
Ambient Environmental Ozone and Variation of Fractional Exhaled Nitric Oxide (FeNO) in Hairdressers and Healthcare Workers

Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. FeNO Measurement and NIOX VERO© Repeatability
2.3. Statistical Analysis
2.4. Ethics
3. Results
3.1. Demographics
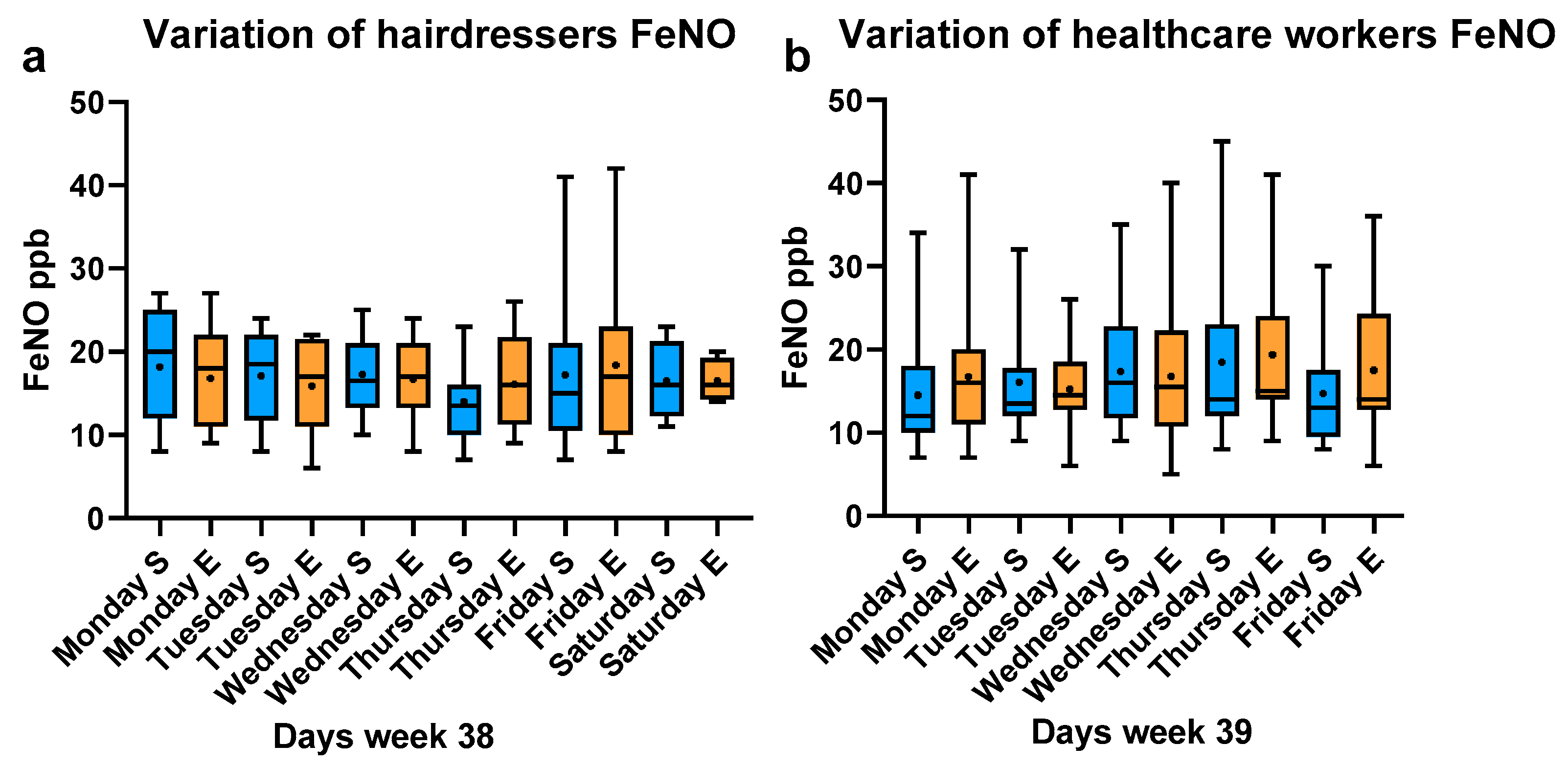
3.2. Diurnal Variation of FeNO
3.3. Air Quality Levels
3.4. FeNO Measurements, Sampling and Commuting Time
3.5. Symptoms of Respiratory Infections
3.6. FeNO, Commuting and Hair Treatments
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Moncada, S.; Palmer, R.M.; Higgs, E.A. Nitric oxide: Physiology, pathophysiology, and pharmacology. Pharmacol. Rev. 1991, 43, 109–142. [Google Scholar] [PubMed]
- Borland, C.; Cox, Y.; Higenbottam, T. Measurement of exhaled nitric oxide in man. Thorax 1993, 48, 1160–1162. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alving, K.; Weitzberg, E.; Lundberg, J.M. Increased amount of nitric oxide in exhaled air of asthmatics. Eur. Respir. J. 1993, 6, 1368–1370. [Google Scholar] [CrossRef] [PubMed]
- Krol, M.; Kepinska, M. Human Nitric Oxide Synthase-Its Functions, Polymorphisms, and Inhibitors in the Context of Inflammation, Diabetes and Cardiovascular Diseases. Int. J. Mol. Sci. 2020, 22, 56. [Google Scholar] [CrossRef]
- Alderton, W.K.; Cooper, C.E.; Knowles, R.G. Nitric oxide synthases: Structure, function and inhibition. Biochem. J. 2001, 357 Pt 3, 593–615. [Google Scholar] [CrossRef]
- Xue, Q.; Yan, Y.; Zhang, R.; Xiong, H. Regulation of iNOS on Immune Cells and Its Role in Diseases. Int. J. Mol. Sci. 2018, 19, 3805. [Google Scholar] [CrossRef] [Green Version]
- Bogdan, C.; Rollinghoff, M.; Diefenbach, A. The role of nitric oxide in innate immunity. Immunol. Rev. 2000, 173, 17–26. [Google Scholar] [CrossRef]
- Salam, M.T.; Byun, H.M.; Lurmann, F.; Breton, C.V.; Wang, X.; Eckel, S.P.; Gilliland, F.D. Genetic and epigenetic variations in inducible nitric oxide synthase promoter, particulate pollution, and exhaled nitric oxide levels in children. J. Allergy Clin. Immunol. 2012, 129, 232–239.e7. [Google Scholar] [CrossRef] [Green Version]
- Ding, R.; Jin, Y.; Liu, X.; Zhu, Z.; Zhang, Y.; Wang, T.; Xu, Y. Characteristics of DNA methylation changes induced by traffic-related air pollution. Mutat. Res. Genet. Toxicol. Environ. Mutagen. 2016, 796, 46–53. [Google Scholar] [CrossRef]
- Leso, V.; Vetrani, I.; Della Volpe, I.; Nocera, C.; Iavicoli, I. Welding Fume Exposure and Epigenetic Alterations: A Systematic Review. Int. J. Environ. Res. Public Health 2019, 16, 1745. [Google Scholar] [CrossRef] [Green Version]
- Niedbala, W.; Cai, B.; Liew, F.Y. Role of nitric oxide in the regulation of T cell functions. Ann. Rheum. Dis. 2006, 65 (Suppl. S3), iii37–iii40. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rupani, H.; Kent, B.D. Using Fractional Exhaled Nitric Oxide Measurement in Clinical Asthma Management. Chest 2022, 161, 906–917. [Google Scholar] [CrossRef] [PubMed]
- Bisgaard, H.; Loland, L.; Oj, J.A. NO in exhaled air of asthmatic children is reduced by the leukotriene receptor antagonist montelukast. Am. J. Respir. Crit. Care Med. 1999, 160, 1227–1231. [Google Scholar] [CrossRef] [PubMed]
- Saito, J.; Gibeon, D.; Macedo, P.; Menzies-Gow, A.; Bhavsar, P.K.; Chung, K.F. Domiciliary diurnal variation of exhaled nitric oxide fraction for asthma control. Eur. Respir. J. 2014, 43, 474–484. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vinnikov, D.; Tulekov, Z.; Blanc, P.D. Fractional exhaled NO in a metalworking occupational cohort. Int. Arch. Occup. Environ. Health 2022, 95, 701–708. [Google Scholar] [CrossRef]
- Ronda, E.; Hollund, B.E.; Moen, B.E. Airborne exposure to chemical substances in hairdresser salons. Environ. Monit. Assess. 2009, 153, 83–93. [Google Scholar] [CrossRef]
- Thurston, G.D.; Balmes, J.R.; Garcia, E.; Gilliland, F.D.; Rice, M.B.; Schikowski, T.; Van Winkle, L.S.; Annesi-Maesano, I.; Burchard, E.G.; Carlsten, C.; et al. Outdoor Air Pollution and New-Onset Airway Disease. An Official American Thoracic Society Workshop Report. Ann. Am. Thorac. Soc. 2020, 17, 387–398. [Google Scholar] [CrossRef]
- Khatri, S.B.; Iaccarino, J.M.; Barochia, A.; Soghier, I.; Akuthota, P.; Brady, A.; Covar, R.A.; Debley, J.S.; Diamant, Z.; Fitzpatrick, A.M.; et al. Use of Fractional Exhaled Nitric Oxide to Guide the Treatment of Asthma: An Official American Thoracic Society Clinical Practice Guideline. Am. J. Respir. Crit. Care Med. 2021, 204, e97–e109. [Google Scholar] [CrossRef]
- Karvonen, T.; Lehtimaki, L. Repeatability and variation of the flow independent nitric oxide parameters. J. Breath Res. 2020, 14, 026002. [Google Scholar] [CrossRef]
- Ulvestad, B.; Lund, M.B.; Bakke, B.; Djupesland, P.G.; Kongerud, J.; Boe, J. Gas and dust exposure in underground construction is associated with signs of airway inflammation. Eur. Respir. J. 2001, 17, 416–421. [Google Scholar] [CrossRef] [Green Version]
- Jonaid, B.S.; Pronk, A.; Doekes, G.; Heederik, D. Exhaled nitric oxide in spray painters exposed to isocyanates: Effect modification by atopy and smoking. Occup. Environ. Med. 2014, 71, 415–422. [Google Scholar] [CrossRef] [PubMed]
- Maniscalco, M.; Grieco, L.; Galdi, A.; Lundberg, J.O.; Sofia, M. Increase in exhaled nitric oxide in shoe and leather workers at the end of the work-shift. Occup. Med. 2004, 54, 404–407. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Otelea, M.R.; Fell, A.K.M.; Handra, C.M.; Holm, M.; Filon, F.L.; Mijakovski, D.; Minov, J.; Mutu, A.; Stephanou, E.; Stokholm, Z.A.; et al. The value of fractional exhaled nitric oxide in occupational diseases—A systematic review. J. Occup. Med. Toxicol. 2022, 17, 14. [Google Scholar] [CrossRef] [PubMed]
- Su, W.; Liu, C.; Hu, Q.; Fan, G.; Xie, Z.; Huang, X.; Zhang, T.; Chen, Z.; Dong, Y.; Ji, X.; et al. Characterization of ozone in the lower troposphere during the 2016 G20 conference in Hangzhou. Sci. Rep. 2017, 7, 17368. [Google Scholar] [CrossRef] [Green Version]
- Liu, H.H.; Wu, Y.C.; Chen, H.L. Production of ozone and reactive oxygen species after welding. Arch. Environ. Contam. Toxicol. 2007, 53, 513–518. [Google Scholar] [CrossRef]
- OSHA Occupational Chemical Database. OZONE. Available online: https://www.osha.gov/chemicaldata/9 (accessed on 29 December 2022).
- World Health Organization. WHO Global Air Quality Guidelines: Particulate Matter (PM2.5 and PM10), Ozone, Nitrogen Dioxide, Sulfur Dioxide and Carbon Monoxide; WHO: Geneva, Switzerland, 2021. [Google Scholar]
- Othman, M.; Latif, M.T.; Yee, C.Z.; Norshariffudin, L.K.; Azhari, A.; Halim, N.D.A.; Alias, A.; Sofwan, N.M.; Hamid, H.H.A.; Matsumi, Y. PM2.5 and ozone in office environments and their potential impact on human health. Ecotoxicol. Environ. Saf. 2020, 194, 110432. [Google Scholar] [CrossRef]
- Lund, M.B.; Kongerud, J.; Nystad, W.; Boe, J.; Harris, J.R. Genetic and environmental effects on exhaled nitric oxide and airway responsiveness in a population-based sample of twins. Eur. Respir. J. 2007, 29, 292–298. [Google Scholar] [CrossRef] [Green Version]
- Modig, L.; Dahgam, S.; Olsson, D.; Nyberg, F.; Wass, K.; Forsberg, B.; Olin, A.C. Short-term exposure to ozone and levels of exhaled nitric oxide. Epidemiology 2014, 25, 79–87. [Google Scholar] [CrossRef]
- Delfino, R.J.; Staimer, N.; Tjoa, T.; Arhami, M.; Polidori, A.; Gillen, D.L.; George, S.C.; Shafer, M.M.; Schauer, J.J.; Sioutas, C. Associations of primary and secondary organic aerosols with airway and systemic inflammation in an elderly panel cohort. Epidemiology 2010, 21, 892–902. [Google Scholar] [CrossRef] [Green Version]
- Barath, S.; Mills, N.L.; Adelroth, E.; Olin, A.C.; Blomberg, A. Diesel exhaust but not ozone increases fraction of exhaled nitric oxide in a randomized controlled experimental exposure study of healthy human subjects. Environ. Health 2013, 12, 36. [Google Scholar] [CrossRef] [Green Version]
- Bohadana, A.; Michaely, J.P.; Teculescu, D.; Wild, P. Reproducibility of exhaled nitric oxide in smokers and non-smokers: Relevance for longitudinal studies. BMC Pulm. Med. 2008, 8, 4. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McConnell, R.; Berhane, K.; Gilliland, F.; London, S.J.; Islam, T.; Gauderman, W.J.; Avol, E.; Margolis, H.G.; Peters, J.M. Asthma in exercising children exposed to ozone: A cohort study. Lancet 2002, 359, 386–391. [Google Scholar] [CrossRef] [PubMed]
- Lin, C.H.; Wong, L.T.; Hsu, J.Y.; Chao, W.C. Relationship between exposure to ozone and exacerbation requiring hospital admission among patients with asthma: A case-control study in central Taiwan. BMJ Open 2022, 12, e050861. [Google Scholar] [CrossRef] [PubMed]
- Ong, C.B.; Kumagai, K.; Brooks, P.T.; Brandenberger, C.; Lewandowski, R.P.; Jackson-Humbles, D.N.; Nault, R.; Zacharewski, T.R.; Wagner, J.G.; Harkema, J.R. Ozone-Induced Type 2 Immunity in Nasal Airways. Development and Lymphoid Cell Dependence in Mice. Am. J. Respir. Cell Mol. Biol. 2016, 54, 331–340. [Google Scholar] [CrossRef] [PubMed]
- Harkema, J.R.; Plopper, C.G.; Hyde, D.M.; St George, J.A.; Wilson, D.W.; Dungworth, D.L. Response of macaque bronchiolar epithelium to ambient concentrations of ozone. Am. J. Pathol. 1993, 143, 857–866. [Google Scholar]
- Devlin, R.B.; McDonnell, W.F.; Mann, R.; Becker, S.; House, D.E.; Schreinemachers, D.; Koren, H.S. Exposure of humans to ambient levels of ozone for 6.6 hours causes cellular and biochemical changes in the lung. Am. J. Respir. Cell Mol. Biol. 1991, 4, 72–81. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Hairdressers N = 14 | Healthcare Workers N = 15 | ||||||
|---|---|---|---|---|---|---|---|
| Female/Male (N) | 12/2 | 12/3 | |||||
| Atopy (N) | 3 | 2 | |||||
| Mean | SD | Range | Mean | SD | Range | p-value * | |
| Age (Y) | 33.4 | 7.3 | 21–50 | 45.9 | 12.5 | 22–66 | 0.001 |
| Weight (Kg) | 70.3 | 14.3 | 48–95 | 70.8 | 13.3 | 50–93 | 0.460 |
| Height (Cm) | 166.5 | 5.7 | 158–174 | 170.2 | 8.7 | 160–190 | 0.093 |
| Body Mass Index (Kg/M2) | 25.2 | 4.5 | 18.7–33.7 | 24.0 | 3.3 | 19.5–30.8 | 0.224 |
| Hairdresser Years | 12.7 | 5.9 | 2–26 | ||||
| Saloon Employees (N) | 6.3 | 1.1 | 3–7 | ||||
| Saloon Area (M2) | 103.3 | 30.9 | 60–140 | ||||
| Feno S | Feno E | p-Value | Sampling * | Commuting * | |
|---|---|---|---|---|---|
| Hairdressers | |||||
| N | 62 | 61 | 61 | 62 | |
| Mean | 16.71 | 16.82 | 0.456 | 211.9 | 23.5 |
| Median | 16.00 | 17.00 | 194.0 | 25.0 | |
| Sd | 6.5 | 6.3 | 39.7 | 10.7 | |
| Range | 7–41 | 6–42 | 180–337 | 1–55 | |
| Healthcare workers | |||||
| N | 70 | 70 | 70 | 70 | |
| Mean | 16.17 | 17.09 | 0.315 | 220.0 | 41.0 |
| Median | 13.50 | 15.00 | 194.5 | 30.0 | |
| Sd | 7.5 | 8.2 | 41.7 | 28.0 | |
| Range | 7–45 | 5–41 | 180–317 | 4–120 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hildre, T.T.; Heiro, H.; Sandven, I.; Hammarström, B. Ambient Environmental Ozone and Variation of Fractional Exhaled Nitric Oxide (FeNO) in Hairdressers and Healthcare Workers. Int. J. Environ. Res. Public Health 2023, 20, 4271. https://doi.org/10.3390/ijerph20054271
Hildre TT, Heiro H, Sandven I, Hammarström B. Ambient Environmental Ozone and Variation of Fractional Exhaled Nitric Oxide (FeNO) in Hairdressers and Healthcare Workers. International Journal of Environmental Research and Public Health. 2023; 20(5):4271. https://doi.org/10.3390/ijerph20054271
Chicago/Turabian StyleHildre, Tonje Trulssen, Hilde Heiro, Ingvill Sandven, and Bato Hammarström. 2023. "Ambient Environmental Ozone and Variation of Fractional Exhaled Nitric Oxide (FeNO) in Hairdressers and Healthcare Workers" International Journal of Environmental Research and Public Health 20, no. 5: 4271. https://doi.org/10.3390/ijerph20054271