
A Systematic Review of Child Health, Developmental and Educational Outcomes Associated with High Mobility in Indigenous Children from Australia, Canada and New Zealand
 , , , and
, , , and
Abstract
:1. Introduction
1.1. Definitions
First Nations Peoples
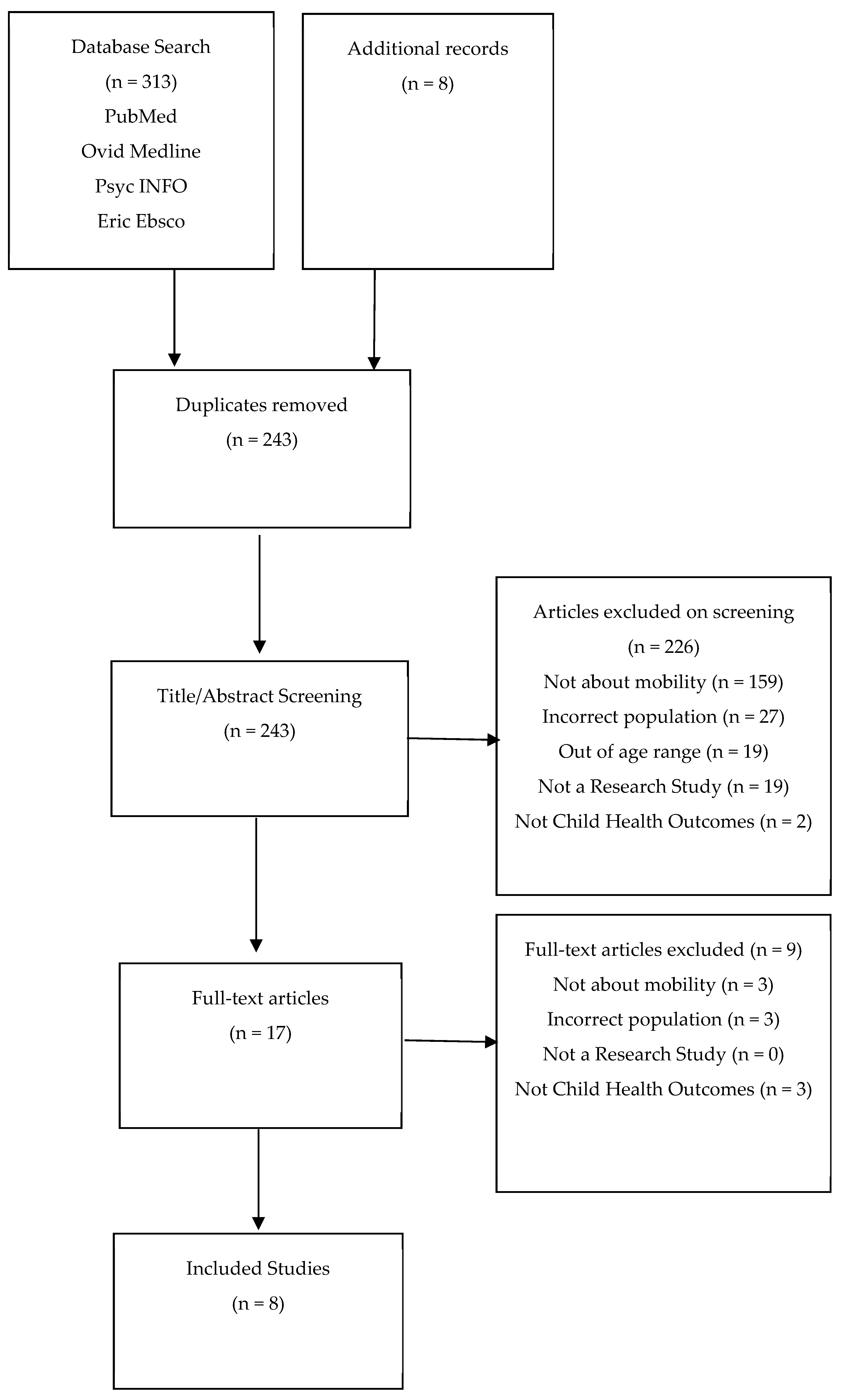
2. Materials and Methods
2.1. Search Strategy
2.2. Study Selection
2.2.1. Inclusion Criteria
- Original research including cross-sectional, prospective, and retrospective cohort studies, case-control studies, randomized trials, record linkage studies, and qualitative studies. Grey literature was included once reference lists of included research articles were searched;
- Indigenous or First Nation children aged 0–12 years from Australia, Canada, and New Zealand were included in the study population;
- Studies providing a definition of ‘high mobility’ and identifying children and families with high mobility;
- Studies reporting child health outcomes examined by mobility. Child health outcomes were broadly defined to include development, physical health, mental health and well-being, social and emotional well-being, cognition, behavioral issues, and academic outcomes.
2.2.2. Exclusion Criteria
2.3. Data Extraction
2.4. Critical and Cultural Appraisal
3. Results
3.1. Study Characteristics
3.1.1. Quantitative Studies
3.1.2. Qualitative Studies
3.2. Defining and Measuring Mobility in the Studies (Aim 1)
3.2.1. Quantitative Studies
3.2.2. Qualitative Studies
3.3. Child Health Outcomes Reported in Included Studies (Aim 2)
3.4. Physical Health
3.4.1. Quantitative Studies
3.4.2. Qualitative Studies
3.5. Social and Emotional Outcomes
3.5.1. Quantitative Studies
3.5.2. Qualitative Studies
3.6. Learning and Development Outcomes
3.6.1. Quantitative Outcomes
3.6.2. Qualitative Studies
3.7. Critical Appraisal
3.8. Cultural Appraisal
4. Discussion
Strengths and Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Australian Institute of Health and Welfare. Australia’s Children; Cat. No. CWS 69; AIHW: Canberra, Australia, 2020. [Google Scholar]
- Bernard, A.; Forder, P.; Kendig, H.; Byles, J. Residential mobility in Australia and the United States: A retrospective study. Aust. Popul. Stud. 2017, 1, 41–54. [Google Scholar] [CrossRef]
- Jelleyman, T.; Spencer, N. Residential mobility in childhood and health outcomes: A systematic review. J. Epidemiol. Community Health 2008, 62, 584–592. [Google Scholar] [CrossRef]
- Phinney, R. Exploring Residential Mobility among Low-Income Families. Soc. Serv. Rev. 2013, 87, 780–815. [Google Scholar] [CrossRef] [Green Version]
- Ziol-Guest, K.M.; McKenna, C.C. Early childhood housing instability and school readiness. Child Dev. 2014, 85, 103–113. [Google Scholar] [CrossRef] [PubMed]
- Baker, E.; Bentley, R.; Lester, L.; Beer, A. Housing affordability and residential mobility as drivers of locational inequality. Appl. Geogr. 2016, 72, 65–75. [Google Scholar] [CrossRef]
- Mallett, S.; Bentley, R.; Baker, E.; Mason, K.; Keys, D.; Kolar, V.; Krnjacki, L. Precarious Housing and Health Inequalities: What Are the Links? Summary Report; Hanover Welfare Services, University of Melbourne, University of Adelaide: Melbourne Citymission, Australia, 2011. [Google Scholar]
- Snyder, M.; Wilson, K. “Too much moving... there’s always a reason”: Understanding urban Aboriginal peoples’ experiences of mobility and its impact on holistic health. Health Place 2015, 34, 181–189. [Google Scholar] [CrossRef] [PubMed]
- Lawrence, E.; Root, E.D.; Mollborn, S. Residential Mobility in Early Childhood: Household and Neighborhood Characteristics of Movers and Non-Movers. Demogr. Res. 2016, 33, 939–950. [Google Scholar] [CrossRef] [Green Version]
- Saghapour, T.; Moridpour, S. The role of neighbourhoods accessibility in residential mobility. Cities 2019, 87, 1–9. [Google Scholar] [CrossRef]
- Bronfenbrenner, U.; Morris, P.A. Handbook of child psychology: Theoretical models of human development. In The Ecology of Developmental Processes; Lerner, W.D.a.R.M., Ed.; John Wiley & Sons Inc.: Hoboken, NJ, USA, 1998; pp. 993–1028. [Google Scholar]
- Simsek, M.; Costa, R.; de Valk, H.A.G. Childhood residential mobility and health outcomes: A meta-analysis. Health Place 2021, 71, 102650. [Google Scholar] [CrossRef]
- Coley, R.L.; Kull, M. Cumulative, Timing-Specific, and Interactive Models of Residential Mobility and Children’s Cognitive and Psychosocial Skills. Child Dev. 2016, 87, 1205. [Google Scholar] [CrossRef]
- Garboden, P.M.E.; Leventhal, T.; Newman, S. Estimating the Effects of Residential Mobility: A Methodological Note. J. Soc. Serv. Res. 2017, 43, 246–261. [Google Scholar] [CrossRef]
- Taylor Matthew, E.B. Housing and children’s wellbeing and development. Evidence from a national longitudinal study. Fam. Matters 2012, 91, 47–61. [Google Scholar]
- Rumbold, A.; Giles, L.; Whitrow, M.; Steele, E.; Davies, C.; Davies, M.; Moore, V. The effects of house moves during early childhood on child mental health at age 9 years. BMC Public Health 2012, 12, 583. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vidal, S.; Baxter, J. Residential relocations and academic performance of Australian children: A longitudinal analysis. Longitud. Life Course Stud. 2018, 9, 133–156. [Google Scholar] [CrossRef]
- Dockery, L.J.; Mahendran, A.; Ong, R.; Strazdins, L. Housing and Children’s Development and Wellbeing a Scoping Study AHURI Final Report No. 149; Melbourne Australian Housing and Urban Research Institute: Melbourne, Australia, 2010. [Google Scholar]
- CASP Checklists. Available online: https://casp-uk.net/casp-tools-checklists/ (accessed on 13 November 2022).
- Aboriginal and Torres Strait Islander Quality Appraisal Tool. Available online: https://create.sahmri.org/wp-content/uploads/2020/04/Aboriginal-and-Torres-Strait-Islander-QAT.pdf (accessed on 27 February 2023).
- Harfield, S.; Pearson, O.; Morey, K.; Kite, E.; Canuto, K.; Glover, K.; Gomersall, J.S.; Carter, D.; Davy, C.; Aromataris, E.; et al. Assessing the quality of health research from an Indigenous perspective: The Aboriginal and Torres Strait Islander quality appraisal tool. BMC Med. Res. Methodol. 2020, 20, 79. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Williamson, A.; D’Este, C.; Clapham, K.; Redman, S.; Manton, T.; Eades, S.; Schuster, L.; Raphael, B. What are the factors associated with good mental health among Aboriginal children in urban New South Wales, Australia? Phase I findings from the Study of Environment on Aboriginal Resilience and Child Health (SEARCH). BMJ Open 2016, 6, e011182. [Google Scholar] [CrossRef] [Green Version]
- Chando, S.; Craig, J.C.; Burgess, L.; Sherriff, S.; Purcell, A.; Gunasekera, H.; Banks, S.; Smith, N.; Banks, E.; Woolfenden, S. Developmental risk among Aboriginal children living in urban areas in Australia: The Study of Environment on Aboriginal Resilience and Child Health (SEARCH). BMC Pediatr. 2020, 20, 13. [Google Scholar] [CrossRef]
- Anderson, M.; Williamson, A.; Fernando, P.; Redman, S.; Vincent, F. “There’s a housing crisis going on in Sydney for Aboriginal people”: Focus group accounts of housing and percieved associations with health. BMC Public Health 2016, 16, 429. [Google Scholar] [CrossRef] [Green Version]
- Lowell, A.; Maypilama, L.; Fasoli, L.; Guyula, Y.; Guyula, A.; Yunupiŋu, M.; Godwin-Thompson, J.; Gundjarranbuy, R.; Armstrong, E.; Garrutju, J.; et al. The ‘invisible homeless’—Challenges faced by families bringing up their children in a remote Australian Aboriginal community. BMC Public Health 2018, 18, 1382. [Google Scholar] [CrossRef]
- Zubrick, S.R.; Silburn, S.R.; Lawrence, D.M.; Mitrou, F.; Dalby, R.B.; Blair, E.M.; Griffin, J.; Milroy, H.; De Maio, J.A.; Cox, A.; et al. The Western Australian Aboriginal Child Health Survey: The Social and Emotional Wellbeing of Aboriginal Children and Young People; Curtin University of Technology and Telethon Institute for Child Health Research: Perth, Australia, 2005. [Google Scholar]
- Zubrick, S.; Silburn, S.; De Maio, J.; Shepherd, C.; Griffin, J.; Dalby, R.; Mitrou, F.; Lawrence, D.; Hayward, C.; Pearson, G.; et al. The Western Australian Aboriginal Child Health Survey: Improving the Educational Experiences of Aboriginal Children and Young People; Curtin University of Technology and Telethon Institute for Child Health Research: Perth, Australia, 2006. [Google Scholar]
- Dockery, A.; Ong, R.; Colquhourthn, S.; Jianghong, L.; Kendall, G. Housing and Children’s Development and Wellbeing: Evidence from Australian Data; Australian Housing and Urban Research Institute: Melbourne, Australia, 2013. [Google Scholar]
- Guevremont, A.; Bougie, E.; Kohen, D. Housing and Health among Young First Nations Children Living Off Reserve: Results from the 2006 Aboriginal Children’s Survey. Aborig. Policy Stud. 2016, 5, 2. [Google Scholar] [CrossRef] [Green Version]
- Aboriginal Children’s Survey. 2006. Available online: https://www150.statcan.gc.ca/n1/en/catalogue/89-634-X (accessed on 10 January 2023).
- Barnabe, C. Towards attainment of Indigenous health through empowerment: Resetting health systems, services and provider approaches. BMJ Glob. Health 2021, 6, e004052. [Google Scholar] [CrossRef] [PubMed]
- United Nations General Assembly. Declaration on the Rights of Indigenous Peoples; United Nations General Assembly: Geneva, Switzerland, 2007. [Google Scholar]
- Silburn, S.R.; De Maio, J.A.; Shepherd, C.; Griffin, J.A.; Mitrou, F.G.; Dalby, R.B.; Hayward, C.; Pearson, G. The Western Australian Aboriginal Child Health Survey: Strengthening the Capacity of Aboriginal Children, Families and Communities; Curtin University of Technology and Telethon Institute for Child Health Research: Perth, Australia, 2006. [Google Scholar]
- Bronfenbrenner, M.P. The Bioecological Model of Human Development. In Handbook of Child Psychology, 6th ed.; Damon, W., Ed.; Tufts University: Medford, MA, USA, 2007; pp. 793–827. [Google Scholar]
- Anderson, S.; Leventhal, T.; Newman, S.; Dupéré, V. Residential Mobility Among Children: A Framework for Child and Family Policy. Cityscape A J. Policy Dev. Res. 2014, 16, 1. [Google Scholar]
- Schmitt, S.A.; Lipscomb, S.T. Longitudinal associations between residential mobility and early academic skills among low-income children. Early Child. Res. Q. 2016, 36, 190–200. [Google Scholar] [CrossRef]
- Snyder, M.; Wilson, K. Urban Aboriginal mobility in Canada: Examining the association with health care utilization. Soc. Sci. Med. 2012, 75, 2420–2424. [Google Scholar] [CrossRef] [Green Version]
- Andersen, M.J.; Williamson, A.B.; Fernando, P.; Eades, S.; Redman, S. ‘They took the land, now we’re fighting for a house’: Aboriginal perspectives about urban housing disadvantage. Hous. Stud. 2017, 33, 635–660. [Google Scholar] [CrossRef]
- Anderson, J.T.; Collins, D. Prevalence and Causes of Urban Homelessness Among Indigenous Peoples: A Three-Country Scoping Review. Hous. Stud. 2014, 29, 959–976. [Google Scholar] [CrossRef]
- Tedmanson, D.; Tually, S.; Habibis, D.; McKinley, K.; Chong, A.; Goodwin-Smith, I.; Akbar, S.; Deuter, K. Urban Indigenous Homelessness: Much More than Housing; AHURI Final Report; Australian Housing and Urban Research Institute Limited: Melbourne, Australia, 2022; No. 383. [Google Scholar] [CrossRef]
- Guenther, J.; Bat, M.; Osborne, S. Red Dirt Thinking on Educational Disadvantage. Aust. J. Indig. Educ. 2013, 42, 100–110. [Google Scholar] [CrossRef] [Green Version]
- Williamson, A.; McElduff, P.; Dadds, M.; D’Este, C.; Redman, S.; Raphael, B.; Daniels, J.; Eades, S. The Construct Validity of the Strengths and Difficulties Questionnaire for Aboriginal Children Living in Urban New South Wales, Australia. Aust. Psychol. 2020, 49, 163–170. [Google Scholar] [CrossRef]
- Young, N.L.; Wabano, M.J.; Usuba, K.; Pangowish, B.; Trottier, M.; Jacko, D.; Burke, T.A.; Corbiere, R.G. Validity of the Aboriginal children’s health and well-being measure: Aaniish Naa Gegii? Health Qual. Life Outcomes 2015, 13, 148. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Saunders, V.; McCalman, J.; Tsey, S.; Askew, D.; Campbell, S.; Jongen, C.; Angelo, C.; Spurling, G.; Cadet-James, Y. Counting what counts: A systematic scoping review of instruments used in primary healthcare services to measure the wellbeing of Indigenous children and youth. BMC Prim. Care 2023, 24, 51. [Google Scholar] [CrossRef] [PubMed]
- Australian Govenment Department of Social Services. Footprints in Time The Longitudinal Study of Indigenous Children Report from Wave 5; Wave 5; Australian Govenment Department of Social Services: Adelaide, SA, Australia, 2015. [Google Scholar]
- Cripps, K.; Habibis, D. Improving Housing and Service Responses to Domestic and Family Violence for Indigenous Individuals and Families; AHURI Final Report; Australian Housing and Urban Research Institute Limited: Melbourne, Australia, 2019; No. 320. [Google Scholar] [CrossRef]
- Andersen, M.J.; Williamson, A.B.; Fernando, P.; Wright, D.; Redman, S. Housing conditions of urban households with Aboriginal children in NSW Australia: Tenure type matters. BMC Public Health 2017, 18, 70. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cohen, R.; Wardrip, K. Should I Stay or Should I Go? Exploring the Effects of Housing Instability and Mobility on Children. 2011. Available online: https://mcstudy.norc.org/publications/files/CohenandWardrip_2009.pdf (accessed on 27 February 2023).
- World Health Organization. Social Determinants of Health. 2022. Available online: https://www.who.int/health-topics/social-determinants-of-health#tab=tab_1 (accessed on 1 August 2022).
- Buckskin, M.; Ah Kit, J.; Glover, K.; Mitchell, A.; Miller, R.; Weetra, D.; Wiebe, J.; Yelland, J.S.; Newbury, J.; Robinson, J.; et al. Aboriginal Families Study: A population-based study keeping community and policy goals in mind right from the start. Int. J. Equity Health 2013, 12, 41. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- The Lowitja Institute. We Nurture Our Culture for Our Future, and out Culture Nurtures Us. Close the Gap; The Lowitja Institute: Melbourne, Australia, 2020. [Google Scholar]
- Habibis, D.; Dunbar, T.; Scrimgeour, M.; Taylor, E.; Nethercote, M. Improving Housing Responses to Indigenous Patterns of Temporary Mobility; AHURI Final Report No. 162; Australian Housing and Urban Research Institute Melbourne: Melbourne, Australia, 2011. [Google Scholar]
- Gee Graham, D.P.; Schultz, C.; Hart, A.; Kelly, K. Aboriginal and Torres Strait Islander Social and Emotional Wellbeing. In Working Together: Aboriginal and Torres Strait Islander Mental Health and Wellbeing Principles and Practice; Dudgeon Pat, M.H., Roz, W., Eds.; 2014; pp. 55–68. Available online: https://www.telethonkids.org.au/globalassets/media/documents/aboriginal-health/working-together-second-edition/working-together-aboriginal-and-wellbeing-2014.pdf (accessed on 28 February 2023).
- Gee, G. Resilience and Recovery from Trauma among Aboriginal Help Seeking Clients in an Urban Aboriginal Community Controlled Organisation. Ph.D. Thesis, University of Melbourne, Melbourne, Australia, 2016. [Google Scholar]
- Gartland, D.; Riggs, E.; Giallo, R.; Glover, K.; Stowe, M.; Mongta, S.; Weetra, D.; Brown, S.J.; Members of the Childhood Resilience Study Collaborative Group. Development and validation of a multidimensional, culturally and socially inclusive Child Resilience Questionnaire (parent/caregiver report) to measure factors that support resilience: A community-based participatory research and psychometric testing study in Australia. BMJ Open 2022, 12, e061129. [Google Scholar] [CrossRef] [PubMed]
- Verbunt, E.; Luke, J.; Paradies, Y.; Bamblett, M.; Salamone, C.; Jones, A.; Kelaher, M. Cultural determinants of health for Aboriginal and Torres Strait Islander people—A narrative overview of reviews. Int. J. Equity Health 2021, 20, 181. [Google Scholar] [CrossRef]


{kind=link}
| First Author | Study Type | Study | Country | Year | Setting | Sample | Indigenous | Child Age (Years) | Data Collection Method |
|---|---|---|---|---|---|---|---|---|---|
| Quantitative | |||||||||
| Zubrick [26] | Cross-sectional | WAACHS 1 | Australia | 2005 | Community | 3993 | 3993 | 4–17 | Parent/Caregiver Survey |
| Zubrick [27] | Cross-sectional | WAACHS 1 | Australia | 2006 | Community | 2379 | 2379 | 4–17 | Parent/Caregiver Survey Teacher/School Principal Survey Child Assessment administered by teacher |
| Dockery [28] | Prospective cohort study | LSIC 2 | Australia | 2013 | Community | B-cohort: 960 K-cohort: 727 | 960 727 | 0–7 | Parent/Caregiver Survey |
| Williamson [22] | Cross-sectional | SEARCH 3 | Australia | 2016 | Community | 1005 | 1005 | 4–17 | Parent/Caregiver Survey |
| Guévremont [29] | Cross-sectional | ACS 4 | Canada | 2016 | Community | 3640 | 3640 | 2–5 | Parent/Caregiver Survey |
| Chando [23] | Cross-sectional | SEARCH 3 | Australia | 2020 | Community | 725 | 725 | 0–8 | Parent/Caregiver Survey |
| Qualitative | |||||||||
| Andersen [24] | Qualitative | Australia | 2016 | Community | 38 adults | 35 adults | 0–18 | Focus Groups | |
| Lowell [25] | Qualitative | Australia | 2018 | Remote Community | 6 families 30 community adults | 6 children | 0–7 | Parent/Caregiver Interviews Family Member Interview Video Recording |
| (a) | |||||||
| First Author | Child (Years) | Definition of High Mobility | High Mobility = n (%) | Physical Health | Social Emotional | Learning Development | Measures |
| Zubrick (2005) [26] | 4–17 | ≥5 moves over child’s lifetime | 3993 (27.4%) | x | Strengths and Difficulties Questionnaire (Modified) -Parent/caregiver report | ||
| Zubrick (2006) [27] | 4–17 | ≥5 moves over child’s lifetime | Not reported | x | Principal Report: ≥26 absences per year ≥10 unexplained absences per year Teacher classification of academic performance | ||
| Dockery [28] | 0–7 | ≥1 move per year of life | 1687 (20%) | x | x | x | General Health Status item (SF-36) Parent Evaluation of Development: 2 Items Social emotional development 3 Items Learning/development |
| Williamson [22] | 4–17 | ≥4 homes previously lived in over child’s lifetime | 327 (37%) | x | Strengths and Difficulties Questionnaire -Parent/caregiver report | ||
| Guévremont [29] | 2–5 | ≥1 move per year of life | 364 (10%) | x | x | Strengths and Difficulties Questionnaire -Parent/caregiver report General Health Status item (SF-36) Single Item Measures: Ear Infections per year Chronic conditions Activity Limitation (yes/no) Chronic Respiratory Conditions (yes/no) Serious Injury in the past year (yes/no) | |
| Chando [23] | 0–8 | Number homes lived in (1, 2, 3, 4+) (Number with 4+ moves reported) | 111 (15%) | x | Parent Evaluation of Development Status 10 Items | ||
| (b) | |||||||
| First Author | Child Age (Years) | Respondent | Housing Mobility Definition | Physical Health | Social Emotional | Learning Development | Concerns Raised for Children Relating to Housing Mobility |
| Anderson [24] | 0–18 | Mothers, Fathers, Grandmothers, Health service staff and clients | Secondary homelessness: frequent relocation, house hopping, and precarious housing. | x | x | x | Concerns with social and emotional behavior Otitis Media or ear infections Asthma and respiratory conditions Injury Risk Disrupted schooling Inadequate sleep High rates of communicable disease Chronic stress of parent/caregiver |
| Lowell [25] | 0–7 | Family and community members | Housing insecurity and moving from house to house: insecure and insufficient housing. | x | x | x | Physical health Behavioral concerns Children’s safety and the potential for accidents Disrupted and inadequate sleep Sharing sickness Limited access to kitchen, bathroom, laundry facilities Food security Conflict/stress amongst families and children |
| First Author | Critical Appraisal Quality | Cultural Appraisal Quality |
|---|---|---|
| Quantitative | ||
| Zubrick 2005 [26] | Medium | Medium |
| Zubrick 2006 [27] | Medium | Medium |
| Dockery [28] | High | Low |
| Williamson [22] | High | High |
| Guévremont [29] | High | Low |
| Chando [23] | High | High |
| Qualitative | ||
| Andersen [24] | High | High |
| Lowell [25] | High | High |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nikolof, A.; Brown, S.J.; Clark, Y.; Glover, K.; Gartland, D. A Systematic Review of Child Health, Developmental and Educational Outcomes Associated with High Mobility in Indigenous Children from Australia, Canada and New Zealand. Int. J. Environ. Res. Public Health 2023, 20, 4332. https://doi.org/10.3390/ijerph20054332
Nikolof A, Brown SJ, Clark Y, Glover K, Gartland D. A Systematic Review of Child Health, Developmental and Educational Outcomes Associated with High Mobility in Indigenous Children from Australia, Canada and New Zealand. International Journal of Environmental Research and Public Health. 2023; 20(5):4332. https://doi.org/10.3390/ijerph20054332
Chicago/Turabian StyleNikolof, Arwen, Stephanie J. Brown, Yvonne Clark, Karen Glover, and Deirdre Gartland. 2023. "A Systematic Review of Child Health, Developmental and Educational Outcomes Associated with High Mobility in Indigenous Children from Australia, Canada and New Zealand" International Journal of Environmental Research and Public Health 20, no. 5: 4332. https://doi.org/10.3390/ijerph20054332