK Population Analysis. PLoS ONE 2022, 17, e0274052. Available online: https://journals.plos.org/plosone/article?id=10.1371/journal.pone.0274052 (accessed on 3 January 2023). [CrossRef]
- Maslow, A.H. A Theory of Human Motivation. Psychol. Rev. 1943, 50, 370–396. [Google Scholar] [CrossRef] [Green Version]
- Loxton, M.; Truskett, R.; Scarf, B.; Sindone, L.; Baldry, G.; Zhao, Y. Consumer Behaviour during Crises: Preliminary Research on How Coronavirus Has Manifested Consumer Panic Buying, Herd Mentality, Changing Discretionary Spending and the Role of the Media in Influencing Behaviour. J. Risk Financ. Manag. 2020, 13, 166. [Google Scholar] [CrossRef]
- Afify, A.S. Effect of COVID-19 Pandemic on Consumption Patterns among Egyptian Consumers and Its Relation to Maslow’s Hierarchy of Needs. Mod. Econ. 2022, 13, 186–207. [Google Scholar] [CrossRef]
- Forbes, S.L. Post-Disaster Consumption: Analysis from the 2011 Christchurch Earthquake. Int. Rev. Retail. Distrib. Consum. Res. 2017, 27, 28–42. [Google Scholar] [CrossRef]
- Luhby, T. The Child Tax Credit May Be Helping Ease Economic Hardship after Just One Round. CNN Politics, 12 August 2021. Available online: https://www.cnn.com/2021/08/11/politics/child-tax-credit-economic-hardship/index.html (accessed on 29 December 2022).
- Hamilton, L.; Roll, S.; Despard, M.; Maag, E.; Chun, Y.; Brugger, L.; Grinstein-Weiss, M. The Impacts of the 2021 Expanded Child Tax Credit on Family Employment, Nutrition, and Financial Well-Being: Findings from the Social Policy Institute’s Child Tax Credit Panel (Wave 2); Working Paper; Brookings Global: Washington, DC, USA, 2022; p. 173. [Google Scholar]
- Rummo, P.E.; Bragg, M.A.; Yi, S.S. Supporting Equitable Food Access During National Emergencies—The Promise of Online Grocery Shopping and Food Delivery Services. JAMA Health Forum 2020, 1, e200365. [Google Scholar] [CrossRef] [PubMed]
- Kemp, M. The Expanded Child Tax Credit Is Helping Families, but National Survey Shows Continued Outreach Remains Essential; The Center for Law and Social Policy: Washington, DC, USA, 2022. [Google Scholar]
- Javaid, S.; Tucker, J. Women of Color Use Their Advance Child Tax Credit to Cover Food Costs. National Women’s Law Center, 7 September 2021. Available online: https://nwlc.org/resource/women-of-color-use-their-advance-child-tax-credit-to-cover-food-costs (accessed on 5 January 2023).
- Zippel, C. After Child Tax Credit Payments Begin, Many More Families Have Enough to Eat; Center on Budget and Policy Priorities: Washington, DC, USA, 2021. [Google Scholar]
- Perez-Lopez, D.J. Household Pulse Survey Collected Responses Just Before and Just After the Arrival of the First CTC Checks. Census Bureau’s Social, Economic and Housing Statistics Division, 11 August 2021. Available online: https://www.census.gov/library/stories/2021/08/economic-hardship-declined-in-households-with-children-as-child-tax-credit-payments-arrived.html (accessed on 6 January 2023).
- Samuelson, K. Food Stamp Work Requirements Increase Mental Health Care Use. Northwestern News, 28 July 2022. Available online: https://news.northwestern.edu/stories/2022/07/food-stamp-work-requirements-increase-men (accessed on 31 December 2022).
- Polsky, J.Y.; Gilmour, H. Food Insecurity and Mental Health during the COVID-19 Pandemic. Health Rep. 2020, 31, 3–11. [Google Scholar] [CrossRef]
- Dawes, J.; May, T.; McKinlay, A.; Fancourt, D.; Burton, A. Impact of the COVID-19 Pandemic on the Mental Health and Wellbeing of Parents with Young Children: A Qualitative Interview Study. BMC Psychol. 2021, 9, 194. [Google Scholar] [CrossRef]
- Costello, E.J.; Compton, S.N.; Keeler, G.; Angold, A. Relationships between Poverty and Psychopathology: A Natural Experiment. JAMA 2003, 290, 2023–2029. [Google Scholar] [CrossRef] [Green Version]
- Costello, E.J.; Erkanli, A.; Copeland, W.; Angold, A. Association of Family Income Supplements in Adolescence with Development of Psychiatric and Substance Use Disorders in Adulthood among an American Indian Population. JAMA 2010, 303, 1954–1960. [Google Scholar] [CrossRef] [Green Version]
- 2020 Mom. The Child Tax Credit: Tackling Child Poverty and Maternal Mental Health. 2020 Mom, 23 November 2021. Available online: https://www.2020mom.org/blog/2021/11/23/the-child-tax-credit-tackling-child-poverty-and-maternal-mental-health (accessed on 25 December 2022).
- Huang, C.; Feng, Q.; Zhang, B.; Ren, H.; Liu, Z.; Kang, Y.; Zhang, F. Income and Social Support Related with Mental Health during COVID-19 Outbreak in China. Medicine. Baltimore 2022, 101, e29022. [Google Scholar] [CrossRef]
- Simonse, O.; Van Dijk, W.W.; Van Dillen, L.F.; Van Dijk, E. The Role of Financial Stress in Mental Health Changes during COVID-19. NPJ Ment. Health Res. 2022, 1, 15. [Google Scholar] [CrossRef]
- Benfer, E.A.; Wiley, L.F. Health Justice Strategies to Combat COVID-19: Protecting Vulnerable Communities During a Pan-demic. Health Aff. Forefr. 2020. [Google Scholar] [CrossRef]
- Furlong, M.; McGilloway, S.; Mulligan, C.; Killion, M.G.; McGarr, S.; Grant, A.; Davidson, G.; Donaghy, M. Covid-19 and Families with Parental Mental Illness: Crisis and Opportunity. Front. Psychiatry 2021, 12, 567447. [Google Scholar] [CrossRef]
- Gadermann, A.C.; Thomson, K.C.; Richardson, C.G.; Gagné, M.; McAuliffe, C.; Hirani, S.; Jenkins, E. Examining the Impacts of the COVID-19 Pandemic on Family Mental Health in Canada: Findings from a National Cross-Sectional Study. BMJ Open 2021, 11, e042871. [Google Scholar] [CrossRef]
- Kerr, M.L.; Fanning, K.A.; Huynh, T.; Botto, I.; Kim, C.N. Parents’ Self-Reported Psychological Impacts of COVID-19: Associations with Parental Burnout, Child Behavior, and Income. J. Pediatr. Psychol. 2021, 46, 1162–1171. [Google Scholar] [CrossRef]
- Westrupp, E.M.; Bennett, C.; Berkowitz, T.; Youssef, G.J.; Toumbourou, J.W.; Tucker, R.; Andrews, F.J.; Evans, S.; Teague, S.J.; Karantzas, G.C.; et al. Child, Parent, and Family Mental Health and Functioning in Australia during COVID-19: Comparison to Pre-Pandemic Data. Eur. Child Adolesc. Psychiatry 2021, 32, 317–330. [Google Scholar] [CrossRef]
- Marroquín, B.; Vine, V.; Morgan, R. Mental Health during the COVID-19 Pandemic: Effects of Stay-at-Home Policies, Social Distancing Behavior, and Social Resources. Psychiatry Res. 2020, 293, 113419. [Google Scholar] [CrossRef]
- World Health Organization. Mental Health and Psychosocial Considerations during the COVID-19 Outbreak. 18 March 2020. Available online: https://apps.who.int/iris/handle/10665/331490 (accessed on 3 January 2023).
- Wu, M.; Xu, W.; Yao, Y.; Zhang, L.; Guo, L.; Fan, J.; Chen, J. Mental Health Status of Students’ Parents during COVID-19 Pandemic and Its Influence Factors. Gen. Psych. 2020, 33, e100250. [Google Scholar] [CrossRef]
- Plummer, F.; Manea, L.; Trepel, D.; McMillan, D. Screening for Anxiety Disorders with the GAD-7 and GAD-2: A Systematic Review and Diagnostic Metaanalysis. Gen. Hosp. Psychiatry 2016, 39, 24–31. [Google Scholar] [CrossRef]
- Arroll, B.; Goodyear-Smith, F.; Crengle, S.; Gunn, J.; Kerse, N.; Fishman, T.; Falloon, K.; Hatcher, S. Validation of PHQ-2 and PHQ-9 to Screen for Major Depression in the Primary Care Population. Ann. Fam. Med. 2010, 8, 348–353. [Google Scholar] [CrossRef] [Green Version]
- Banks, J.; Xu, X. The Mental Health Effects of the First Two Months of Lockdown during the COVID-19 Pandemic in the UK. Fisc. Stud. 2020, 41, 685–708. [Google Scholar] [CrossRef]
- Emsley, R.; Liu, H. Stata Module to Perform Causal Mediation Analysis Using Parametric Regression Models. 2013. Available online: https://econpapers.repec.org/software/bocbocode/S457581.htm (accessed on 4 January 2023).
- Valeri, L.; Vanderweele, T.J. Mediation Analysis Allowing for Exposure-Mediator Interactions and Causal Interpretation: Theoretical Assumptions and Implementation with SAS and SPSS Macros. Psychol. Methods 2013, 18, 137–150. [Google Scholar] [CrossRef] [Green Version]
- Baron, R.M.; Kenny, D.A. The Moderator–Mediator Variable Distinction in Social Psychological Research: Conceptual, Strategic, and Statistical Considerations. J. Personal. Soc. Psychol. 1986, 51, 1173–1182. [Google Scholar] [CrossRef] [PubMed]
- Blount, D.; Minoff, E. The Child Tax Credit & Family Economic Security: Findings from the Center for the Study of Social Policy’s Survey of Families with Children. 2022. Available online: https://cssp.org/resource/the-child-tax-credit-family-economic-security (accessed on 6 January 2023).
- Collin, D.F.; Shields-Zeeman, L.S.; Batra, A.; White, J.S.; Tong, M.; Hamad, R. The Effects of State Earned Income Tax Credits on Mental Health and Health Behaviors: A Quasi-Experimental Study. Soc. Sci. Med. 2021, 276, 113274. [Google Scholar] [CrossRef] [PubMed]
- Bovell-Ammon, A.; McCann, N.; Mulugeta, M.; Ettinger de Cuba, S.; Raifman, J.; Shafer, P.; Children’s HealthWatch. Food Insufficiency in Families with Children Increased after Expiration of Child Tax Credit Monthly Payments. 2022. Available online: https://childrenshealthwatch.org/food-insufficiency-in-families-with-children-increased-after-expiration-of-child-tax-credit-monthly-payments (accessed on 29 December 2022).
- Grinstein-Weiss, J.J.; Hamilton, L.; Roll, S.; Grinstein-Weiss, M. The New Child Tax Credit Does More than Just Cut Poverty; Brookings: Washington, DC, USA, 2021. [Google Scholar]
- Rachidi, A. Why a Fully Refundable CTC Is the Wrong Policy for Working Families. American Enterprise Institute—AEI. 2021. Available online: https://www.aei.org/articles/why-a-fully-refundable-ctc-is-the-wrong-policy-for-working-families (accessed on 3 January 2023).
- Dasso, R.; Fernandez, F. Temptation Goods and Conditional Cash Transfers in Peru; International Food and Policy Research Institute: Washington, DC, USA, 2014. [Google Scholar]
- Burroughs, J.E.; Rindfleisch, A. Materialism and Well-Being: A Conflicting Values Perspective. J. Consum. Res. 2002, 29, 348–370. [Google Scholar] [CrossRef]
- Duhachek, A. Coping: A Multidimensional, Hierarchical Framework of Responses to Stressful Consumption Episodes. J. Consum. Res. 2005, 32, 41–53. Available online: https://academic.oup.com/jcr/article-abstract/32/1/41/1796354?redirectedFrom=fulltext (accessed on 12 February 2023). [CrossRef]
- Halvatsiotis, P.; Kotanidou, A.; Tzannis, K.; Jahaj, E.; Magira, E.; Theodorakopoulou, M.; Konstandopoulou, G.; Gkeka, E.; Pourzitaki, C.; Kapravelos, N.; et al. Demographic and Clinical Features of Critically Ill Patients with COVID-19 in Greece: The Burden of Diabetes and Obesity. Diabetes Res. Clin. Pract. 2020, 166, 108331. [Google Scholar] [CrossRef]
- Hesham, F.; Riadh, H.; Sihem, N.K. What Have We Learned about the Effects of the COVID-19 Pandemic on Consumer Behavior? Sustainability 2021, 13, 4304. [Google Scholar] [CrossRef]
- Bell, T. The Covid Certainty: More Savings for the Rich, More Debt for the Poor; Resolution Foundation: London, UK, 2021. [Google Scholar]
- Crosta, A.D.; Ceccato, I.; Marchetti, D.; Malva, P.L.; Maiella, R.; Cannito, L.; Cipi, M.; Mammarella, N.; Palumbo, R.; Verrocchio, M.C.; et al. Psychological Factors and Consumer Behavior during the COVID-19 Pandemic. PLoS ONE 2021, 16, e0256095. [Google Scholar] [CrossRef]


{kind=link}
| Variables | Full Sample (n = 98,026), %, Mean (SD) | Generalized Anxiety Disorder | Major Depressive Disorder | ||
|---|---|---|---|---|---|
| Yes (n = 30,604), %, Mean (SD) | No (n = 67,422), %, Mean (SD) | Yes (n = 20,367), %, Mean (SD) | No (n = 77,659), %, Mean (SD) | ||
| Exposures, mean (SD) | |||||
| Receipt of CTC during the COVID-19 pandemic | 0.169 (0.375) | 0.173 (0.378) | 0.167 (0.373) | 0.174 (0.379) | 0.167 (0.373) |
| Mediators, mean (SD) | |||||
| CTC spending on basic necessities as mediator | |||||
| CTC spent on food | 0.514 (0.5) | 0.566 (0.496) | 0.488 (0.5) | 0.579 (0.494) | 0.493 (0.5) |
| CTC spent on rent or mortgage | 0.287 (0.453) | 0.364 (0.481) | 0.25 (0.433) | 0.392 (0.489) | 0.255 (0.436) |
| CTC spent on clothing | 0.292 (0.455) | 0.321 (0.467) | 0.278 (0.448) | 0.328 (0.47) | 0.281 (0.45) |
| CTC spending on child education as mediator | |||||
| CTC spent on childcare | 0.11 (0.313) | 0.126 (0.332) | 0.103 (0.304) | 0.119 (0.324) | 0.108 (0.31) |
| CTC spent on schoolbooks and supplies | 0.169 (0.375) | 0.197 (0.398) | 0.156 (0.363) | 0.201 (0.401) | 0.16 (0.366) |
| CTC spent on school tuition | 0.05 (0.217) | 0.048 (0.214) | 0.05 (0.218) | 0.048 (0.213) | 0.05 (0.218) |
| CTC spent on tutoring services | 0.013 (0.11) | 0.015 (0.12) | 0.012 (0.105) | 0.015 (0.121) | 0.012 (0.107) |
| CTC spent on afterschool programs | 0.036 (0.185) | 0.037 (0.187) | 0.035 (0.183) | 0.037 (0.187) | 0.035 (0.184) |
| CTC spent on transportation for school | 0.041 (0.197) | 0.055 (0.228) | 0.033 (0.179) | 0.059 (0.236) | 0.035 (0.183) |
| CTC spent on recreational goods | 0.043 (0.202) | 0.047 (0.211) | 0.041 (0.198) | 0.044 (0.205) | 0.043 (0.202) |
| CTC spending on household expenditure as mediator | |||||
| CTC spent on utilities and telecommunications | 0.313 (0.464) | 0.403 (0.491) | 0.27 (0.444) | 0.434 (0.496) | 0.276 (0.447) |
| CTC spent on vehicle payments | 0.134 (0.341) | 0.181 (0.385) | 0.111 (0.314) | 0.189 (0.391) | 0.117 (0.322) |
| CTC spent on paying off credit cards or debts | 0.186 (0.389) | 0.218 (0.413) | 0.17 (0.376) | 0.218 (0.413) | 0.176 (0.381) |
| CTC spent on savings or investments | 0.162 (0.368) | 0.104 (0.306) | 0.19 (0.392) | 0.097 (0.296) | 0.182 (0.386) |
| CTC spent on donations or giving to family | 0.012 (0.107) | 0.012 (0.107) | 0.012 (0.108) | 0.011 (0.1) | 0.012 (0.109) |
| Covariates, % of sample | |||||
| Demographic characteristics | |||||
| Age | |||||
| 18–24 (Ref) | 3.0 | 4.0 | 2.5 | 4.5 | 2.6 |
| 25–34 | 23.4 | 27.4 | 21.4 | 28.4 | 21.8 |
| 35–44 | 40.1 | 40.5 | 40.0 | 38.8 | 40.5 |
| 45–54 | 22.9 | 19.7 | 24.5 | 19.4 | 24.0 |
| 55–64 | 7.2 | 5.9 | 7.8 | 6.4 | 7.5 |
| 65–74 | 2.8 | 2.0 | 3.1 | 1.9 | 3.0 |
| 75+ | 0.6 | 0.4 | 0.7 | 0.5 | 0.6 |
| Gender | |||||
| Female (Ref) | 57.1 | 64.8 | 53.4 | 62.1 | 55.6 |
| Male | 42.9 | 35.2 | 46.6 | 37.9 | 44.4 |
| Race/ethnicity | |||||
| Non-Hispanic White (Ref) | 56.2 | 57.5 | 55.6 | 54.9 | 56.6 |
| Non-Hispanic Black | 13.3 | 13.6 | 13.1 | 14.4 | 12.9 |
| Non-Hispanic A and PI | 5.6 | 3.4 | 6.7 | 3.8 | 6.2 |
| Non-Hispanic other | 4.2 | 4.9 | 3.8 | 5.4 | 3.8 |
| Hispanic | 20.7 | 20.6 | 20.8 | 21.6 | 20.5 |
| Marital status | |||||
| Unmarried (Ref) | 30.0 | 38.4 | 26.0 | 42.4 | 26.2 |
| Married | 70.0 | 61.7 | 74.0 | 57.6 | 73.8 |
| Children in household | |||||
| No child (Ref) | 3.9 | 3.9 | 4.0 | 4.7 | 3.7 |
| One or more children | 96.1 | 96.2 | 96.0 | 95.3 | 96.3 |
| Household size | |||||
| Single person (Ref) | 0.4 | 0.4 | 0.3 | 0.6 | 0.3 |
| 2-person | 3.5 | 4.0 | 3.3 | 4.5 | 3.2 |
| 3-person | 21.4 | 21.9 | 21.1 | 21.7 | 21.3 |
| 4-person | 33.8 | 32.4 | 34.4 | 30.7 | 34.7 |
| 5-person | 21.1 | 20.3 | 21.5 | 20.3 | 21.3 |
| 6 or more persons | 19.9 | 20.9 | 19.4 | 22.3 | 19.2 |
| Socioeconomic status (SES) | |||||
| Education | |||||
| Less than high school (Ref) | 8.5 | 8.8 | 8.4 | 9.1 | 8.4 |
| High school | 27.4 | 29.0 | 26.6 | 32.0 | 26.0 |
| Some college and AA | 31.4 | 35.4 | 29.4 | 37.0 | 29.7 |
| BA+ | 32.7 | 26.8 | 35.6 | 22.0 | 36.0 |
| Household income | |||||
| Less than USD 25,000 (Ref) | 13.9 | 19.8 | 11.0 | 21.7 | 11.5 |
| USD 25,000–49,999 | 24.1 | 28.0 | 22.2 | 31.7 | 21.7 |
| USD 50,000–74,999 | 17.2 | 17.9 | 16.8 | 17.1 | 17.2 |
| USD 75,000–99,999 | 13.5 | 12.4 | 14.1 | 11.3 | 14.2 |
| USD 100,000–USD 149,999 | 17.3 | 12.9 | 19.4 | 10.8 | 19.3 |
| USD 150,000 and above | 14.0 | 9.1 | 16.4 | 7.4 | 16.1 |
| Health insurance status | |||||
| Public health insurance | |||||
| No (Ref) | 69.7 | 63.5 | 72.7 | 60.9 | 72.3 |
| Yes | 30.3 | 36.5 | 27.4 | 39.1 | 27.7 |
| Private health insurance | |||||
| No (Ref) | 25.7 | 32.8 | 22.2 | 36.0 | 22.6 |
| Yes | 74.3 | 67.2 | 77.7 | 64.0 | 77.4 |
| Location of residence | |||||
| 15 largest metropolitan statistical area | |||||
| None (Ref) | 68.8 | 71.4 | 67.5 | 71.0 | 68.1 |
| New York | 4.8 | 4.1 | 5.2 | 3.8 | 5.1 |
| Los Angeles | 3.8 | 3.2 | 4.2 | 3.4 | 4.0 |
| Chicago | 2.6 | 2.4 | 2.7 | 2.4 | 2.6 |
| Dallas | 2.5 | 2.5 | 2.6 | 2.8 | 2.5 |
| Houston | 2.4 | 2.4 | 2.4 | 2.4 | 2.4 |
| Washington, D.C. | 1.8 | 1.6 | 2.0 | 1.6 | 1.9 |
| Miami | 1.6 | 1.6 | 1.6 | 1.5 | 1.7 |
| Philadelphia | 1.8 | 2.0 | 1.8 | 2.0 | 1.8 |
| Atlanta | 1.9 | 1.7 | 2.0 | 1.7 | 1.9 |
| Phoenix | 1.7 | 1.6 | 1.8 | 1.6 | 1.8 |
| Boston | 1.2 | 1.0 | 1.4 | 0.9 | 1.4 |
| San Francisco | 0.9 | 0.8 | 1.0 | 0.8 | 0.9 |
| Riverside | 1.6 | 1.3 | 1.7 | 1.6 | 1.6 |
| Detroit | 1.2 | 1.2 | 1.2 | 1.3 | 1.1 |
| Seattle | 1.2 | 1.3 | 1.2 | 1.2 | 1.2 |
| 50 States and Washington, D.C. | - | - | - | - | - |
| Mediator Variables | CTC Receipt–Anxiety Relationship | |||
|---|---|---|---|---|
| OR | (95% CI) | p | % of Total Effect | |
| CTC spending on basic necessities as mediator | ||||
| CTC spent on food | ||||
| Direct | 0.954 | (0.912, 0.998) | 0.039 | 54 |
| Indirect | 0.958 | (0.938, 0.98) | <0.001 | 46 |
| Total | 0.914 | (0.879, 0.952) | <0.001 | 100 |
| CTC spent on rent or mortgage | ||||
| Direct | 0.957 | (0.919, 0.998) | 0.036 | 56 |
| Indirect | 0.965 | (0.952, 0.98) | <0.001 | 44 |
| Total | 0.924 | (0.888, 0.962) | <0.001 | 100 |
| CTC spent on clothing | ||||
| Direct | 0.920 | (0.884, 0.959) | <0.001 | 96 |
| Indirect | 0.997 | (0.986, 1.009) | 0.575 | 4 |
| Total | 0.917 | (0.882, 0.955) | <0.001 | 100 |
| CTC spending on child education as mediator | ||||
| CTC spent on childcare | ||||
| Direct | 0.926 | (0.89, 0.965) | <0.001 | 87 |
| Indirect | 0.988 | (0.981, 0.995) | 0.001 | 13 |
| Total | 0.915 | (0.88, 0.953) | <0.001 | 100 |
| CTC spent on schoolbooks and supplies | ||||
| Direct | 0.926 | (0.888, 0.967) | <0.001 | 90 |
| Indirect | 0.991 | (0.974, 1.009) | 0.304 | 10 |
| Total | 0.918 | (0.882, 0.955) | <0.001 | 100 |
| CTC spent on school tuition | ||||
| Direct | 0.920 | (0.884, 0.958) | <0.001 | 93 |
| Indirect | 0.994 | (0.989, 0.999) | 0.027 | 7 |
| Total | 0.914 | (0.879, 0.952) | <0.001 | 100 |
| CTC spent on tutoring services | ||||
| Direct | 0.916 | (0.881, 0.954) | <0.001 | 98 |
| Indirect | 0.998 | (0.997, 1.001) | 0.065 | 2 |
| Total | 0.915 | (0.879, 0.952) | <0.001 | 100 |
| CTC spent on afterschool programs | ||||
| Direct | 0.917 | (0.881, 0.955) | <0.001 | 97 |
| Indirect | 0.997 | (0.995, 1.001) | 0.059 | 3 |
| Total | 0.914 | (0.879, 0.952) | <0.001 | 100 |
| CTC spent on transportation for school | ||||
| Direct | 0.919 | (0.884, 0.957) | <0.001 | 96 |
| Indirect | 0.996 | (0.994, 0.999) | 0.004 | 4 |
| Total | 0.916 | (0.881, 0.954) | <0.001 | 100 |
| CTC spent on recreational goods | ||||
| Direct | 0.915 | (0.879, 0.952) | <0.001 | 99 |
| Indirect | 0.999 | (0.998, 1.001) | 0.244 | 1 |
| Total | 0.914 | (0.879, 0.952) | <0.001 | 100 |
| CTC spending on household expenditure as mediator | ||||
| CTC spent on utilities and telecommunications | ||||
| Direct | 0.948 | (0.91, 0.988) | 0.010 | 64 |
| Indirect | 0.969 | (0.959, 0.98) | <0.001 | 36 |
| Total | 0.918 | (0.883, 0.956) | <0.001 | 100 |
| CTC spent on vehicle payments | ||||
| Direct | 0.928 | (0.892, 0.966) | <0.001 | 87 |
| Indirect | 0.988 | (0.983, 0.994) | <0.001 | 13 |
| Total | 0.917 | (0.882, 0.955) | <0.001 | 100 |
| CTC spent on paying off credit cards or debts | ||||
| Direct | 0.937 | (0.899, 0.978) | 0.002 | 73 |
| Indirect | 0.975 | (0.964, 0.988) | <0.001 | 27 |
| Total | 0.914 | (0.879, 0.952) | <0.001 | 100 |
| CTC spent on savings or investments | ||||
| Direct | 0.871 | (0.836, 0.909) | <0.001 | 140 |
| Indirect | 1.043 | (1.026, 1.06) | <0.001 | −40 |
| Total | 0.908 | (0.873, 0.946) | <0.001 | 100 |
| CTC spent on charitable donations or giving to family | ||||
| Direct | 0.914 | (0.879, 0.952) | <0.001 | 100 |
| Indirect | 1.000 | (1, 1.001) | 0.947 | 0 |
| Total | 0.914 | (0.879, 0.952) | <0.001 | 100 |
| Mediator Variables | CTC Receipt–Anxiety Relationship | |||
|---|---|---|---|---|
| OR | (95% CI) | p | % of Total Effect | |
| CTC spending on basic necessities as mediator | ||||
| CTC spent on food | ||||
| Direct | 0.965 | (0.918, 1.016) | 0.170 | 47 |
| Indirect | 0.959 | (0.936, 0.983) | 0.001 | 53 |
| Total | 0.926 | (0.885, 0.969) | 0.001 | 100 |
| CTC spent on rent or mortgage | ||||
| Direct | 0.982 | (0.938, 1.029) | 0.437 | 30 |
| Indirect | 0.958 | (0.943, 0.974) | <0.001 | 70 |
| Total | 0.940 | (0.899, 0.984) | 0.008 | 100 |
| CTC spent on clothing | ||||
| Direct | 0.929 | (0.888, 0.973) | 0.002 | 91 |
| Indirect | 0.992 | (0.98, 1.005) | 0.233 | 9 |
| Total | 0.922 | (0.882, 0.965) | <0.001 | 100 |
| CTC spending on child education as mediator | ||||
| CTC spent on childcare | ||||
| Direct | 0.931 | (0.89, 0.975) | 0.002 | 87 |
| Indirect | 0.989 | (0.981, 0.997) | 0.006 | 13 |
| Total | 0.921 | (0.881, 0.964) | <0.001 | 100 |
| CTC spent on schoolbooks and supplies | ||||
| Direct | 0.938 | (0.894, 0.985) | 0.010 | 81 |
| Indirect | 0.984 | (0.965, 1.005) | 0.125 | 19 |
| Total | 0.924 | (0.884, 0.967) | 0.001 | 100 |
| CTC spent on school tuition | ||||
| Direct | 0.924 | (0.883, 0.967) | 0.001 | 95 |
| Indirect | 0.996 | (0.991, 1.002) | 0.184 | 5 |
| Total | 0.920 | (0.88, 0.963) | <0.001 | 100 |
| CTC spent on tutoring services | ||||
| Direct | 0.921 | (0.881, 0.964) | <0.001 | 98 |
| Indirect | 0.999 | (0.998, 1.001) | 0.116 | 2 |
| Total | 0.920 | (0.88, 0.963) | <0.001 | 100 |
| CTC spent on afterschool programs | ||||
| Direct | 0.922 | (0.882, 0.965) | <0.001 | 97 |
| Indirect | 0.998 | (0.995, 1.001) | 0.150 | 3 |
| Total | 0.920 | (0.88, 0.963) | <0.001 | 100 |
| CTC spent on transportation for school | ||||
| Direct | 0.926 | (0.886, 0.969) | 0.001 | 96 |
| Indirect | 0.997 | (0.995, 1) | 0.017 | 4 |
| Total | 0.923 | (0.883, 0.966) | 0.001 | 100 |
| CTC spent on recreational goods | ||||
| Direct | 0.920 | (0.88, 0.963) | <0.001 | 100 |
| Indirect | 1.000 | (0.999, 1.002) | 0.852 | 0 |
| Total | 0.920 | (0.88, 0.962) | <0.001 | 100 |
| CTC spending on household expenditure as mediator | ||||
| CTC spent on utilities and telecommunications | ||||
| Direct | 0.964 | (0.921, 1.009) | 0.114 | 54 |
| Indirect | 0.968 | (0.957, 0.98) | <0.001 | 46 |
| Total | 0.933 | (0.892, 0.976) | 0.003 | 100 |
| CTC spent on vehicle payments | ||||
| Direct | 0.937 | (0.896, 0.98) | 0.004 | 87 |
| Indirect | 0.990 | (0.984, 0.997) | 0.002 | 13 |
| Total | 0.927 | (0.887, 0.97) | 0.001 | 100 |
| CTC spent on paying off credit cards or debts | ||||
| Direct | 0.944 | (0.901, 0.99) | 0.016 | 71 |
| Indirect | 0.976 | (0.963, 0.989) | <0.001 | 29 |
| Total | 0.921 | (0.881, 0.964) | <0.001 | 100 |
| CTC spent on savings or investments | ||||
| Direct | 0.896 | (0.854, 0.942) | <0.001 | 133 |
| Indirect | 1.029 | (1.008, 1.051) | 0.007 | −33 |
| Total | 0.922 | (0.882, 0.965) | <0.001 | 100 |
| CTC spent on charitable donations or giving to family | ||||
| Direct | 0.920 | (0.88, 0.963) | <0.001 | 100 |
| Indirect | 1.000 | (1, 1.001) | 0.638 | 0 |
| Total | 0.920 | (0.88, 0.963) | <0.001 | 100 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Park, J.; Kim, S. Child Tax Credit, Spending Patterns, and Mental Health: Mediation Analyses of Data from the U.S. Census Bureau’s Household Pulse Survey during COVID-19. Int. J. Environ. Res. Public Health 2023, 20, 4425. https://doi.org/10.3390/ijerph20054425
Park J, Kim S. Child Tax Credit, Spending Patterns, and Mental Health: Mediation Analyses of Data from the U.S. Census Bureau’s Household Pulse Survey during COVID-19. International Journal of Environmental Research and Public Health. 2023; 20(5):4425. https://doi.org/10.3390/ijerph20054425
Chicago/Turabian StylePark, JungHo, and Sujin Kim. 2023. "Child Tax Credit, Spending Patterns, and Mental Health: Mediation Analyses of Data from the U.S. Census Bureau’s Household Pulse Survey during COVID-19" International Journal of Environmental Research and Public Health 20, no. 5: 4425. https://doi.org/10.3390/ijerph20054425